
Editorial
Select search scope: search across all journals or within the current journal
A quarter of ischaemic strokes are lacunar subtype, typically neurologically mild, usually resulting from intrinsic cerebral small vessel pathology, with risk factor profiles and outcome rates differing from other stroke subtypes. This European Stroke Organisation (ESO) guideline provides evidence-based recommendations to assist with clinical decisions about management of lacunar ischaemic stroke to prevent adverse clinical outcomes. The guideline was developed according to ESO standard operating procedures and Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) methodology. We addressed acute treatment (including progressive lacunar stroke) and secondary prevention in lacunar ischaemic stroke, and prioritised the interventions of thrombolysis, antiplatelet drugs, blood pressure lowering, lipid lowering, lifestyle, and other interventions and their potential effects on the clinical outcomes recurrent stroke, dependency, major adverse cardiovascular events, death, cognitive decline, mobility, gait, or mood disorders. We systematically reviewed the literature, assessed the evidence and where feasible formulated evidence-based recommendations, and expert concensus statements. We found little direct evidence, mostly of low quality. We recommend that patients with suspected acute lacunar ischaemic stroke receive intravenous alteplase, antiplatelet drugs and avoid blood pressure lowering according to current acute ischaemic stroke guidelines. For secondary prevention, we recommend single antiplatelet treatment long-term, blood pressure control, and lipid lowering according to current guidelines. We recommend smoking cessation, regular exercise, other healthy lifestyle modifications, and avoid obesity for general health benefits. We cannot make any recommendation concerning progressive stroke or other drugs. Large randomised controlled trials with clinically important endpoints, including cognitive endpoints, are a priority for lacunar ischaemic stroke.
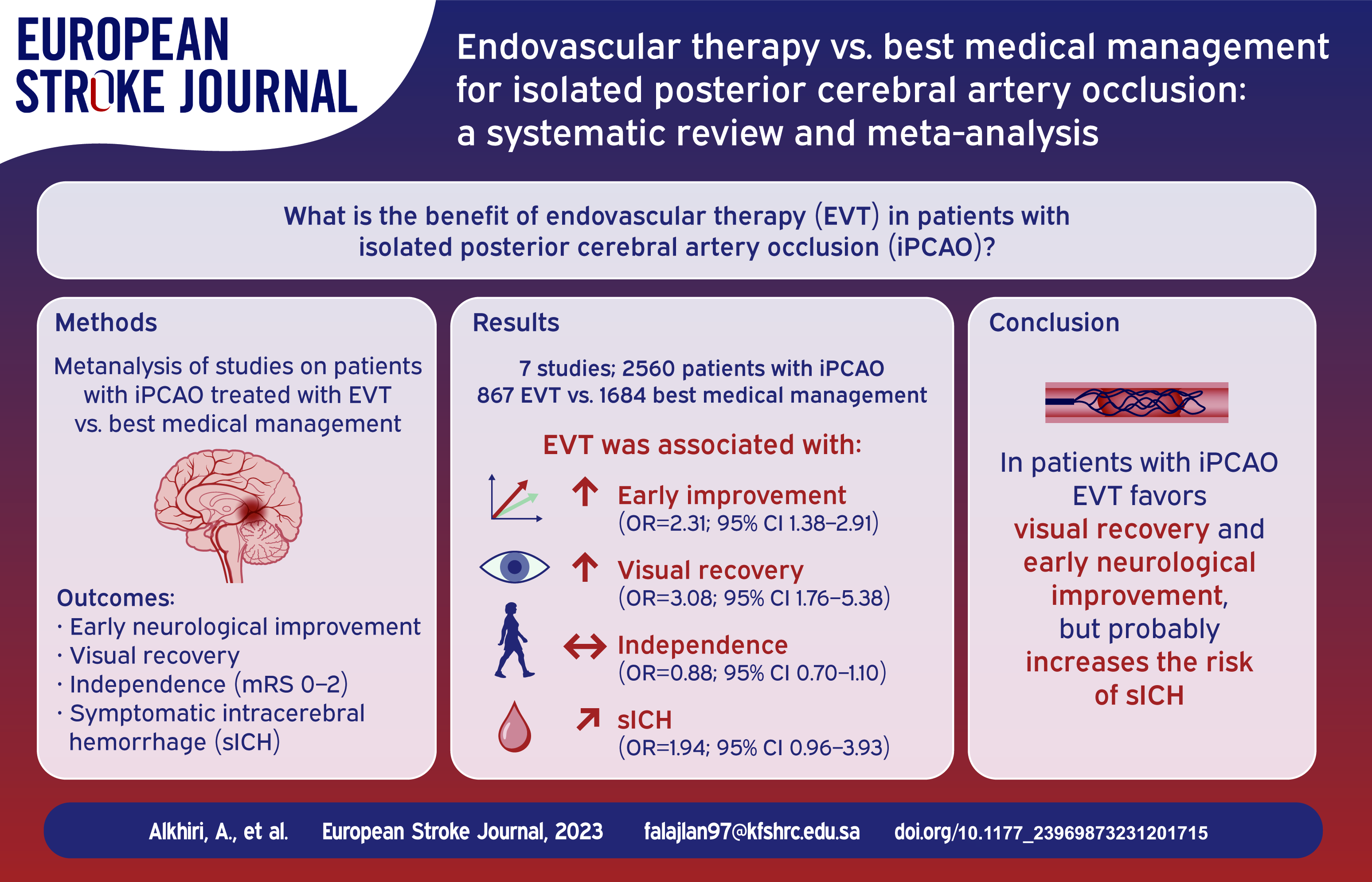
Isolated posterior cerebral artery occlusions (iPCAO) were underrepresented in pivotal randomized clinical trial (RCTs) of endovascular thrombectomy (EVT) in ischemic stroke, and the benefit of EVT in this population is still indeterminate. We performed a systematic review and a meta-analysis to compare the safety and efficacy of EVT compared to best medical management (BMM) in patients with iPCAO.
We searched Medline/PubMed, Embase, Web of Science, and the Cochrane databases up to May 2023 for eligible studies reporting outcomes of patients with iPCAO treated with EVT or BMM. We pooled odds ratios (ORs) with corresponding 95% confidence intervals (CI) using a random-effects model.
Seven studies involving 2560 patients were included. EVT was associated with significantly higher likelihood of early neurological improvement (OR, 2.31 [95% CI, 1.38–2.91];
In patients with iPCAO, EVT was associated with visual and early neurological improvement but with a strong trend toward increased sICH. Survival and functional outcomes may be slightly poorer. The role of EVT in iPCAO remains uncertain.
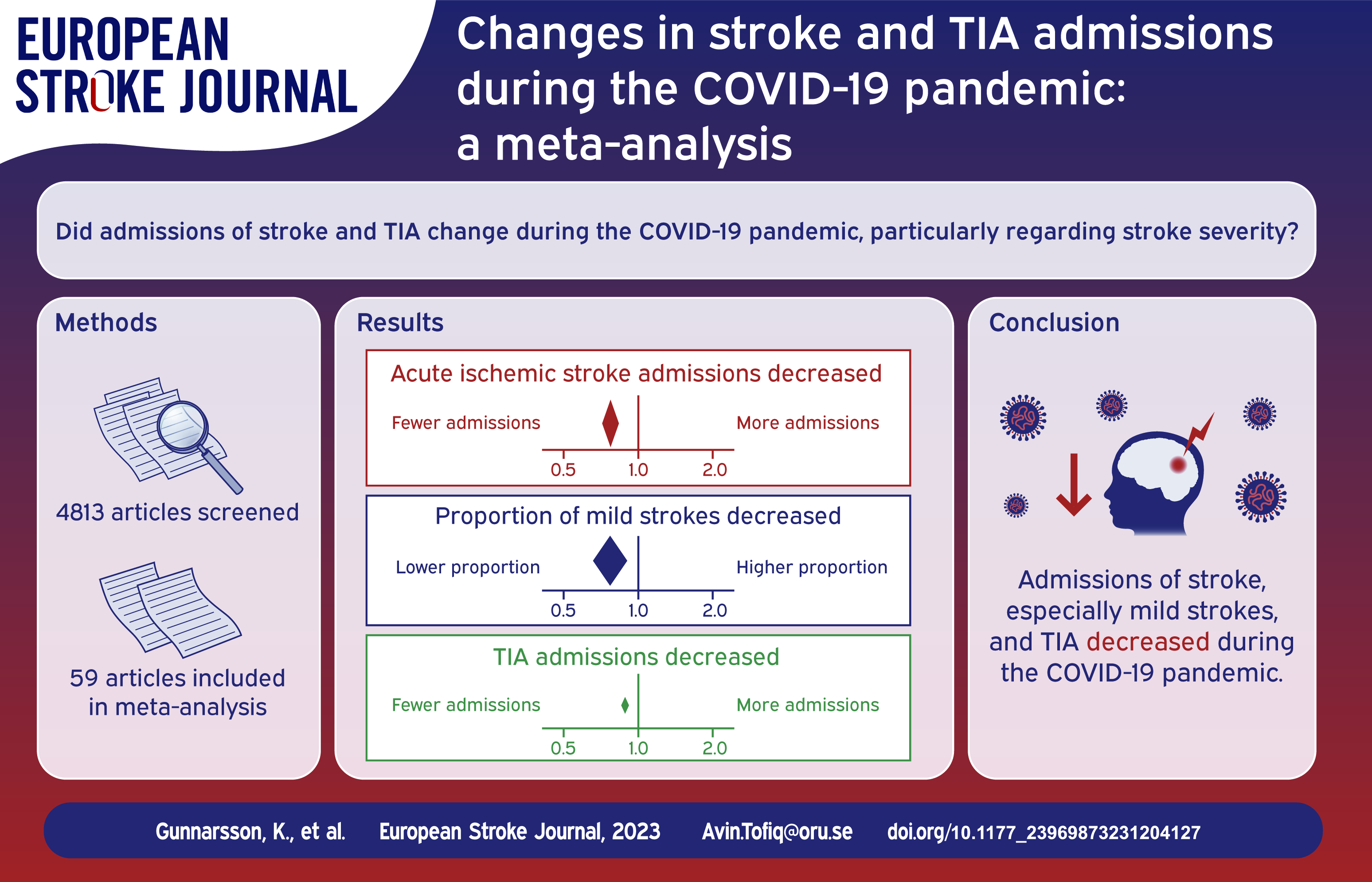
To perform a meta-analysis on how the admissions of stroke and transient ischemic attack (TIA) changed during the Corona Virus infection-19 (COVID-19) pandemic and evaluate if the effect was depending on stroke severity.
Observational cohort studies comparing the number of stroke and/or TIA admissions during a period of the pandemic compared to a period before the pandemic were identified in PubMed and Embase. After excluding studies with overlapping populations and studies without satisfactory case ascertainment, data was extracted and meta-analyzed.
A total of 59 studies were included. During the pandemic, there was a decrease in admissions of ischemic stroke (admission rate ratio (ARR) = 0.77, 95% confidence interval (CI): 0.72, 0.82), intracerebral hemorrhage (ARR = 0.79, 95% CI: 0.70, 0.90) and TIA (ARR = 0.66, 95% CI: 0.58, 0.75). Albeit admission rates of both mild (ARR = 0.61, 95% CI: 0.49, 0.77) and severe (ARR = 0.82, 95% CI = 0.71, 0.95) strokes decreased, milder strokes decreased more (proportion ratio (PR) = 0.76, 95% CI: 0.65, 0.89).
Potential causes for the admission reduction could be strict prioritizations within the health care, patients’ fear of acquiring COVID-19, or decreased access to health care due to lockdowns.
During the COVID-19 pandemic, there was a reduction in admissions of stroke and TIA, possibly caused by reluctance to seek medical care.
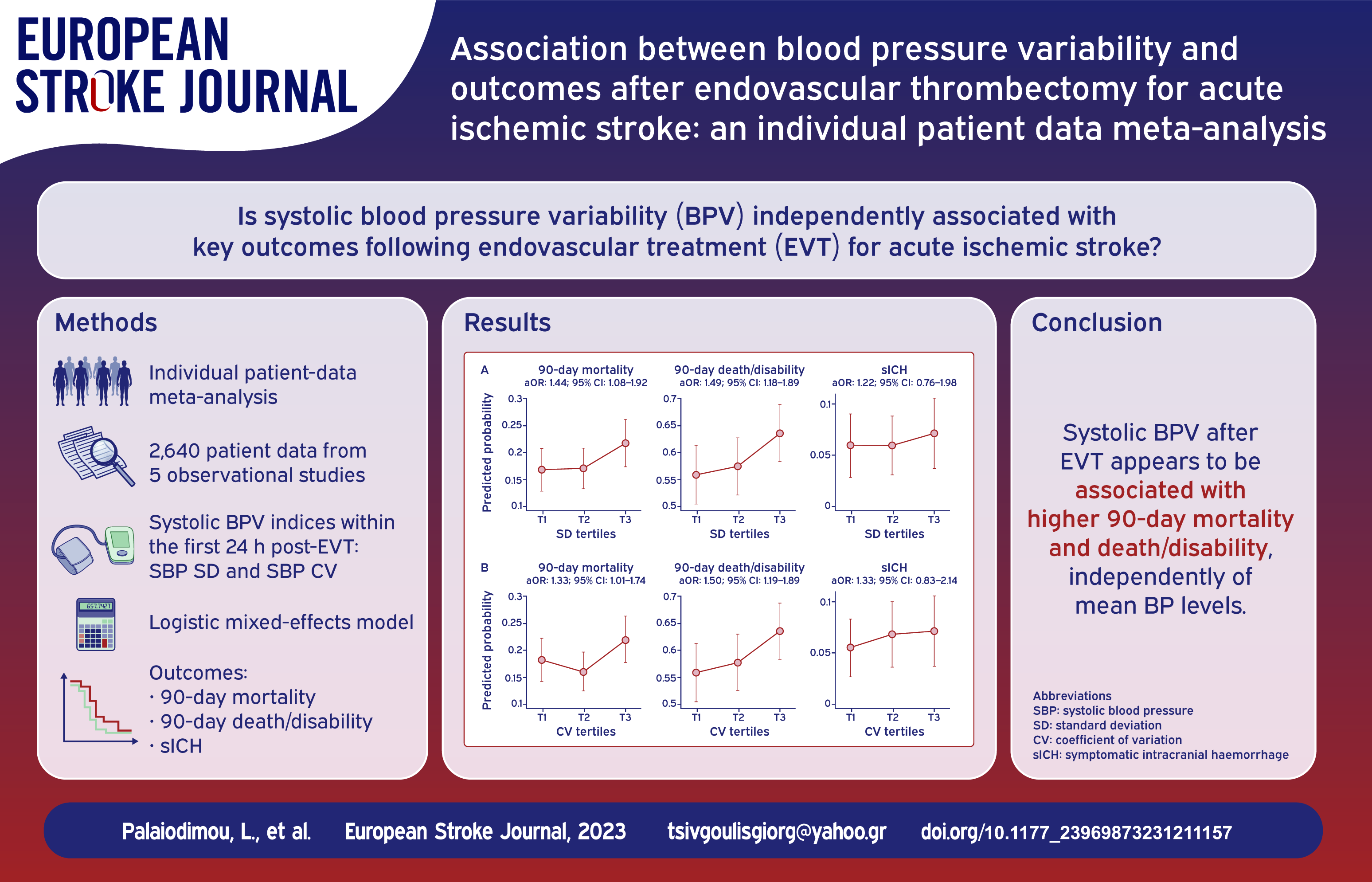
Data on the association between blood pressure variability (BPV) after endovascular thrombectomy (EVT) for acute ischemic stroke (AIS) and outcomes are limited. We sought to identify whether BPV within the first 24 hours post EVT was associated with key stroke outcomes.
