Adham Ahmed, Kathryn S. Varghese, Peter J. Fusco , [...]
View All
Abstract
Objective:
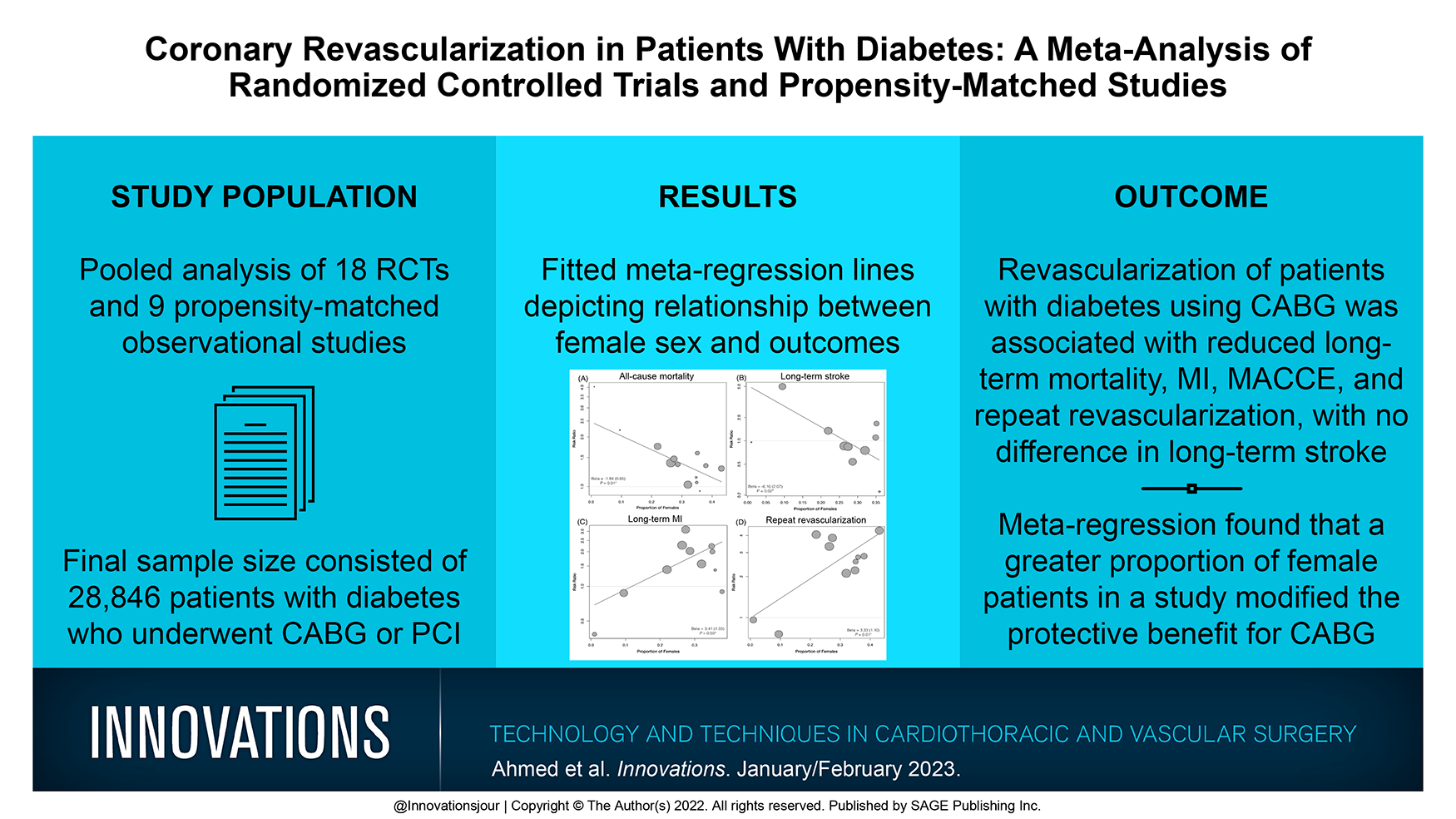
Patients with diabetes have poorer outcomes with coronary artery disease (CAD) and pose a unique clinical population for revascularization. We performed a pairwise meta-analysis of randomized trials (RCTs) and propensity-matched observational studies (PMS) to compare the clinical outcomes of coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) in patients with diabetes.
Methods:
A comprehensive literature search was performed to identify RCT and PMS studies comparing CABG with PCI in patients with diabetes with concurrent CAD. Studies were pooled using the random-effects model to perform a pairwise meta-analysis. Primary outcomes included long-term all-cause mortality, cardiac mortality, myocardial infarction (MI), major adverse cardiac and cerebrovascular events (MACCE), and repeat revascularization. Meta-regression was used to explore the effects of baseline risk factors on primary outcomes with moderate to high heterogeneity.
Results:
A total of 18 RCTs and 9 PMS with 28,846 patients were included. PCI was associated with increased long-term all-cause mortality (risk ratio [RR] = 1.34, P < 0.001), cardiac mortality (RR = 1.52, P < 0.001), MI (RR = 1.51, P = 0.009), MACCE (RR = 1.65, P < 0.001), and repeat revascularization (RR = 2.48, P < 0.001) compared with CABG. There was no difference in long-term stroke between the 2 groups (RR = 0.95, P = 0.82). At meta-regression, a greater proportion of female patients in studies was associated with a decreased protective benefit for CABG for long-term all-cause mortality but an increased protective benefit for long-term MI and repeat revascularization.
Conclusions:
Revascularization of patients with diabetes using CABG is associated with significantly reduced long-term mortality, MI, MACCE, and repeat revascularizations. Future studies exploring the influence of gender on revascularization outcomes are necessary to elucidate the ideal treatment modality in patients with diabetes.
