Yazan N. AlJamalORCID, Robert Burgin, Hiroto Kitahara , [...]
View All
Abstract
Objective:
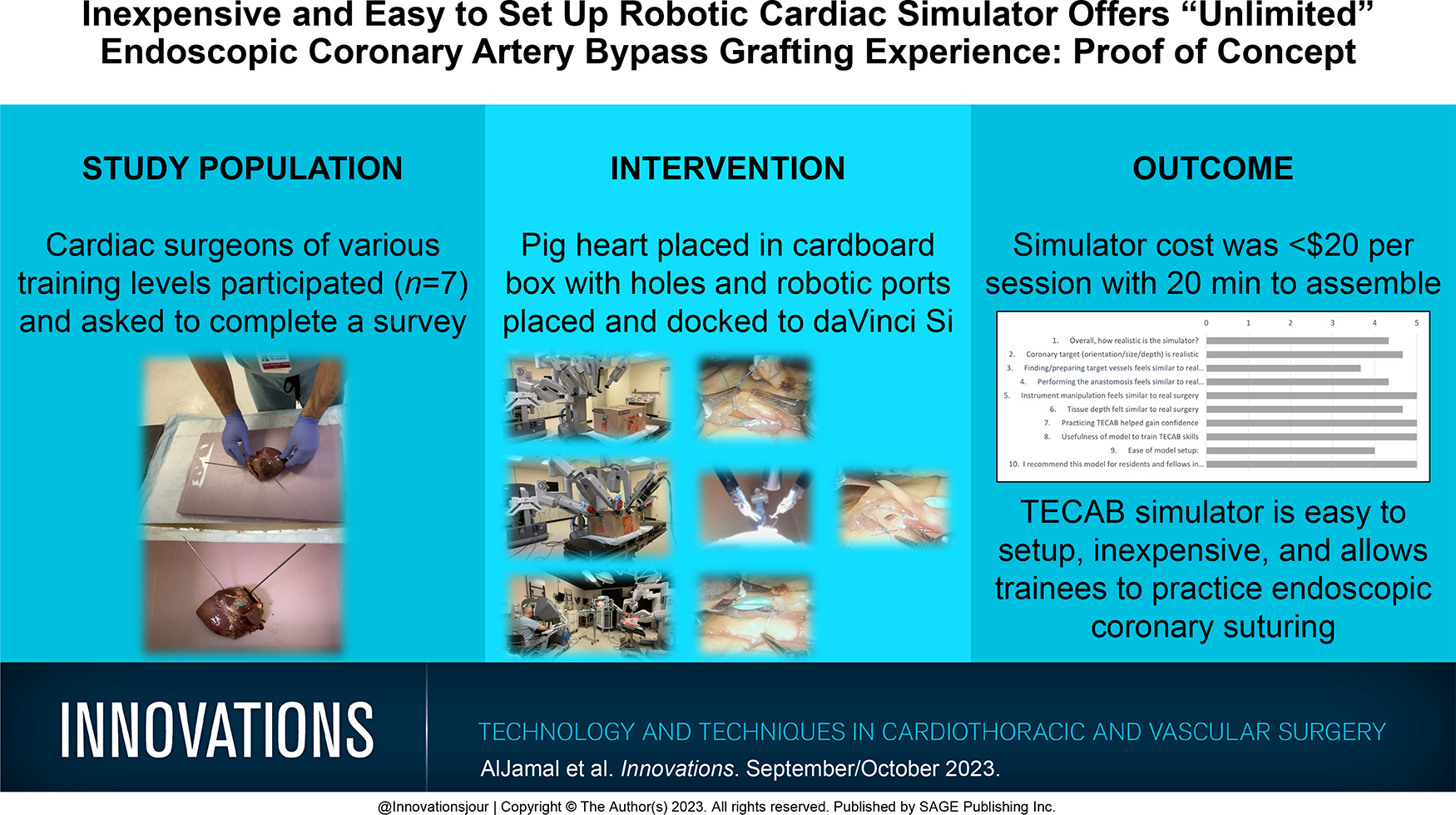
Robotic totally endoscopic coronary artery bypass (TECAB) grafting is the least invasive form of coronary bypass surgery. However, despite its advantages, this approach has not gained widespread adoption. One possible reason is the advanced and complex robotic skills required to execute a totally endoscopic sutured coronary anastomosis. We prepared a novel, inexpensive, easy to set up robotic TECAB simulator.
Methods:
A pig heart was placed in a cardboard box, and 3 holes were made on the side to mimic the exposure and surgical ergonomics of TECAB port placement. Four robotic ports were placed and docked to the da Vinci Si robot (Intuitive Surgical, Sunnyvale, CA, USA). Monofilament 7:0 suture (7 cm long) was used to perform the anastomosis to the left anterior descending artery using remnant conduit. Seven cardiac surgeons of various training levels participated and were asked to fill out a 10-point questionnaire.
Results:
The cost of the simulator totaled $20 per session, with 20 min to assemble. Each session allowed each trainee to practice 3 to 4 coronary anastomoses. Three cardiac surgeons completed the survey and strongly agreed that the model was easy to set up, the anastomotic exercise was realistic, and that this practice helped them gain confidence.
Conclusions:
Our TECAB simulator is inexpensive, easy to set up, and allows trainees to practice endoscopic coronary suturing. We believe this to be a valuable training tool to learn how to do TECAB for established surgeons and that such a simulator may be of great value to cardiothoracic training programs and their trainees. Further studies are warranted.
Review article
Restricted accessReview articleFirst published September, 2023pp. 424-434
Adham Ahmed, Ahmed K. Awad, Kathryn S. Varghese , [...]