We combined individual patient-data from five studies among AIS-patients who underwent EVT, that provided individual BP measurements after the end of the procedure. BPV was estimated as either systolic-BP (SBP) standard deviation (SD) or coefficient of variation (CV) over 24 h post-EVT. We used a logistic mixed-effects model to estimate the association [expressed as adjusted odds ratios (aOR)] between tertiles of BPV and outcomes of 90-day mortality, 90-day death or disability [modified Rankin Scale-score (mRS) > 2], 90-day functional impairment (⩾1-point increase across all mRS-scores), and symptomatic intracranial hemorrhage (sICH), adjusting for age, sex, stroke severity, co-morbidities, pretreatment with intravenous thrombolysis, successful recanalization, and mean SBP and diastolic-BP levels within the first 24 hours post EVT.
There were 2640 AIS-patients included in the analysis. The highest tertile of SBP-SD was associated with higher 90-day mortality (aOR:1.44;95% CI:1.08–1.92), 90-day death or disability (aOR:1.49;95% CI:1.18–1.89), and 90-day functional impairment (adjusted common OR:1.42;95% CI:1.18–1.72), but not with sICH (aOR:1.22;95% CI:0.76–1.98). Similarly, the highest tertile of SBP-CV was associated with higher 90-day mortality (aOR:1.33;95% CI:1.01–1.74), 90-day death or disability (aOR:1.50;95% CI:1.19–1.89), and 90-day functional impairment (adjusted common OR:1.38;95% CI:1.15–1.65), but not with sICH (aOR:1.33;95% CI:0.83–2.14).
BPV after EVT appears to be associated with higher mortality and disability, independently of mean BP levels within the first 24 h post EVT. BPV in the first 24 h may be a novel target to improve outcomes after EVT for AIS.
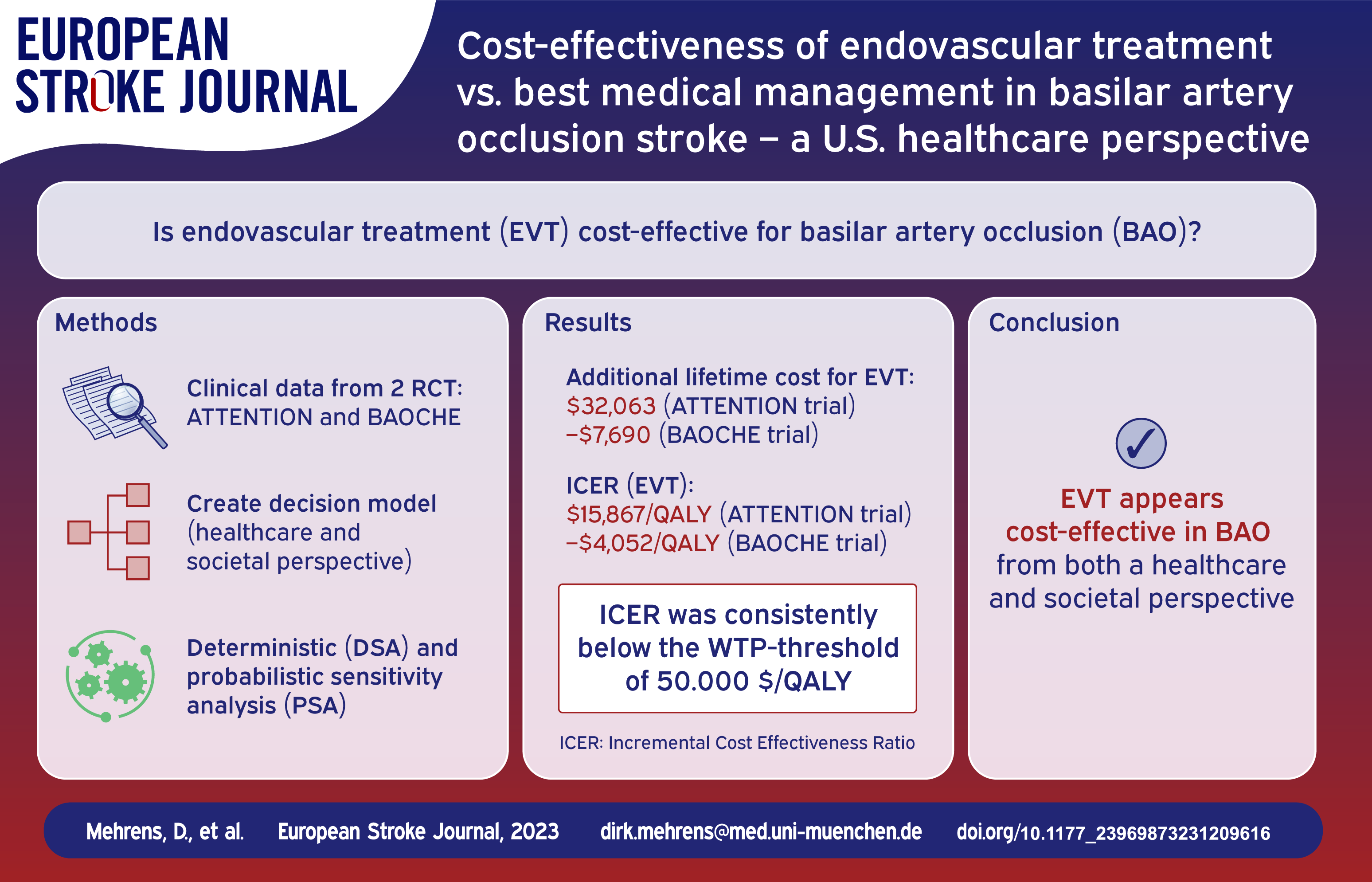
Two recent studies showed clinical benefit for endovascular treatment (EVT) in basilar artery occlusion (BAO) stroke up to 12 h (ATTENTION) and between 6 and 24 h from onset (BAOCHE). Our aim was to investigate the cost-effectiveness of EVT from a U.S. healthcare perspective.
Clinical input data were available for both trials, which were analyzed separately. A decision model was built consisting of a short-run model to analyze costs and functional outcomes within 90 days after the index stroke and a long-run Markov state transition model (cycle length of 12 months) to estimate expected lifetime costs and outcomes from a healthcare and a societal perspective. Incremental cost-effectiveness ratios (ICER) were calculated, deterministic (DSA) and probabilistic (PSA) sensitivity analyses were performed.
EVT in addition to best medical management (BMM) resulted in additional lifetime costs of $32,063 in the ATTENTION trial and lifetime cost savings of $7690 in the BAOCHE trial (societal perspective). From a healthcare perspective, EVT led to incremental costs and effectiveness of $37,389 and 2.0 QALYs (ATTENTION) as well as $3516 and 1.9 QALYs (BAOCHE), compared to BMM alone. The ICER values were $−4052/QALY (BAOCHE) and $15,867/QALY (ATTENTION) from a societal perspective. In each trial, PSA showed EVT to be cost-effective in most calculations (99.9%) for a willingness-to-pay threshold of $100,000/QALY. Cost of EVT and age at stroke represented the greatest impact on the ICER.
From an economic standpoint with a lifetime horizon, EVT in addition to BMM is estimated to be highly effective and cost-effective in BAO stroke.
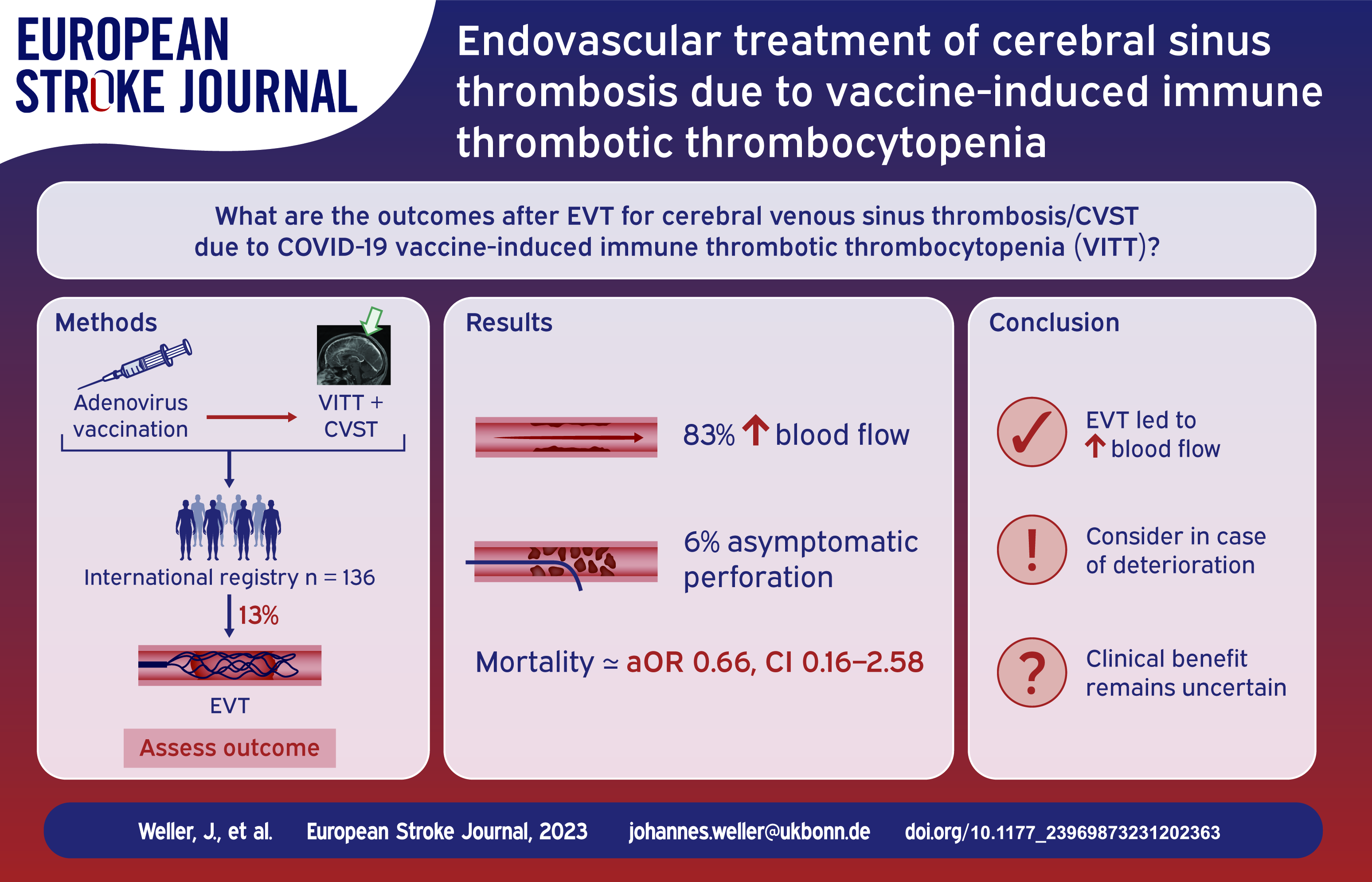
There is little data on the role of endovascular treatment (EVT) of cerebral venous sinus thrombosis (CVST) due to vaccine-induced immune thrombotic thrombocytopenia (VITT). Here, we describe clinical characteristics and outcomes of CVST-VITT patients who were treated with EVT.
We report data from an international registry of patients who developed CVST within 28 days of SARS-CoV-2 vaccination, reported between 29 March 2021 and 6 March 2023. VITT was defined according to the Pavord criteria.
EVT was performed in 18/136 (13%) patients with CVST-VITT (92% aspiration and/or stent retrieval, 8% local thrombolysis). Most common indications were extensive thrombosis and clinical or radiological deterioration. Compared to non-EVT patients, those receiving EVT had a higher median thrombus load (4.5 vs 3). Following EVT, local blood flow was improved in 83% (10/12, 95% confidence interval [CI] 54–96). One (6%) asymptomatic sinus perforation occurred. Eight (44%) patients treated with EVT also underwent decompressive surgery. Mortality was 50% (9/18, 95% CI 29–71) and 88% (8/9, 95% CI 25–66) of surviving EVT patients achieved functional independence with a modified Rankin Scale score of 0–2 at follow-up. In multivariable analysis, EVT was not associated with increased mortality (adjusted odds ratio, 0.66, 95% CI 0.16–2.58).