Review article
Restricted accessReview articleFirst published January, 2023pp. 41-48
In the field of modern cardiothoracic surgery, chest drainage has become ubiquitous and yet characterized by a wide variation in practice. Meanwhile, the evolution of chest drain technology has created gaps in knowledge that represent opportunities for new research to support the development of best practices in chest drain management. The chest drain is an indispensable tool in the recovery of the cardiac surgery patient. However, decisions about chest drain management—including those about type, material, number, maintenance of patency, and the timing of removal—are largely driven by tradition due to a scarcity of quality evidence. This narrative review surveys the available evidence regarding chest-drain management practices with the objective of highlighting scientific gaps, unmet needs, and opportunities for further research.
Research article
Restricted accessResearch articleFirst published January, 2023pp. 49-57
Rochelle Prokupets, Nivedha Kannapadi, Henry Chang , [...]
View All
Abstract
Objective:
Despite the common occurrence of extracorporeal membrane oxygenation (ECMO)–associated acute ischemic stroke (AIS) and intracranial hemorrhage (ICH), there are little data to guide optimal anticoagulation management. We sought to describe antithrombotic therapy management after stroke and outcomes.
Methods:
A retrospective analysis was conducted of venoarterial (VA) and venovenous (VV) ECMO patients treated at a tertiary care center from June 2016 to February 2021. Patients with image-confirmed diagnosis of AIS or ICH while receiving ECMO were included for study with data collected regarding anticoagulation management and clinical outcomes.
Results:
Overall, 216 patients (153 VA-ECMO, 63 VV-ECMO) were included in this study. Of the 153 patients on VA-ECMO, 13 (8.4%) had AIS and 6 (3.9%) had ICH. Of the 63 patients on VV-ECMO, none had AIS and 5 (7.9%) had ICH. One patient (9%) received anticoagulation reversal after ICH. Anticoagulation was discontinued and later resumed in all 5 ICH survivors (median cessation time, 30 h) and 1 of 2 (50%) AIS survivors (median cessation time, 96 h). While off anticoagulation, 2 of 11 patients (18%) had thromboembolic events and none had new AIS. Upon resumption, there were no cases of hemorrhagic transformation of AIS or ICH expansion. There was no difference in in-hospital mortality between patients with ICH and those without in both the VA-ECMO and VV-ECMO cohorts nor between VA-ECMO patients with AIS and those without.
Conclusions:
Early cessation and judicious resumption of anticoagulation appeared feasible in the cohort of patients with ECMO-associated AIS and ICH.
Research article
Restricted accessResearch articleFirst published January, 2023pp. 58-66
Ahmed AlnajarORCID, Yingyot AroraORCID, Kelley N. Benck , [...]
View All
Abstract
Objective:
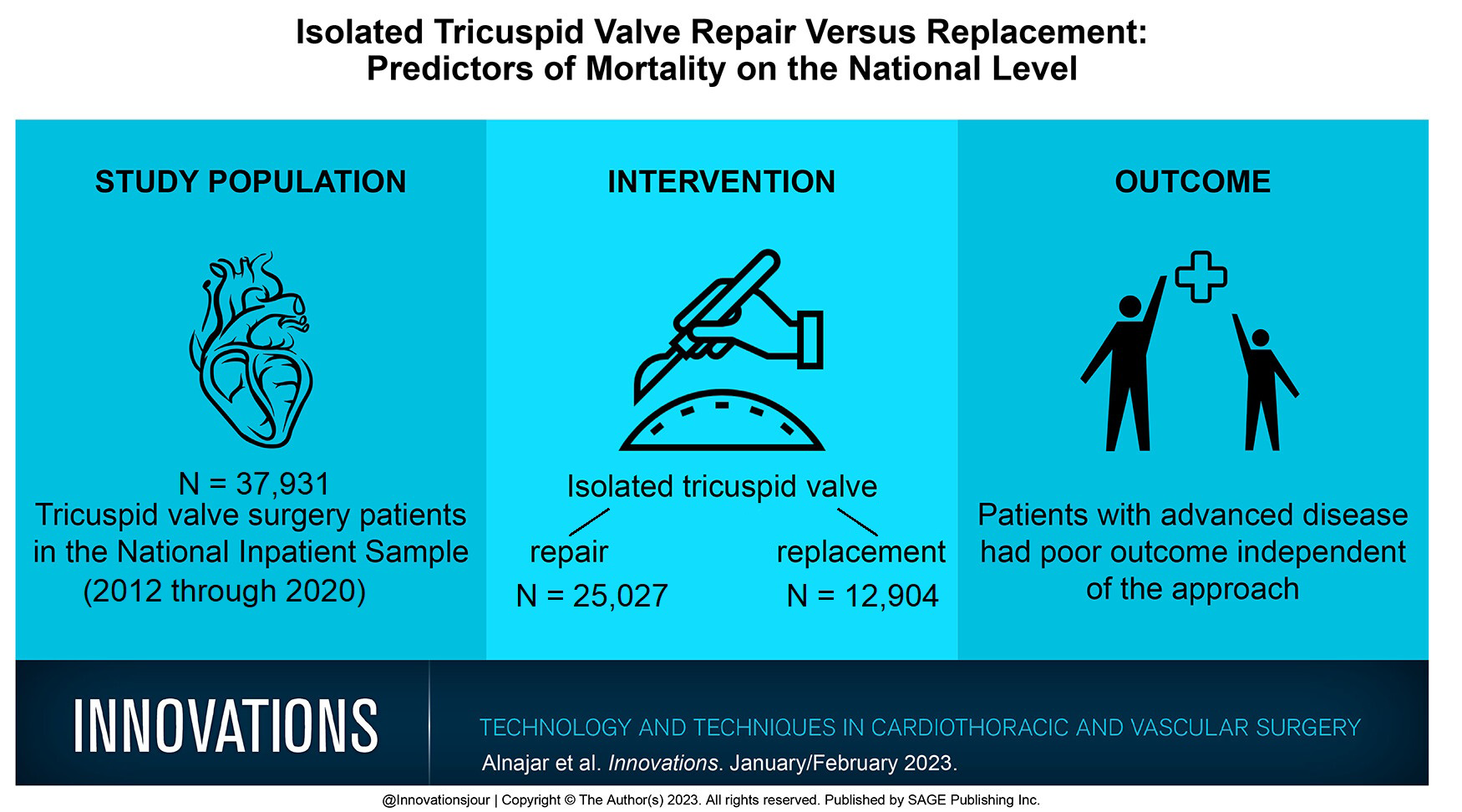
Isolated tricuspid valve surgery (TVR) is rarely performed, and literature reports are confined to small sample sizes and old studies. Thus, the advantage of repair over replacement could not be determined. We aimed to evaluate repair and replacement outcomes along with predictors of mortality for TVR on a national level.