View All
Abstract
Objective:
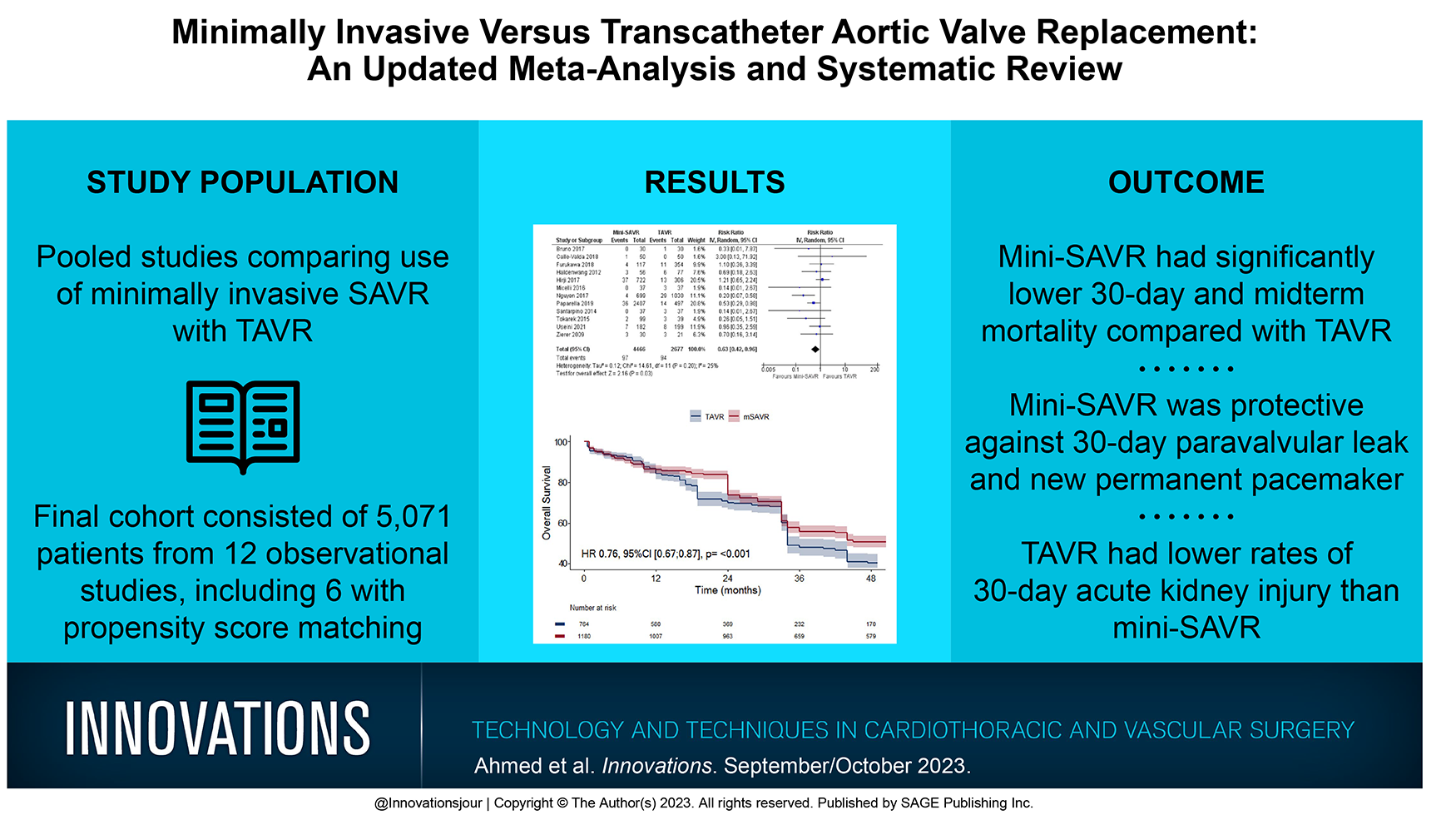
Transcatheter aortic valve replacement (TAVR) has arisen as a viable alternative to surgery. Similarly, minimally invasive surgical aortic valve replacement (mini-SAVR), such as ministernotomy and minithoracotomy, have also gained interest. We conducted a pairwise meta-analysis to further investigate the efficacy of TAVR versus mini-SAVR.
Methods:
Medical databases were comprehensively searched for studies comparing TAVR with a mini-SAVR modality, defined as minimally invasive aortic surgery, ministernotomy, minithoracotomy, or rapid-deployment or sutureless SAVR. Random-effects meta-analysis was conducted using the generic inverse variance method. Primary outcomes included 30-day mortality, midterm mortality, 30-day stroke, acute kidney injury (AKI), paravalvular leak (PVL), new permanent pacemaker (PPM), new-onset atrial fibrillation, and postintervention mean and peak valve pressure gradients and were pooled as risk ratio (RR), mean difference (MD), or hazard ratio (HR) with 95% confidence interval (CI).
Results:
A total of 5,071 patients (2,505 mini-SAVR vs 2,566 TAVR) from 12 studies were pooled. Compared with TAVR, mini-SAVR showed significantly lower rates of both 30-day (RR = 0.63, 95% CI: 0.42 to 0.96, P = 0.03) and midterm mortality at 4 years of follow-up (HR = 0.76, 95% CI: 0.67 to 0.87, P < 0.001). Furthermore, mini-SAVR was protective against 30-day PVL (RR = 0.07, 95% CI: 0.04 to 0.13, P < 0.001) and new PPM (RR = 0.25, 95% CI: 0.11 to 0.57, P < 0.001). Conversely, TAVR was protective against 30-day AKI (RR = 1.67, 95% CI: 1.20 to 2.32, P = 0.002) and postinterventional mean gradients (MD = 1.65, 95% CI: 0.25 to 3.05, P = 0.02). No difference was observed for 30-day stroke (RR = 0.84, 95% CI: 0.56 to 1.24, P = 0.38), new-onset atrial fibrillation (RR = 1.79, 95% CI: 0.93 to 3.44, P = 0.08), or postinterventional peak gradients (MD = 3.24, 95% CI: −1.10 to 7.59, P = 0.14).
Conclusions:
Compared with TAVR, mini-SAVR was protective against 30-day and midterm mortality, 30-day PVL, and new permanent pacemaker, while TAVR patients had lower 30-day AKI. Future randomized trials comparing the efficacy of mini-SAVR approaches with TAVR are needed.
Research article
Restricted accessResearch articleFirst published September, 2023pp. 435-444
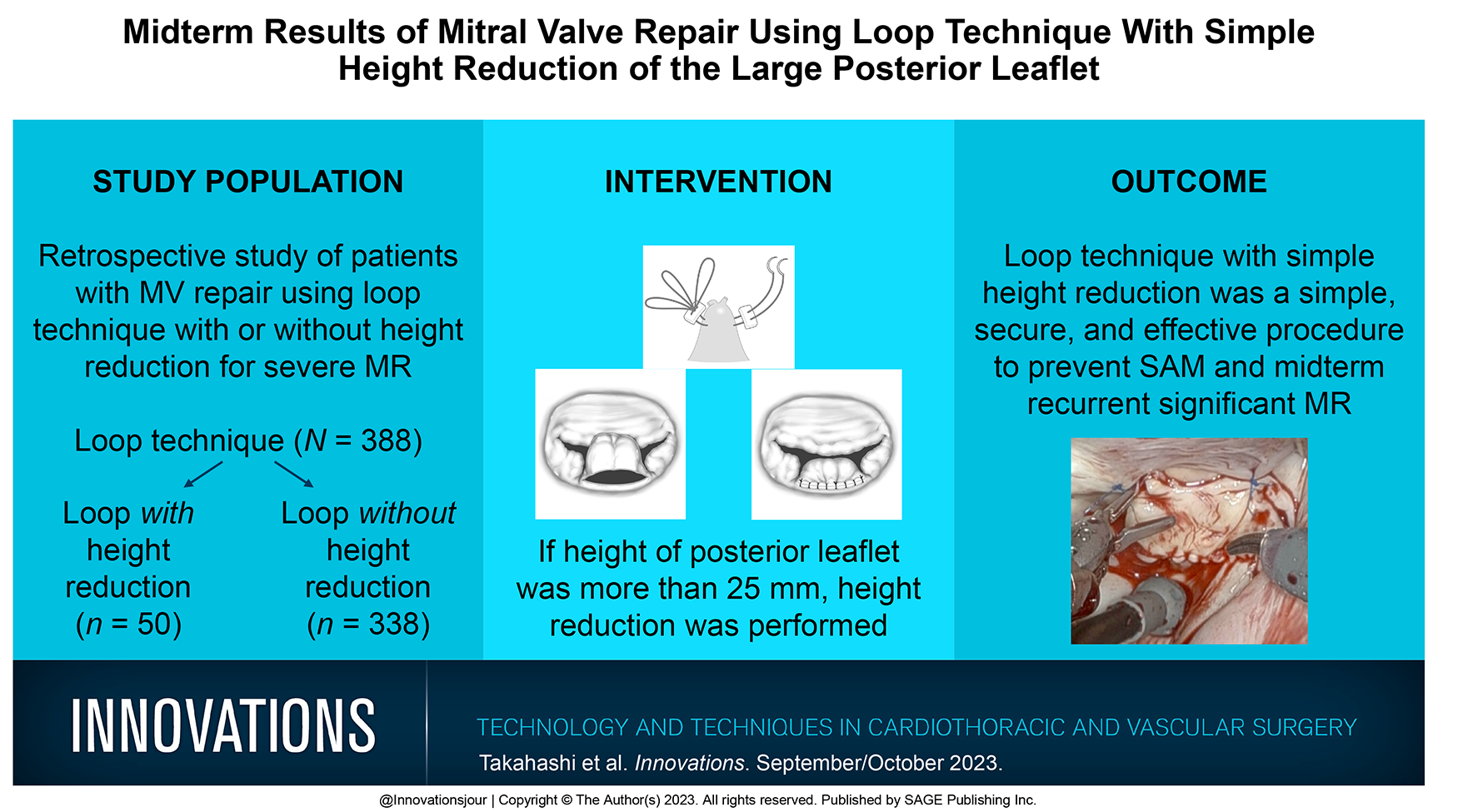
Systolic anterior motion (SAM) is one of the most serious problems in mitral valve repair. Height reduction is a key procedure to solve SAM, and there are limited data on the surgical results of height reduction procedure. This study is to assess the effectiveness and midterm results of simple height reduction procedure for SAM in patients with severe mitral regurgitation (MR).