We describe the largest cohort of CVST-VITT patients receiving EVT. Half of the patients receiving EVT died during hospital admission, but most survivors achieved functional independence.
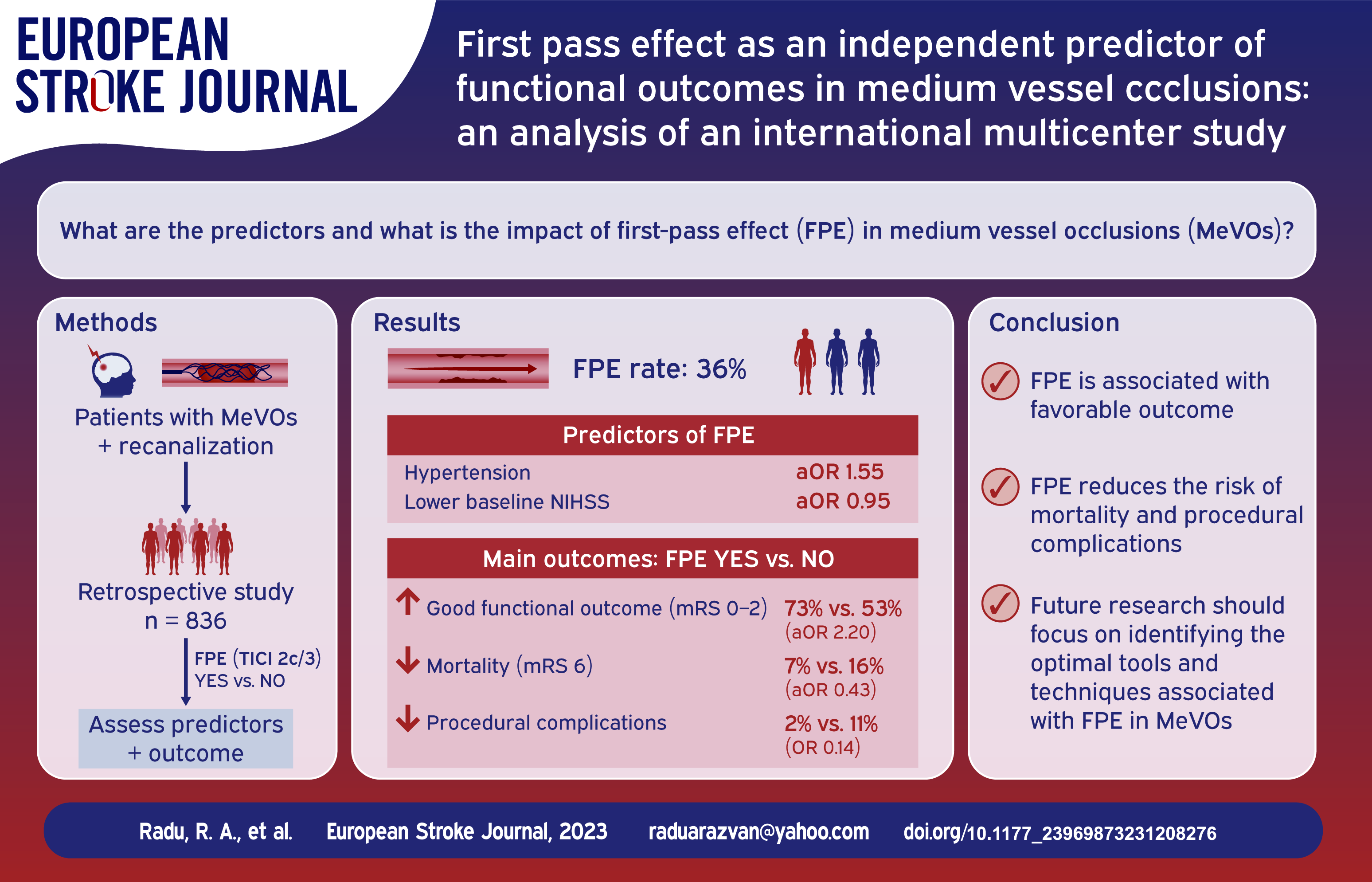
First pass effect (FPE), achievement of complete recanalization (mTICI 2c/3) with a single pass, is a significant predictor of favorable outcomes for endovascular treatment (EVT) in large vessel occlusion stroke (LVO). However, data concerning the impact on functional outcomes and predictors of FPE in medium vessel occlusions (MeVO) are scarce.
We conducted an international retrospective study on MeVO cases. Multivariable logistic modeling was used to establish independent predictors of FPE. Clinical and safety outcomes were compared between the two study groups (FPE vs non-FPE) using logistic regression models. Good outcome was defined as modified Rankin Scale 0–2 at 3 months.
Eight hundred thirty-six patients with a final mTICI ⩾ 2b were included in this analysis. FPE was observed in 302 patients (36.1%). In multivariable analysis, hypertension (aOR 1.55, 95% CI 1.10–2.20) and lower baseline NIHSS score (aOR 0.95, 95% CI 0.93–0.97) were independently associated with an FPE. Good outcomes were more common in the FPE versus non-FPE group (72.8% vs 52.8%), and FPE was independently associated with favorable outcome (aOR 2.20, 95% CI 1.59–3.05). 90-day mortality and intracranial hemorrhage (ICH) were significantly lower in the FPE group, 0.43 (95% CI, 0.25–0.72) and 0.55 (95% CI, 0.39–0.77), respectively.
Over 2/3 of patients with MeVOs and FPE in our cohort had a favorable outcome at 90 days. FPE is independently associated with favorable outcomes, it may reduce the risk of any intracranial hemorrhage, and 3-month mortality.
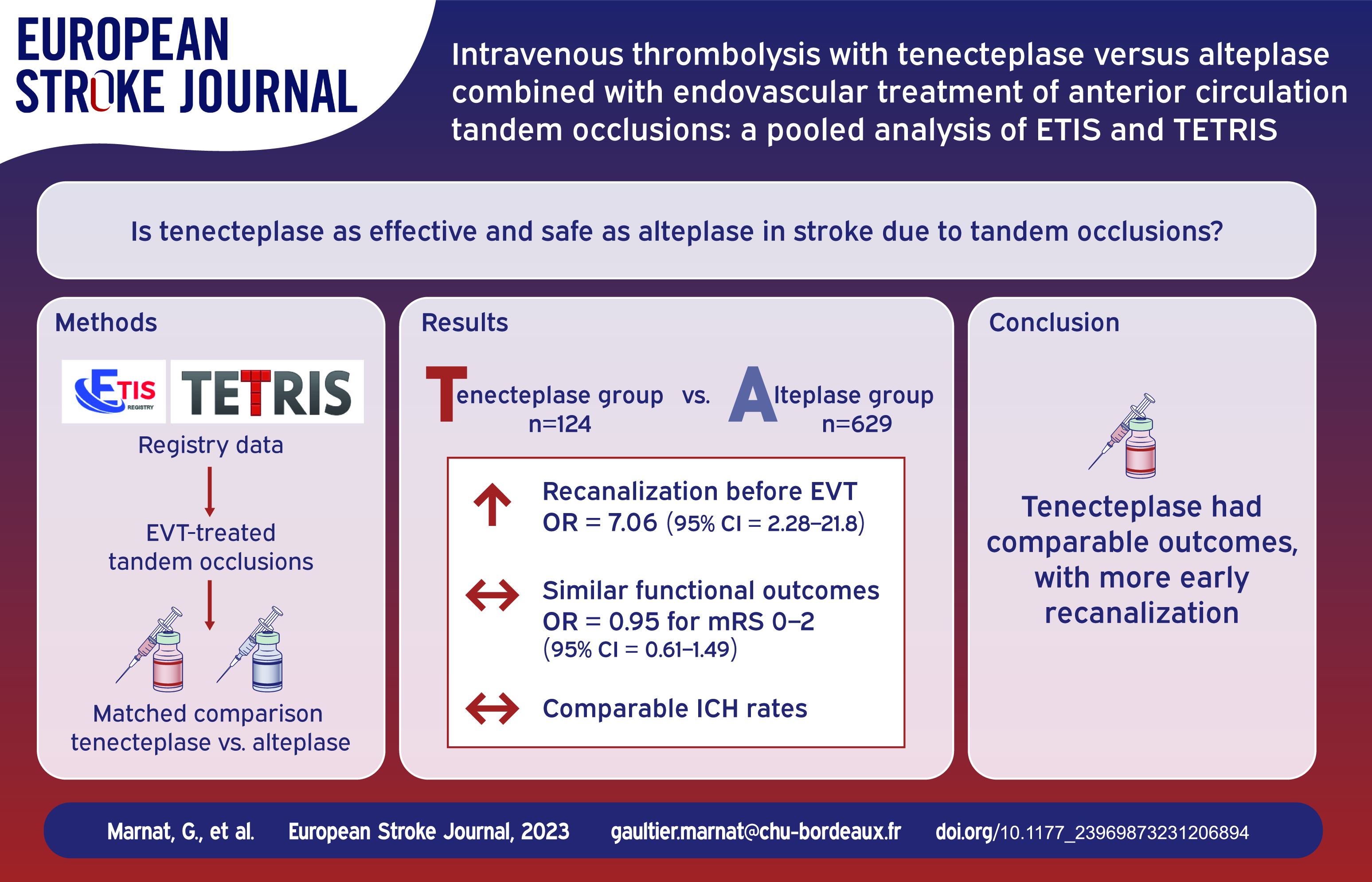
Tandem occlusions are a singular large vessel occlusion entity involving specific endovascular and perioperative antithrombotic management. In this context, data on safety and efficacy of prior intravenous thrombolysis (IVT) with tenecteplase is scarce. We aimed to compare IVT with tenecteplase or alteplase in patients with acute tandem occlusions intended for endovascular treatment.
A retrospective pooled analysis of two large observational registries (ETIS (Endovascular Treatment of Ischemic Stroke) and TETRIS (Tenecteplase Treatment in Ischemic Stroke)) was performed on consecutive patients presenting with anterior circulation tandem occlusion treated with IVT using either alteplase (ETIS) or tenecteplase (TETRIS) followed by endovascular treatment between January 2015 and June 2022. Sensitivity analyses on atherosclerosis related tandem occlusions and on patient treated with emergent carotid stenting were conducted. Propensity score overlap weighting analyses were performed.
We analyzed 753 patients: 124 in the tenecteplase and 629 in the alteplase group. The overall odds of favorable outcome (3-month modified Rankin score 0–2) were comparable between both groups (49.4% vs 47.1%; OR = 1.10, 95%CI 0.85–1.41). Early recanalization, final successful recanalization and mortality favored the use of tenecteplase. The occurrence of any intracranial hemorrhage (ICH) was more frequent after tenecteplase use (OR = 2.24; 95%CI 1.75–2.86). However, risks of symptomatic ICH and parenchymal hematoma remained similar. In atherosclerotic tandems, favorable outcome, mortality, parenchymal hematoma, early recanalization, and final successful recanalization favored the tenecteplase group. In the carotid stenting subgroup, PH were less frequent in the tenecteplase group (OR = 0.18; 95%CI 0.05–0.69).
In patients with tandem occlusions, IVT with tenecteplase seemed reasonably safe in particular with increased early recanalization rates. These findings remain preliminary and should be further confirmed in randomized trials.
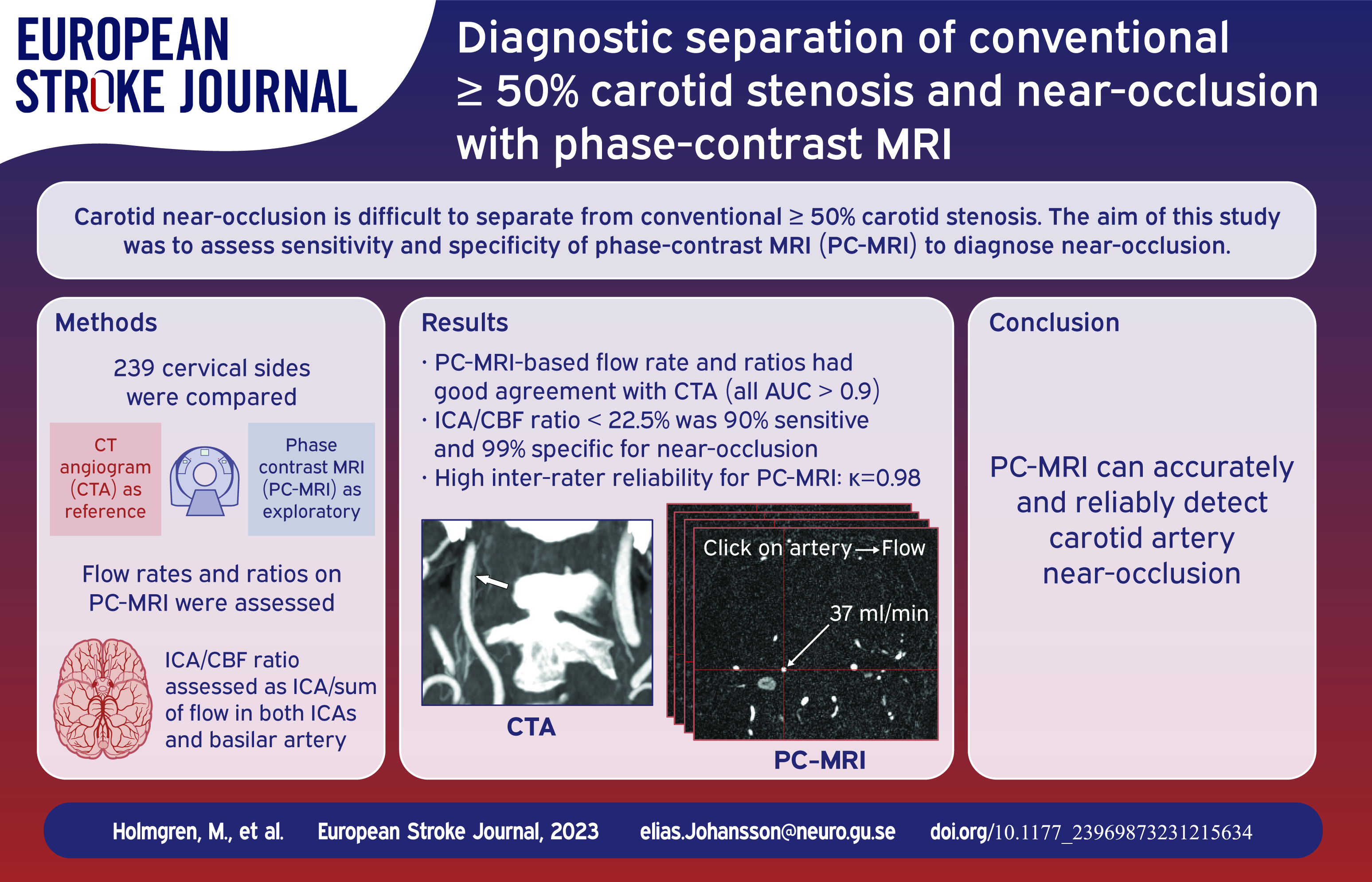
The aim of this study was to assess sensitivity, specificity and interrater reliability of phase-contrast MRI (PC-MRI) for diagnosing carotid near-occlusion.
