Editorial
Select search scope: search across all journals or within the current journal
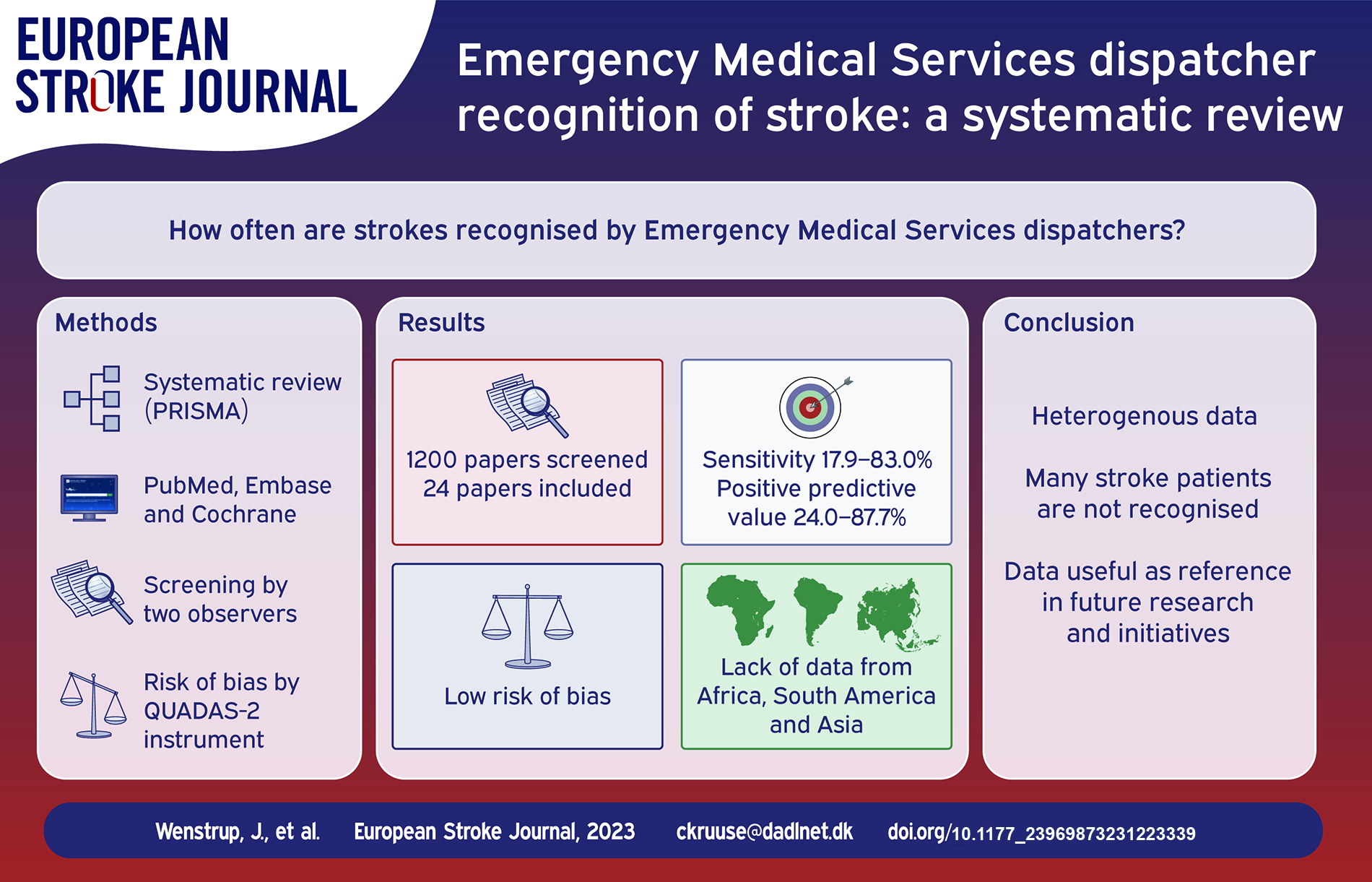
Stroke treatments are time-sensitive, and thus early and correct recognition of stroke by Emergency Medical Services is essential for outcomes. This is particularly important with the adaption of mobile stroke units. In this systematic review, we therefore aimed to provide a comprehensive overview of Emergency Medical Services dispatcher recognition of stroke.
The review was registered on PROSPERO and the PRISMA guidelines were applied. We searched PubMed, Embase, and Cochrane Review Library. Screening and data extraction were performed by two observers. Risk of bias was assessed using the QUADAS-2 instrument.
Of 1200 papers screened, 24 fulfilled the inclusion criteria. Data on sensitivity was reported in 22 papers and varied from 17.9% to 83.0%. Positive predictive values were reported in 12 papers and ranged from 24.0% to 87.7%. Seven papers reported specificity, which ranged from 20.0% to 99.1%. Six papers reported negative predictive value, ranging from 28.0% to 99.4%. In general, the risk of bias was low.
Stroke recognition by dispatchers varied greatly, but overall many patients with stroke are not recognised, despite the initiatives taken to improve stroke literacy. The available data are of high quality, however Asian, African, and South American populations are underrepresented.
While the data are heterogenous, this review can serve as a reference for future research in emergency medical dispatcher stroke recognition and initiatives to improve prehospital stroke recognition.
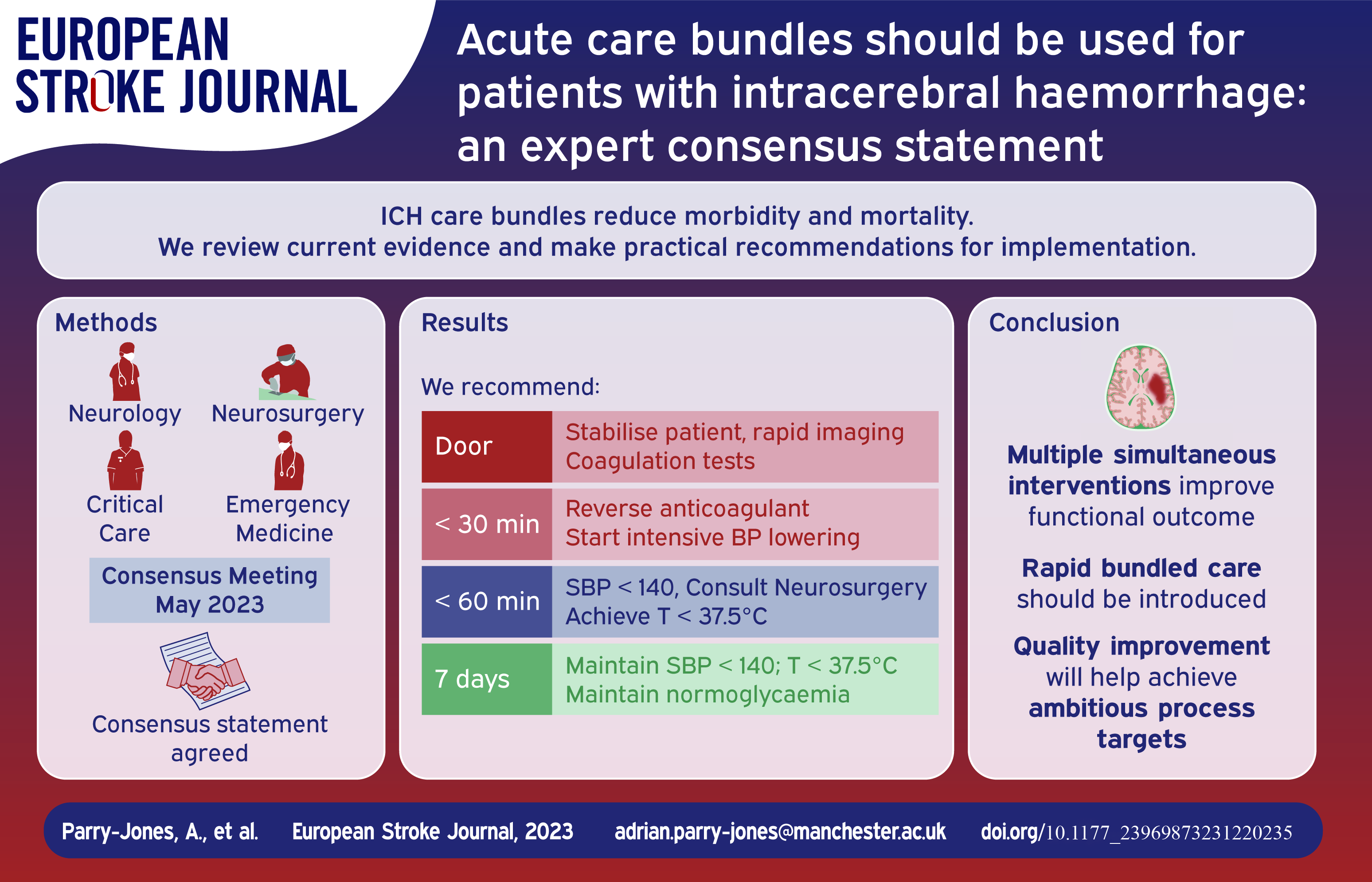
Intracerebral haemorrhage (ICH) is the most devastating form of stroke and a major cause of disability. Clinical trials of individual therapies have failed to definitively establish a specific beneficial treatment. However, clinical trials of introducing care bundles, with multiple therapies provided in parallel, appear to clearly reduce morbidity and mortality. Currently, not enough patients receive these interventions in the acute phase.
We convened an expert group to discuss best practices in ICH and to develop recommendations for bundled care that can be delivered in all settings that treat acute ICH, with a focus on European healthcare systems.
In this consensus paper, we argue for widespread implementation of formalised care bundles in ICH, including specific metrics for time to treatment and criteria for the consideration of neurosurgical therapy.
There is an extraordinary opportunity to improve clinical care and clinical outcomes in this devastating disease. Substantial evidence already exists for a range of therapies that can and should be implemented now.
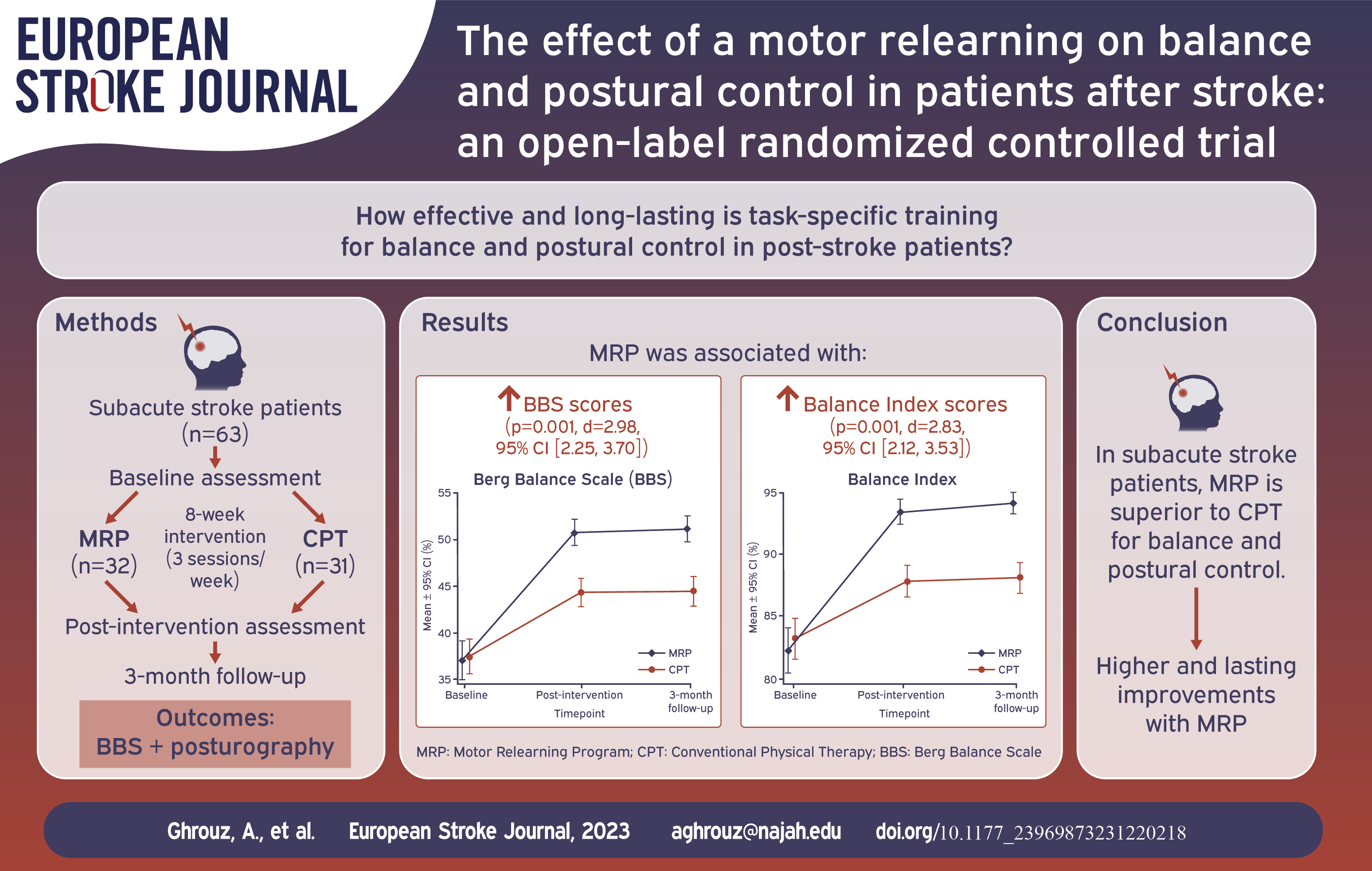
Balance and postural control impairments are common in stroke patients, increasing fall risk and limiting their daily and social activities. Current research lacks comprehensive studies evaluating the efficacy and long-term effects of task-specific training on balance and postural control among stroke patients, especially when considering biomechanical and posturographic assessments.
A randomized controlled trial included 63 subacute stroke patients recruited from the outpatient rehabilitation department. Participants were randomly assigned to the MRP group (n=32), receiving task-specific training based on MRP, or the CPT group (n=31), receiving conventional physical therapy. Both groups completed an 8-week intervention (3 sessions/week; 1 h./session). Balance and postural control were assessed at baseline, post-intervention, and 3-month follow-up using the Berg Balance Scale (BBS) and posturography.
The MRP group exhibited significantly larger improvements than the CPT group in both BBS scores (p=0.001, d=2.98, 95% CI [2.25, 3.70]) and Balance Index scores (p=0.001, d=2.83, 95% CI [2.12, 3.53]) after the intervention. These improvements were sustained at 3-month follow-up.
The findings suggest that task-specific training based on MRP is more effective than CPT for improving balance and postural control. The MRP intervention may enhance the motor learning and neural plasticity of the patients, leading to better functional outcomes. However, the study’s open-label design represents a limitation, and further research with adequate blinding is needed.
Task-specific training based on MRP was superior to CPT for improving balance and postural control in subacute stroke patients. Participants undergoing MRP exhibited significant and clinically relevant improvements that were sustained at follow-up.
