Emmanuel Lansac, Kevin M. Veen, Andria Joseph , [...]
View All
Abstract
Objective:
Globally significant variation in treatment and course of heart valve disease (HVD) exists, and outcome measurement is procedure focused instead of patient focused. This article describes the development of a patient-related (International Consortium for Health Outcomes Measurement) standard set of outcomes and case mix to be measured in patients with HVD.
Methods:
A multisociety working group was formed that included patient representatives and representatives from scientific cardiology and cardiothoracic surgery societies that publish current guidelines for HVD. The standard set was developed to monitor the patient’s journey from diagnosis to treatment with either a surgical or transcatheter procedure. Candidate clinical and patient-reported outcome measures (PROMs) and case mix were identified through benchmark analyses and systematic reviews. Using an online modified Delphi process, the working group voted on final outcomes/case mix and corresponding definition.
Results:
Patients with aortic/mitral/tricuspid valve disease or root/ascending aorta >40 mm were included in the standard set. Patients entered the dataset when the diagnosis of HVD was established, allowing outcome measurement in the preprocedural, periprocedural, and postprocedural phases of patients’ lives. The working group defined 5 outcome domains: vital status, patient-reported outcomes, progression of disease, cardiac function and durability, and complications of treatment. Subsequently, 16 outcome measures, including 2 patient-reported outcomes, were selected to be tracked in patients with HVD. Case-mix variables included demographic factors, demographic variables, echocardiographic variables, heart catheterization variables, and specific details on aortic/mitral/tricuspid valves and their specific interventions.
Conclusions:
Through a unique collaborative effort between patients and cardiology and cardiothoracic surgery societies, a standard set of measures for HVD was developed. This dataset focuses on outcome measurement regardless of treatment, moving from procedure- to patient-centered outcomes. Implementation of this dataset will facilitate global standardization of outcome measurement, allow meaningful comparison between health care systems and evaluation of clinical practice guidelines, and eventually improve patient care for those experiencing HVD worldwide.
Review article
Open accessReview articleFirst published March, 2025pp. 148-157
Paul WernerORCID, Martin Winter, Iuliana Coti , [...]
View All
Abstract
The choice of cannulation technique for cardiopulmonary bypass remains a critical decision in cardiac surgery with direct consequences for intraoperative management and patient outcomes. Central and femoral cannulation represent the 2 dominant approaches, each associated with unique anatomical considerations, hemodynamic implications, and perioperative risks. The correct selection of a cannulation strategy should limit the risk of embolic events and associated complications such as vascular injury and stroke. The purpose of this review is to provide a detailed comparison of central and femoral cannulation techniques, with an emphasis on clinical scenarios and outcomes, recent innovations, and state-of-the-art technology. By critically analyzing current evidence, we aim to offer insights into the optimal cannulation strategy tailored to specific patients.