Prospective cross-sectional study conducted between 2018 and 2021. We included participants with suspected 50%–100% carotid stenosis on at least one side, all were examined with CT angiography (CTA) and PC-MRI and both ICAs were analyzed. Degree of stenosis on CTA was the reference test. PC-MRI-based blood flow rates in extracranial ICA and intracranial cerebral arteries were assessed. ICA-cerebral blood flow (CBF) ratio was defined as ICA divided by sum of both ICAs and Basilar artery.
We included 136 participants. The ICAs were 102 < 50% stenosis, 88 conventional ⩾50% stenosis (31 with ⩾70%), 49 near-occlusion, 12 occlusions, 20 unclear cause of small distal ICA on CTA and one excluded. For separation of near-occlusion and conventional stenoses, ICA flow rate and ICA-CBF ratio had the highest area under the curve (AUC; 0.98–0.99) for near-occlusion. ICA-CBF ratio ⩽0.225 was 90% (45/49) sensitive and 99% (188/190) specific for near-occlusion. Inter-rater reliability for this threshold was excellent (kappa 0.98). Specificity was 94% (29/31) for cases with ⩾70% stenosis. PC-MRI had modest performance for separating <50% and conventional ⩾50% stenosis (highest AUC 0.74), and eight (16%) of near-occlusions were not distinguishable from occlusion (no visible flow).
ICA-CBF ratio ⩽0.225 on PC-MRI is an accurate and reliable method to separate conventional ⩾50% stenosis and near-occlusion that is feasible for routine use. PC-MRI should be considered further as a potential standard method for near-occlusion detection, to be used side-by-side with established modalities as PC-MRI cannot separate other degrees of stenosis.
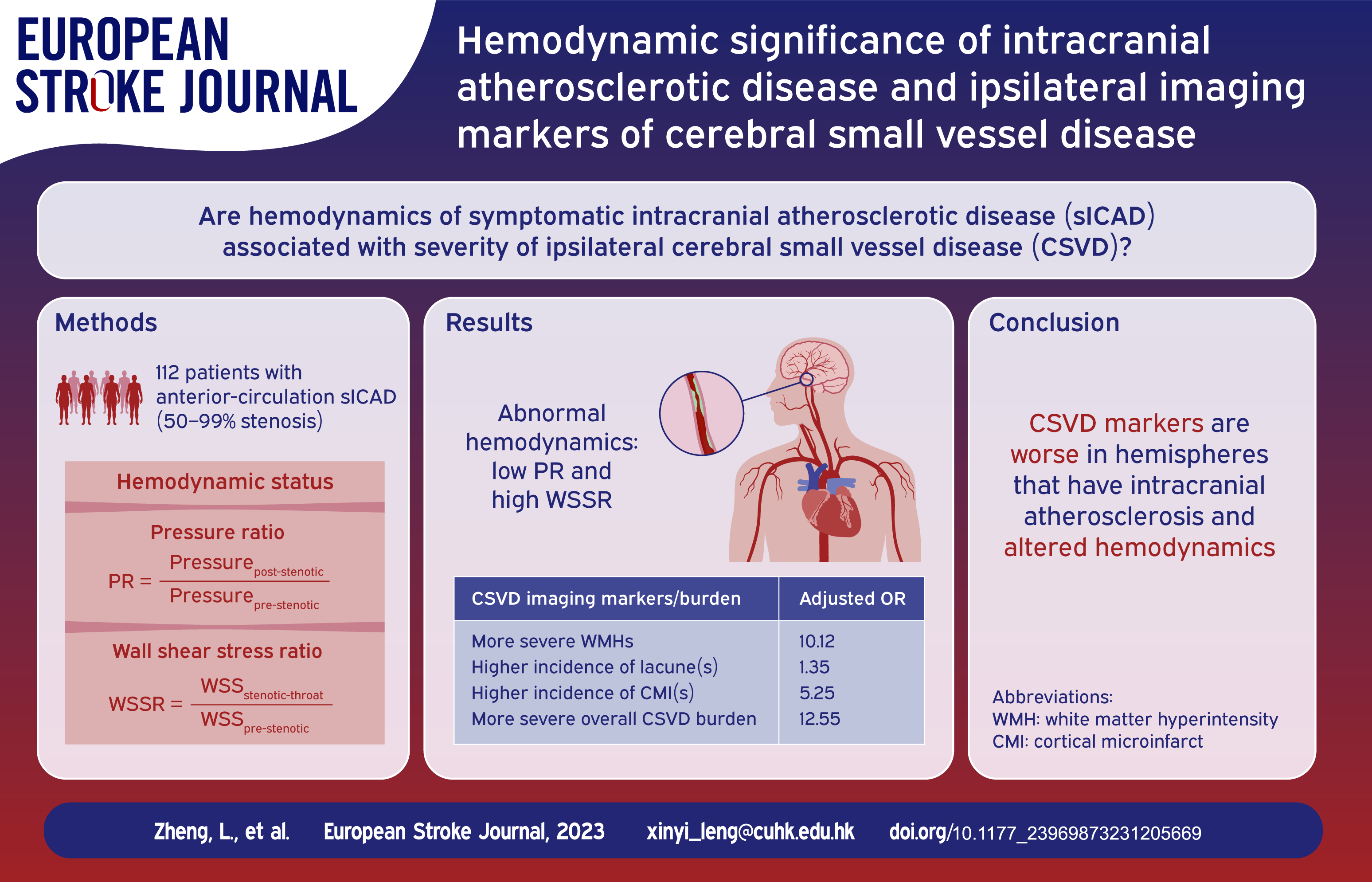
Cerebral small vessel disease (CSVD) commonly exists in patients with symptomatic intracranial atherosclerotic disease (sICAD). We aimed to investigate the associations of hemodynamic features of sICAD lesions with imaging markers and overall burden of CSVD.
Patients with anterior-circulation sICAD (50%–99% stenosis) were analyzed in this cross-sectional study. Hemodynamic features of a sICAD lesion were quantified by translesional pressure ratio (PR = Pressurepost-stenotic/Pressurepre-stenotic) and wall shear stress ratio (WSSR = WSSstenotic-throat/WSSpre-stenotic) via CT angiography-based computational fluid dynamics modeling. PR ⩽median was defined as low (“abnormal”) PR, and WSSR ⩾ fourth quartile as high (“abnormal”) WSSR. For primary analyses, white matter hyperintensities (WMHs), lacunes, and cortical microinfarcts (CMIs) were assessed in MRI and summed up as overall CSVD burden, respectively in ipsilateral and contralateral hemispheres to sICAD. Enlarged perivascular spaces (EPVSs) and cerebral microbleeds (CMBs) were assessed for secondary analyses.
Among 112 sICAD patients, there were more severe WMHs, more lacunes and CMIs, and more severe overall CSVD burden ipsilaterally than contralaterally (all
There are more severe WMHs and CMI(s) in the hemisphere ipsilateral than contralateral to sICAD. The hemodynamic significance of sICAD lesions was independently associated with severities of WMHs and CMI(s) ipsilaterally.
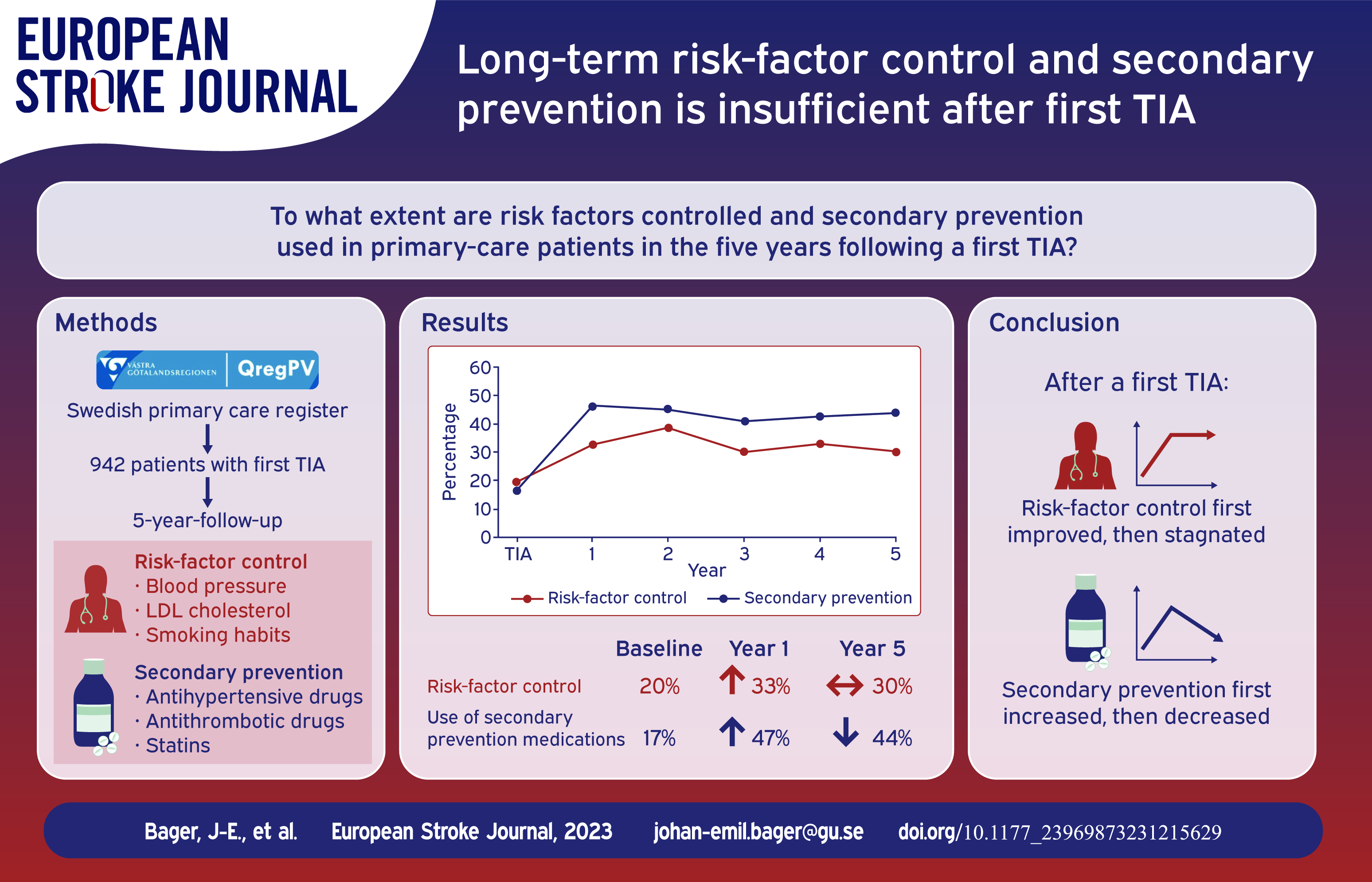
Long-term risk-factor control and secondary prevention are not well characterized in patients with a first transient ischemic attack (TIA). With baseline levels as reference, we compared primary-care data on blood pressure (BP), low-density lipoprotein cholesterol (LDL-C), smoking, and use of antihypertensives, statins and antiplatelet treatment/oral anticoagulation (APT/OAC) during 5 years after a first TIA.
Patients in QregPV, a Swedish primary-care register for the Region of Västra Götaland, with a first TIA discharge diagnosis from wards proficient in stroke care 2010 to 2012 were identified and followed up to 5 years. BP, LDL-C, smoking, use of antihypertensives, statins, APT/OAC, and achievement of target levels were calculated. We used logistic mixed-effect models to analyze the effect of follow-up over time on risk-factor control and secondary prevention treatment.
We identified 942 patients without prior cerebrovascular disease who had a first TIA. Compared to baseline, the first year of follow-up was associated with improvements in concomitant attainment of BP <140/90 mmHg, LDL-C < 2.6 mmol/L and non-smoking, which rose from 20% to 33% (OR 2.08, 95% CI 1.38–3.13), but then stagnated in years 2–5. In the first year of follow-up, 47% of patients had complete secondary prevention treatment (antihypertensives, APT/OAC and statin), but continued follow-up was associated with a yearly decrease in secondary prevention treatment (OR 0.94, 95% CI 0.94–0.98).
Risk-factor control was inadequate, leaving considerable potential for improved secondary prevention treatment after a first TIA in Swedish patients followed up to 5 years.
Early neurological deterioration (END) is associated with poor outcomes in patients with acute ischemic stroke due to large vessel occlusion (AIS-LVO). Causes of END after mechanical thrombectomy (MT) include unsuccessful recanalization and reperfusion hemorrhages. However, little is known about END excluding the aforementioned causes. We aimed to investigate factors associated with unexplained END (ENDunexplained) with regard to the cerebral collateral status.