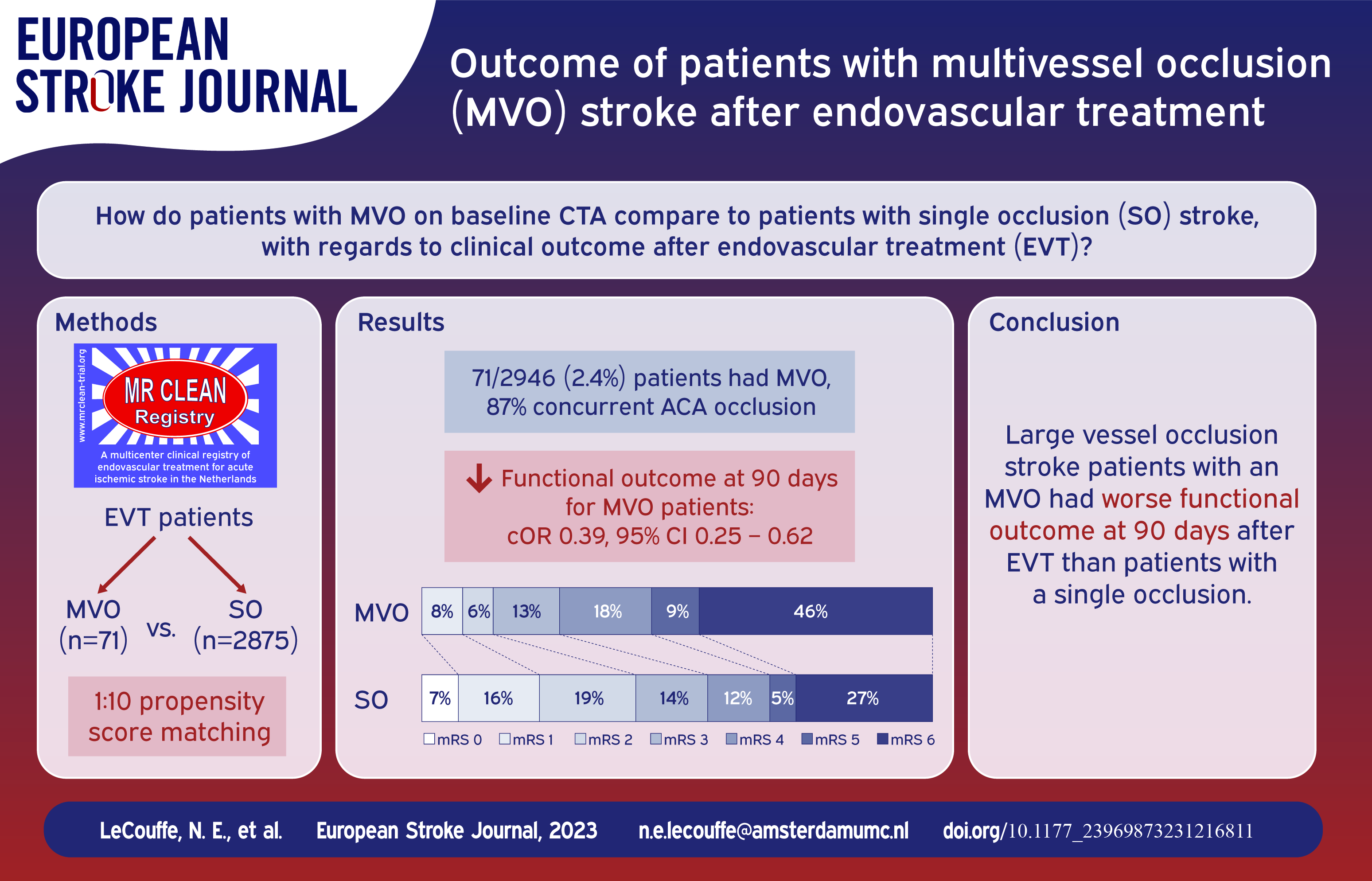
Little is known about the implications of multivessel occlusions (MVO) in large vessel occlusion stroke patients who undergo endovascular treatment (EVT).
We report data from the MR CLEAN Registry: a prospective, observational study on all stroke patients who underwent EVT in the Netherlands (March 2014–November 2017). We included patients with an intracranial target occlusion in the anterior circulation. An MVO was defined as an MCA occlusion (M1/M2) or intracranial ICA/ICA-T occlusion, with a concurrent second occlusion in the ACA or PCA territory confirmed on baseline CTA. To compare outcomes, we performed a 10:1 propensity score matching analysis with a logistic regression model including potential confounders. Outcome measures included 90-day functional outcome (modified Rankin Scale, mRS) and mortality.
Of 2946 included patients, 71 patients (2.4%) had an MVO (87% concurrent ACA occlusion, 10% PCA occlusion, 3% ⩾3 occlusions). These patients were matched to 71 non-MVO patients. Before matching, MVO patients had a higher baseline NIHSS (median 18 vs 16,
MVOs on baseline imaging were uncommon in LVO stroke patients undergoing EVT, but were associated with poor functional outcome.
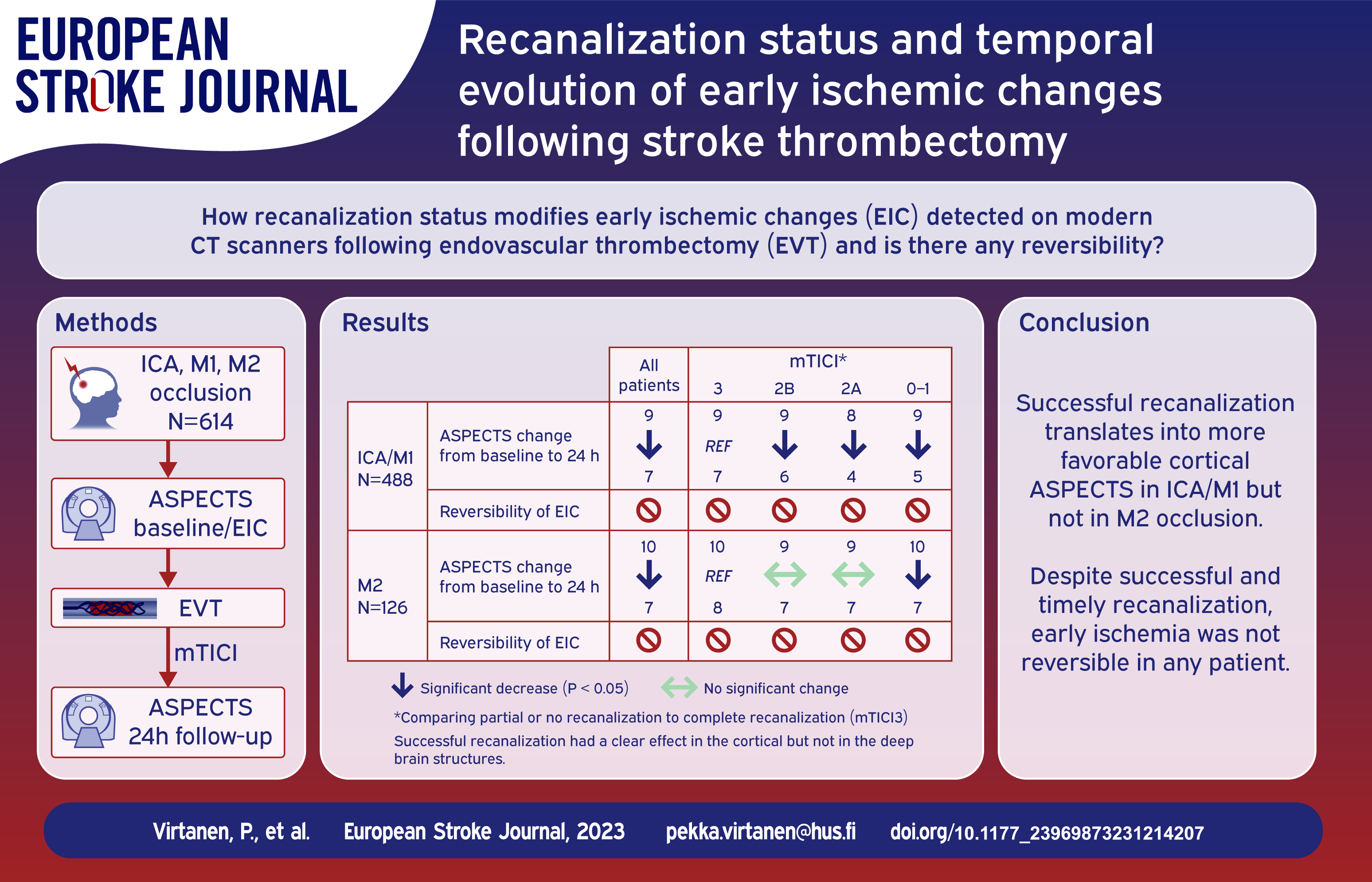
Present-day computer tomography (CT) scanners have excellent spatial resolution and signal-to-noise ratio and are instrumental detecting early ischemic changes (EIC) in brain. We assessed the temporal changes of EIC based on the recanalization status after thrombectomy.
The cohort comprises consecutive patients with acute ischemic stroke in anterior circulation treated with thrombectomy in tertiary referral hospital. All baseline and follow-up scans were screened for any ischemic changes and further classified using Alberta Stroke Program Early CT Score (ASPECTS). Generalized linear mixed models were used to analyze the impact of recanalization status using modified Thrombolysis in Cerebral Infarction (mTICI) on temporal evolution of ischemic changes.
We included 614 patients with ICA, M1, or M2 occlusions. Median ASPECTS score was 9 (IQR 7–10) at baseline and 7 (5-8) at approximately 24 h. mTICI 3 was achieved in 207 (33.8%), 2B 241 (39.3%), 2A in 77 (12.6%), and 0–1 in 88 (14.3%) patients. Compared to patients with mTICI 3, those with mTICI 0–1 and 2A had less favorable temporal changes of ASPECTS (
Temporal evolution of the ischemic changes and ASPECTS are related to the success of the recanalization therapy in cortical regions of ICA/M1 patients, but not in their deep brain structures or M2 patients. In none of the patients did EIC revert in any brain region after successful recanalization.
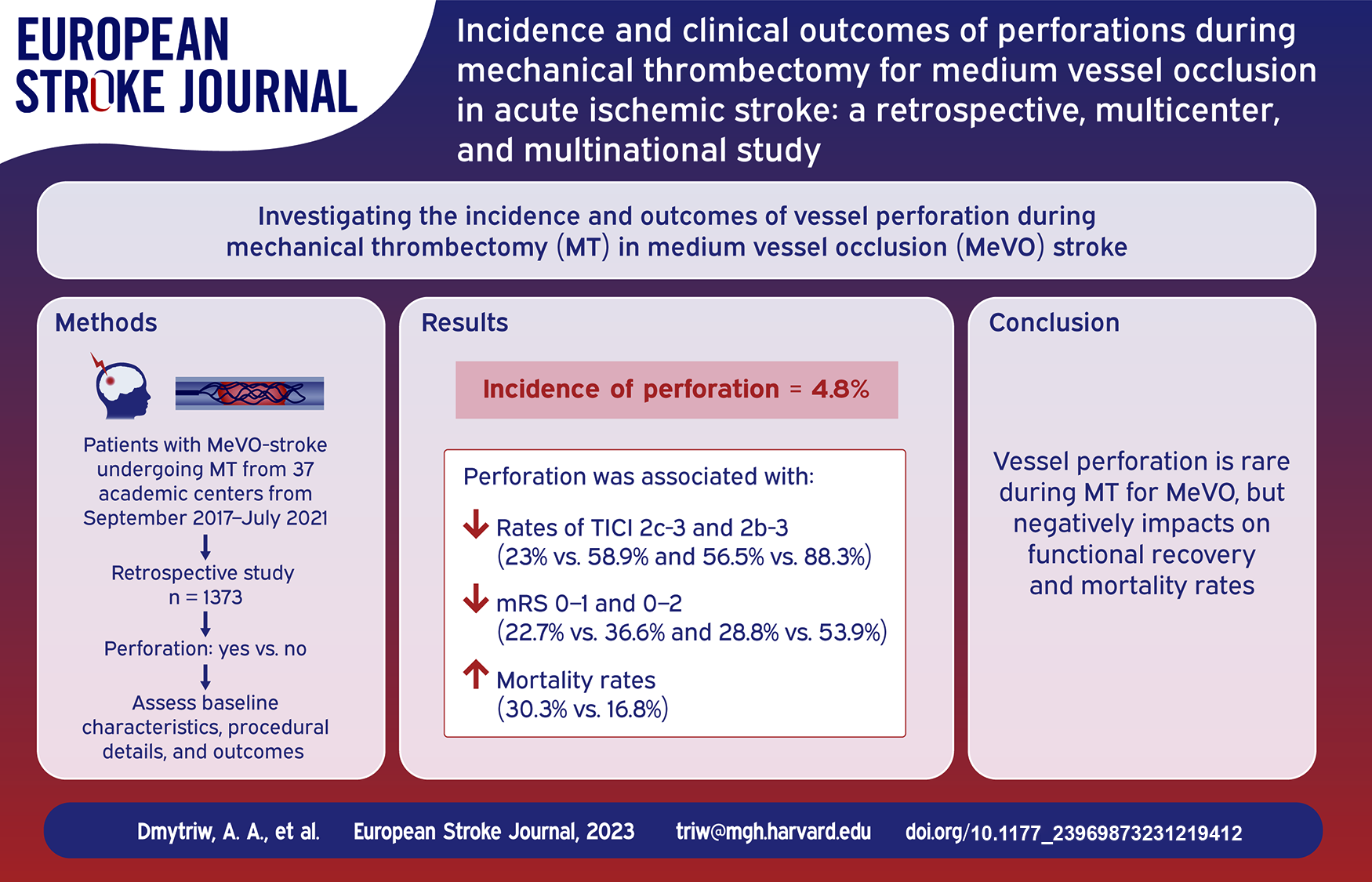
Mechanical thrombectomy (MT) has revolutionized the treatment of acute ischemic stroke (AIS) due to large vessel occlusion (LVO), but its efficacy and safety in medium vessel occlusion (MeVO) remain less explored. This multicenter, retrospective study aims to investigate the incidence and clinical outcomes of vessel perforations (confirmed by extravasation during an angiographic series) during MT for AIS caused by MeVO.
Data were collected from 37 academic centers across North America, Asia, and Europe between September 2017 and July 2021. A total of 1373 AIS patients with MeVO underwent MT. Baseline characteristics, procedural details, and clinical outcomes were analyzed.
The incidence of vessel perforation was 4.8% (66/1373). Notably, our analysis indicates variations in perforation rates across different arterial segments: 8.9% in M3 segments, 4.3% in M2 segments, and 8.3% in A2 segments (
This study reveals that while the occurrence of vessel perforation in MT for AIS due to MeVO is relatively rare, it is associated with poor functional outcomes and higher mortality. The findings highlight the need for increased caution and specialized training in performing MT for MeVO. Further prospective research is required for risk mitigation strategies.