Methods:
All adult patients (18+ years old) who underwent TVR from 2011 to 2020 were identified using the National Inpatient Sample dataset. The primary outcome was in-hospital mortality. Secondary outcomes included complications, length of stay (LOS), hospitalization cost, and discharge disposition.
Results:
Over a 10-year period, 37,931 patients had TVR and predominantly underwent repair (n = 25,027, 66.0%). In comparison with patients who underwent tricuspid replacement, more patients with a history of liver disease and pulmonary hypertension presented for repair surgery, and fewer patients had endocarditis and rheumatic valve disease (P < 0.001). The repair group had less mortality, less stroke, shorter LOS, and reduced cost, while the replacement group had fewer myocardial infarctions (P < 0.05). However, the outcomes were not different for cardiac arrest, wound complications, or bleeding. After excluding congenital TV disease and adjusting for relevant factors, TV repair was associated with a reduced in-hospital mortality by 28% (adjusted odds ratio [aOR] = 0.72, P = 0.011). Older age increased mortality risk by 3-fold, prior stroke by 2-fold, and liver diseases by 5-fold (P < 0.001). Patients undergoing TVR in recent years had a better chance of survival (aOR = 0.92, P < 0.001).
Conclusions:
TV repair has better outcomes than replacement does. Patient comorbidities and late presentation play an independently significant role in determining outcomes.
Research article
Restricted accessResearch articleFirst published January, 2023pp. 67-72
Ira Goldsmith, Lawrence Dovgalski, Peter Llewelyn Evans
Abstract
Objective:
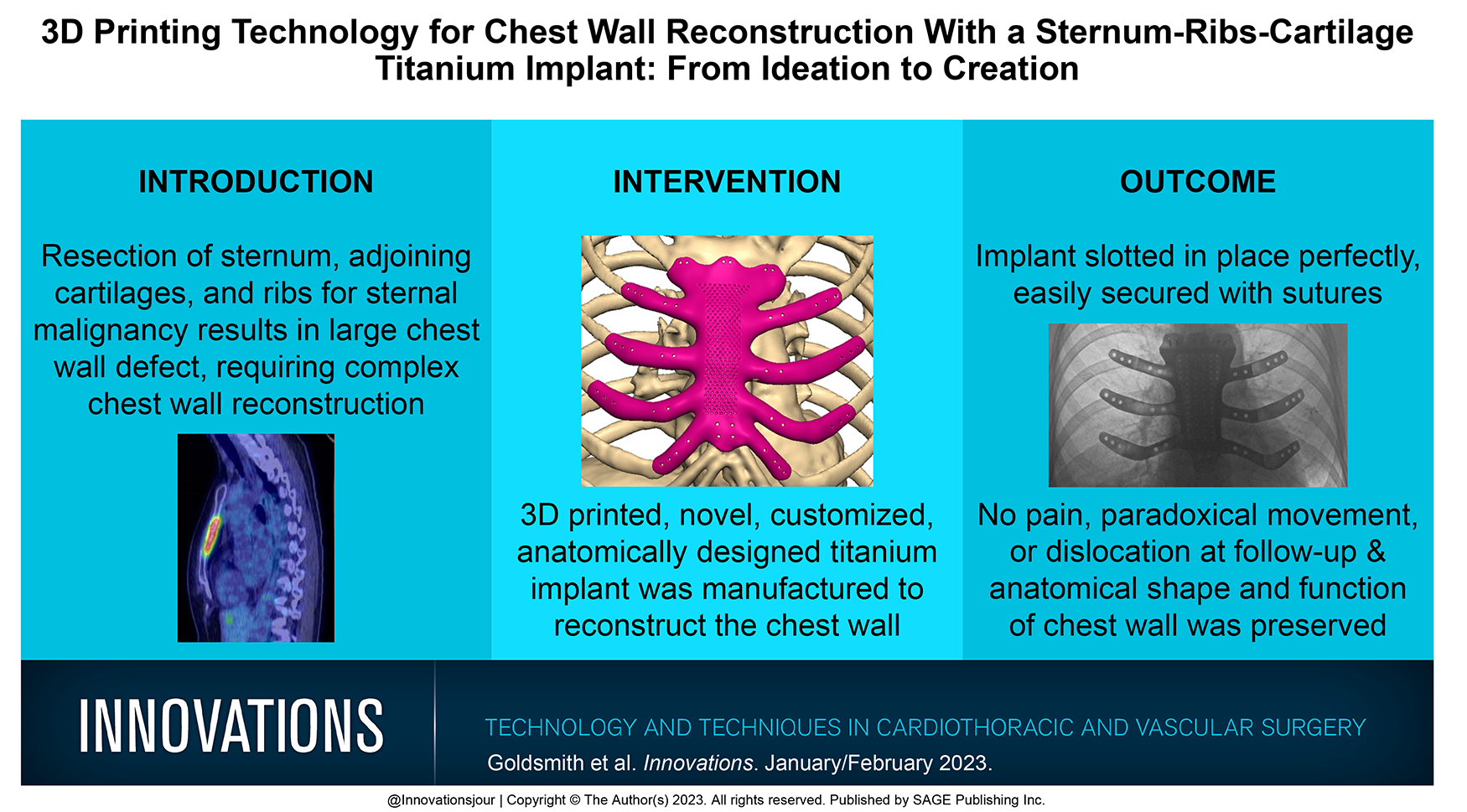
We describe the use of 3-dimensional (3D) printing technology to plan and reconstruct the sternum, adjoining cartilages, and ribs with a custom-made, anatomically designed, 3D-printed titanium implant for an isolated sternal metastasis complicated with a pathological fracture.