Methods:
From 2008 to 2022, 50 patients underwent loop technique with an additional simple height reduction procedure for prevention of SAM. We examined the midterm results of patients with simple height reduction regarding recurrent MR and reoperation. The follow-up period ranged from 171 to 3,816 days (median, 883 days).
Results:
There were 338 patients (87%) who underwent loop technique without height reduction and 50 patients (13%) who underwent loop technique with height reduction. After the height reduction procedure, SAM was prevented in 44 patients, and 6 patients needed volume loading to suppress SAM. Freedom from recurrence of moderate to severe or severe MR at 1, 3, and 5 years was 98%, 88%, and 88% in the height reduction group versus 98%, 96%, and 94% in the group with loop technique alone (P = 0.074). Receiver operating characteristic curves showed that a systolic dimension of 26 mm had a sensitivity of 75% and a specificity of 83% for predicting SAM after height reduction.
Conclusions:
Loop technique with simple height reduction was a simple, secure, and effective procedure to prevent SAM and recurrent significant MR in the midterm periods.
Research article
Restricted accessResearch articleFirst published September, 2023pp. 445-451
Madelaine Hack, Katherine L. Wood, Milica Bjelic , [...]
View All
Abstract
Objective:
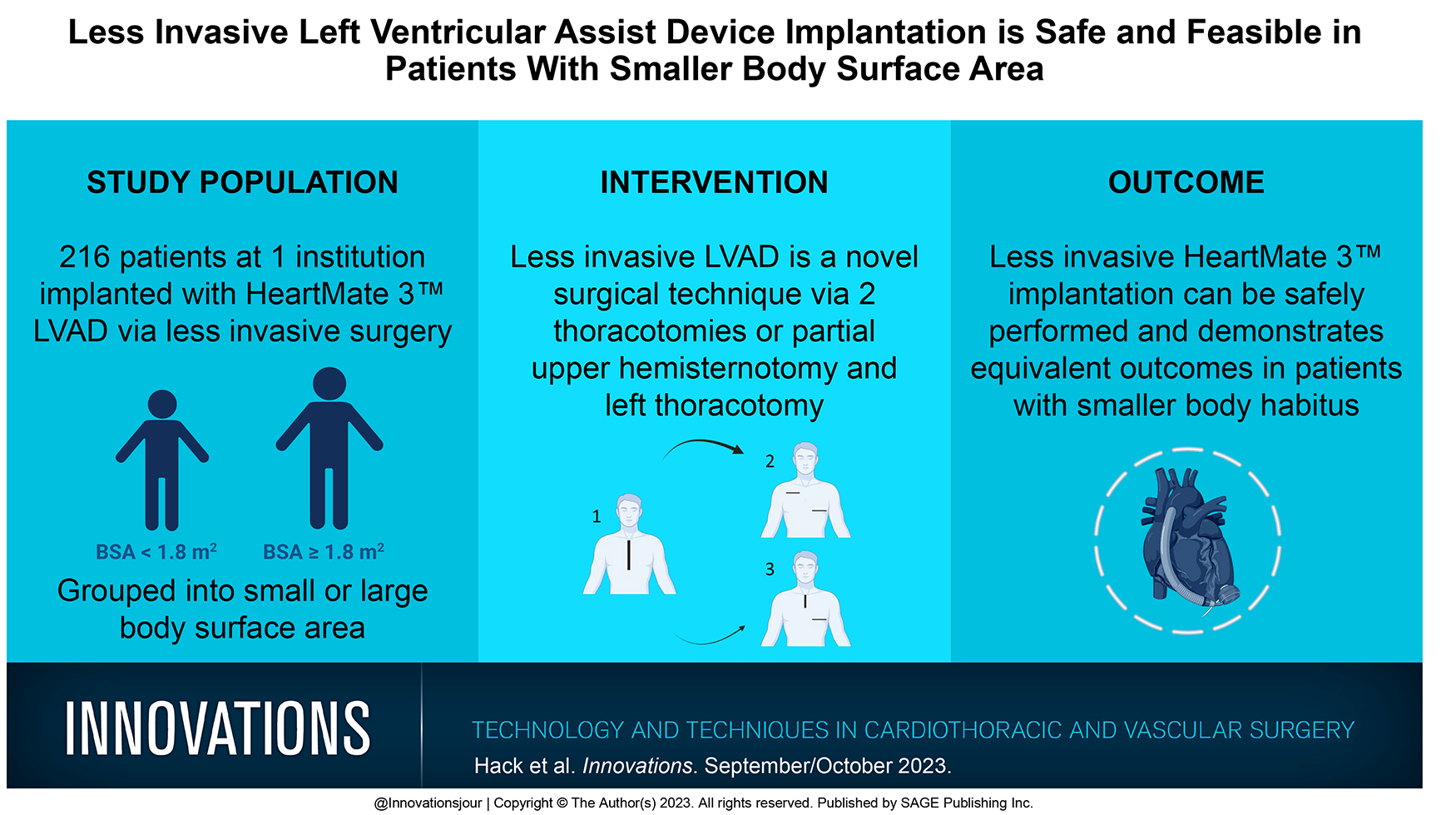
Smaller body surface area (BSA) frequently precludes patients from left ventricular assist device (LVAD) therapy. We sought to investigate the clinical outcomes in patients with small BSA undergoing less invasive LVAD implantation.