Multicenter retrospective study of AIS-LVO patients with successful MT (mTICI 2b-3). On admission CT angiography (CTA), pial arterial collaterals and venous outflow (VO) were assessed using the modified Tan-Scale and the Cortical Vein Opacification Score (COVES), respectively. ENDunexplained was defined as an increase in NIHSS score of ⩾ 4 within the first 24 hours after MT without parenchymal hemorrhage on follow-up imaging. Multivariable regression analyses were performed to examine factors of ENDunexplained and unfavorable functional outcome (modified Rankin Scale score 3-6).
A total of 620 patients met the inclusion criteria. ENDunexplained occurred in 10% of patients. While there was no significant difference in pial arterial collaterals, patients with ENDunexplained exhibited more often unfavorable VO (81% vs. 53%;
Unfavorable VO on admission CTA was associated with ENDunexplained. ENDunexplained was independently linked to unfavorable functional outcomes at 90 days. Identifying AIS-LVO patients at risk of ENDunexplained may help to select patients for intensified monitoring and guide to optimal treatment regimes.

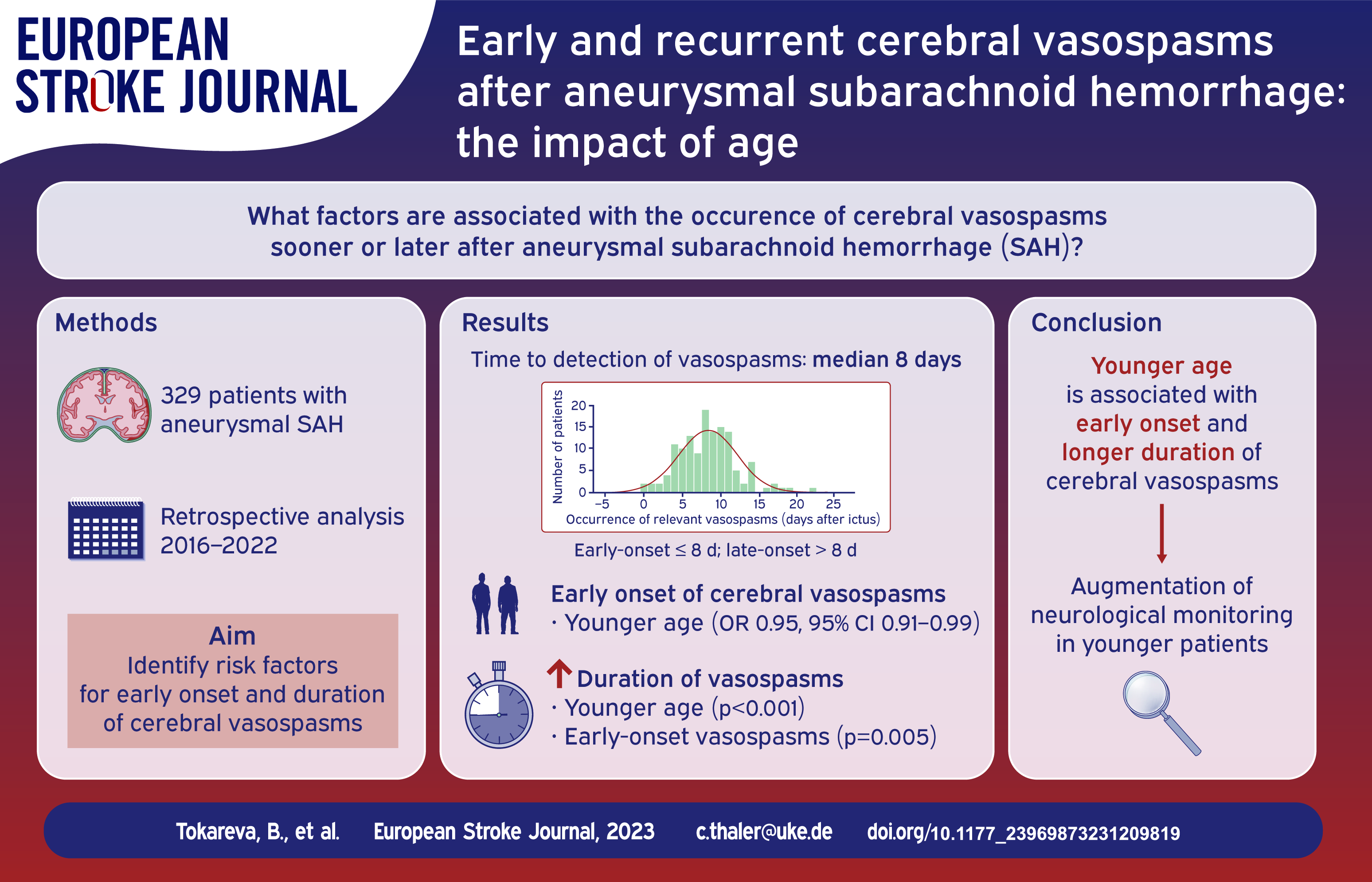
Cerebral vasospasms remain a strong predictor of poor outcome after aneurysmal SAH. The aim of this study was to describe the time course of relevant vasospasms after aneurysmal SAH and to determine the variables associated with early-onset or prolonged and recurrent vasospasms.
We conducted a retrospective, single-center study of consecutive adult patients with aneurysmal SAH admitted between 2016 and 2022 at our tertiary stroke center. Relevant vasospasms, defined as vessel narrowing detected in DSA in combination with clinical deterioration or new perfusion deficit, were detected according to our in-house algorithm and eventually treated endovascularly. The primary endpoint was the diagnosis of relevant vasospasms. As secondary endpoints, the time from hemorrhage to the onset of vasospasms and the time from the first to the last endovascular intervention were measured.
Of 368 patients with aneurysmal SAH, 135 (41.0%) developed relevant vasospasms. The median time between ictus and detection of vasospasms was 8 days (IQR: 6–10). Patients with early-onset vasospasms were significantly younger (mean 52.7 ± 11.2 years vs 58.7 ± 11.5 years,
Younger age was associated with early-onset and longer duration of relevant vasospasms in this study. More frequent clinical and diagnostic follow-up should be considered in this subgroup of patients that are at risk for poor outcomes.
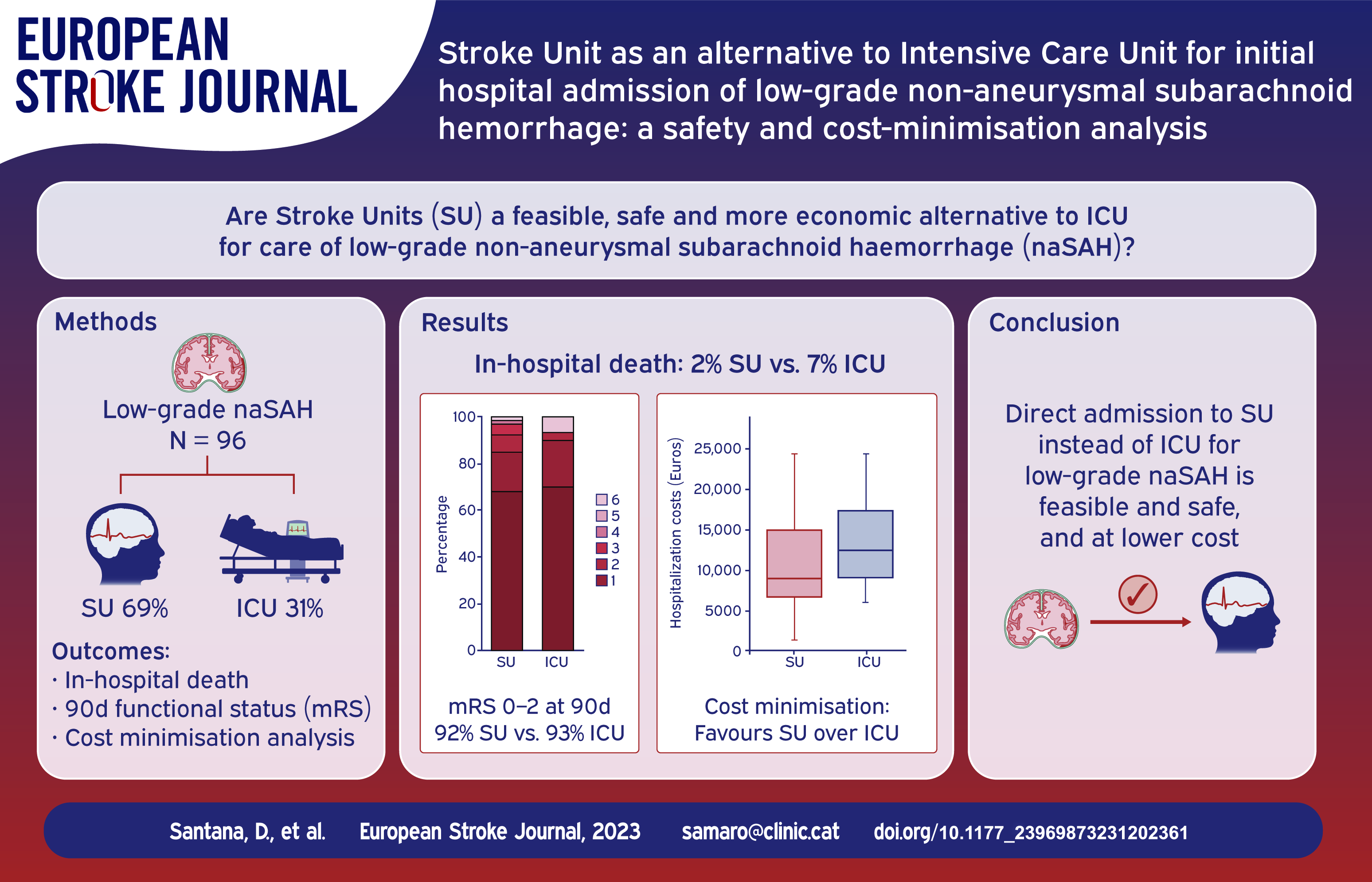
Stroke Units (SU) have been suggested as an alternative to Intensive Care units (ICU) for initial admission of low-grade non-aneurysmal spontaneous subarachnoid haemorrhage (naSAH). We hypothesised that the incidence of in-hospital complications and long-term clinical outcomes in low-grade naSAH patients would be comparable in both settings, and that a cost-minimisation analysis would favour the use of SU.
Retrospective, single-centre study at a third-level stroke-referral hospital, including low-grade spontaneous naSAH patients with WFNS 1–2. Primary outcomes were death and functional status at 3 months. Secondary outcomes were incidence of in-hospital major neurological and systemic complications. Additionally, a cost-minimisation analysis was conducted to estimate the average cost savings that could be achieved with the most efficient approach.
Out of 96 naSAH patients, 30 (31%) were initially admitted to ICU and 66 (69%) to SU. Both groups had similar demographic and radiological features except for a higher proportion of WFNS 2 in ICU subgroup. There were no statistically significant differences between ICU and SU-managed subgroups in death rate (2 (7%) and 1 (2%), respectively), functional outcome at 90 days (28 (93%) and 61 (92%) modified Rankin Scale 0–2) or neurological and systemic in-hospital complications. Cost-minimisation analysis demonstrated significant monetary savings favouring the SU strategy.
Initial admission to the SU appears to be a safe and cost-effective alternative to the ICU for low-grade naSAH patients, with comparable clinical outcomes and a reduction of hospitalisation-related costs. Prospective multicenter randomised studies are encouraged to further evaluate this approach.
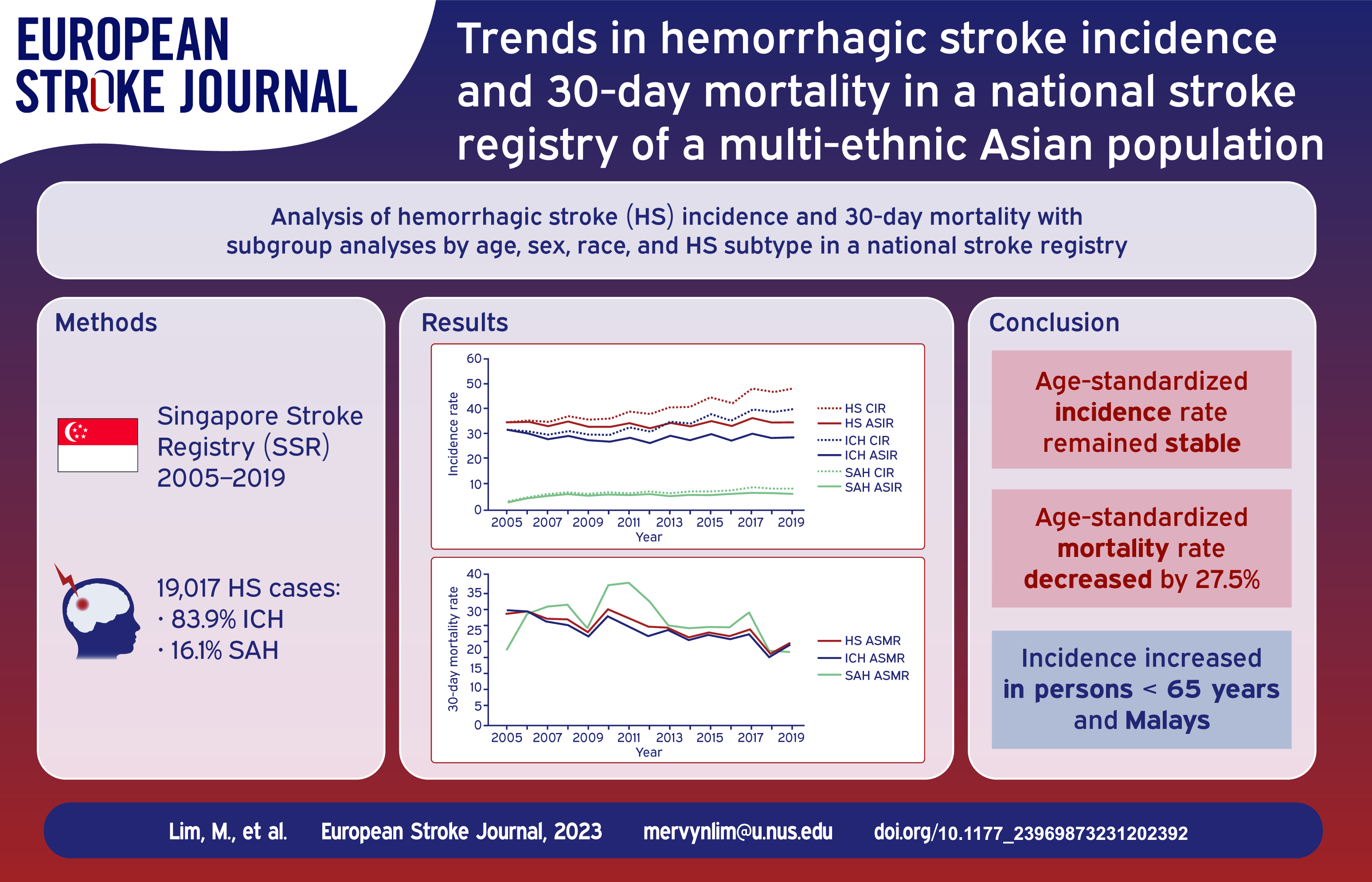
High-quality epidemiological data on hemorrhagic stroke (HS) and its subtypes, intracerebral hemorrhage (ICH) and subarachnoid hemorrhage (SAH), remains limited in Asian ethnicities. We investigated the trends in HS incidence and 30-day mortality from 2005 to 2019 in a multi-ethnic Asian population from a national registry.