Methods:
We imported submillimeter slice computed tomography scan data into Mimics Medical 20.0 software and by manual bone threshold segmentation created a 3D virtual model of the patient’s chest wall and tumor. For all-around tumor-free margins, we grew the tumor by 2 cm. The replacement implant was designed in 3D using the anatomical features of the sternum, cartilages, and ribs and manufactured using TiMG 1 powder fusion technology. Physiotherapy was provided prior to and following surgery, and the impact of reconstruction on pulmonary functions was assessed.
Results:
At surgery, the precise resection, clear margins, and a secure fit were achieved. At follow-up, there was no dislocation, paradoxical movement, change in performance status, or dyspnea. There was a decrease in forced expiratory volume in 1 s (FEV1) from 105% prior to surgery to 82% following surgery and in forced vital capacity (FVC) from 108% to 75%, with no difference in the FEV1/FVC ratio, suggesting a restrictive pattern of impairment.
Conclusions:
With 3D printing technology, reconstructing a large anterior chest wall defect with a custom-made, anatomical, 3D-printed titanium alloy implant is feasible and safe, and it preserves the shape, structure, and function of the chest wall, albeit with a restrictive pattern of pulmonary function, which can be addressed with physiotherapy.
Research article
Open accessResearch articleFirst published January, 2023pp. 73-79
Anne R. de Jong, Monica Gianoli, Hanae F. Namba , [...]
View All
Abstract
Objective:
Robot-assisted minimally invasive direct coronary artery bypass (RA-MIDCAB) surgery and hybrid coronary revascularization (HCR) are minimally invasive alternative strategies to conventional coronary artery bypass surgery in patients with isolated left anterior descending (LAD) stenosis or multivessel coronary disease. We analyzed a large, multicenter data-set based on the Netherlands Heart Registration including all patients undergoing RA-MIDCAB.
Methods:
We included 440 consecutive patients who underwent RA-MIDCAB with the left internal thoracic artery to LAD between January 2016 and December 2020. A proportion of patients underwent percutaneous coronary intervention (PCI) of non-LAD vessels (i.e., HCR). The primary outcome was all-cause mortality at median follow-up of 1 year, which was subdivided into cardiac and noncardiac. Secondary outcomes included target vessel revascularization (TVR) at median follow-up as well as 30-day mortality, perioperative myocardial infarction, reoperation for bleeding or anastomosis-related problems, and in-hospital ischemic cerebrovascular accident (iCVA).
Results:
Among all patients, 91 (21%) underwent HCR. At median (IQR) follow-up of 19 (8 to 28) months, 11 patients (2.5%) had died. In 7 patients, the cause of death was defined as cardiac. TVR occurred in 25 patients (5.7%), of whom 4 underwent CABG and 21 underwent PCI. At 30-day follow-up, 6 patients (1.4%) had a perioperative myocardial infarction, of whom 1 died. One patient (0.2%) developed an iCVA, and 18 patients (4.1%) underwent reoperation for bleeding or anastomosis-related problems.
Conclusions:
The clinical outcomes of patients undergoing RA-MIDCAB or HCR in the Netherlands are good and promising when compared with the currently available literature.
Research article
Restricted accessResearch articleFirst published January, 2023pp. 80-83
Boris Robič, Rene Petrovič, Anže Djordjević , [...]
View All
Abstract
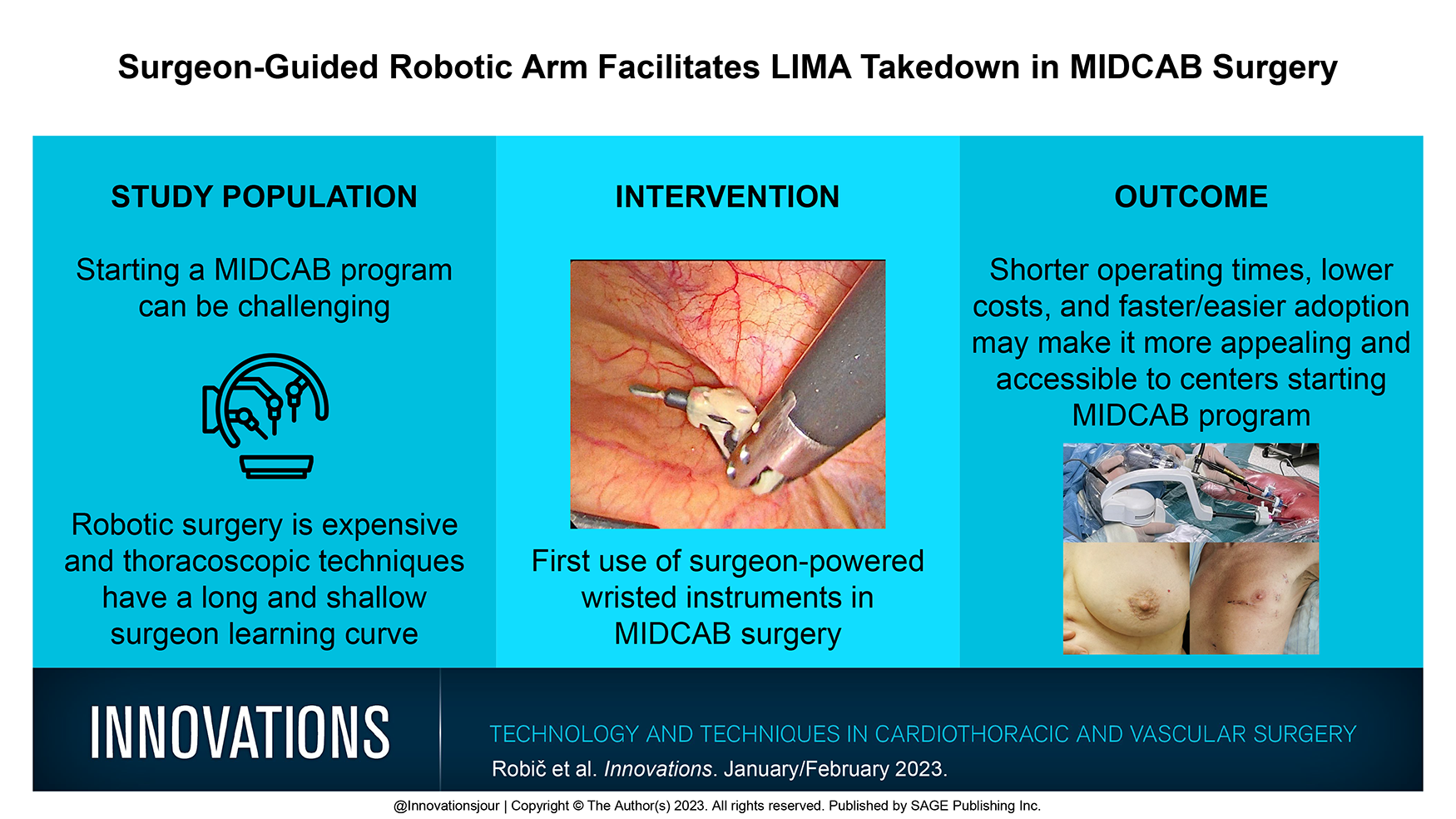
Left internal mammary artery (LIMA) to left anterior descending (LAD) coronary artery bypass has been scientifically proven to have the best patency and long-term results in myocardial revascularization. The latest guidelines suggest minimally invasive LIMA to LAD is the optimal therapy for isolated proximal LAD lesions. The start of a minimally invasive direct coronary artery bypass (MIDCAB) program can be quite challenging as robotic surgery demands high starting costs, while normal thoracoscopic techniques have a longer surgeon learning curve. In this article, we describe to the best of our knowledge the first use of surgeon-guided wristed instruments in LIMA harvesting for MIDCAB surgery. It allows for a facilitated LIMA harvest like in robotic surgery with the comfort of a surgeon constantly standing by the patient, allowing for a faster response time in case of an emergency or the need for instrument exchange. These features result in shorter operating times, lower costs compared with robotic surgery, and faster adoption of this technique for centers just starting MIDCAB surgery.
Research article
Restricted accessResearch articleFirst published January, 2023pp. 84-89
Joseph A. RezaORCID, Charles BakhosORCID, Stacey Su , [...]
View All
Abstract
Objective:
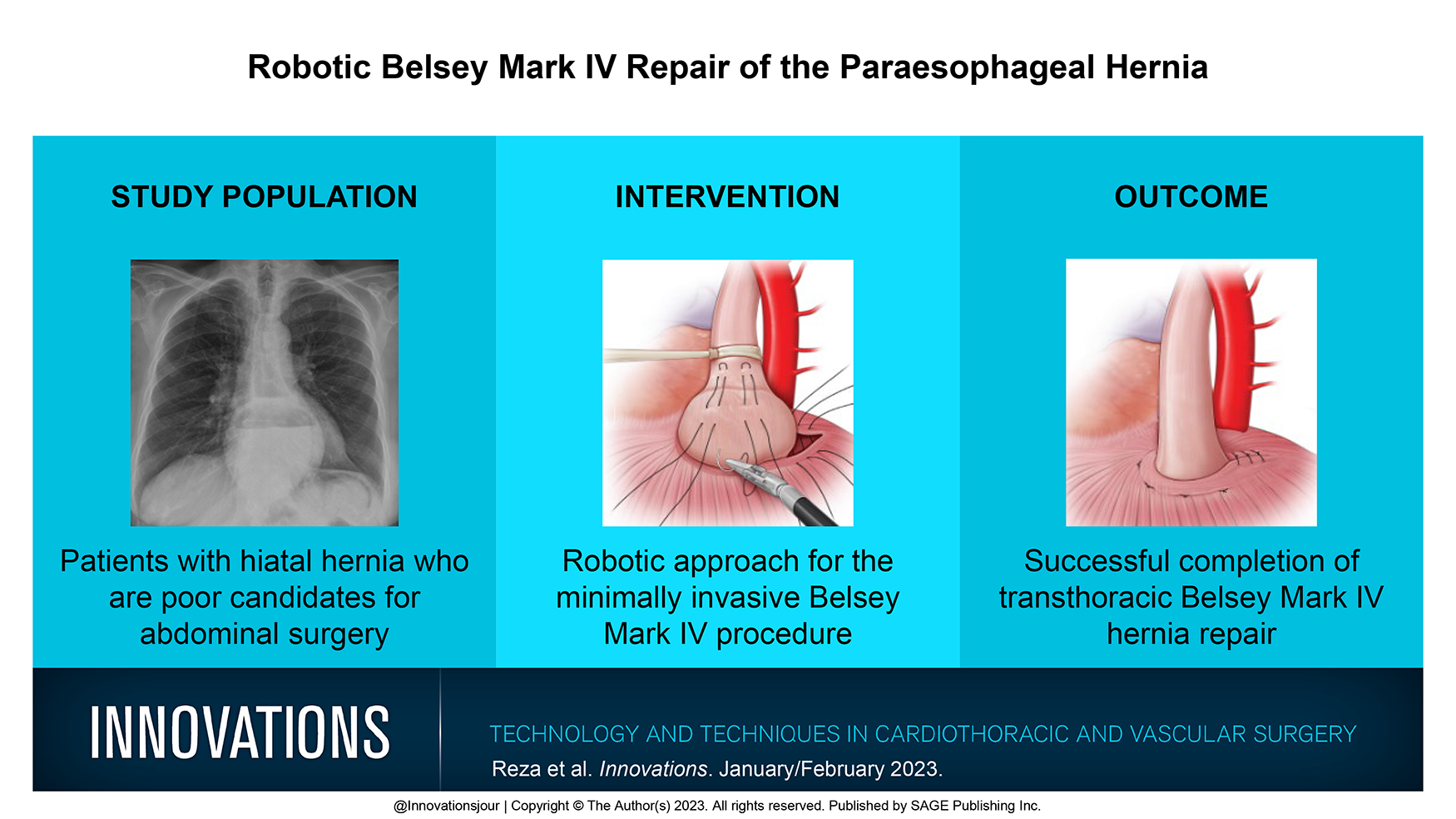
Surgical repair of paraesophageal hernias in patients with hostile abdomen is challenging. Despite its utility as an open procedure, the adoption of the minimally invasive Belsey Mark IV procedure has been limited because of the complexity of using traditional video-assisted thoracoscopic instrumentation. The robotic platform offers additional degrees of freedom, which enables minimally invasive transthoracic approach despite challenging anatomy. The purpose of this article is to describe a technique of robotic approach for the Belsey Mark IV operation.