Methods:
We conducted a retrospective review of 216 patients implanted with HeartMate 3 LVAD (Abbott, Chicago, IL) via less invasive surgery at our institution. Patients were dichotomized based on their preimplant BSA for comparison between small BSA (≤1.8 m2) and normal/large BSA (>1.8 m2). We analyzed patient perioperative characteristics and outcomes.
Results:
In our study, small BSA was found in 32 patients (14.8%), while 184 patients (85.2%) had normal/large BSA. Women were more prevalent in the small BSA group (50.0% vs 13.0%, P < 0.001). Preoperative and intraoperative data showed comparable results. Major complications and hospital length of stay did not differ by BSA group. Patients with smaller BSA had significantly decreased pump parameters at discharge, including LVAD flow (4.11 ± 0.49 vs 4.60 ± 0.54 L/min, P < 0.001) and pump speed (5,200 vs 5,400 rpm, P < 0.001). Survival to discharge and within 6 months after implantation were similar between the groups.
Conclusions:
Our study results suggest that less invasive HeartMate 3 implantation can be safely performed and demonstrates equivalent outcomes in patients with smaller body habitus. Randomized trials are required to confirm our data.
Research article
Restricted accessResearch articleFirst published September, 2023pp. 452-458
William B. Keeling, David Tian, Woodrow Farrington , [...]
View All
Abstract
Objective:
Controversy remains regarding the optimal neuroprotection strategy for elective hemiarch replacement (HEMI). This study sought to compare outcomes in patients who underwent HEMI utilizing the 2 most common contemporary methods of cerebral protection.
Methods:
The ARCH international aortic database was queried, and 782 patients undergoing elective HEMI with circulatory arrest from 2007 to 2012 were identified. There were 418 patients who underwent HEMI using moderate hypothermia (nasopharyngeal temperature 20.1 to 28.0 °C) and antegrade cerebral perfusion (MHCA/ACP). There were 364 patients who underwent HEMI using deep hypothermia (nasopharyngeal temperature 14.1 to 20 °C) and retrograde cerebral perfusion (DHCA/RCP). Adverse outcomes were compared between the groups using both univariable and multivariable analyses.
Results:
Patients who underwent MHCA/ACP were older (64 vs 61 years, P = 0.01) and more frequently had peripheral vascular disease than DHCA/RCP patients (28.5% vs 7.1%, P < 0.001). Patients in the DHCA/RCP group had a greater incidence of full aortic root replacement (55.8% vs 26.4%, P < 0.001) and more frequently had a central cannulation strategy (83% vs 55.7%, P < 0.001). Cardiopulmonary bypass (170 vs 157 min, P = 0.002) and aortic cross-clamp (134 vs 92 min, P < 0.001) times were significantly longer in the DHCA/RCP group. On univariable analysis, overall mortality was statistically similar between groups (MHCA/ACP 3.4% vs DHCA/RCP 2.3%, P = 0.47), but permanent neurologic deficits were significantly lower in the DHCA/RCP cohort (MHCA/ACP 3.9% vs DHCA/RCP 1.0%, P = 0.02). Multivariable analysis showed no difference in mortality nor perioperative stroke between perfusion cohorts.
Conclusions:
Both MHCA/ACP and DHCA/RCP are excellent neuroprotective strategies that produce low mortality in patients undergoing elective HEMI. DHCA/RCP may demonstrate theoretically improved neurologic outcomes compared with MHCA/ACP, but this topic warrants further study.
Research article
Restricted accessResearch articleFirst published September, 2023pp. 459-465
John Y. Lee, Kathryn L. Pedula, Timothy O. Berkley , [...]
View All
Abstract
Objective:
Long-term outcomes of vein morphologies in the endoscopic vein harvesting setting are lacking. We analyzed 15-year follow-up for endoscopic versus open vein harvesting and associated vein morphology outcomes in coronary artery bypass grafting at a single center.
Methods:
This single-center, prospectively collected, retrospective, observational study evaluated 15-year major adverse cardiovascular events (MACE) of endoscopic versus open vein harvesting and associated vein morphologies.
Results:
Among 729 patients, no differences were found between endoscopic and open vein harvesting in MACE hazard ratios despite increased risks with native Hawai’ian, Pacific Islander, and Filipino patients. Asian and Filipino patients had more thin-walled veins and Asian and multirace patients had more vasovasoral branches than White patients. Bifid veins were associated with increased risk of cardiac catheterization. Varicose veins were associated with myocardial infarction, congestive heart failure, and death. Thick-walled veins were associated with revascularization and dense adhesions with cardiac catheterization and revascularization.
Conclusions:
Fifteen-year adjusted MACE was similar between endoscopic and open vein harvesting in small coronary targets despite increased risks with native Hawai’ian, Pacific Islander, and Filipino patients. Bifid, varicose, thick-walled veins, and dense adhesions had worse MACE.
Research article
Restricted accessResearch articleFirst published September, 2023pp. 466-471
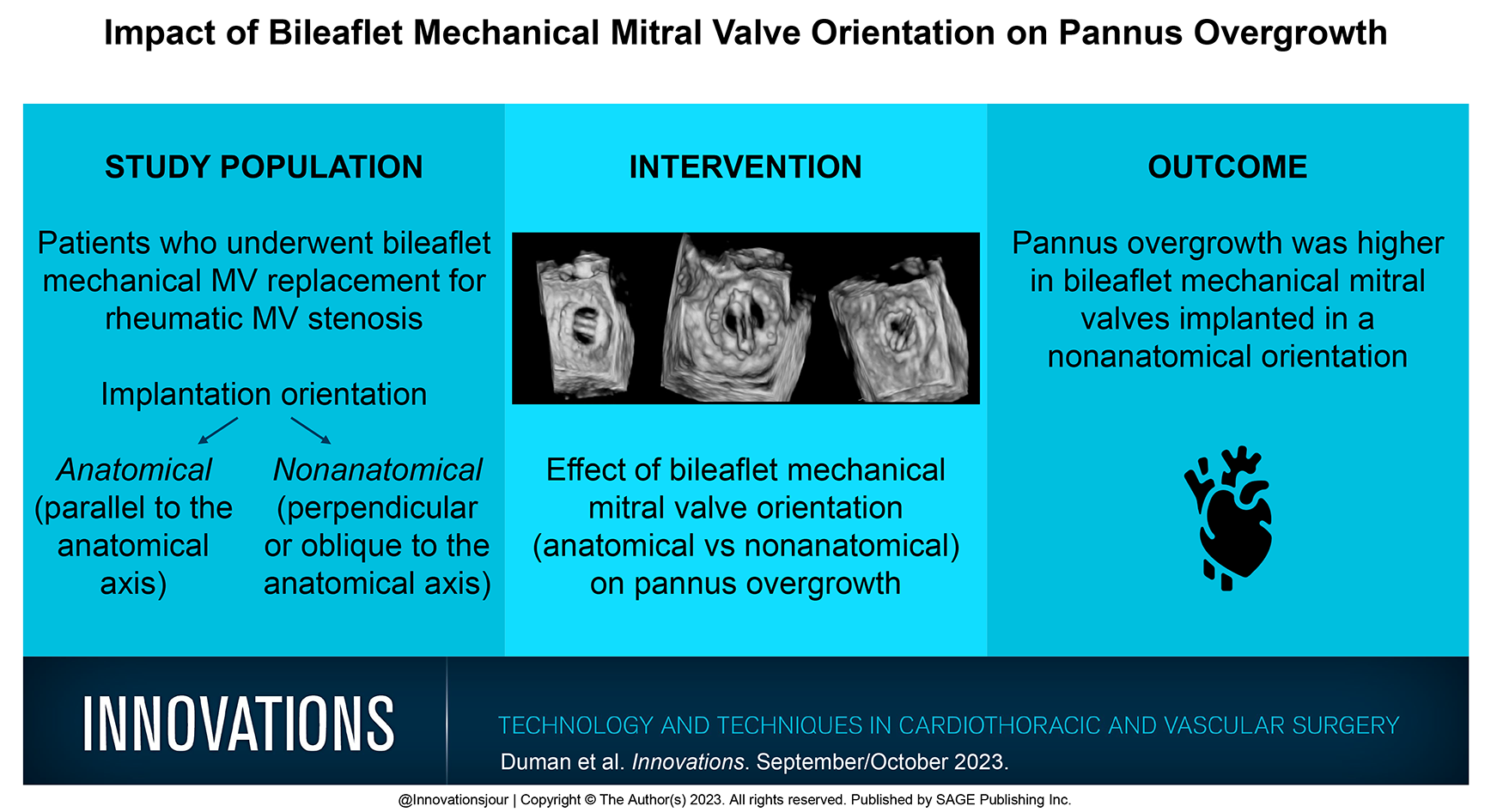
Pannus overgrowth is a chronic inflammatory process that can cause valve dysfunction and threaten the durability of prosthetic valves. Bileaflet mechanical mitral valve can be implanted in either an anatomical (parallel to the anatomical axis) or nonanatomical (perpendicular or oblique to the anatomical axis) orientation. The effect of the rotational orientation of the bileaflet mechanical mitral valve on excessive pannus enlargement is unknown. The present study compared the effect of bileaflet mechanical mitral valve orientation on pannus overgrowth.