As a marker of chronic cerebral small vessel disease, leukoaraiosis (LA) was reported to impact the recruitment of collaterals in acute ischemic stroke (AIS). We intended to explore the impact of LA on the infarct growth rate (IGR) and clinical outcome by impaired collateral development in AIS patients with large vessel occlusion (LVO) who underwent endovascular thrombectomy (EVT).
Two hundred thirty-six AIS patients who underwent EVT were retrospectively reviewed. The severity of LA was graded using the Fazekas scale with non-contrast CT. IGR was calculated by the acute core volume on CT perfusion divided by the time from stroke onset to imaging. The collateral status after LVO was assessed using the ASITN/SIR collateral scale. The clinical outcomes after EVT were evaluated using a
Patients with severe LA had significantly larger core volume on CTP (
The increasing severity of LA is associated with impaired collateral status and fast infarct growth. These findings suggest that LA may become a predictive imaging biomarker for the likelihood of progression of tissue injury and clinical outcome after EVT in acute large vessel occlusion stroke.

The MR CLEAN-LATE trial has shown that patient selection for endovascular treatment (EVT) in the late window (6–24 h after onset or last-seen-well) based on the presence of collateral flow on CT-angiography is safe and effective. We aimed to assess the cost-effectiveness of late-window collateral-based EVT-selection compared to best medical management (BMM) over a lifetime horizon (until 95 years of age).
A model-based economic evaluation was performed from a societal perspective in The Netherlands. A decision tree was combined with a state-transition (Markov) model. Health states were defined by the modified Rankin Scale (mRS). Initial probabilities at 3-months post-stroke were based on MR CLEAN-LATE data. Transition probabilities were derived from previous literature. Information on short- and long-term resource use and utilities was obtained from a study using MR CLEAN-LATE and cross-sectional data. All costs are expressed in 2022 euros. Costs and quality-adjusted life years (QALYs) were discounted at a rate of 4% and 1.5%, respectively. The effect of parameter uncertainty was assessed using probabilistic sensitivity analysis (PSA).
On average, the EVT strategy cost €159,592 (95% CI: €140,830–€180,154) and generated 3.46 QALYs (95% CI: 3.04–3.90) per patient, whereas the costs and QALYs associated with BMM were €149,935 (95% CI: €130,841–€171,776) and 2.88 (95% CI: 2.48–3.29), respectively. The incremental cost-effectiveness ratio per QALY and the incremental net monetary benefit were €16,442 and €19,710, respectively. At a cost-effectiveness threshold of €50,000/QALY, EVT was cost-effective in 87% of replications.
Collateral-based selection for late-window EVT is likely cost-effective from a societal perspective in The Netherlands.

Neurology senior residents and stroke fellows are first to clinically assess and interpret imaging studies of patients presenting to the emergency department with acute stroke. The aim of this study was to compare the diagnostic accuracy of brain CT angiography (CTA) with and without CT perfusion (CTP) between neurology senior residents and stroke fellows.
In this neuroimaging study, nine practitioners (four senior neurology residents (SNRs) and five stroke fellows (SFs)) clinically assessed and interpreted the imaging data of 50 cases (15 normal images, 21 large vessel occlusions (LVOs) and 14 medium vessel occlusions (MeVOs) in two sessions, 1 week apart in comparison to final diagnosis of experienced neuroradiologist and experienced stroke neurologist consensus. Interrater agreement of CTA alone and CTA with CTP was quantified using kappa statistics, sensitivity, specificity and overall accuracy.
Overall, arterial occlusions were correctly identified in 221/315 (70.1%) with CTA alone and in 266/315 (84.4%) with CTA and CTP (
In cerebral arterial occlusions, the rate of LVO and MeVOs detections increases when adding CTP to CTA. The accuracy and time for diagnosing arterial occlusion can be significantly improved if CTP is added to CTA. As MeVOs are commonly missed by front-line neurology senior residents or stroke fellows, cases with significant deficits and no apparent arterial occlusions need to be reviewed with neuroradiological expertise.

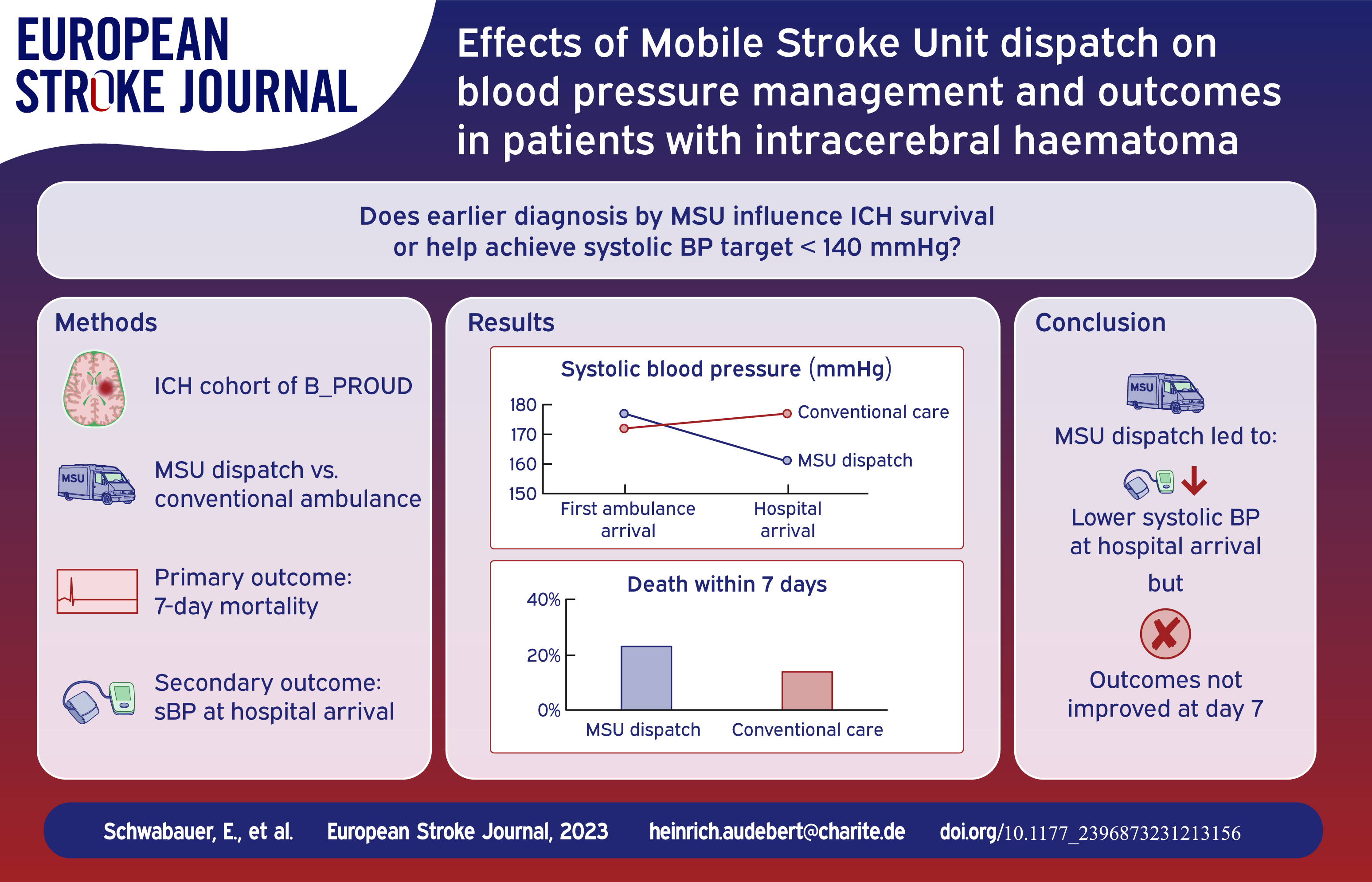
In patients with acute intracerebral haemorrhage (ICH) and elevated systolic blood pressure (BP), guidelines suggest that systolic BP reduction to <140 mmHg should be rapidly initiated. Compared with conventional care, Mobile Stroke Units (MSUs) allow for earlier ICH diagnosis through prehospital imaging and earlier BP lowering.
ICH patients were prospectively evaluated as a cohort of the controlled B_PROUD-study in which MSU availability alone determined MSU dispatch in addition to conventional ambulance. We used inverse probability of treatment weighting to adjust for confounding to estimate the effect of additional MSU dispatch in ICH patients. Outcomes of interest were 7-day mortality (primary), systolic BP (sBP) at hospital arrival, dispatch-to-imaging time, largest haematoma volume, anticoagulation reversal, length of in-hospital stay, 3-month functional outcome.
Between February 2017 and May 2019, MSUs were dispatched to 95 (mean age: 72 ± 13 years, 45% female) and only conventional ambulances to 78 ICH patients (mean age: 71 ± 12 years, 44% female). After adjusting for confounding, we found shorter dispatch-to-imaging time (mean difference: -17.75 min, 95% CI: −27.16 to −8.21 min) and lower sBP at hospital arrival (mean difference = −16.31 mmHg, 95% CI: −30.64 to −6.19 mmHg) in the MSU group. We found no statistically significant difference for the other outcomes, including 7-day mortality (adjusted odds ratio: 1.43, 95% CI: 0.68 to 3.31) or favourable outcome (adjusted odds ratio = 0.67, 95% CI: 0.27 to 1.67).
Although MSU dispatch led to sBP reduction and lower dispatch-to-imaging time compared to conventional ambulance care, we found no evidence of better outcomes in the MSU dispatch group.
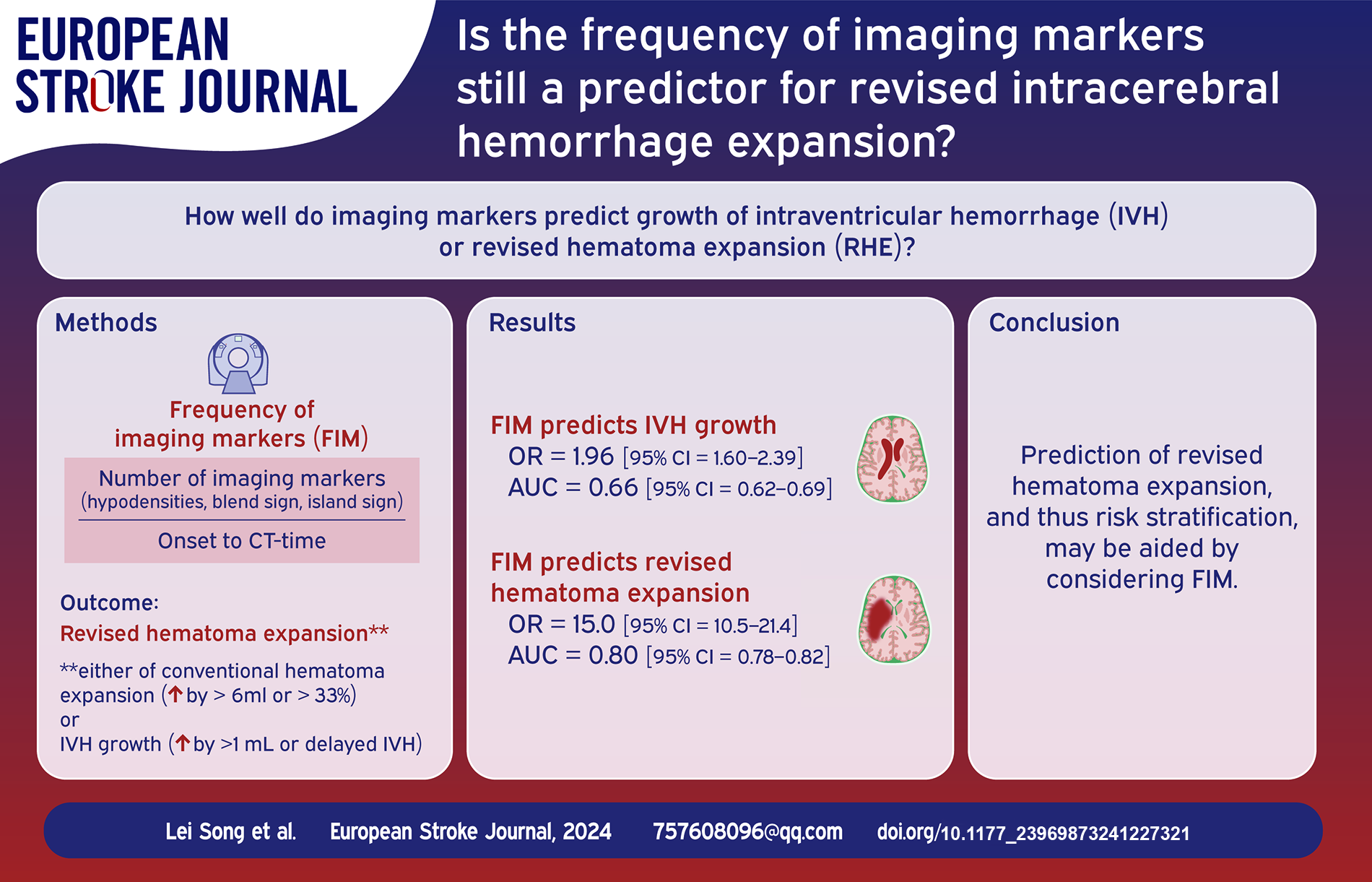
Frequency of imaging markers (FIM) has been described as a novel predictor for hematoma expansion after intracerebral hemorrhage (ICH). A revised definition of hematoma expansion that incorporates intraventricular hemorrhage (IVH) growth, that is, revised hematoma expansion (RHE), has also been proposed. Nevertheless, the associations between FIM and IVH growth or RHE remains unexplored. The objective of this study was to assess the influence and performance of the FIM on two types.
Patient selection and variables were based on our published protocol. FIM was defined as the ratio of the number of imaging markers to the onset-to-neuroimaging time. The association between FIM and two definitions was tested by multivariate analysis. The area under the receiver operating characteristic curve (AUC), sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of the FIM on two definitions were also evaluated.
There were 303 (20.36%) and 583 (39.18%) subjects in the IVH growth and RHE, respectively. Multivariate analysis demonstrated that FIM was associated with both IVH growth and RHE (odds ratio [OR] = 1.96, 95% confidence interval [CI] = 1.60–2.39; OR = 15.01, 95% CI = 10.51–21.43, respectively). The optimal cutoff points for FIM to predict IVH growth and RHE were 0.63 and 0.62, with AUC, sensitivity, specificity, PPV, and NPV of 0.66, 0.50, 0.78, 0.36, and 0.86 versus 0.80, 0.60, 0.93, 0.84, and 0.78, respectively.
FIM was not only a predictor of IVH growth, but also of RHE. These findings may have important clinical implications for decision-making based on risk stratification of patients with ICH.