Methods:
We retrospectively reviewed 5 cases of the robotic Belsey Mark IV procedure completed at a single institution between June 2018 and November 2021. Data were collected from a review of the medical records, including operative reports, anesthesia records, imaging, and clinical notes. The operative technique is described in the present article. There were 4 men and 1 woman. The average age of the patients was 64.4 ± 13.6 years, with an average body mass index of 24.5 kg/m2. Three patients had undergone previous transabdominal hiatal hernia repair, and 2 of them had 2 prior repairs. One patient underwent simultaneous pulmonary left lower lobectomy for cancer with the Belsey Mark IV procedure.
Results:
The average operative time was 209 ± 95 min (110 to 360 min). The average postoperative length of stay was 4.2 days, and 2 patients experienced complications including bleeding and persistent air leak (after lobectomy). The average blood loss was 67 ± 25 mL.
Conclusions:
The robotic platform enables a transthoracic minimally invasive approach to the Belsey Mark IV operation.
Research article
Restricted accessResearch articleFirst published January, 2023pp. 90-96
Daisuke Kaneyuki, Colin C. YostORCID, Kellen Round , [...]
View All
Abstract
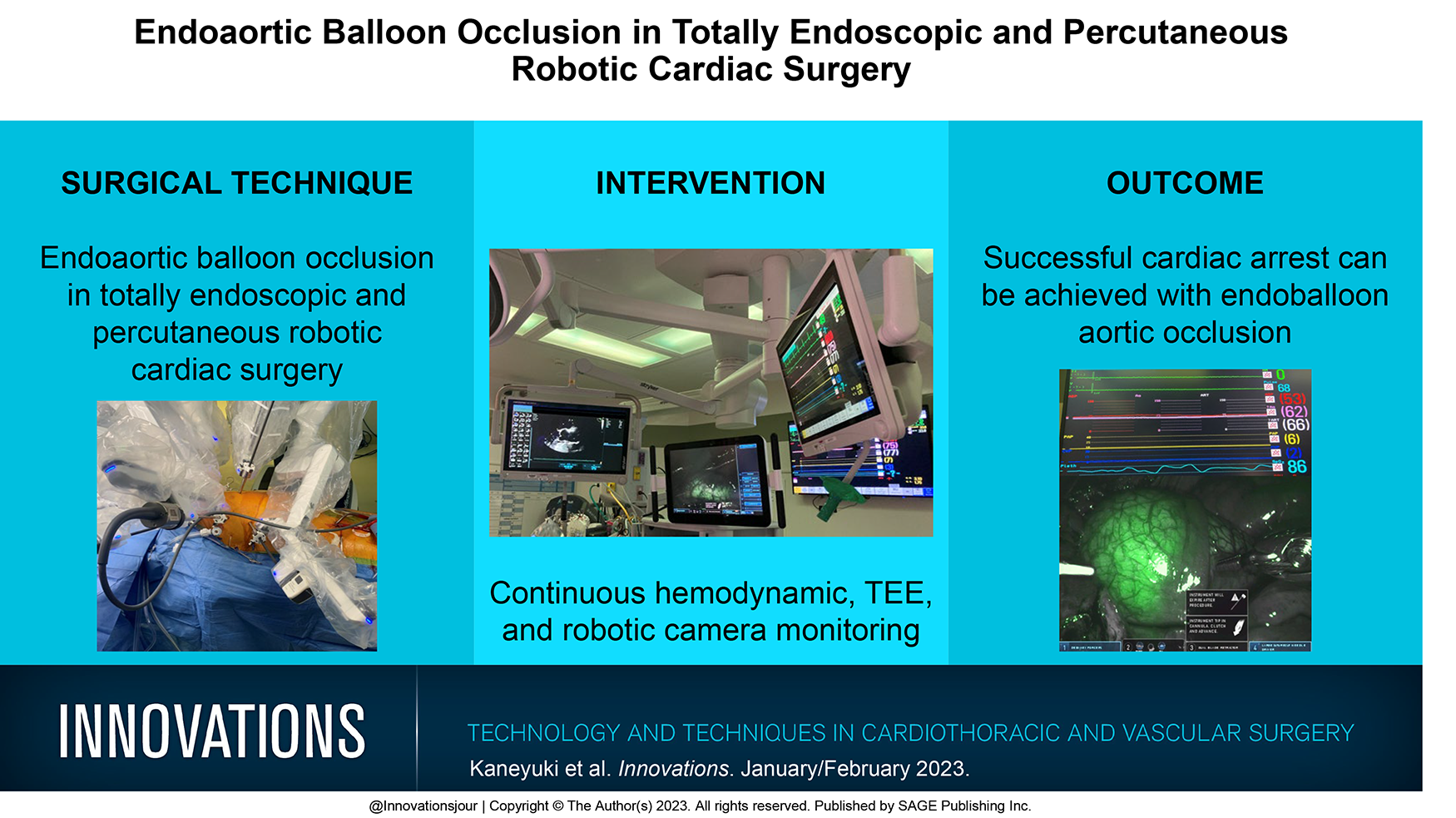
Previous studies have shown that the endoaortic balloon occlusion (EABO) can provide satisfactory aortic cross-clamping with comparable surgical outcomes to thoracic aortic clamping in the setting of minimally invasive and robotic cardiac surgery. We described our approach to EABO use in totally endoscopic and percutaneous robotic mitral valve