Methods:
The study included patients who underwent bileaflet mechanical mitral valve replacement for rheumatic mitral valve stenosis. The pannus formation was confirmed by reexamining all transesophageal echocardiography images in the picture archiving and communication systems between May 2017 and April 2021. The primary aim of this study was the development of pannus overgrowth. Patients were divided into 2 groups based on their implantation orientation of the bileaflet mechanical mitral valve.
Results:
Pannus overgrowth was found in 26 patients (56.5%) in the anatomical orientation group and 71 patients (74.7%) in the nonanatomical orientation group (P = 0.03). Anatomical orientation reduced the development of pannus overgrowth (odds ratio [OR] = 0.39, P = 0.04), and double left heart valve replacement increased the development of pannus overgrowth (OR = 2.73, P = 0.04).
Conclusions:
Pannus overgrowth was less common in bileaflet mechanical mitral valves implanted in the anatomical orientation.
Research article
Restricted accessResearch articleFirst published September, 2023pp. 472-478
Ian A. Tamargo, Christina Creel-Bulos, Maria C. Callahan , [...]
View All
Abstract
Objective:
Obese patients with coronavirus disease 2019 (COVID-19)–associated acute respiratory failure (ARDS) often require prolonged intubation. However, data are sparse regarding optimal tracheostomy timing in obese adults with COVID-19 requiring venovenous extracorporeal membrane oxygenation (VV-ECMO). This study retrospectively describes the course of obese patients with COVID-19 who underwent tracheostomy on VV-ECMO between March 2020 and December 2022.
Methods:
There were 62 participants with a median age of 43 (interquartile range [IQR] 33 to 53) years and a median body mass index of 42 (IQR 34 to 50) kg/m2 who received VV-ECMO for COVID-19–associated ARDS. Of those, 42 underwent tracheostomy on VV-ECMO, and 50% (n = 21) of the 42 patients underwent early (within 14 days of initiated ventilatory support) tracheostomy.
Results:
Among patients who received tracheostomies, the combined respiratory tract and lung parenchymal bleeding rate was 29% (n = 12), but only 7% required surgical intervention for bleeding from the tracheostomy site (n = 3). The hospital length of stay (LOS) was 42 (IQR 36 to 57) days, and mortality rate was 38% (n = 16). Tracheostomy timing was not associated with differences in respiratory tract bleeding, mechanical ventilatory support duration, VV-ECMO support duration, intensive care unit LOS, hospital LOS, mortality, or survival probability.
Conclusions:
Although an individualized and holistic approach to clinical decision making continues to be necessary, the findings of this study suggest that early tracheostomy may be performed safely in obese patients with COVID-19 on VV-ECMO.
Research article
Restricted accessResearch articleFirst published September, 2023pp. 479-488
Daniel OhORCID, Kristen Brown, Sadia Yousaf , [...]
View All
Abstract
Objective:
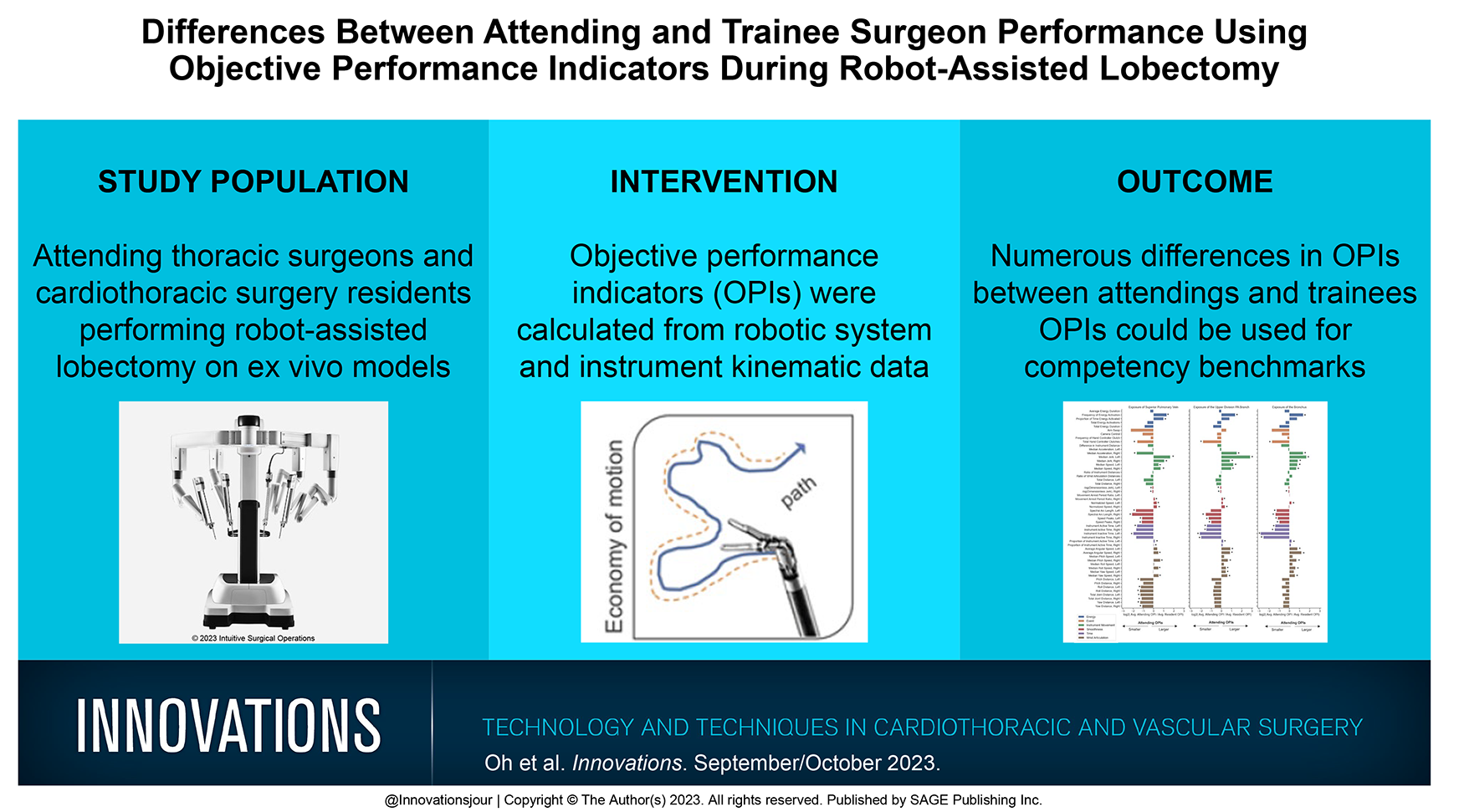
Existing approaches for assessing surgical performance are subjective and prone to bias. In contrast, utilizing digital kinematic and system data from the surgical robot allows the calculation of objective performance indicators (OPIs) that may differentiate technical skill and competency. This study compared OPIs of trainees and attending surgeons to assess differences during robotic lobectomy (RL).