Research article
Restricted accessResearch articleFirst published March, 2025pp. 158-166
Noritsugu NaitoORCID, Homam Ibrahim, Cezar Staniloae , [...]
View All
Abstract
Objective:
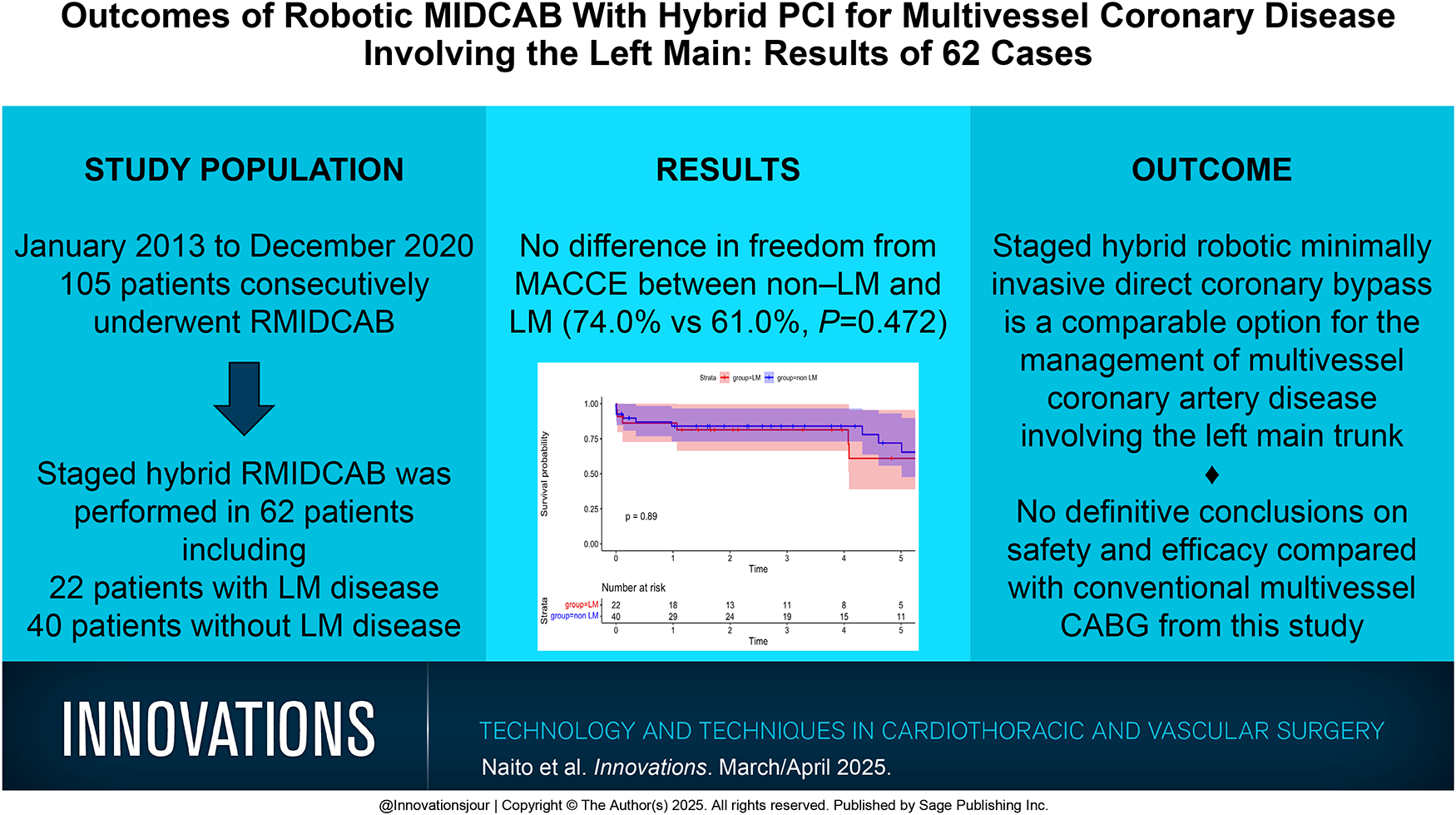
Hybrid coronary revascularization is a clinical strategy that uses a combination of surgical revascularization and percutaneous coronary intervention (PCI). Data on the hybrid approach for coronary artery disease involving the left main (LM) are scarce. We analyzed our cohort of hybrid coronary revascularizations with minimally invasive direct coronary artery bypass (MIDCAB) using robotic left internal mammary artery harvesting and PCI for multivessel disease with and without LM involvement.
Methods:
Between January 2013 and December 2020, 105 patients consecutively underwent robotic MIDCAB. Of those, 62 patients (59.1%) had multivessel coronary artery disease and underwent revascularization via the hybrid approach using robotic MIDCAB and PCI. Patients were then stratified into 2 groups for comparison: LM disease (n = 22, 35.5%) and non-LM disease (n = 40, 64.5%).
Results:
The SYNTAX scores were significantly lower in the non-LM group compared with the LM group (19.06 ± 6.41 vs 24.86 ± 7.04, P = 0.002). There were no other significant differences in demographics between the groups. There were no 30-day mortalities in either group. Freedom from major adverse cardiac and cerebrovascular events at 5 years was 72.2% in the non-LM group and 61.0% in the LM group (P = 0.89). There were no significant differences in 5-year overall survival (94.1% vs 83.3%, P = 0.074) or freedom from coronary reintervention (83.4% vs 75.4%, P = 0.699).
Conclusions:
Hybrid robotic MIDCAB for patients with and without LM disease can be performed with acceptable results in selected patients. However, it is not possible to draw definitive conclusions regarding safety and efficacy compared with conventional coronary artery bypass grafting.
Research article
Restricted accessResearch articleFirst published March, 2025pp. 167-174
Brittany A. Zwischenberger, Jeffrey G. Gaca, Keith Carr , [...]
View All
Abstract
Objective:
The Alfieri stitch is a mitral repair technique that can easily be applied in less invasive approaches to the mitral valve. However, the Alfieri stitch is seldom used and has raised concerns about producing mitral stenosis or recurrent regurgitation.
Methods:
A total of 1,134 consecutive patients undergoing repair of degenerative mitral regurgitation via right minithoracotomy from 1997 to 2019 were examined from a prospectively maintained database. Propensity score matching was performed on patients with and without Alfieri stitch.