Data on all stroke cases from the Singapore Stroke Registry from 2005 to 2019 were collected. Cases were defined using centrally adjudicated review of diagnosis codes. Death outcomes were obtained by linkage with the national death registry. Incidence (per 100,000 people) and 30-day mortality (per 100 people) were measured as crude and age-standardized rates. Trends were analyzed using linear regression.
We analyzed 19,017 cases of HS (83.9% ICH; 16.1% SAH). From 2005 to 2019, age-standardized incidence rates (ASIR) for HS remained stable from 34.4 to 34.5. However, age-standardized mortality rates (ASMR) decreased significantly from 29.5 to 21.4 (
From 2005 to 2019, ASIR of HS remained stable while ASMR decreased. Decreasing ASMR reflects improvements in the overall management of HS, consistent with global trends.
Population health efforts to address modifiable risk factors for HS in specific demographic subgroups may be warranted to reduce incidence and mortality of HS.
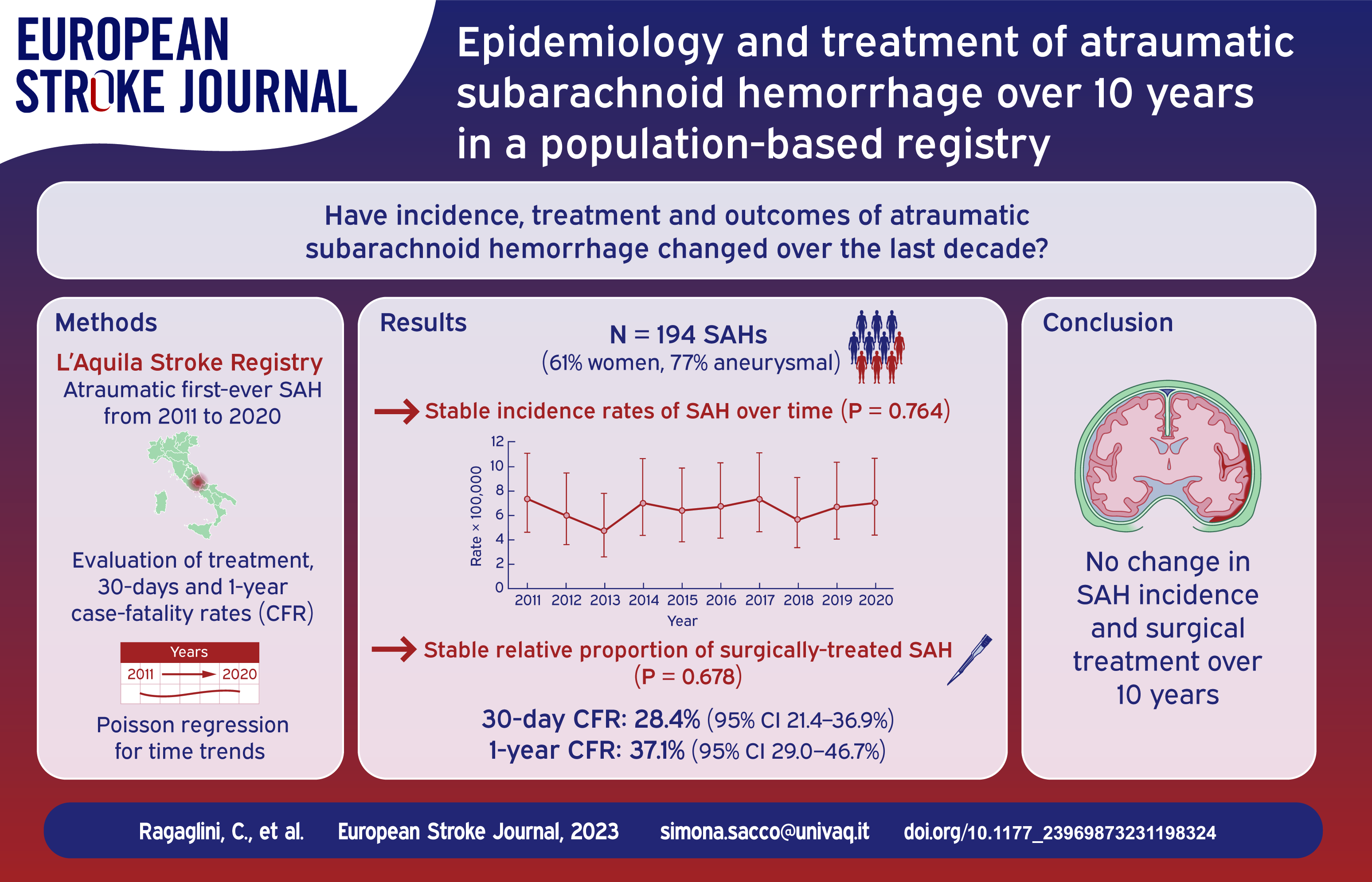
Incidence of atraumatic subarachnoid hemorrhage (SAH) is decreasing over time and its treatment is changing. We reported epidemiologic data on aneurysmal (a-) and non-aneurysmal (na-) SAH over 10 years.
Our prospective population-based registry included patients with first-ever SAH occurring from January 2011 to December 2020. Clinical and neuroimaging records were screened to evaluate the presence and location of intracranial aneurysms, to identify naSAH subtypes and to retrieve information on surgical treatments. Incidence rates were standardized to the 2011 Italian and European population. We also estimated 30-day and 1-year case-fatality rates after SAH. Multivariate hazard ratios for 30-days and 1-year fatality were estimated with Cox regression analysis.
194 patients (60.8% women; mean age 62.5 ± 16.0 years) were included (76.8% aSAH and 23.2% naSAH). The crude incidence rates per 100,000 person-years of SAH, aSAH, and naSAH were 6.5 (95% CI 5.6–7.5), 5.0 (95% CI 4.2–5.9), and 1.5 (95% CI 1.1–2.0), respectively, and remained stable over time. Compared to aSAH, naSAH patients had higher age (68.8 ± 19.7 yearsvs 60.6 ± 14.2 years;
We found a low and stable incidence of SAH over the 2011–2020 period. naSAH remained rare and deserves further investigation in larger prospective cohorts.
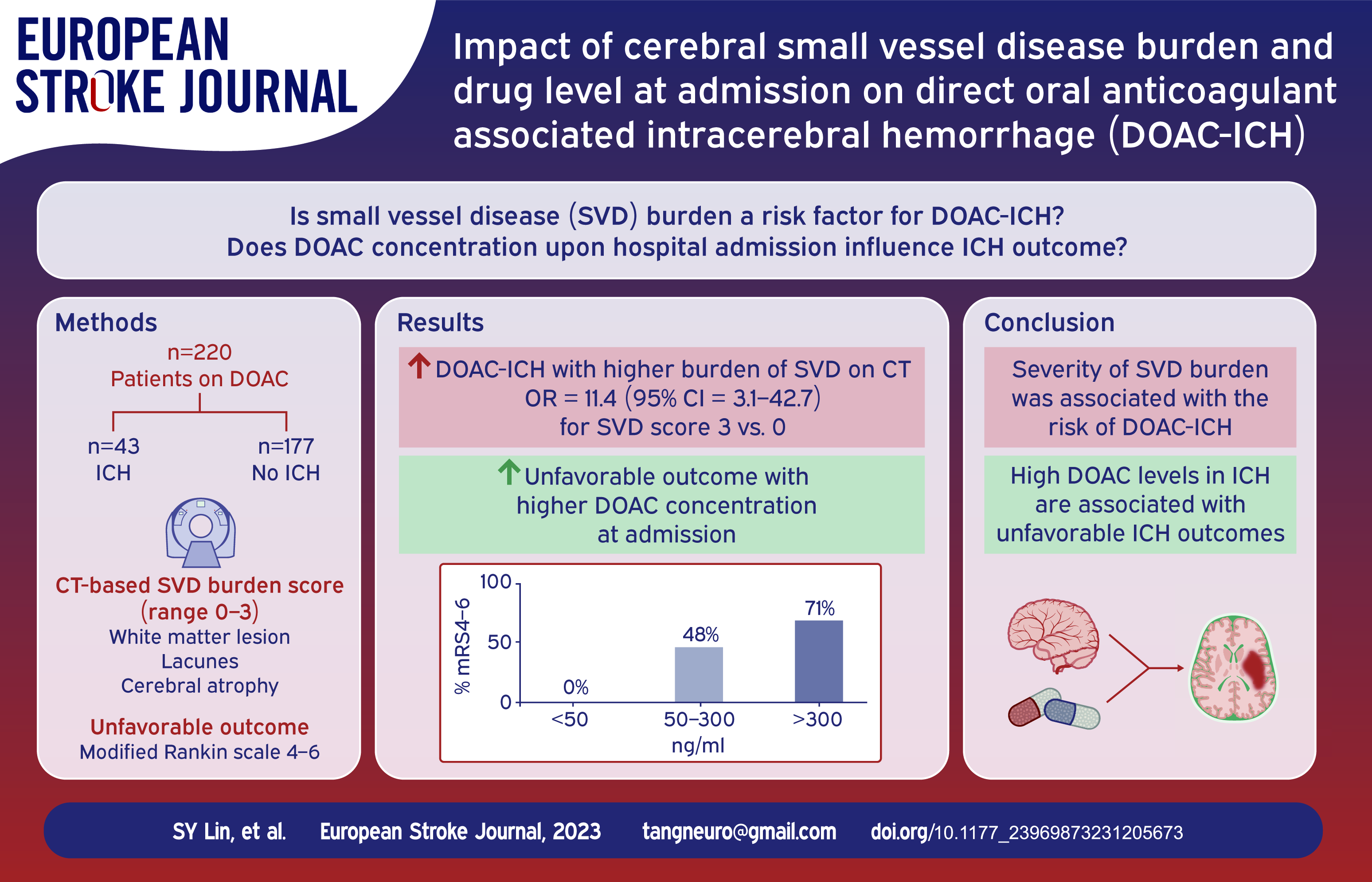
Direct oral anticoagulant (DOAC)-associated intracerebral hemorrhage (ICH) is a catastrophic complication. The aim of this study was to investigate the association between computed tomography (CT)-based cerebrovascular small vessel disease (SVD) burden and DOAC-ICH as well as the DOAC concentration upon hospital admission and ICH outcome.
The study included two cohorts: (1) DOAC-ICH: patients who suffered from DOAC-ICH and underwent drug level measurements upon admission; (2) DOAC-non-ICH: stable DOAC users who underwent head CT without ICH during treatment. We categorized the DOAC levels of the DOAC-ICH patients as low (<50 ng/mL), medium (50–300 ng/mL), and high (>300 ng/mL). The CT-based SVD burden (including white matter lesions [WML], lacunes, and cerebral atrophy) was evaluated, and SVD scores (range, 0–3) were used to evaluate SVD severity.
A total of 43 DOAC-ICH patients and 177 DOAC-non-ICH patients were enrolled. DOAC-ICH patients were more likely to have WML, lacunes, or cerebral atrophy compared to DOAC-non-ICH patients. After adjustment, the SVD burden was associated with DOAC-ICH, with a higher risk of more severe SVD (SVD score of 2; odds ratio [OR], 10.3 [3.17, 33.3]; score of 3; OR, 16.8 [4.50, 62.6]). The proportions of patients with high, medium, and low drug levels in the DOAC-ICH group were 16.3%, 55.8%, and 27.9%, respectively. Additionally, the high-level group displayed a larger hematoma size and had worse functional outcomes at 3 months than the other two groups.
The severity of SVD burden was associated with DOAC-ICH. Furthermore, high DOAC levels in ICH were associated with unfavorable clinical outcomes. To address the potential selection bias from these two cohorts, a prospective study to investigate the co-contribution of drug levels and SVD to DOAC-ICH is essential.