Methods:
There were 50 cardiothoracic surgery residents and 7 attending surgeons who performed RL on a left upper lobectomy of an ex vivo perfused model. A novel recorder simultaneously captured video and data from the system and instruments. The lobectomy was annotated into discrete tasks, and OPIs were analyzed for both hands during 6 tasks: exposure of the superior pulmonary vein, upper division of the pulmonary artery and bronchus, and the stapling of these structures.
Results:
There were significant differences between attendings and trainees in all tasks. Among 20 OPIs during exposure tasks, significant differences were observed for the left hand in 31 of 60 (52%) of OPIs and for the right hand in 42 of 60 (70%). During stapling tasks, significant differences were observed for the stapling hand in 28 of 60 (47%) of OPIs and for the nonstapling hand in 14 of 60 (25%).
Conclusions:
Use of a novel data and video recorder to generate OPIs for both hands revealed significant differences in the operative gestures performed by trainees compared to attendings during RL. This method of assessing performance has potential for establishing objective competency benchmarks and use for tracking progress.
Research article
Open accessResearch articleFirst published September, 2023pp. 489-493
Ismael A. Salas De Armas, Juan Marcano, Mehmet H. Akay , [...]
View All
Abstract
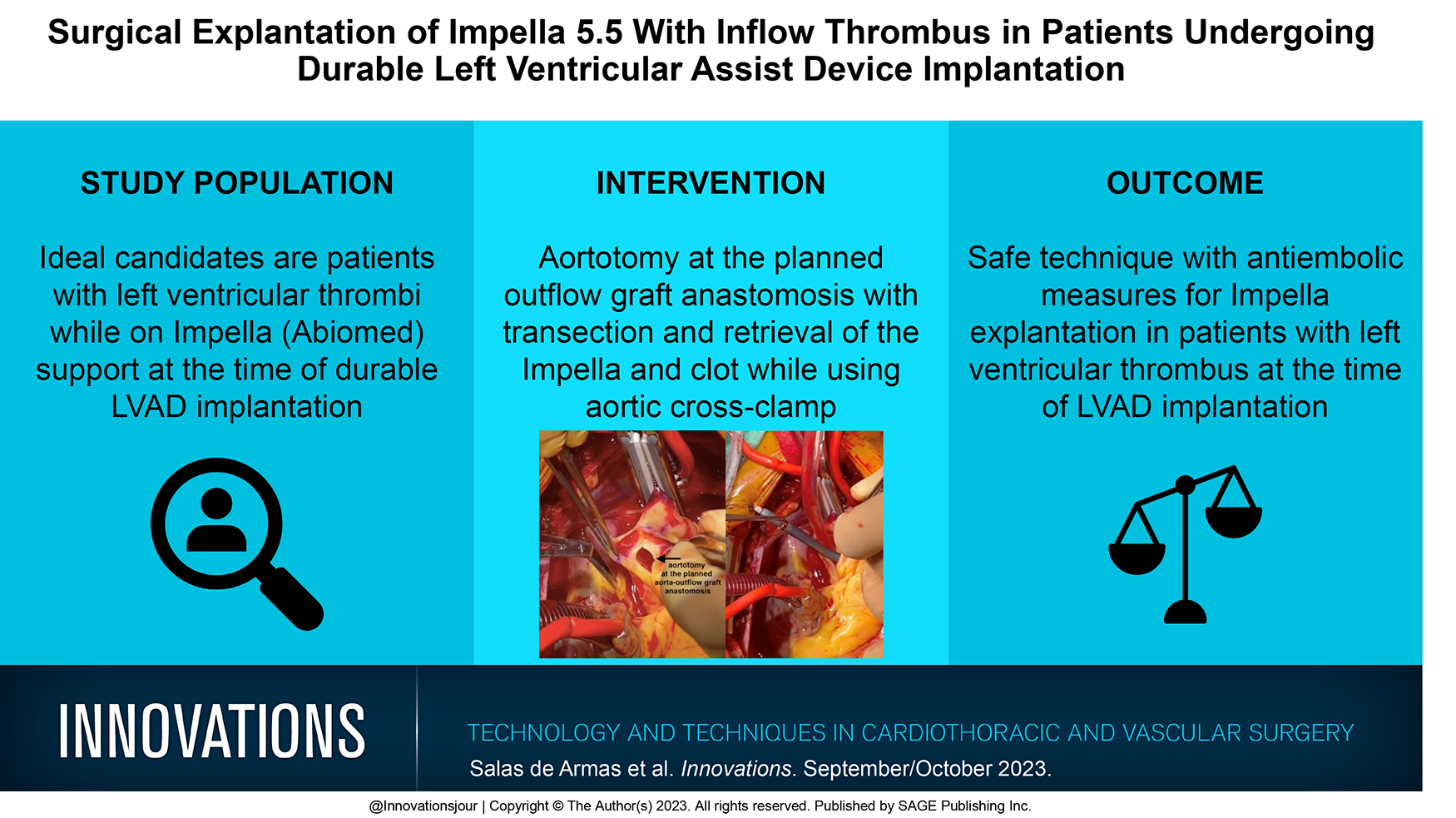
The Impella 5.5® (Abiomed, Danvers, MA, USA) is a microaxial flow pump that promotes left ventricular unloading and improves end-organ perfusion before durable left ventricular assist device (LVAD) implantation. Thrombus formation after Impella 5.5 insertion can occur and represents a significant challenge to device explantation. Durable LVAD implantation is typically performed without aortic cross-clamping, so a dislodged thrombus can potentially embolize and lead to catastrophic events. We describe our technique to safely explant an Impella 5.5 in patients who develop a thrombus on the inflow portion of the device before surgical LVAD implantation.