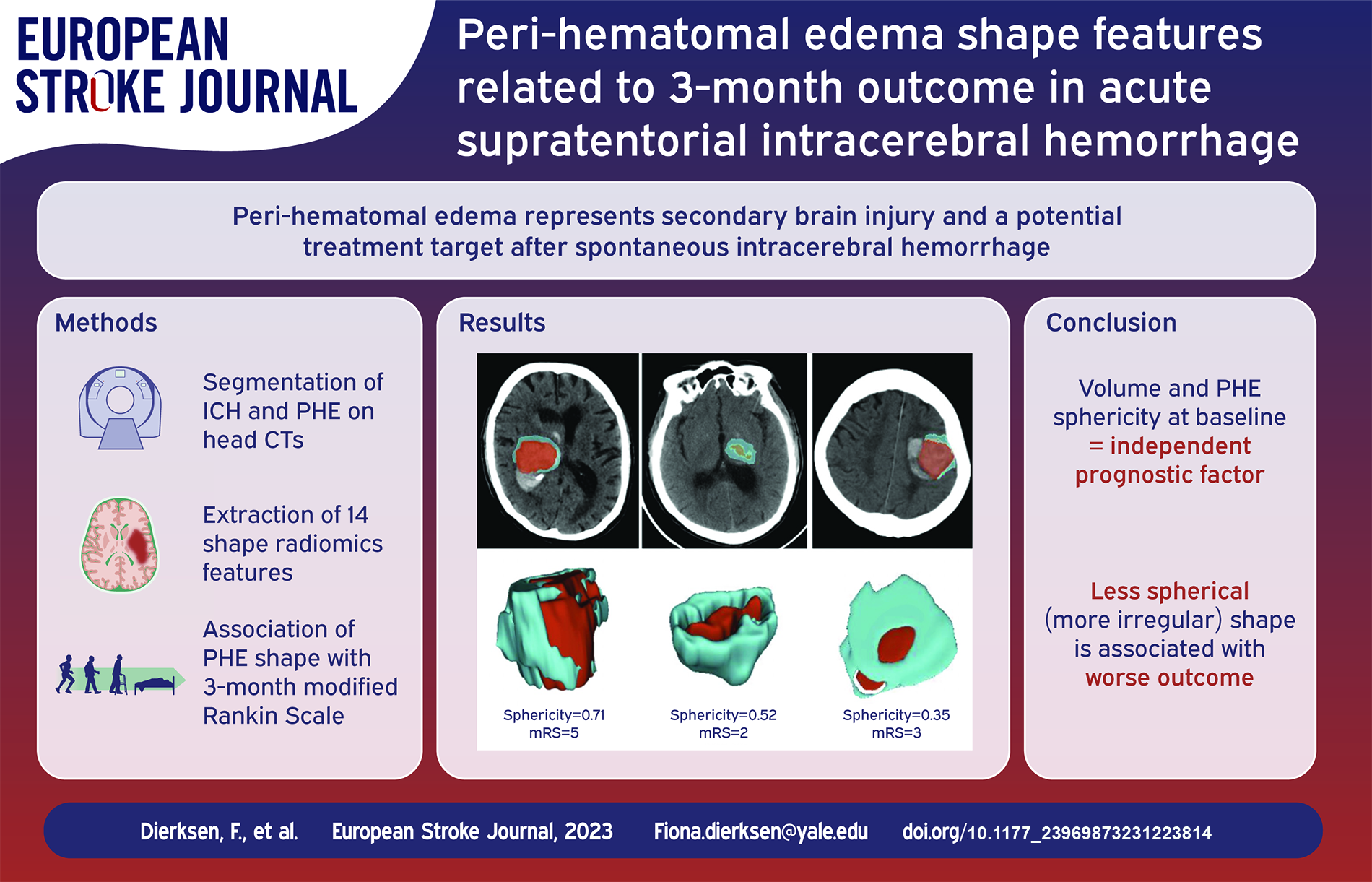
Perihematomal edema (PHE) represents secondary brain injury and a potential treatment target in intracerebral hemorrhage (ICH). However, studies differ on optimal PHE volume metrics as prognostic factor(s) after spontaneous, non-traumatic ICH. This study examines associations of baseline and 24-h PHE shape features with 3-month outcomes.
We included 796 patients from a multicentric trial dataset and manually segmented ICH and PHE on baseline and follow-up CTs, extracting 14 shape features. We explored the association of baseline, follow-up, difference (baseline/follow-up) and temporal rate (difference/time gap) of PHE shape changes with 3-month modified Rankin Score (mRS) – using Spearman correlation. Then, using multivariable analysis, we determined if PHE shape features independently predict outcome adjusting for patients’ age, sex, NIH stroke scale (NIHSS), Glasgow Coma Scale (GCS), and hematoma volume.
Baseline PHE maximum diameters across various planes, main axes, volume, surface, and sphericity correlated with 3-month mRS adjusting for multiple comparisons. The 24-h difference and temporal change rates of these features had significant association with outcome – but not the 24-h absolute values. In multivariable regression, baseline PHE shape sphericity (OR = 2.04, CI = 1.71–2.43) and volume (OR = 0.99, CI = 0. 98–1.0), alongside admission NIHSS (OR = 0.86, CI = 0.83–0.88), hematoma volume (OR = 0.99, CI = 0. 99–1.0), and age (OR = 0.96, CI = 0.95–0.97) were independent predictors of favorable outcomes.
In acute ICH patients, PHE shape sphericity at baseline emerged as an independent prognostic factor, with a less spherical (more irregular) shape associated with worse outcome. The PHE shape features absolute values over the first 24 h provide no added prognostic value to baseline metrics.
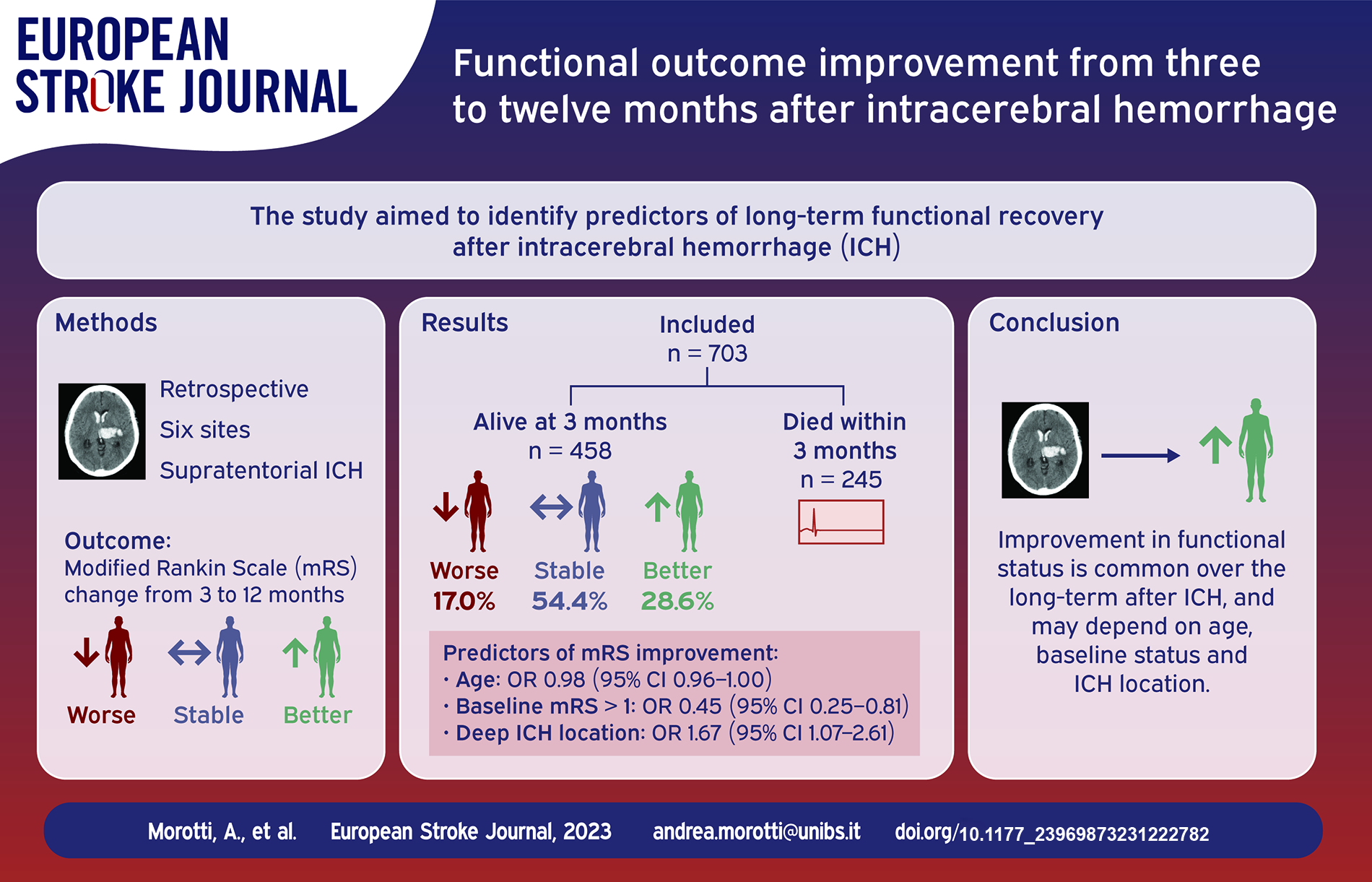
Most intracerebral hemorrhage (ICH) trials assessed outcome at 3 months but the recovery trajectory of ICH survivors may continue up to 1 year after the index event. We aimed to describe the predictors of functional outcome improvement from 3 to 12 months after ICH.
Retrospective analysis of patients admitted to six European Stroke Centers for supratentorial ICH. Functional outcome was measured with the modified Rankin Scale (mRS) at 3 and 12 months. Predictors of functional outcome improvement were explored with binary logistic regression.
We included 703 patients, of whom 245 (34.9%) died within 3 months. Among survivors, 131 (28.6%) had an mRS improvement, 78 (17.0%) had a worse mRS and 249 (54.4%) had a stable functional status at 12 months. Older age and the presence of baseline disability (defined as pre-stroke mRS > 1), were associated with lower odds of functional outcome improvement (Odds Ratio (OR) 0.98 per year increase, 95% Confidence Interval (CI) 0.96–1.00,
Long term recovery is common after ICH and associated with age, baseline functional status, mRS at 3 months and hematoma location. Our findings might inform future trials and improve long-term prognostication in clinical practice.
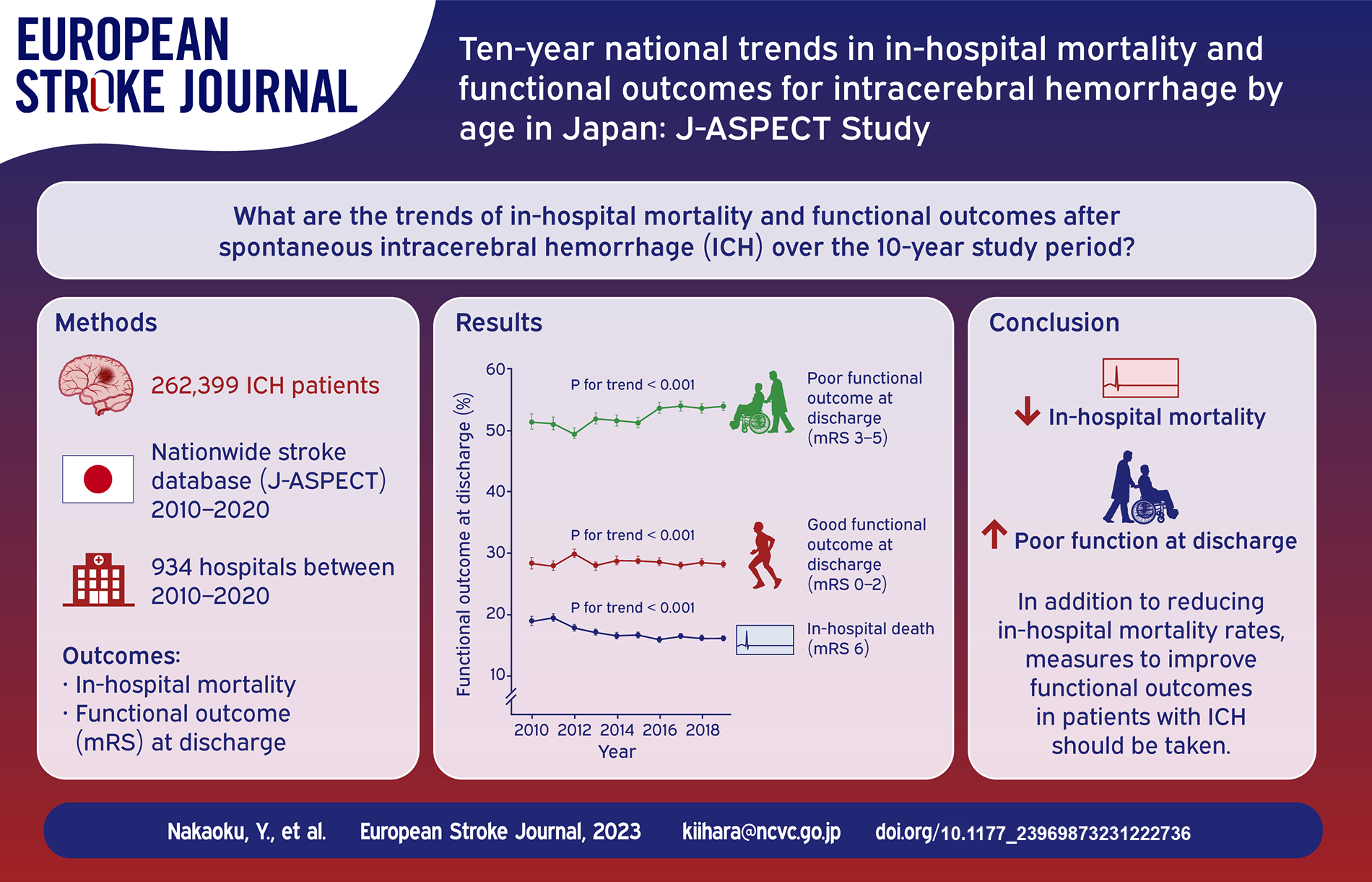
National-level data on trends in the prognosis of age-stratified patients with intracerebral hemorrhage (ICH) are lacking. This study aimed to assess time trends in in-hospital mortality and functional outcomes of ICH patients by sex and age, and to explore factors associated with changes in in-hospital mortality trend.
Using the largest nationwide, J-ASPECT stroke database in Japan, this serial cross-sectional study included ICH patients aged ⩾18 years who were hospitalized for non-traumatic ICH from April 2010 to March 2020. We examined trends in in-hospital mortality and functional outcomes using the modified Rankin Scale at discharge, as well as differences in in-hospital mortality change between age groups.
Among 262,399 ICH patients from 934 hospitals, crude in-hospital mortality showed a significant decreasing time trend (from 19.5% to 16.7%), and this trend was consistent across sex and age groups. In addition, differences in in-hospital mortality change over the 10-year study period were significant between male patients aged ⩾75 years and those aged ⩽64 years (−3.9% [95% confidence interval, −5.4 to −2.4] for 75–84 years; −4.1% [−6.3 to −1.9] for ⩾85 years). On the other hand, the proportion of dependent patients (mRS 3–5) at discharge increased from 52.0% to 54.9% over the 10-year study period.
The in-hospital mortality of ICH patients improved, whereas the proportion of patients with dependent functional outcome at discharge increased, over the 10-year study period. Elucidating the mechanism underlying differences in in-hospital mortality reduction in men may provide insights into effective interventions in the future.