surgery. Preoperative computed tomography angiography is required to evaluate the quality and size of the ascending aorta, identify access sites for peripheral cannulation and endoaortic balloon insertion, and screen for other vascular anomalies. Continuous bilateral upper extremity arterial pressure and cranial near-infrared spectroscopy monitoring are essential to detect obstruction of the innominate artery due to distal balloon migration. Transesophageal echocardiography is needed for continuous monitoring of balloon positioning and antegrade cardioplegia delivery. Direct fluorescent visualization of the endoaortic balloon on the robotic camera allows for verification of balloon and efficient repositioning if needed. The surgeon should assess hemodynamic and imaging information simultaneously during the balloon inflation and delivery of antegrade cardioplegia. Aortic root pressure, systemic blood pressure, and balloon catheter tension affect the position of the inflated endoaortic balloon in the ascending aorta. The surgeon should eliminate all slack in the balloon catheter and lock it into position to prevent proximal balloon migration after the completion of antegrade cardioplegia. Using scrupulous preoperative imaging assessment and continuous intraoperative monitoring, the EABO can achieve adequate cardiac arrest in totally endoscopic robotic cardiac surgery, even in patients with previous sternotomy without compromise of surgical outcomes.
Case report
Restricted accessCase reportFirst published January, 2023pp. 97-99
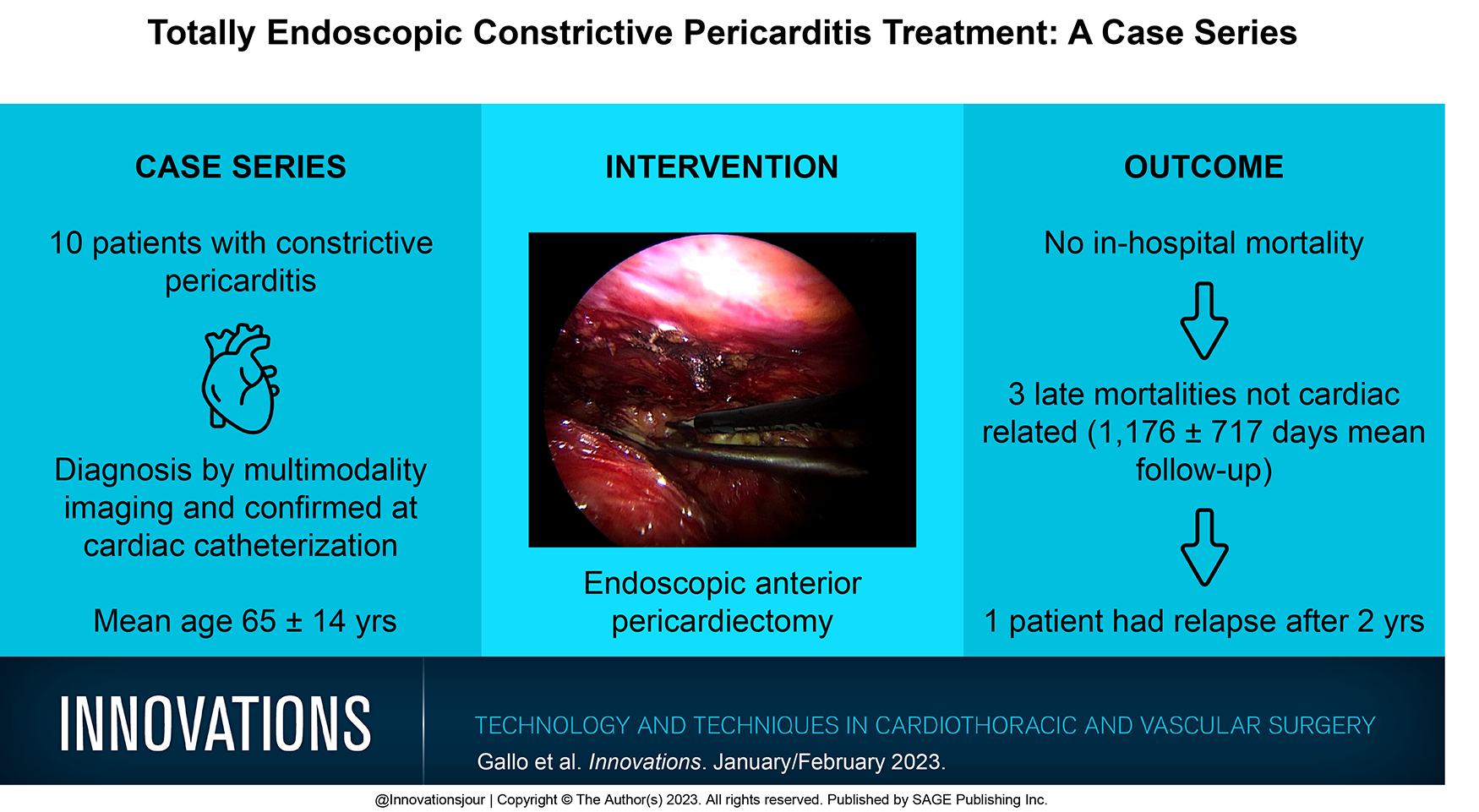
Michele GalloORCID, Giovanni Domenico Cresce, Alessandro Favaro , [...]