Brief report
Restricted accessBrief reportFirst published September, 2023pp. 494-497
Nicholas J.S. ChilversORCID, Zachariah M. EvansORCID, Sankar Balasubramanian , [...]
View All
Abstract
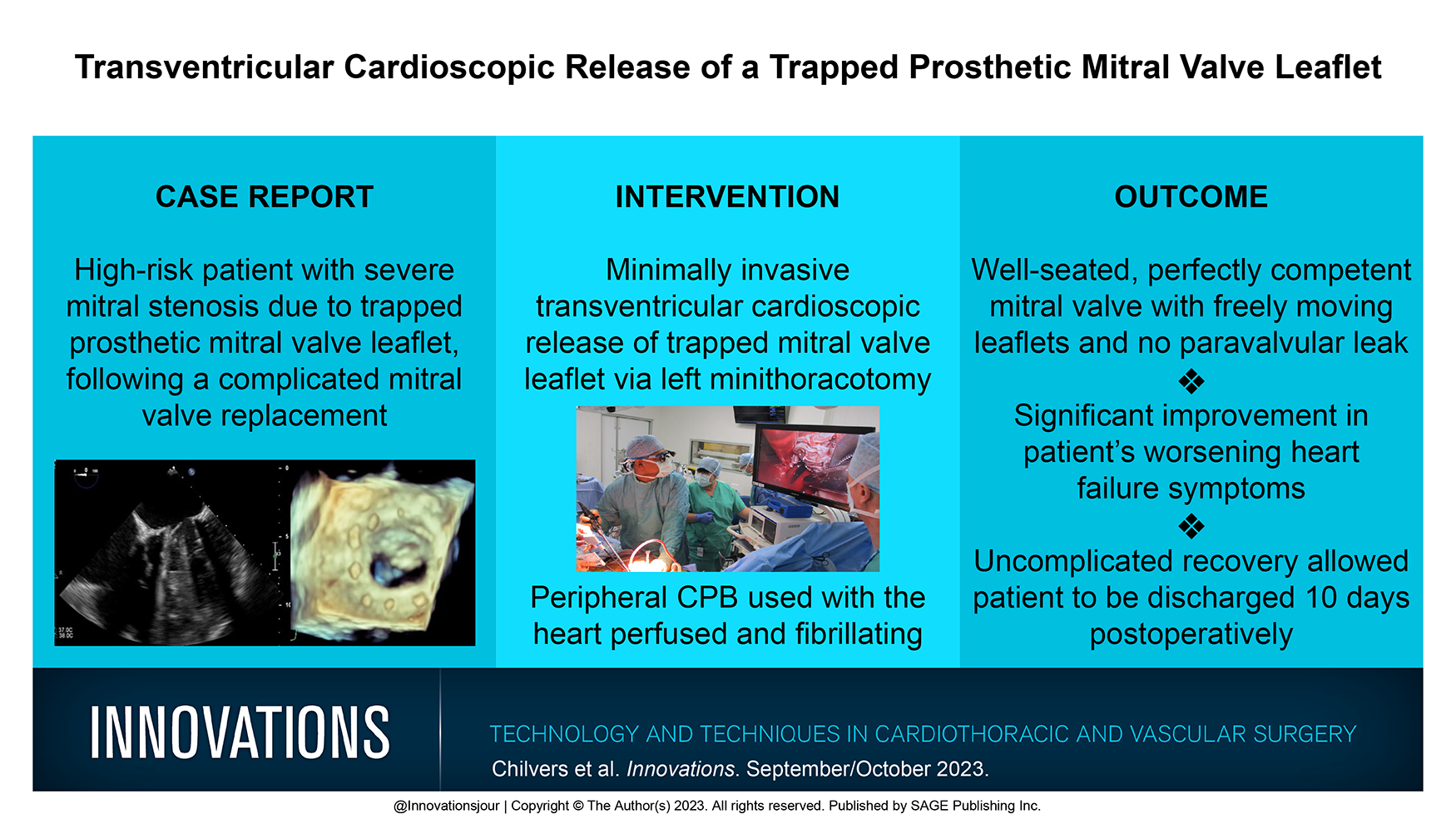
Trapped prosthetic valve leaflets are a rare but challenging complication. A 68-year-old male patient had previously undergone redo aortic valve replacement. Postoperatively, he decompensated with severe mitral regurgitation, requiring extracorporeal membrane oxygenation and a salvage mitral valve replacement via right thoracotomy with very difficult access. This procedure was complicated by a trapped valve leaflet. He recovered well initially but presented 2 years later with worsening heart failure due to mitral stenosis and rising pulmonary artery pressures. Due to the high risk of sternotomy and right thoracotomy, a transventricular cardioscopic release of the trapped mitral valve leaflet was undertaken by left minithoracotomy. The procedure was successful, and the patient was discharged home on day 12. This novel minimally invasive approach, which does not require myocardial preservation, is ideal for high-risk patients with this rare complication and has not previously been described. We hope that by sharing our experience, others will consider this innovative approach.
Brief report
Restricted accessBrief reportFirst published September, 2023pp. 498-502
Endotension remains an enigmatic rare cause of endovascular abdominal aortic aneurysm repair failure leading to aneurysm growth and/or rupture. We present a patient with a long-standing endotension treated with open reconstruction and graft explantation. We also provide a unique clinical video, which gives a key view of the intrasac operative findings.