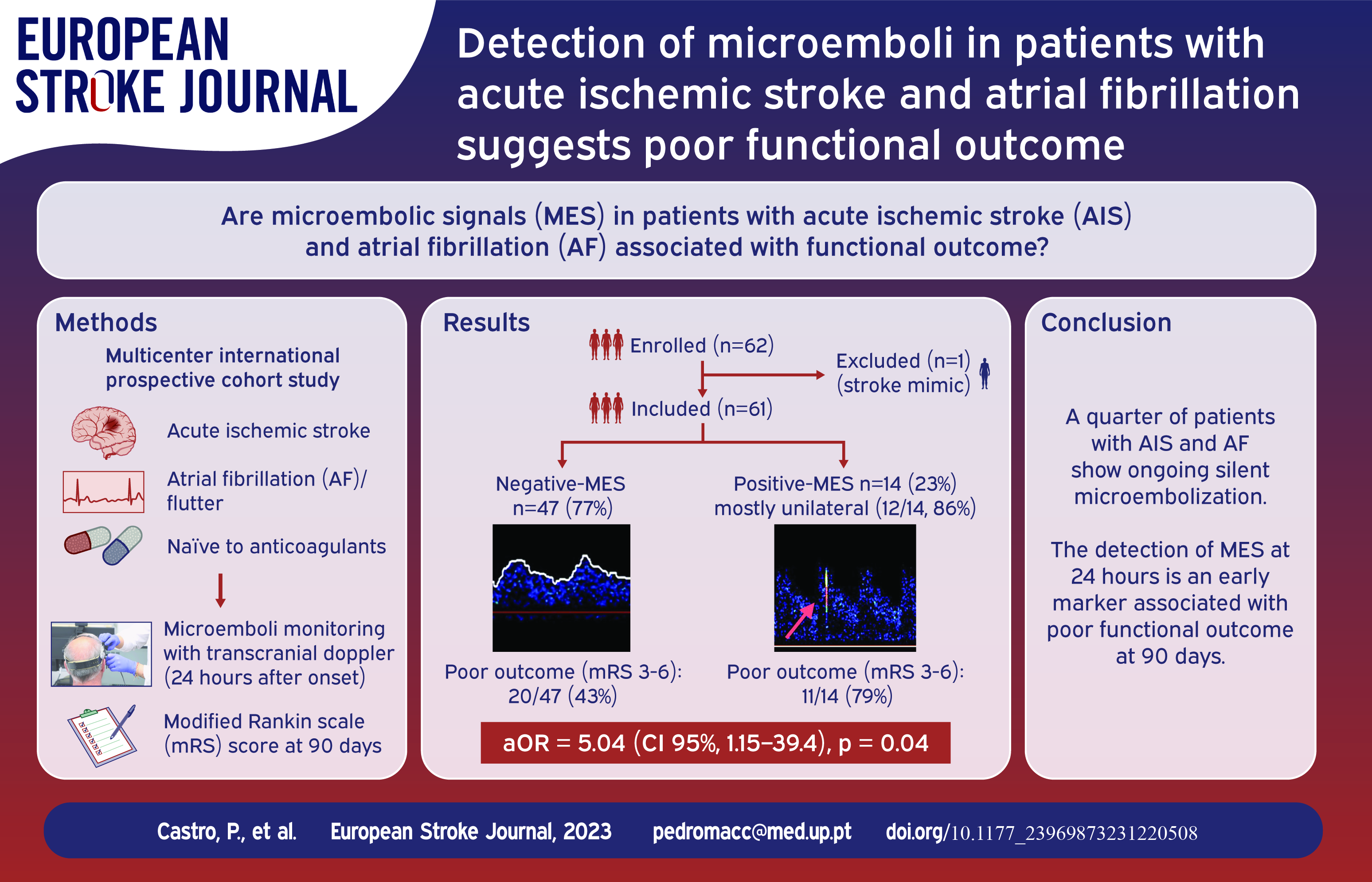
We investigated the burden of microembolic signals (MES) in patients with acute ischaemic stroke (AIS) and atrial fibrillation (AF), assessing their impact on functional outcomes.
This multicentre international prospective cohort study involved patients with AIS and either a known or newly diagnosed anticoagulant-naïve AF. All centres utilised the same transcranial Doppler machine for 1-h monitoring with bilateral 2 MHz probes within 24 h of symptom onset. Recordings underwent MES analysis by a blinded central reader. The primary objectives were to ascertain the MES proportion and its association with functional outcomes assessed by the modified Rankin scale (mRS) score at 90 days.
Between September 2019 and May 2021, we enrolled 61 patients, with a median age of 78 years (interquartile range 73–83) and a median stroke severity score of 11 (interquartile range 4–18). MES were observed in 14 patients (23%), predominantly unilateral (12/14, 86%), with a median rate of 6 counts/hour (interquartile range 4–18). MES occurrence was higher post-thrombectomy and among those with elevated brain natriuretic peptide levels (
Nearly a quarter of patients with AIS and AF exhibited silent microembolization after the index event. Detecting MES within 24 h post-stroke (using transcranial Doppler) could signify a marker of poor functional outcomes. Subsequent trials will assess if very early antithrombotic treatment might enhance outcomes in this highly selective group of cardioembolic stroke patients. (Clinicaltrials.gov ID: NCT06018090).
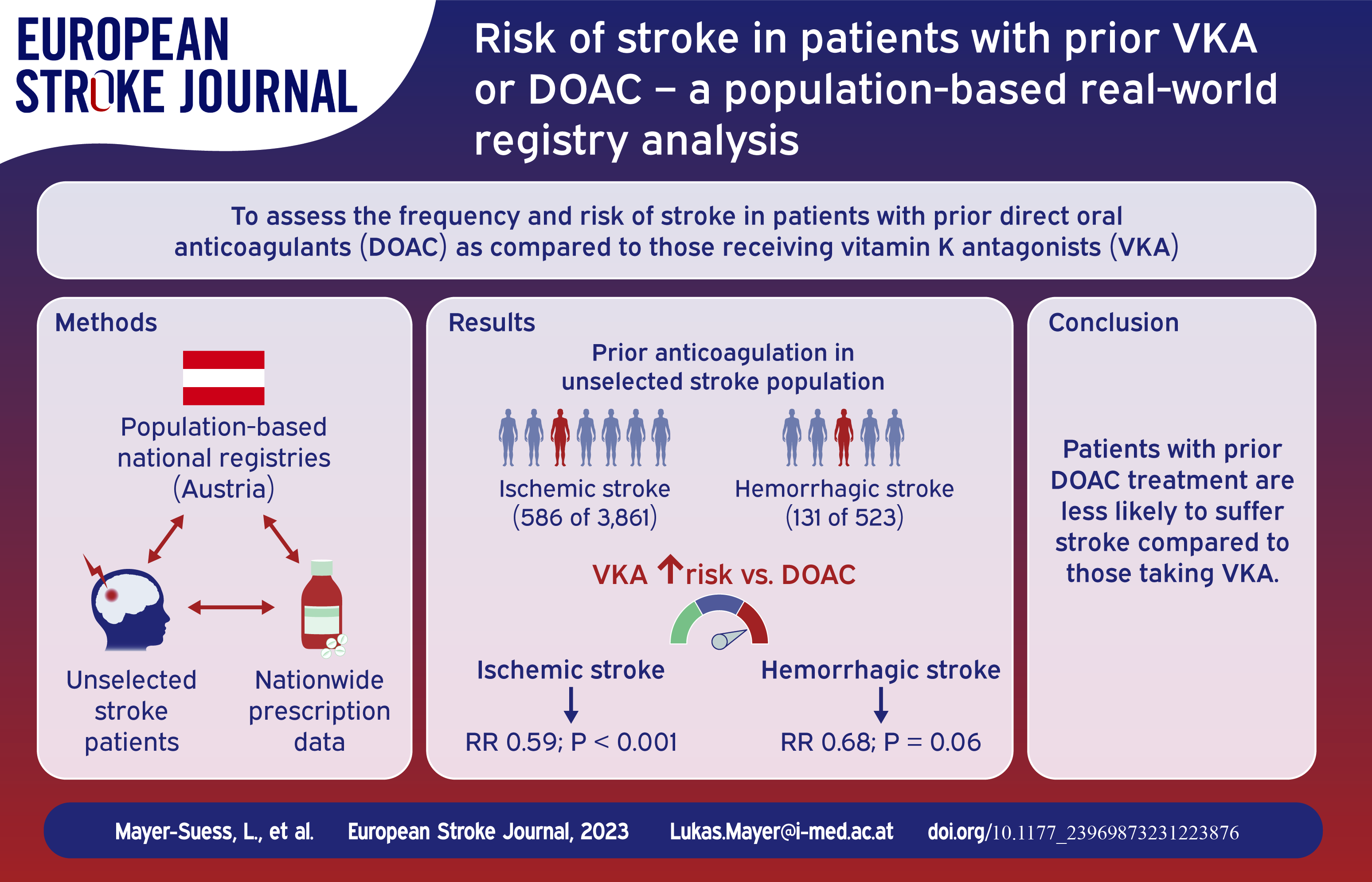
To date, risk assessment of suffering ischemic and hemorrhagic stroke in individuals under oral anticoagulation (OAC) is limited to hospital-based cohorts and patients with atrial fibrillation.
Through the combination of three individual datasets, (1) the population-based Tyrolean Stroke Pathway database, prospectively documenting all (unselected) stroke patients in the entire federal state of the Tyrol and (2) nation-wide prescription data, detailing each reimbursed prescription in Austria as well as (3) the Austrian Stroke Unit Registry, a nation-wide registry comprising data on all patients admitted to any of the 38 stroke units in Austria, we assessed risk of stroke in patients with prior oral anticoagulation and compared characteristics of patients taking direct oral anticoagulants and Vitamin-K-Antagonists.
In Austria, oral anticoagulant prescription reimbursements increased from 292,475 in 2015 to 389,407 in 2021. In the Tyrol, prior oral anticoagulation treatment was evident in 586 of 3861 (15.2%) patients with ischemic and 131 of 523 (25.0%) with hemorrhagic stroke, with 20% and 35% of those stroke patients respectively having prior oral anticoagulation due to other indications than non-valvular atrial fibrillation. Considering prescription rates, treatment with direct oral anticoagulants was associated with a reduced stroke risk compared to Vitamin-K-Antagonists, especially in ischemic (1.05% vs 0.62%; RR 0.59,
One in seven patients suffering ischemic and one in four suffering hemorrhagic stroke had prior oral anticoagulation treatment. Both ischemic and hemorrhagic strokes are less frequent in those with direct oral anticoagulant intake compared to those taking Vitamin-K-Antagonists. Establishment of clear standard operating procedures on how to best care for acute stroke patients with oral anticoagulation is essential.
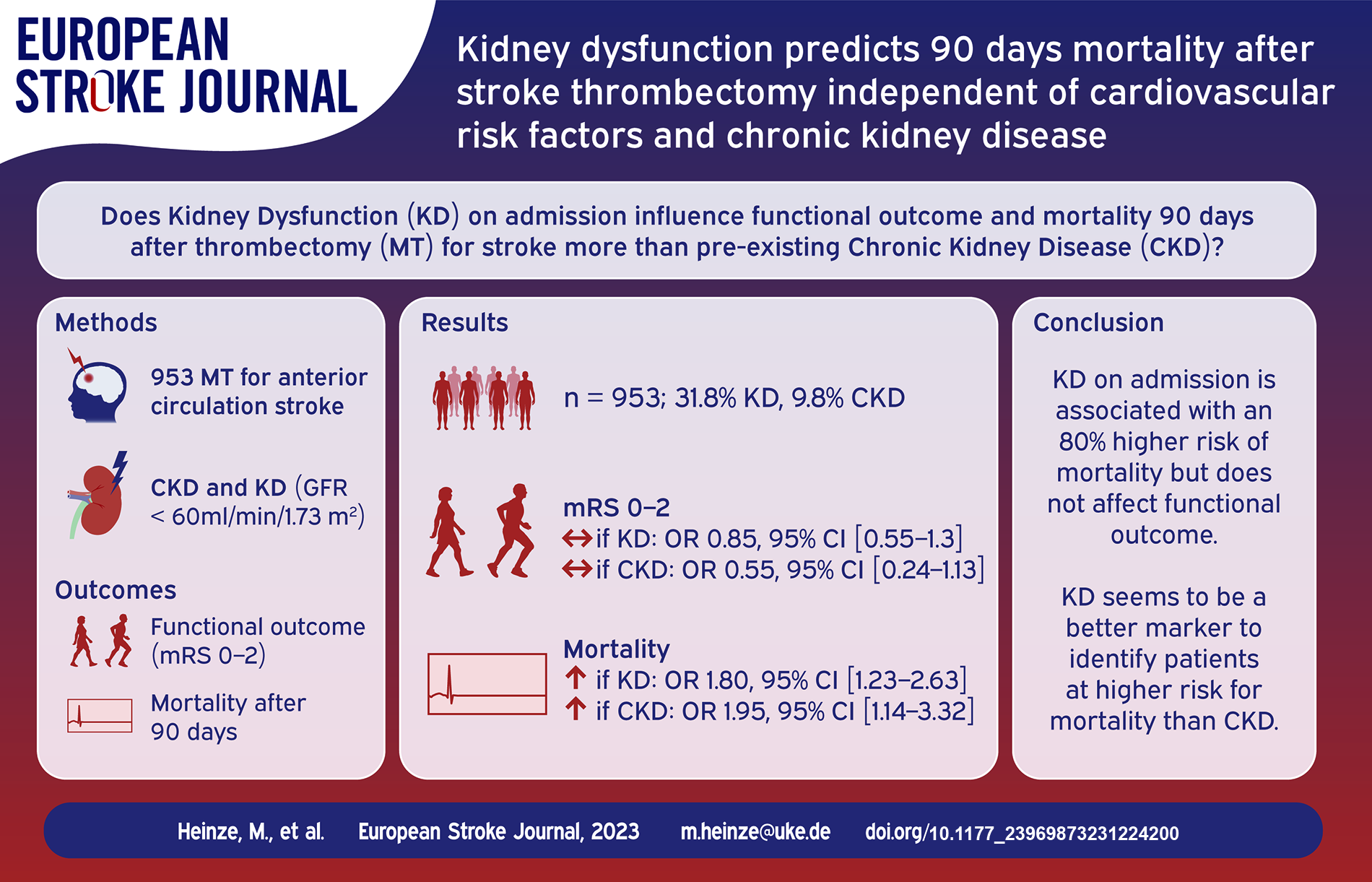
Kidney dysfunction (KD) is a risk factor for cerebrovascular events and has been shown to have a detrimental effect on outcome after stroke. We evaluated the influence of KD at admission and pre-existing diagnosis of chronic kidney disease (CKD) before thrombectomy for anterior circulation stroke on functional independence and mortality 90 days after stroke in this cross-sectional study.