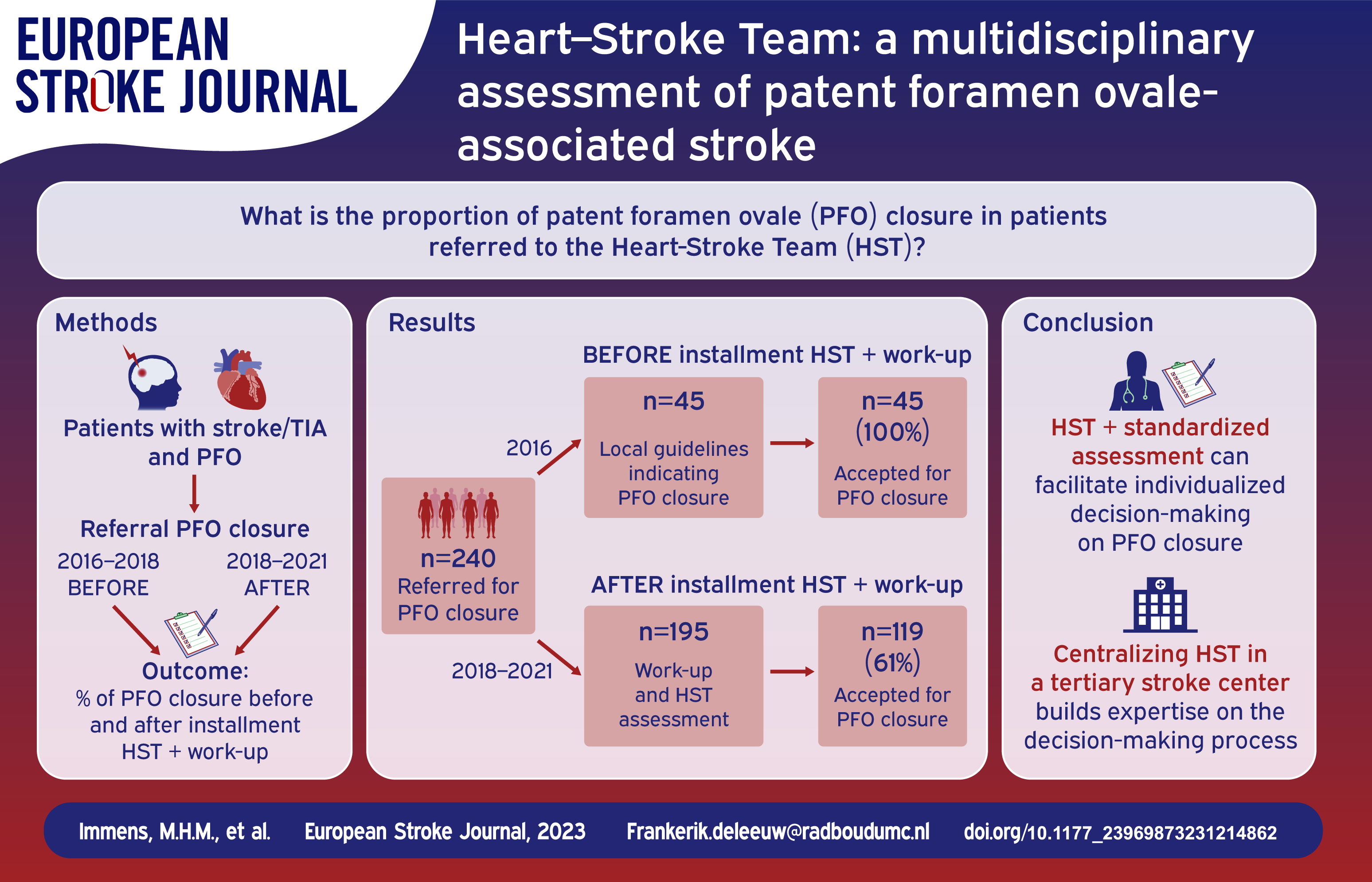
Patent foramen ovale (PFO) closure prevents recurrent ischemic stroke in selected patients with a cryptogenic stroke. Trial results tend to be generalized to daily practice, often extending original trial inclusion criteria. This may result in unnecessary closure without benefit, but with risk of complications. We therefore introduced a standardized and structured evaluation by an interdisciplinary Heart-Stroke Team (HST). Our aim was to investigate the proportion of actual PFO closure of all referred patients with a cryptogenic stroke, after evaluation by the HST.
We conducted a single-center, retrospective cohort study. Patients with an assumed cryptogenic ischemic stroke or transient ischemic attack (TIA) and a PFO who were referred for PFO closure were analyzed. As part of the HST approach, all patients underwent a standardized work-up, first to demonstrate the ischemic event on neuroimaging, second to evaluate all potential causes of stroke and finally, to assess the possible relation between the PFO and stroke. Outcome was the proportion of patients treated with PFO closure after referral.
A total of 195 patients were included. In 124 patients (64%) PFO closure was advised. Fourty-two (22%) patients had a clear alternative cause of stroke and in 13 (7%) patients the initial stroke diagnosis could not be confirmed.
After careful analysis of patients referred for PFO closure a relationship between the PFO and stroke could not be demonstrated in 32% of referrals, and 3% preferred best medical treatment over percutaneous closure. This stresses the need for a complete neurovascular work-up and multidisciplinary assessment.
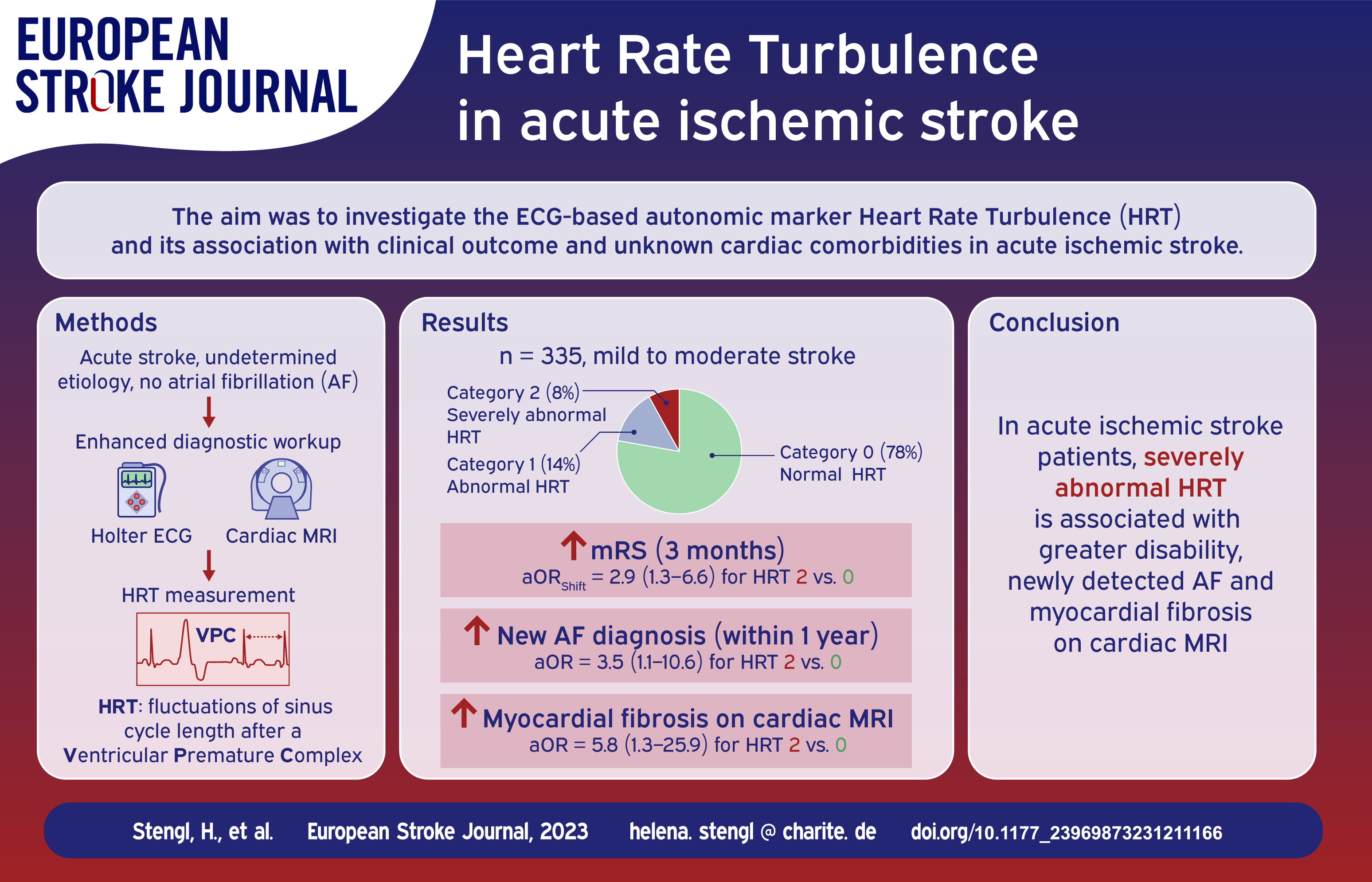
Heart rate turbulence (HRT), an ECG-based marker of autonomic cardiac regulation, has shown high prognostic value in patients with established cardiovascular diseases, while data in patients with acute ischemic stroke are scarce.
The HRT parameters turbulence onset and turbulence slope were analyzed using Holter-ECG recordings from patients with acute ischemic stroke, consecutively enrolled in the prospective observational HEBRAS study. HRT was categorized as normal (category 0; both parameters normal), abnormal (category 1; one parameter abnormal), or severely abnormal (category 2; both parameters abnormal). Outcomes of interest were functional outcome according to modified Rankin Scale (mRS) score at 3 months, mortality at 1 year, newly detected atrial fibrillation (AF), and evidence of focal myocardial fibrosis on cardiovascular MRI.
HRT was assessed in 335 patients in sinus rhythm (median age 69 years, 37% female, median NIHSS score 2 on admission), including 262 (78%) with normal HRT, 47 (14%) with abnormal and 26 (8%) with severely abnormal HRT. Compared with normal HRT, severely abnormal HRT was associated with increased disability [higher mRS] at 3 months (adjusted odds ratio [aOR]: 2.9, 95% confidence interval [CI]: 1.3–6.6), new AF (aOR: 3.5, 95% CI: 1.1–10.6), MRI-detected myocardial fibrosis (aOR: 5.8, 95% CI: 1.3–25.9), but not with mortality at 1 year after stroke (aOR: 3.0, 95% CI: 0.7–13.9). Abnormal HRT was not associated with the analyzed outcomes.
Severely abnormal HRT was associated with increased disability and previously unknown cardiac comorbidities. The potential role of HRT in selecting patients for extended AF monitoring and cardiac imaging should be further investigated.
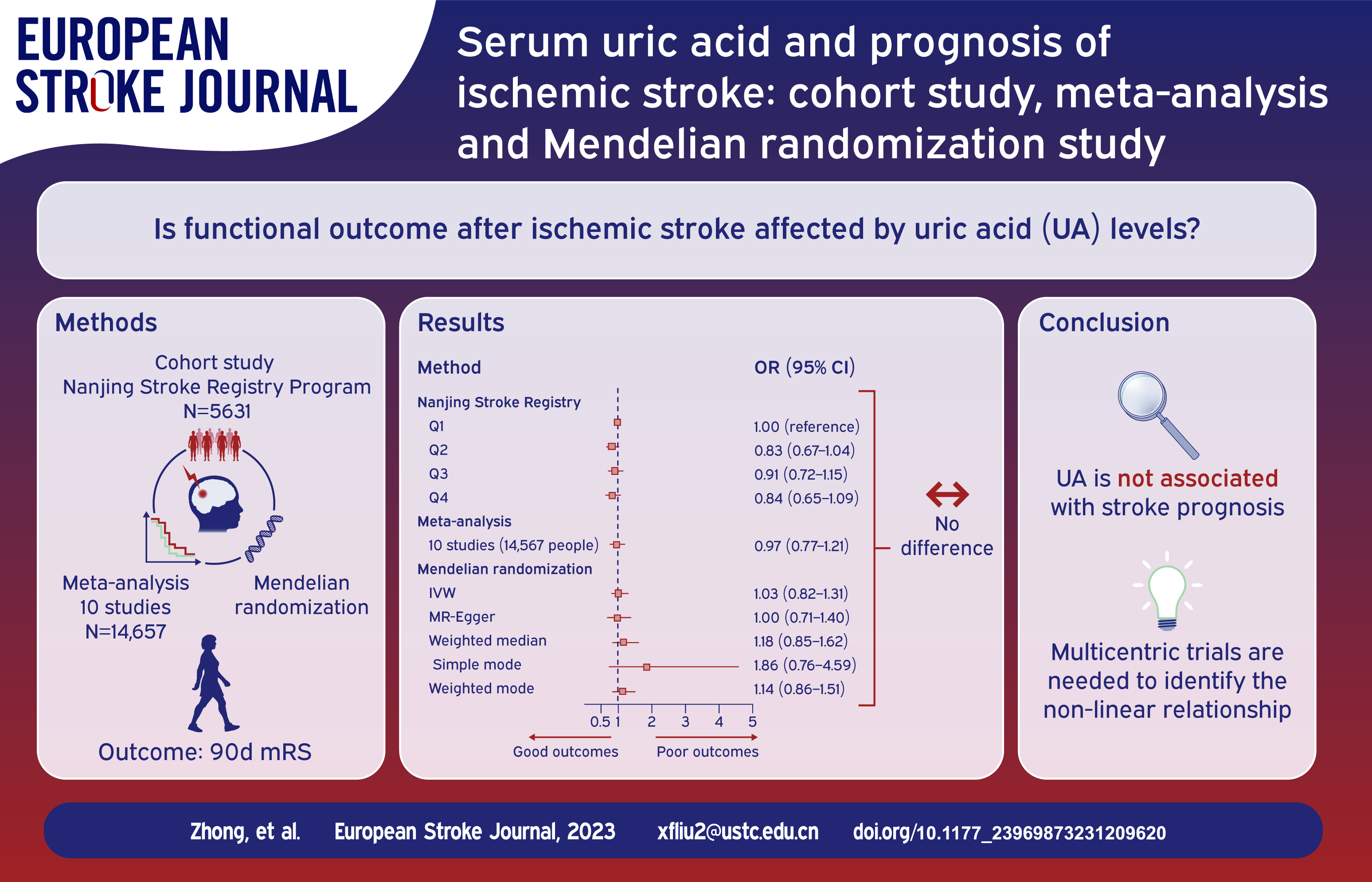
The role of serum uric acid (UA) levels in the functional recovery of ischemic stroke remains uncertain. To evaluate whether UA could predict clinical outcomes in patients with ischemic stroke.