Brief report
Restricted accessBrief reportFirst published September, 2023pp. 503-505
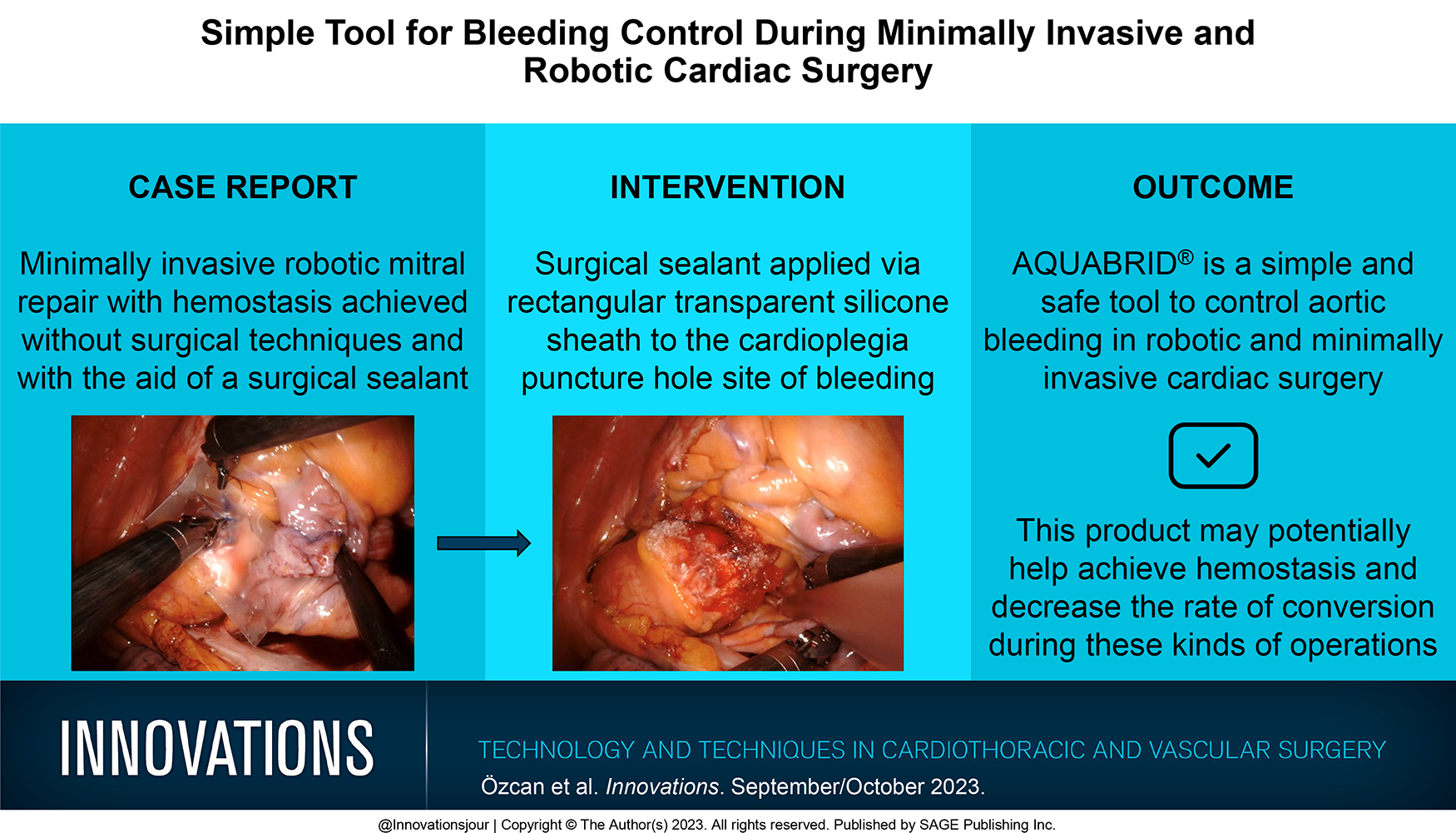
Achievement of complete hemostasis is a key element to success in cardiac surgery. Bleeding control is of utmost importance in minimally invasive and robotic cardiac surgery to avoid conversion, as major bleeding is one of the most common indications for conversion to sternotomy. Bleeding control with surgical techniques can be technically more difficult in robotic and minimally invasive cardiac surgery as access to the bleeding area is limited and it is harder to intervene compared with open cardiac surgery with sternotomy. We present in this case the achievement of hemostasis in a minimally invasive robotic mitral repair, without the employment of surgical techniques and with the aid of a surgical sealant.
Brief report
Restricted accessBrief reportFirst published September, 2023pp. 506-508
Samuel J. Martin, Courtney Maxey-Jones, Zhandong Zhou , [...]
View All
Abstract
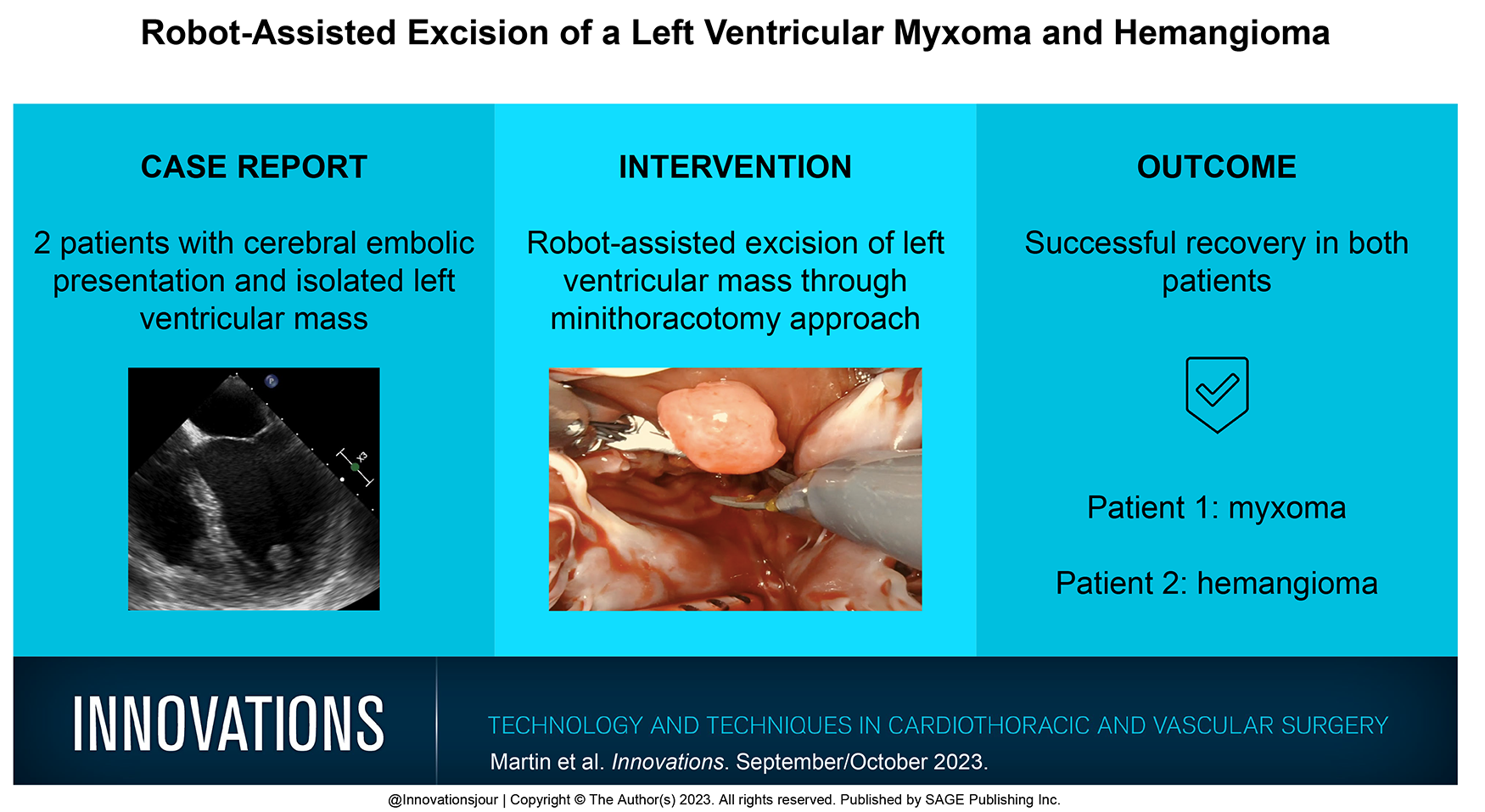
Left ventricular masses are rare entities that often require surgical excision when diagnosed due to the risk of embolization. We report 2 separate patients presenting with evidence of cerebral embolization both of whom were diagnosed with isolated left ventricular masses and underwent surgical excision through a robot-assisted approach. Microscopic pathology revealed a myxoma and hemangioma, respectively. Both cases demonstrate that left ventricular masses can be feasibly excised through a robot-assisted minithoracotomy approach.