We included patients with acute ischemic stroke in the anterior circulation treated with thrombectomy at our hospital between June 2015 and May 2022. We analyzed clinical characteristics, laboratory values and pre-existing diagnosis of CKD. KD at admission was defined as glomerular filtration rate (GFR) <60 ml/min/1.73 m2. Outcomes were defined as a modified Rankin Scale Score of 0-2 for functional independence and mortality at 90 days. We fitted multivariate regression analysis to examine the influence of pre-treatment KD and pre-diagnosed CKD on outcome.
Nine hundred fifty-three patients were included in this analysis (mean age 73.8 years, 54.2% female). KD was present in 31.8%, and patients with KD were older and more often female, presented more often with comorbidities such as arterial hypertension, diabetes, and atrial fibrillation, and were less often independent before the index stroke. In multivariate analysis adjusted for age, independence before the index stroke, diabetes, hypertension, atrial fibrillation, initial NIHSS, thrombolysis treatment, and recanalization outcome, KD on admission had no significant influence on functional independence 90 days after stroke, but predicted mortality with an odds ratio of 1.80 (95% CI 1.23–2.63,
KD might function as a surrogate parameter for comorbidity burden and thus increased risk of mortality in this cohort.
KD on admission is associated with an 80% higher risk of mortality at 90 days after stroke thrombectomy independent of cardiovascular risk factors and CKD awareness. KD on admission should not exclude patients from thrombectomy but might support prognostic evaluation.
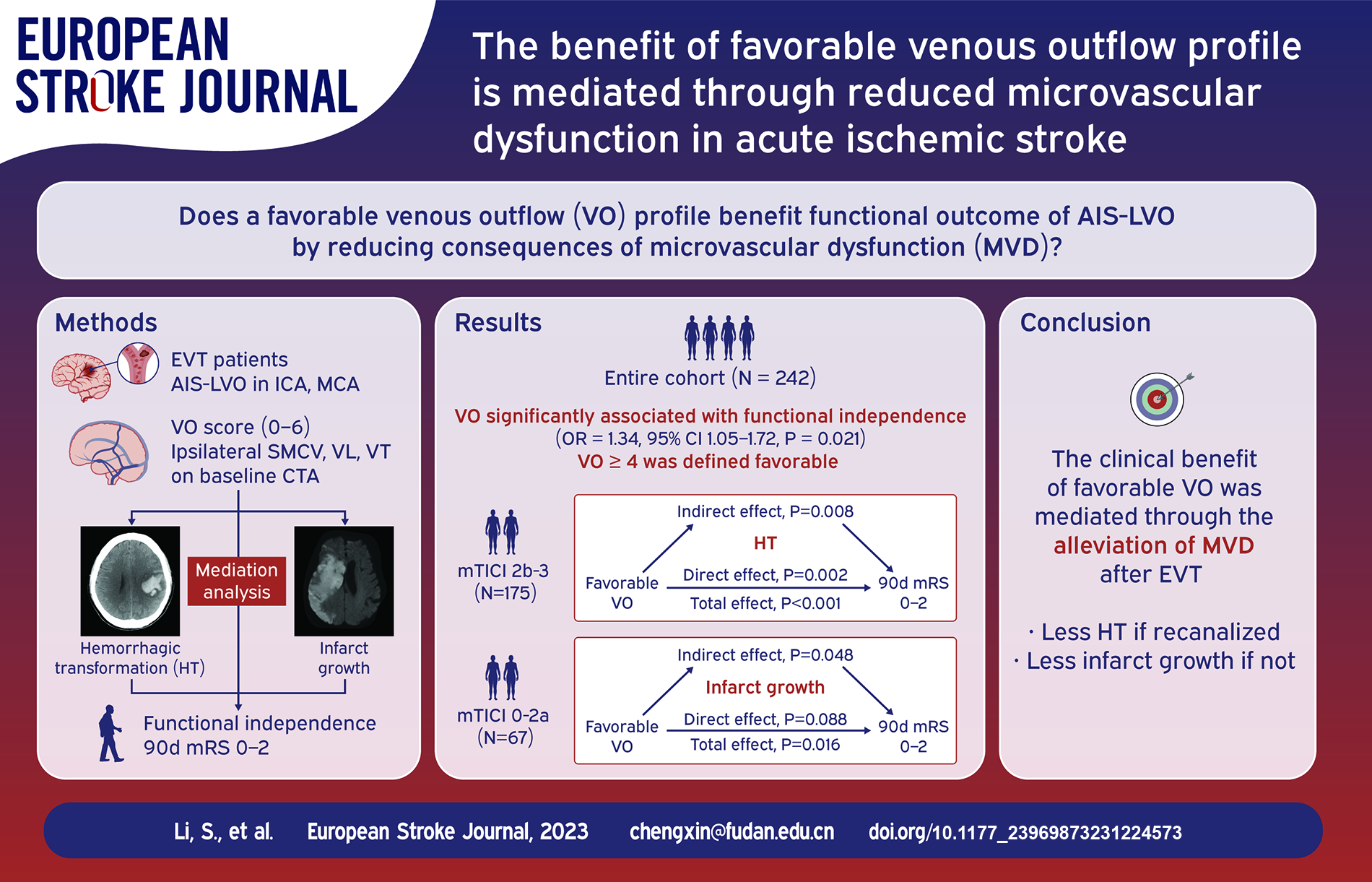
Venous outflow (VO) is emerging as a marker of microvascular integrity in acute ischemic stroke. Using hemorrhagic transformation (HT) and infarct growth as mediators, we tested whether a favorable VO profile benefited functional outcome by reducing consequences of microvascular dysfunction.
Patients receiving thrombectomy in three comprehensive stroke centers due to acute anterior circulation occlusion were included. VO was assessed semi-quantitatively by the opacification of ipsilateral vein of Labbé, Trolard and superficial middle cerebral vein. HT was graded on follow-up CT. Infarct growth volume (IGV) was the difference of final infarct volume and baseline core volume. The association of VO and functional independence (90-day modified Rankin Scale ⩽ 2) was examined by logistic regression. Mediation analysis was performed among VO, HT or IGV, and functional outcome in patients with or without recanalization, respectively.
In 242 patients analyzed, VO was strongly correlated with functional independence and VO ⩾ 4 was defined favorable. In 175 patients recanalized, favorable VO was associated with a reduced risk of HT (OR = 0.82, 95% CI 0.71–0.95,
In patients with acute anterior large vessel occlusion, the clinical benefit of VO may be mediated through reduced microvascular dysfunction.
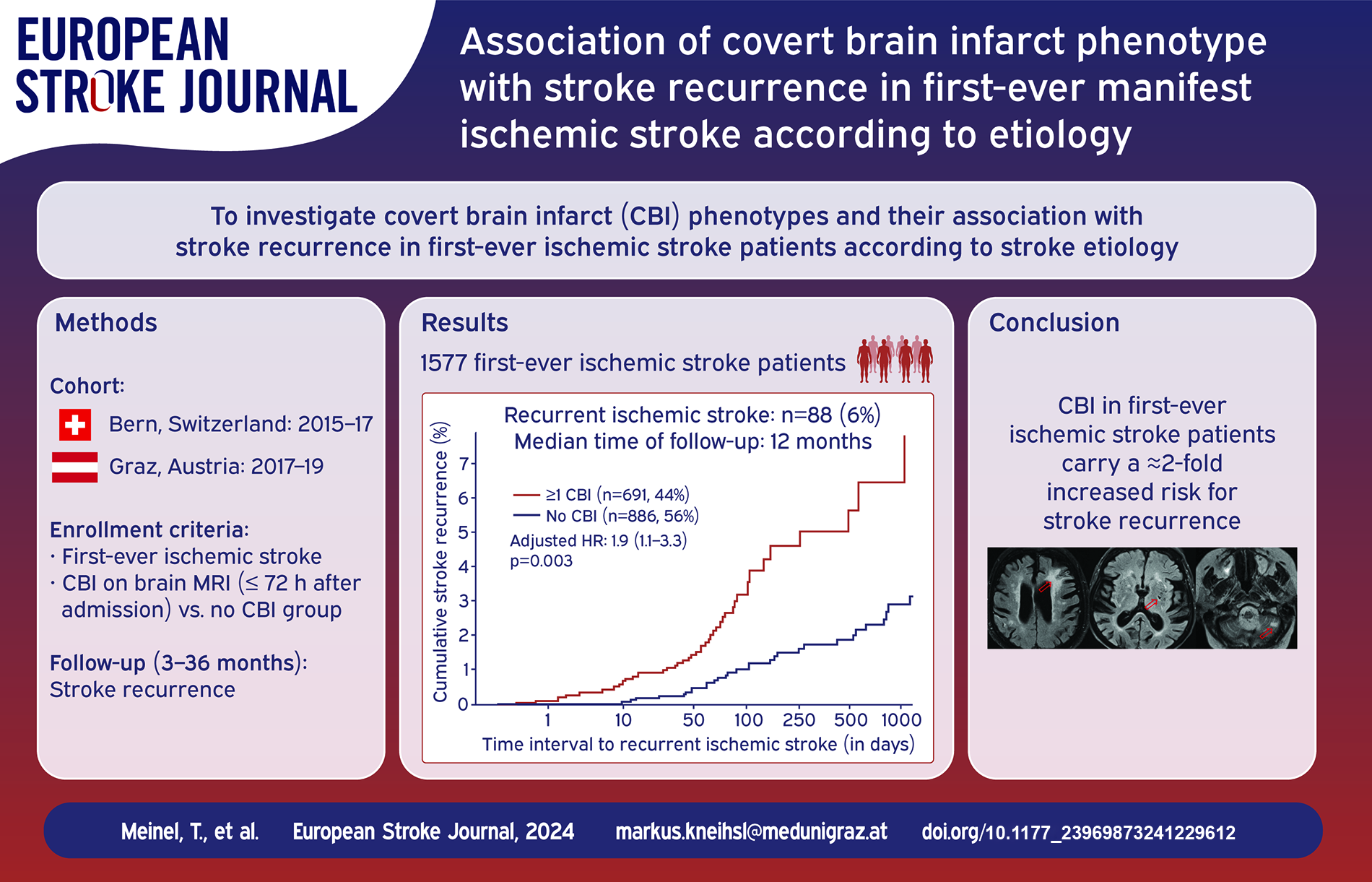
Covert brain infarcts (CBI) are frequent incidental findings on MRI and associated with future stroke risk in patients without a history of clinically evident cerebrovascular events. However, the prognostic value of CBI in first-ever ischemic stroke patients is unclear and previous studies did not report on different etiological stroke subtypes. We aimed to test CBI phenotypes and their association with stroke recurrence in first-ever ischemic stroke patients according to stroke etiology.
This study is a pooled data analysis of two prospectively collected cohorts of consecutive first-ever ischemic stroke patients admitted to the comprehensive stroke centers of Bern (Switzerland) and Graz (Austria). CBI phenotypes were identified on brain MRI within 72 h after admission. All patients underwent a routine follow-up (median: 12 months) to identify stroke recurrence.
Of 1577 consecutive ischemic stroke patients (median age: 71 years), 691 patients showed CBI on brain MRI (44%) and 88 patients had a recurrent ischemic stroke (6%). Baseline CBI were associated with stroke recurrence in multivariable analysis (HR 1.9, 95% CI 1.1–3.3). CBI phenotypes with the highest risk for stroke recurrence were cavitatory CBI in small vessel disease (SVD)-related stroke (HR 7.1, 95% CI 1.6–12.6) and cortical CBI in patients with atrial fibrillation (HR 3.0, 95% CI 1.1–8.1).
This study reports
Subject terms: Covert brain infarcts, stroke
Severe sleep apnea (SA) affects one-third of stroke patients. Sleepiness, one of the cardinal symptoms of SA, negatively impacts functional stroke outcomes. The impact of continuous positive airway pressure (CPAP) on post-stroke sleepiness is poorly described. We aimed to compare through a propensity score matching the trajectories of self-reported sleepiness post-stroke with matched individuals including SA patients adherent or not to CPAP.
Sixty five (80.2%) ischemic stroke and 16 (19.8%) TIA patients (median [Q1;Q3] age = 67.0 [58.0;74.0] years, 70.4% male, body mass index [BMI] = 26.1 [24.5;29.8] kg·m−2, admission NIHSS = 3.0 [1.0;5.0]), with polysomnography and an Epworth Sleepiness Scale (ESS) performed within 1 year following stroke and with a follow-up ESS (delay = 236 [147;399] days) were included in the analysis. A 2:1 propensity score matching based on age, gender, BMI, and the apnea-hypopnea index was performed to identify 162 matched individuals referred for SA suspicion, free of stroke or TIA. Multivariable negative binomial regression models were performed to identify the determinants of sleepiness trajectories post-stroke.
Baseline ESS was comparable between stroke/TIA and matched individuals (median [Q1; Q3] ESS = 7 [4;10] versus 6 [4;10],
Sleepiness improvement was unexpectedly higher in stroke patients compared to matched individuals, with no significant influence of comorbid SA and CPAP on its trajectory. Sleepiness may not be primarily indicative of SA in stroke or TIA patients.

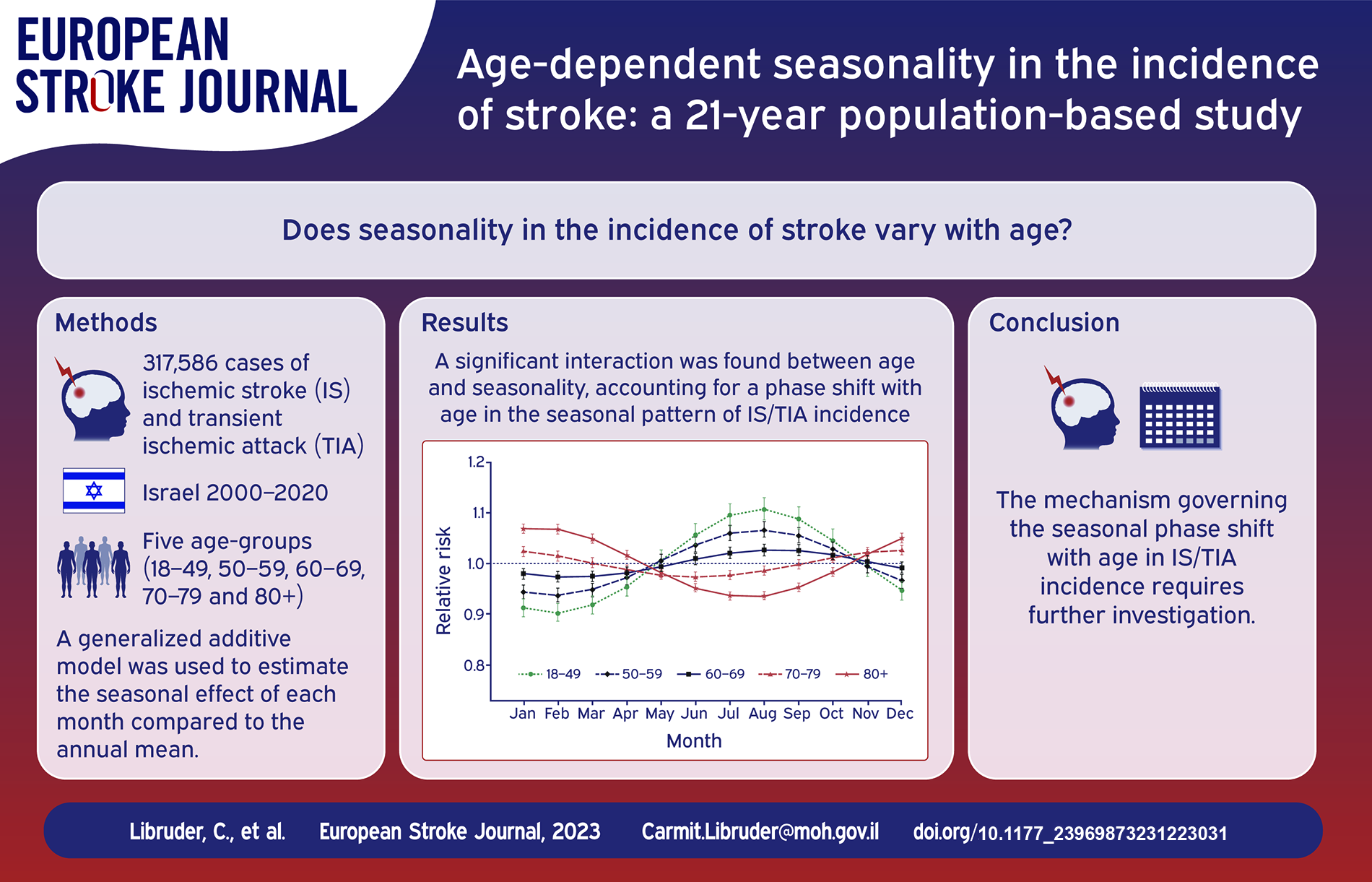
Seasonality in the incidence of stroke has been examined in numerous studies, yet data on whether it differs with age are limited. To fill this gap, we utilized a largescale dataset from Israel.