A three-stage study design was employed, combining a large-scale prospective cohort study, a meta-analysis and a Mendelian randomization (MR) analysis. Firstly, we conducted a cohort study using data from the Nanjing Stroke Registry Program (NSRP) to assess the association between UA levels and 3-month functional outcomes in ischemic stroke patients. Secondly, the meta-analysis was conducted to integrate currently available cohort evidence. Lastly, MR analysis was utilized to explore whether genetically determined UA had a causal link to the functional outcomes of ischemic stroke using summary data from the CKDGen and GISCOME datasets.
In the first stage, the cohort study included 5631 patients and found no significant association between UA levels and functional outcomes at 3 months after ischemic stroke. In the second stage, the meta-analysis, including 10 studies with 14,657 patients, also showed no significant association between UA levels and stroke prognosis. Finally, in the third stage, MR analysis using data from 6165 patients in the GISCOME study revealed no evidence of a causal relationship between genetically determined UA and stroke functional outcomes.
Our comprehensive triangulation approach found no significant association between UA levels and functional outcomes at 3 months after ischemic stroke.
Observational studies suggest that different classes of antihypertensive drugs may have different effects on the occurrence of intracranial aneurysms (IA) and subarachnoid hemorrhage (SAH). However, the reported results in previous studies are inconsistent, and randomized data are absent. We performed a two-sample Mendelian randomization (MR) analysis to study the causal effects of genetically determined blood pressure (BP) and genetic proxies for antihypertensive drug classes on the risk of IA and SAH.
Genetic instruments and outcome data were obtained from independent genome-wide association studies (GWAS) or published data, which were exclusively restricted to European ancestry. Causal relationships were identified using inverse-variance weighted MR analyses and a series of statistical sensitivity analyses. The FinnGen consortium was used for repeated analysis to verify results obtained from the above GWAS.
Two-sample MR analysis showed that genetically determined Systolic BP, Dystolic BP, and Pulse Pressure were related to a higher risk of IA and SAH. Based on identified single nucleotide polymorphisms (SNPs) that influence the effect of calcium channel blockers (CCB, 42 SNPs), beta-blockers (BB, 8 SNPs), angiotensin-converting enzyme inhibitors (ACEI, 2 SNPs), angiotensin receptor blockers (ARB, 1 SNPs), and thiazides (5 SNPs), genetically determined effect of CCBs was associated with a higher risk of IA (OR, 1.07 [95% CI, 1.03–1.10],
This MR analysis supports the role of elevated blood pressure in the occurrence of intracranial aneurysms and subarachnoid hemorrhage. However, genetic proxies for calcium channel blockers were associated with an increased risk of intracranial aneurysms and subarachnoid hemorrhage. Further studies are required to confirm these findings and investigate the underlying mechanisms.
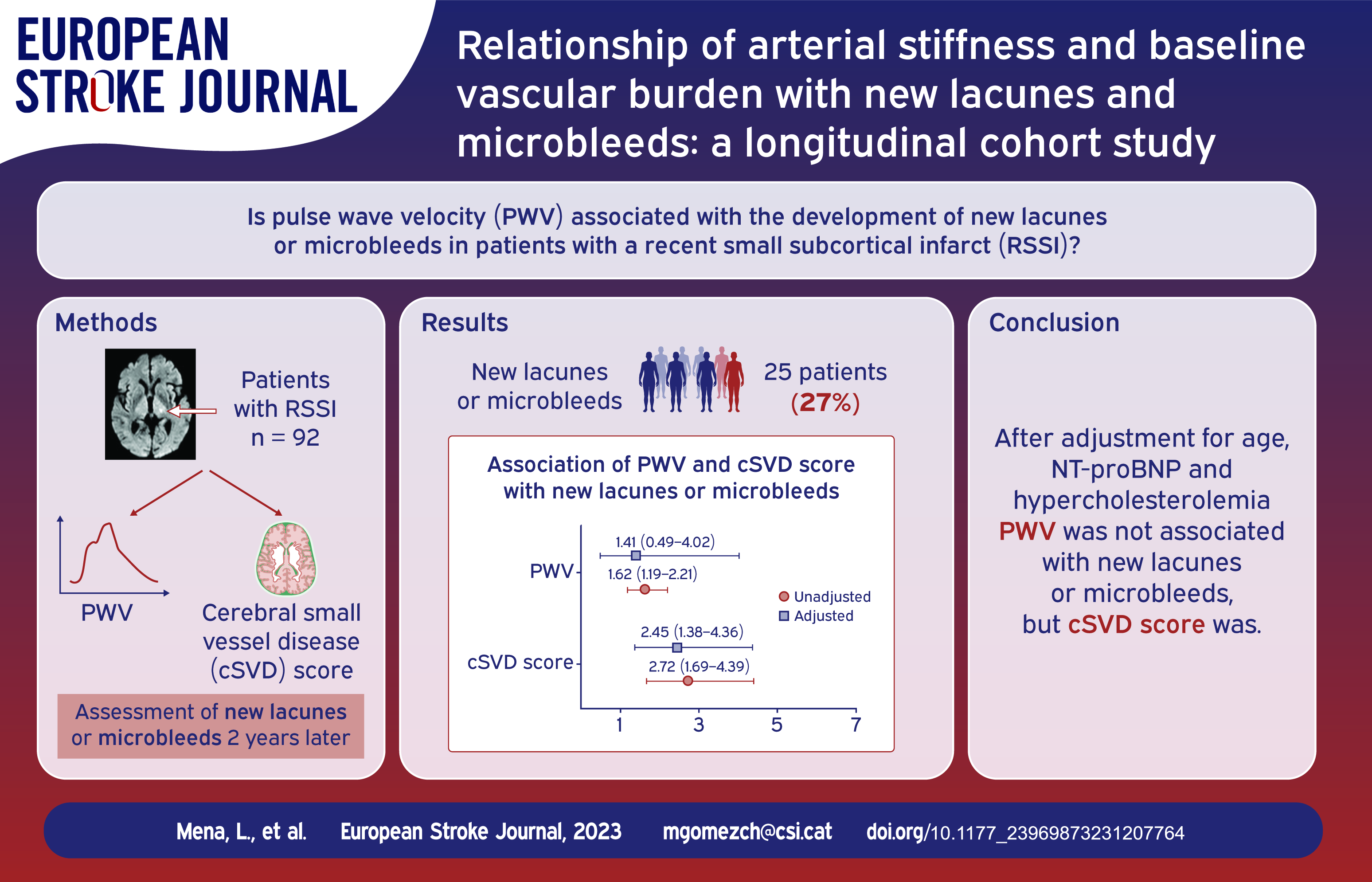
Arterial stiffness may have a significant impact on the development of cerebral small vessel disease (cSVD).
We obtained pulse wave velocity (24-h PWV) by means of ambulatory blood pressure monitoring (ABPM) in patients with a recent small subcortical infarct (RSSI). Patients with known cardiac or arterial embolic sources were excluded. Lacunes, microbleeds, white matter hyperintensities and enlarged perivascular spaces at baseline were assessed in a brain MRI and included in a cSVD score. A follow-up MRI was obtained 2 years later and assessed for the appearance of new lacunes or microbleeds. We constructed both unadjusted and adjusted models, and subsequently selected the optimal models based on the area under the curve (AUC) of the predicted probabilities.
Ninety-two patients (mean age 67.04 years, 69.6% men) were evaluated and 25 had new lacunes or microbleeds during follow-up. There was a strong correlation between 24-h PWV and age (
cSVD score is a stronger predictor for cSVD progression than age or hemodynamic parameters in patients with a RSSI.
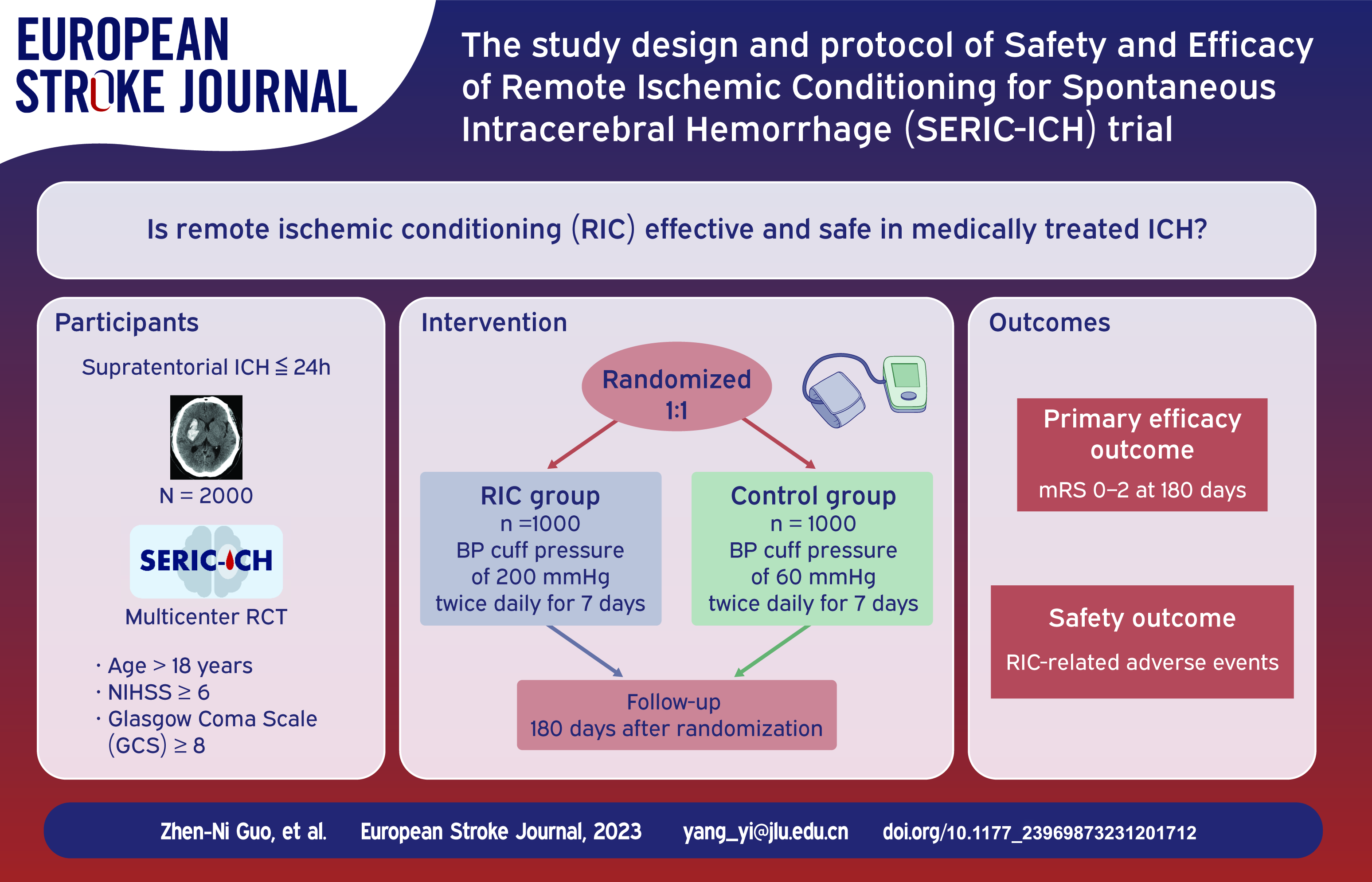
Previous studies have revealed that remote ischemic conditioning (RIC) may have a neuroprotective function. However, the potential benefit of RIC for patients with ICH remain unclear.
The primary aim of this study is to assess the safety and efficacy of RIC for patients with ICH.
The Safety and Efficacy of RIC for Spontaneous ICH (SERIC-ICH) is an ongoing prospective, randomized, multicenter, parallel-controlled, and blinded-endpoint clinical trial. The study will enroll an estimated 2000 patients aged ⩾18 years within 24 h after ICH onset, with National Institutes of Health Stroke Scale ⩾6 and Glasgow Coma Scale ⩾8 upon presentation. The patients will be randomly assigned to the RIC or control groups (1:1) and will be treated with cuffs inflated to a pressure of 200 or 60 mmHg, respectively, twice daily for 7 days. Each RIC treatment will consist of four cycles of arm ischemia for 5 min, followed by reperfusion for another 5 min, for a total procedure time of 35 min. The primary efficacy outcome measure is the proportion of patients with good functional outcomes (modified Rankin scale 0–2) at 180 days. The safety outcome measures will include all adverse events and severe adverse events occurring in the course of the study.
RIC is an inexpensive intervention and might be a strategy to improve outcomes in patients with ICH. The SERIC-ICH trial will investigate whether RIC treatment can be applied as an adjuvant treatment in the acute phase of ICH and identify safety issues.
Inflammation plays a vital role in the development of secondary brain injury after spontaneous intracerebral haemorrhage (ICH). Interleukin-1 beta is an early pro-inflammatory cytokine and a potential therapeutic target.
To determine the effect of treatment with recombinant human interleukin-1 receptor antagonist anakinra on perihematomal oedema (PHO) formation in patients with spontaneous ICH compared to standard medical management, and investigate whether this effect is dose-dependent.
ACTION is a phase-II, prospective, randomised, three-armed (1:1:1) trial with open-label treatment and blinded end-point assessment (PROBE) at three hospitals in The Netherlands. We will include 75 patients with a supratentorial spontaneous ICH admitted within 8 h after symptom onset. Participants will receive anakinra in a high dose (loading dose 500 mg intravenously, followed by infusion with 2 mg/kg/h over 72 h;
Primary outcome is PHO, measured as oedema extension distance on MRI at day 7 ± 1. Secondary outcomes include the safety profile of anakinra, the effect of anakinra on serum inflammation markers, MRI measures of blood brain barrier integrity, and functional outcome at 90 ± 7 days.
The ACTION trial will provide insight into whether targeting interleukin-1 beta in the early time window after ICH onset could ameliorate secondary brain injury. This may contribute to the development of new treatment options to improve clinical outcome after ICH.