View All
Abstract
Minimally invasive cardiac surgery has increased in popularity to reduce the morbidity associated with open heart surgery. In this article, a totally endoscopic case series is presented in which anterior pericardiectomy is performed by peripheral femoral arterial and venous cannulation. Right periareoal incision and right submammary incision were used for male and female patients, respectively, to access the heart by the fourth intercostal space.
Brief report
Open accessBrief reportFirst published January, 2023pp. 100-102
Kyle G. Mitchell, Blaz Podgorsek, Diego E. Fiorito , [...]
View All
Abstract
The application of robot-assisted thoracoscopy to cardiac surgery affords an opportunity to leverage the exceptional intraoperative exposure, visualization, and dexterity of the robotic platform. Here, we report the case of a 72-year-old woman who presented to our institution for evaluation of a left ventricular mass that was identified following workup for an embolic event. We present an intraoperative video that provides technical details of the robot-assisted resection of the lesion, which was found to be a left ventricular papillary fibroelastoma arising from the mitral chordal apparatus. This case highlights the advantages provided by the robotic platform, which permitted complete, minimally invasive surgical excision of the lesion while minimizing the burden of surgical trauma.
Brief report
Restricted accessBrief reportFirst published January, 2023pp. 103-105
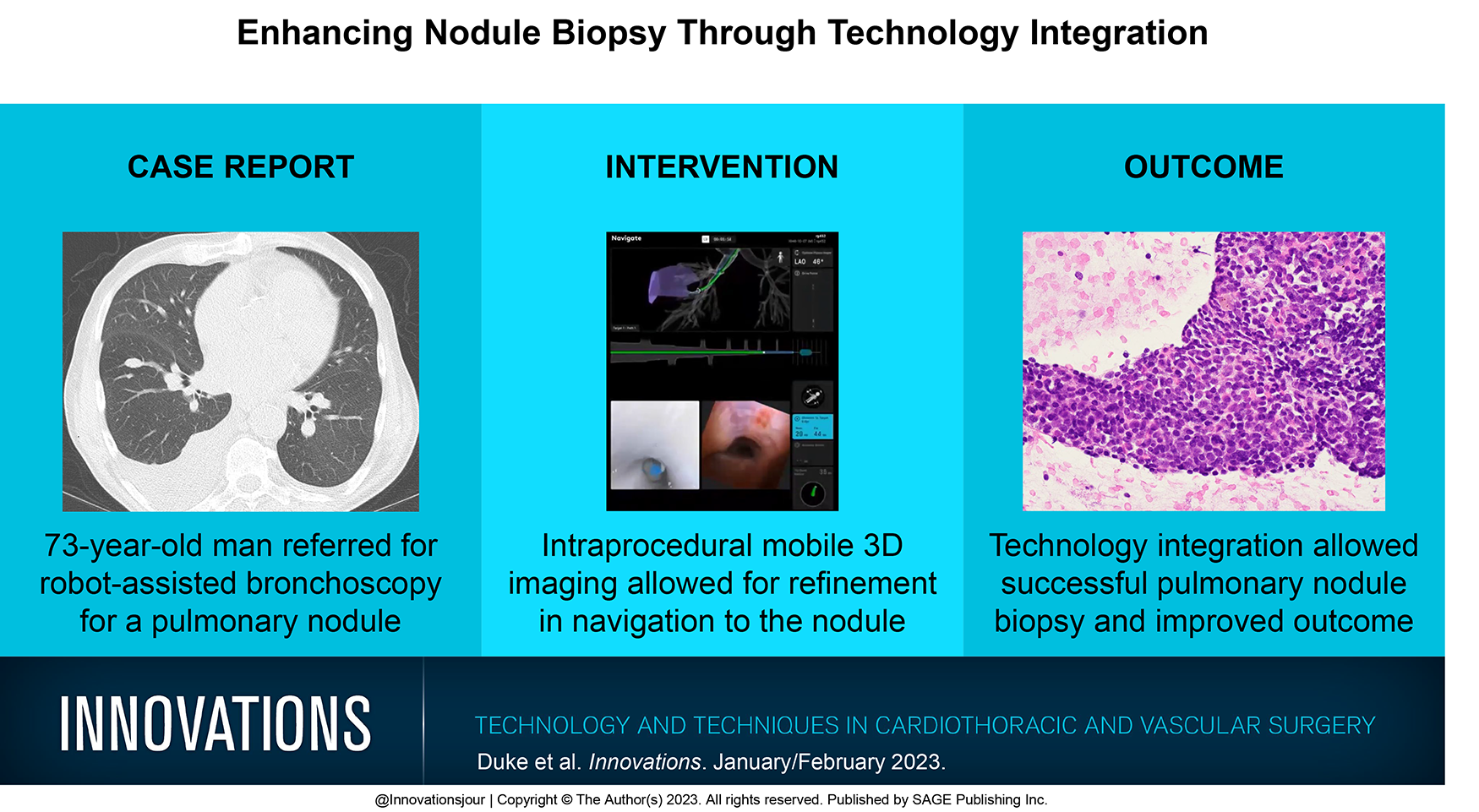
Jennifer D. Duke, David Sanborn, Janani Reisenauer
Abstract
Technology in navigating to peripheral pulmonary nodules has improved in recent years. The recent integration of a robotic platform using shape-sensing technology and mobile cone-beam computed tomography imaging technology has enhanced confidence in sampling lesions with intraprocedural imaging by complimenting the pre-planned navigation to peripheral pulmonary nodules. We present 2 cases using the software integration that improved the robotic catheter positioning to allow for diagnostic specimens to be obtained in the initial biopsies.