We retrieved data of all hospitalizations for ischemic stroke (IS), transient ischemic attack (TIA) and intra cerebral hemorrhage (ICH) from 2000 to 2020. We maintained separate datasets for IS/TIA and ICH, divided into five age groups: 18–49, 50–59, 60–69, 70–79, and 80+. We modeled the monthly incidence using a generalized additive model. The seasonal effect was defined by the rate ratio (RR) of each month compared to the annual mean.
The analysis included 317,586 and 23,789 events of IS/TIA and ICH respectively. We found an interaction between age and seasonality, accounting for a phase shift with age in the seasonal pattern of IS/TIA incidence. For cases under 70 years, the peak was during summertime and the RRs increased with decreasing age, reaching 1.11 (95% CI 1.09–1.13) at the youngest age group. In contrast, among the elderly, a winter peak was observed and the RRs increased with age to 1.07 (95% CI 1.06–1.08) at the oldest age group. For ICH, a winter/autumn peak was identified and the RRs increased with age to 1.20 (95% CI 1.16–1.24).
Our finding of age-dependent seasonal patterns in the occurrence of stroke, suggests closer monitoring of cardiovascular risk factors during wintertime among elderly individuals. The mechanism governing the seasonal phase shift with age in IS/TIA incidence, requires further investigation.
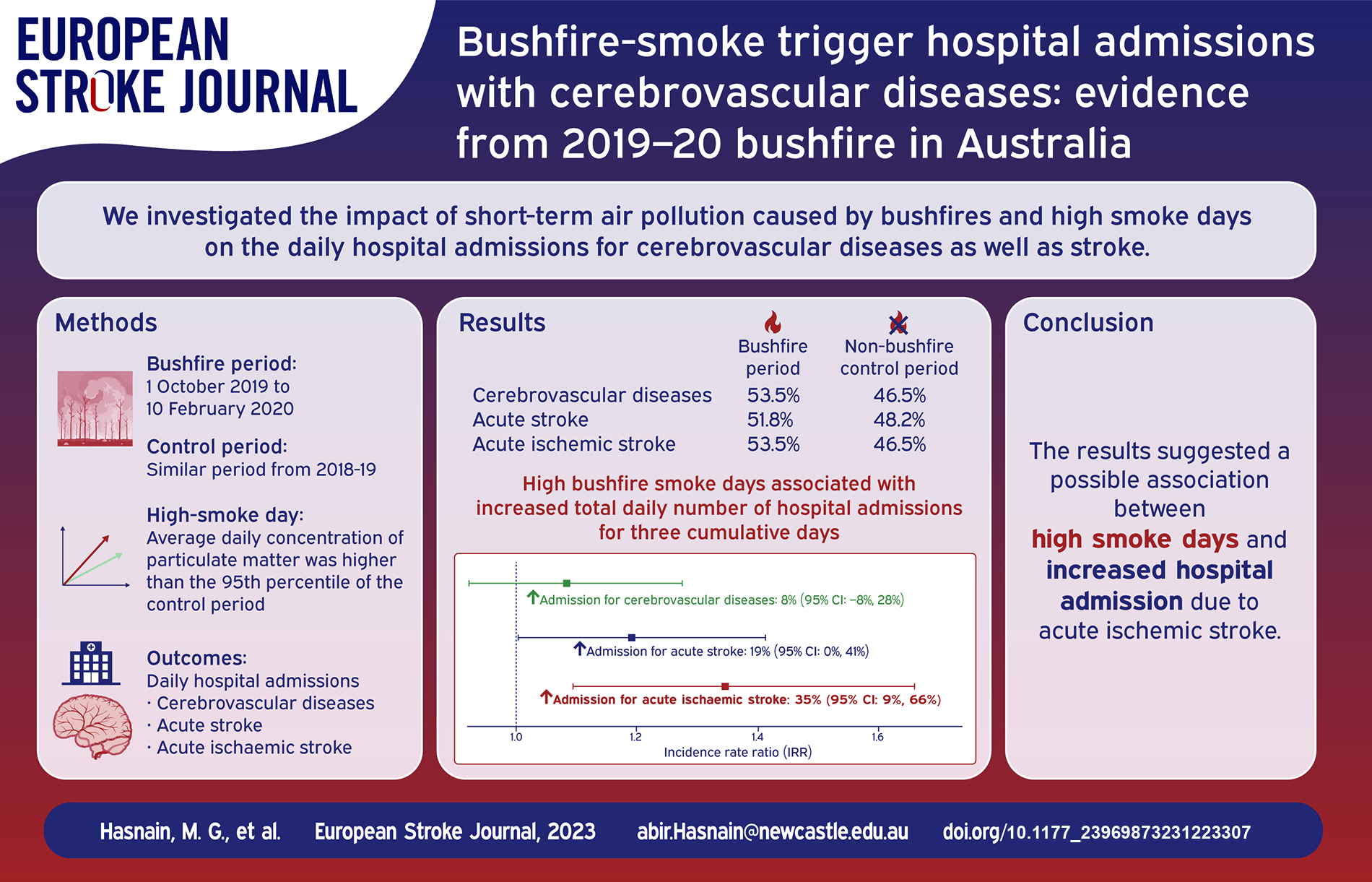
Exposure to ambient air pollution is strongly associated with increased cerebrovascular diseases. The 2019–20 bushfire season in Australia burnt 5.4 million hectares of land in New South Wales alone, with smoke so severe it affected cities in Argentina, 11,000 km away. The smoke emitted by bushfires consists of both gaseous and particle components. It is important to note that exposure to particulate matter has been shown to be linked to a heightened risk of stroke, which is the primary kind of cerebrovascular illness, as well as an increased likelihood of hospitalisations and mortality. However, the available data is inadequate in terms of documenting the response of patients diagnosed with a proven cerebrovascular illness to bushfire smoke. Additionally, there is a lack of information about the health effects associated with particulate matter throughout the bushfire season and on days when smoke was present in 2019 and 2020.
Therefore, we aimed to determine the effects of (i) short-term air pollution triggered by bushfires and (ii) high smoke days in increasing the daily number of hospital admissions with cerebrovascular diseases.
Hospitalisation data were accessed from the admitted patient dataset from seven local Government areas of Hunter New England Local Health District. The bushfire period was defined from 1 October 2019 to 10 February 2020, and a same period from 2018–19 as the control. High bushfire smoke days were days when the average daily concentration of particulate matter was higher than the 95th percentile of the control period. Poisson regression models and fixed effect meta-analysis were used to analyse the data.
In total, 275 patients with cerebrovascular admissions were identified, with 147 (53.5%) during the bushfire (2019-20) and 128 (46.5%) in the control period (2018–19). There was no significant increase in daily admissions for cerebrovascular disease (Incidence Rate Ratio, IRR: 1.04; 95% CI: 0.81–1.34;
The results suggested a possible association between particulate matter and high smoke days with increased hospital admissions due to acute ischaemic stroke during the recent Australian bushfire season.
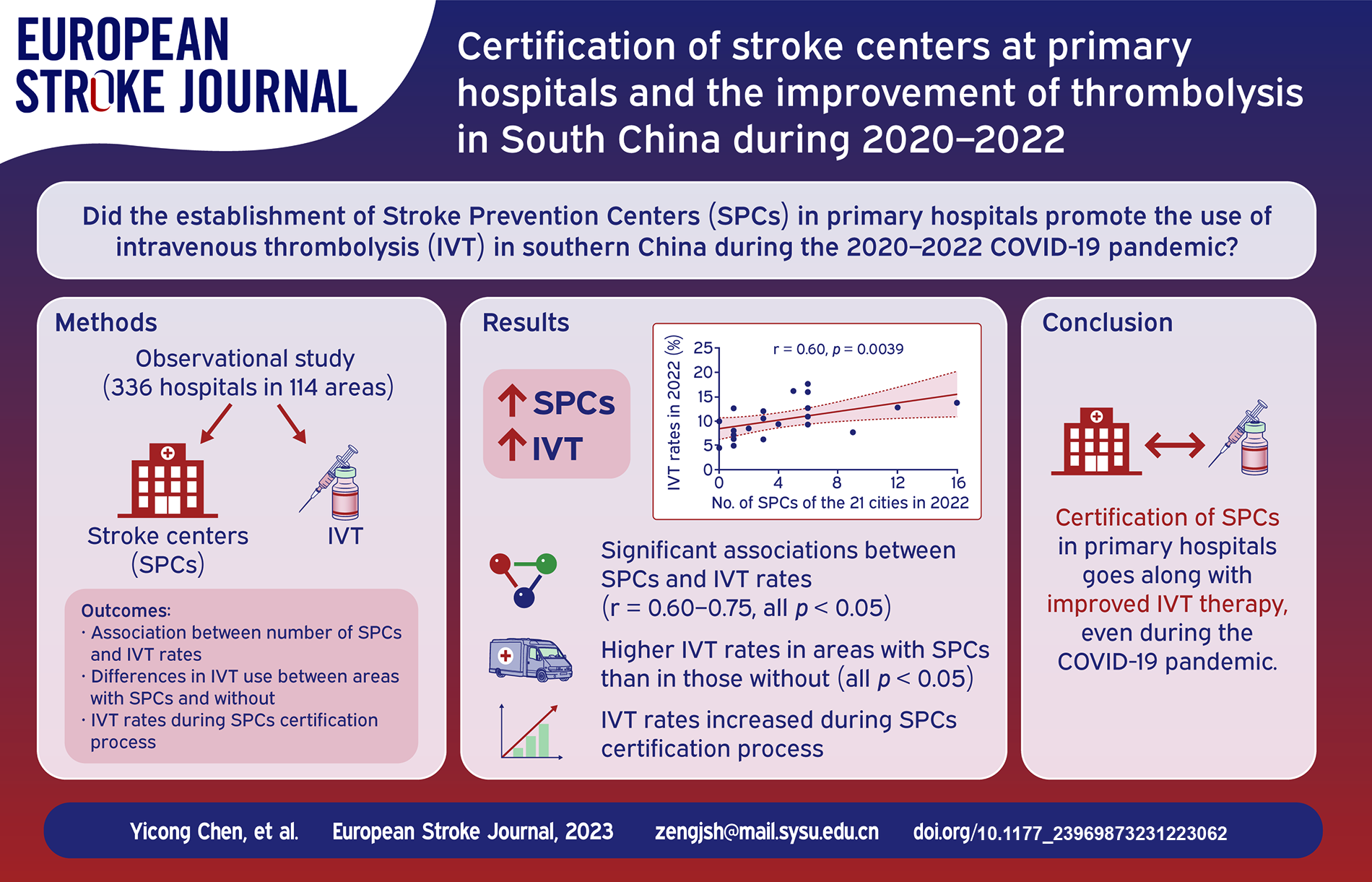
IVT use declined globally in 2020 due to the Corona Virus Disease 2019 (COVID-19) pandemic, but it increased in South China. This study was conducted to evaluate the association of establishing Stroke Prevention Centers (SPCs) at primary hospitals with IVT increase in South China.
We conducted a longitudinal observational study across 336 hospitals in 114 areas in South China during 2020–2022. Data regarding certified stroke centers, IVT volumes, and IVT rates were collected. Correlations between IVT rates and the number or density of stroke centers were accessed. IVT use was compared among areas with different levels of stroke centers or on different certification process.
During 2020–2022, there were 83, 125, and 152 stroke centers, with 26, 65, and 92 SPCs, respectively. IVT therapies were 12,795, 17,266, and 20,411, representing a 29.8% increase/year (all
Well-organised SPCs and IVT therapy demonstrated substantial increase during the 3-year period. Certification of SPCs at primary hospitals is associated with improved IVT therapy in South China even with city lockdown during COVID-19 pandemic.
Reperfusion therapies represent promising treatments for patients with Central Retinal Artery Occlusion (CRAO), but access is limited due to low incidence and lack of protocols. We aimed to describe the benefit of implementing a Retinal Stroke-Code protocol regarding access to reperfusion, visual acuity and aetiological assessment.
Prospective cohort study performed at a Comprehensive Stroke Centre. Criteria for activation were sudden monocular, painless vision loss within 6 h from onset. Eligible patients received IAT when immediately available and IVT otherwise. All patients were followed by ophthalmologists to assess best-corrected visual acuity (BCVA) and visual complications, and by neurologists for aetiological workup. Visual amelioration was defined as improvement of at least one Early Treatment Diabetic Retinopathy Study (ETDRS) letter from baseline to 1 week.
Of 49 patients with CRAO, 15 (30.6%) received reperfusion therapies (12 IVT, 3 IAT). Presentation beyond 6 h was the main contraindication. Patients receiving reperfusion therapies had better rates of visual improvement (33.3% vs 5.9%,
A comprehensive acute management of CRAO is feasible despite low incidence. In our study, reperfusion therapies were safe and associated with higher rates of visual recovery. A similar etiological workup than ischemic stroke led to of high proportion of underlying aetiologies.

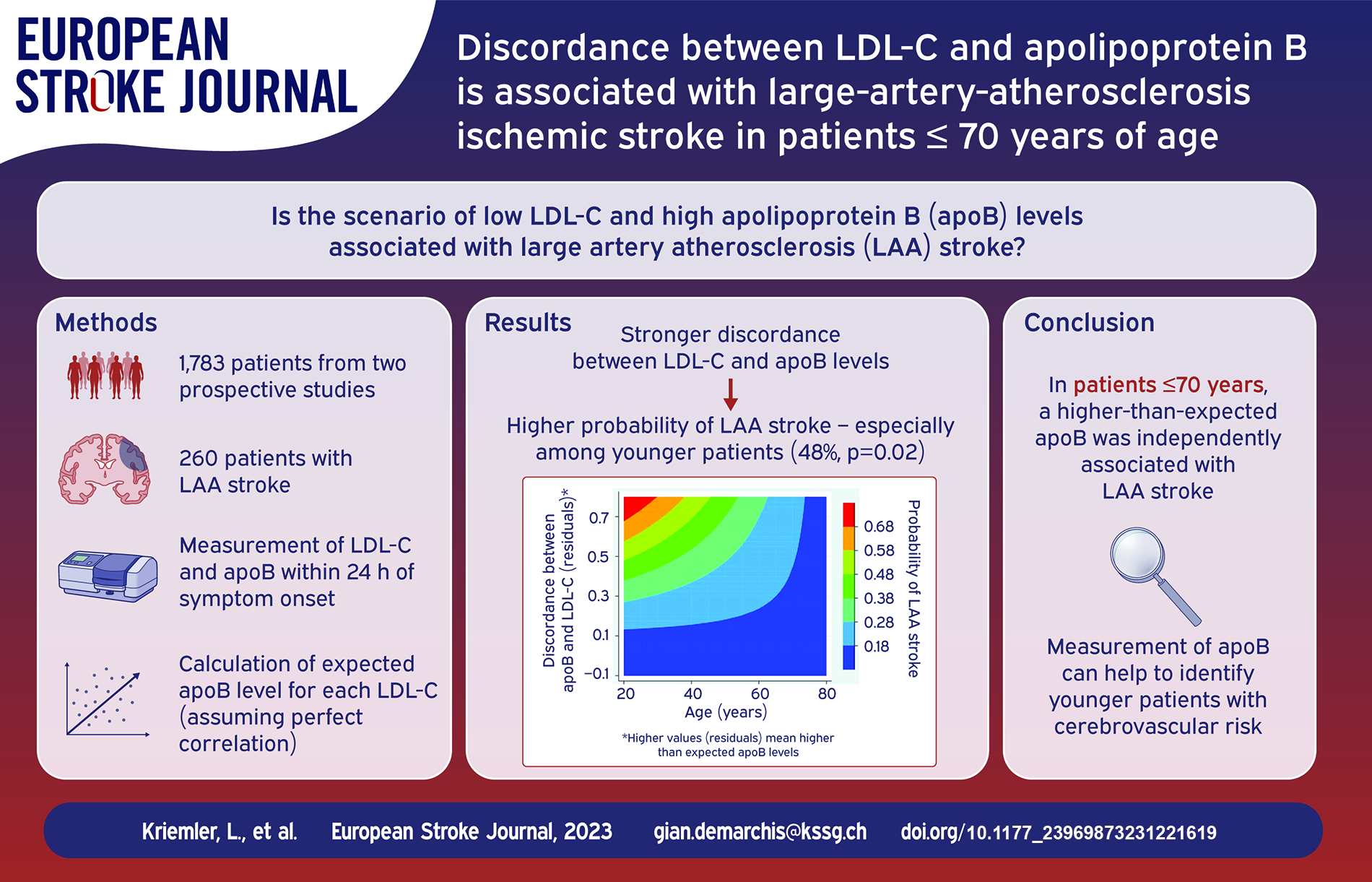
Low density lipoprotein (LDL-C) and other atherogenic lipoproteins are coated by apolipoprotein B100 (apoB). The correlation between LDL-C and apoB is usually thight, but in some cases LDL-C underestimates apoB levels and residual cardiovascular risk. We aimed to assess if a discordance of LDL-C-levels with apoB levels is associated with LAA stroke.
We included patients with an acute ischemic stroke from two prospective studies enrolled at the University Hospital Bern, Basel and Zurich, Switzerland. LDL-C and apoB were measured within 24 h of symptom onset. By linear regression, for each LDL-C, we computed the expected apoB level assuming a perfect correlation. Higher-than-expected apoB was defined as apoB level being in the upper residual tertile.
Overall, we included 1783 patients, of which 260 had a LAA stroke (15%). In the overall cohort, higher-than-expected apoB values were not associated with LAA. However, a significant interaction with age was present. Among the 738 patients ⩽70 years of age, a higher-than-expected apoB was more frequent in patients with LAA- versus non LAA-stroke (48% vs 36%,
Among patients aged ⩽70 years, a higher-than-expected apoB was independently associated with LAA stroke. Measuring apoB may help identify younger stroke patients potentially benefiting from intensified lipid-lowering therapy.
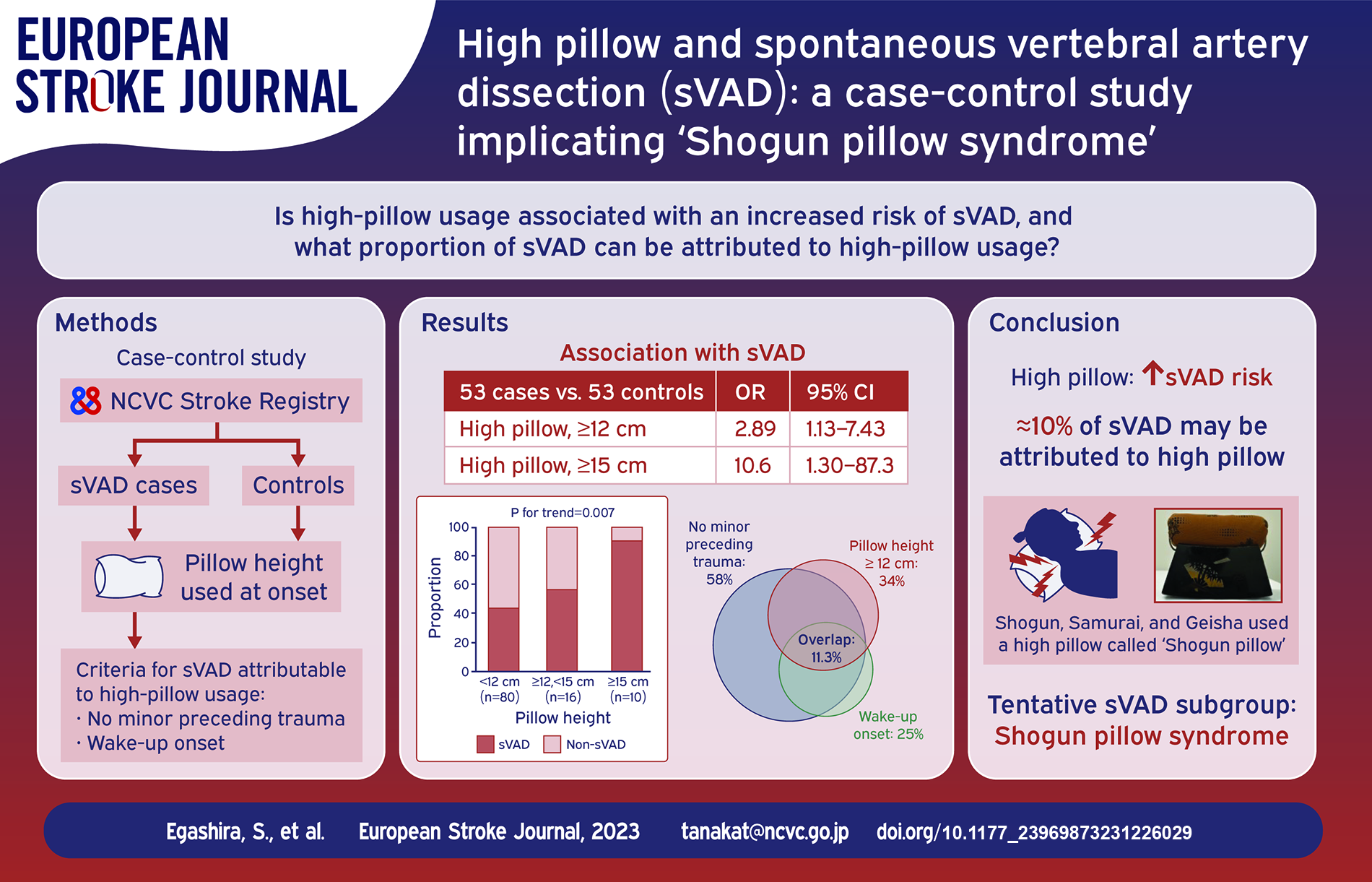
The underlying causes of spontaneous vertebral artery dissection (sVAD) remain insufficiently understood. This study aimed to determine whether high-pillow usage is associated with an increased risk of sVAD and evaluate the frequency of sVAD attributable to high-pillow usage.
This case-control study identified patients with sVAD and age- and sex-matched non-sVAD controls (case-to-control ratio: 1:1) treated at a certified comprehensive stroke center in Japan between 2018 and 2023. The pillow height used at the onset of the index disease was measured and classified into three categories between 12 and 15 cm boundaries. Univariable logistic regression was performed to assess the odds ratio (OR) with a 95% confidence interval (CI) of high-pillow usage for sVAD development. A subgroup of sVAD attributable to high-pillow usage was defined with the following three conditions: high-pillow usage (⩾12 or ⩾15 cm); no minor preceding trauma; and wake-up onset.
Fifty-three patients with sVAD and 53 non-sVAD controls (42% women, median age: 49 years) were identified. High-pillow usage (⩾12 and ⩾15 cm) was more common in the sVAD group than in the non-sVAD group (34 vs 15%; OR = 2.89; 95%CI = 1.13–7.43 and 17 vs 1.9%; OR = 10.6; 95%CI = 1.30–87.3, respectively). The subgroup of sVAD attributed to high-pillow usage (⩾12 and ⩾15 cm) was found in 11.3% (95%CI = 2.7%–19.8%) and 9.4% (95%CI = 1.5%–17.3%), respectively.
High-pillow usage was associated with an increased risk of sVAD and accounted for approximately 10% of all sVAD cases. This tentative subgroup of sVAD may represent a distinct spectrum of disease—Shogun pillow syndrome.
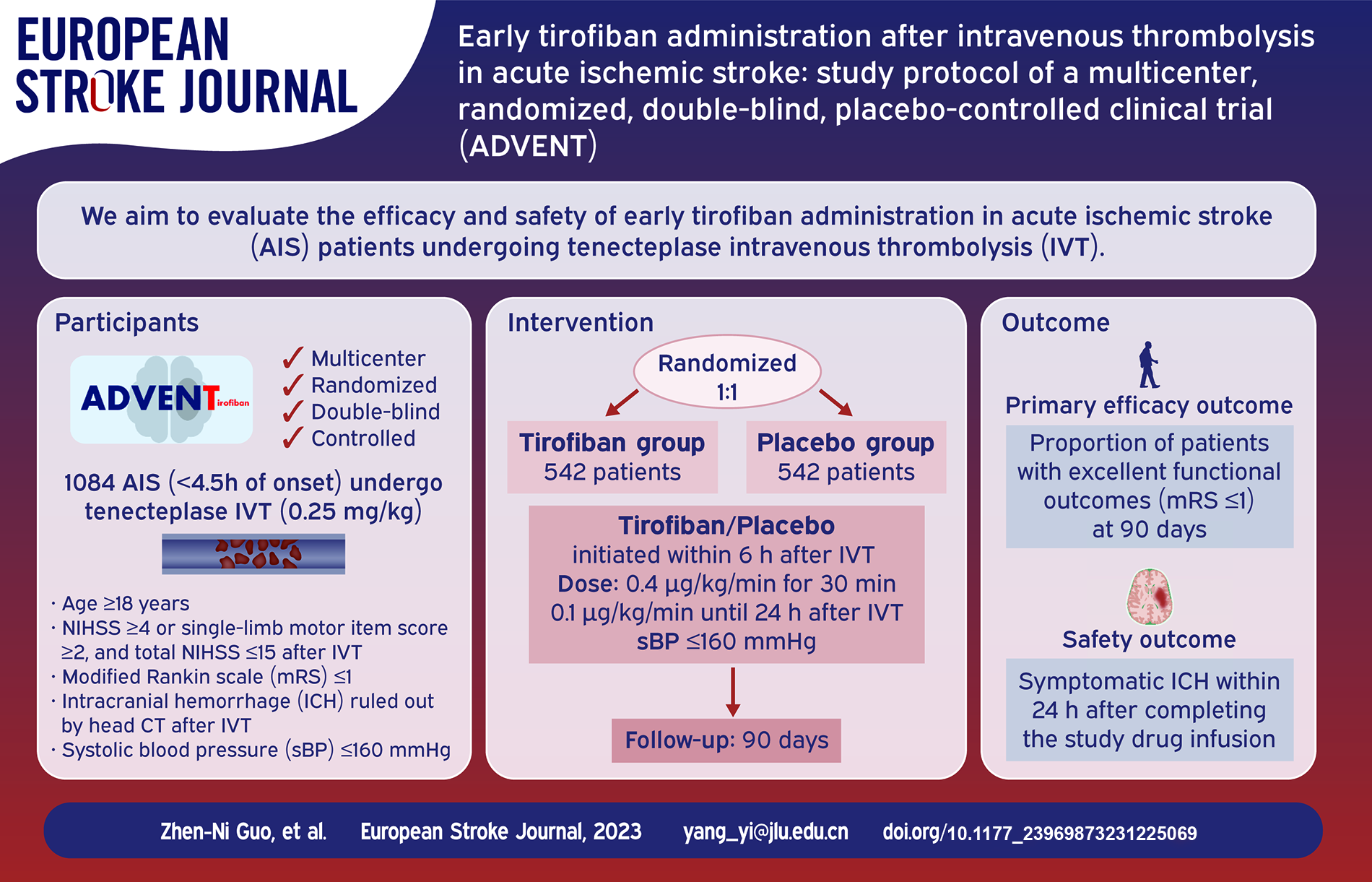
Nearly half of patients with acute ischemic stroke who undergo intravenous thrombolysis (IVT) fail to achieve excellent functional outcomes. Early administration of tirofiban after IVT may improve patient outcomes.
To evaluate the efficacy and safety of early tirofiban administration after intravenous tenecteplase in patients with acute ischemic stroke.
The ADVENT trial is a multicenter, randomized, parallel-controlled, double-blind clinical trial. A total of 1084 patients undergoing IVT without subsequent endovascular treatment will be recruited from multiple hospitals in China. Subjects will be randomized in a 1:1 ratio to receive tirofiban or placebo, which will be infused within 6 h after IVT until 24 h after IVT, at 0.4 μg/kg/min for 30 min and then at 0.1 μg/kg/min. The primary efficacy outcome is the proportion of patients with excellent functional outcomes (modified Rankin Scale (mRS) ⩽ 1) at 90 days. Secondary outcomes include the proportion of patients with favorable functional outcomes (mRS ⩽ 2) at 90 days and neurological functional assessments evaluated during hospitalization. Symptomatic intracranial hemorrhage will be the primary safety outcome. Mortality and other adverse events will be recorded.
This pivotal trial will provide important data on the early administration of antiplatelet therapy after IVT and may promote progress in treatment standards.
ClinicalTrials.gov (NCT06045156)