Results:
The Alfieri stitch was used in 697 of 1,134 patients (53%) with annuloplasty in all patients. Patients receiving the Alfieri stitch had more flail leaflet (P = 0.001), larger rings (P < 0.001), more chordal replacement (P < 0.001), and more cleft closure (P < 0.001). In 201 matched patient pairs, Alfieri patients did not differ significantly in baseline characteristics or procedure performed other than the Alfieri stitch. Matched patients with Alfieri stitch had similar clamp and pump times and no difference in postoperative course. Matched patients with Alfieri stitch had only slightly higher mean postoperative gradient (4.0 ± 1.5 vs 3.2 ± 1.3 mm Hg, P < 0.001). At 10 years, matched patients with Alfieri stitch showed nonsignificant differences in survival (P = 0.5), cumulative incidence of severe mitral regurgitation (5% ± 3% vs 3% ± 3%, P = 0.3), and moderate or more mitral regurgitation (17% ± 4% vs 12% ± 4%, P = 0.8) but more mitral reoperation at 10 years (6% ± 3% vs 1% ± 1%, P = 0.02).
Conclusions:
The Alfieri stitch can be applied via right minithoracotomy to repair a wide variety of degenerative mitral pathology with minimally higher mitral gradient and a late trend toward increased mitral reoperation at 10 years.
Research article
Restricted accessResearch articleFirst published March, 2025pp. 175-179
This study aims to identify the perceived barriers and factors contributing to the slow adoption of robotic technology among coronary surgeons.
Methods:
We administered an anonymous online survey during the 2023 Society for Thoracic Surgeons (STS) Coronary Conference and included questions about factors associated with the lack of, or slow adoption of, robotics in coronary artery bypass surgery.
Results:
A total of 75 coronary surgeons completed the anonymous online survey. Of these respondents, 30 surgeons (39.4%) reported having more than 15 years of experience as independent coronary surgeons. Among the 71 surgeons (95%) who were not using robotic technology, the barriers to adoption (from most important to less important) were lack of skill or experience with robotic technology (mean score, 2.56 ± 1.84), followed by the lack of referral of patients with hybrid or single-vessel disease from cardiologists (2.81 ± 1.76), the need for more support and learning opportunities (e.g., hands-on courses, online courses; 3.44 ± 1.98), and more data to support the efficacy and safety of robotic coronary surgery (3.63 ± 2.22). Moreover, 38 surgeons (50%) expressed a willingness to consider robotic coronary surgery if industry provided appropriate devices such as stabilizers and automated anastomotic devices. Finally, 53 surgeons (69.7%) reported being unaware of the Thoracic Surgery Foundation and STS Advanced Robotic Cardiac Surgery Fellowship award with a coronary track.
Conclusions:
The findings from this survey identify the barriers to adopting robotic technology in coronary surgery. Addressing these barriers through targeted interventions could foster wider acceptance and use of robotic technology in coronary bypass surgery.
Research article
Restricted accessResearch articleFirst published March, 2025pp. 180-187
Giovanni ConcistréORCID, Max Baghai, Giuseppe Santarpino , [...]
View All
Abstract
Objective:
Perceval sutureless valve (Corcym, Saluggia, Italy) has been in clinical use for more than 15 years. The aim of this study is to report clinical and hemodynamic performance from a real-world registry in patients who underwent aortic valve replacement (AVR) with a Perceval, comparing outcomes of minimally invasive (MICS) versus full sternotomy (FS) settings.
Methods:
This prospective international registry enrolled 1,652 patients implanted with a sutureless aortic valve in 55 institutions from 2011 to 2021. Patients with isolated AVR were analyzed by MICS and FS approaches. Preoperative covariates were adjusted with propensity score matching 2:1, reaching a final cohort of 857 isolated AVR patients with 558 patients in MICS and 299 in FS groups.
Results:
Successful first implantation was 98.0% for both approaches (P > 0.999). As expected, surgical timings were significantly longer in MICS versus FS (P = 0.004 and P < 0.001), but intensive care unit and hospital lengths of stay were significantly lower in the MICS cohort, resulting in about 0.5 days and 1.5 days less spent in the intensive care unit and hospital, respectively. The surgical approach did not show any effect on early or late survival, disabling stroke, leaks greater than 2, pacemaker rate, or hemodynamics.
Conclusions:
Our propensity-matched analysis demonstrates the noninferiority of MICS with regard to hard endpoints and better outcomes for secondary endpoints such as reduced length of intensive care and in-hospital stay.
Research article
Restricted accessResearch articleFirst published March, 2025pp. 188-193
Riya BhasinORCID, Sarah NisivacoORCID, Douglas Rybar , [...]
View All
Abstract
Objective:
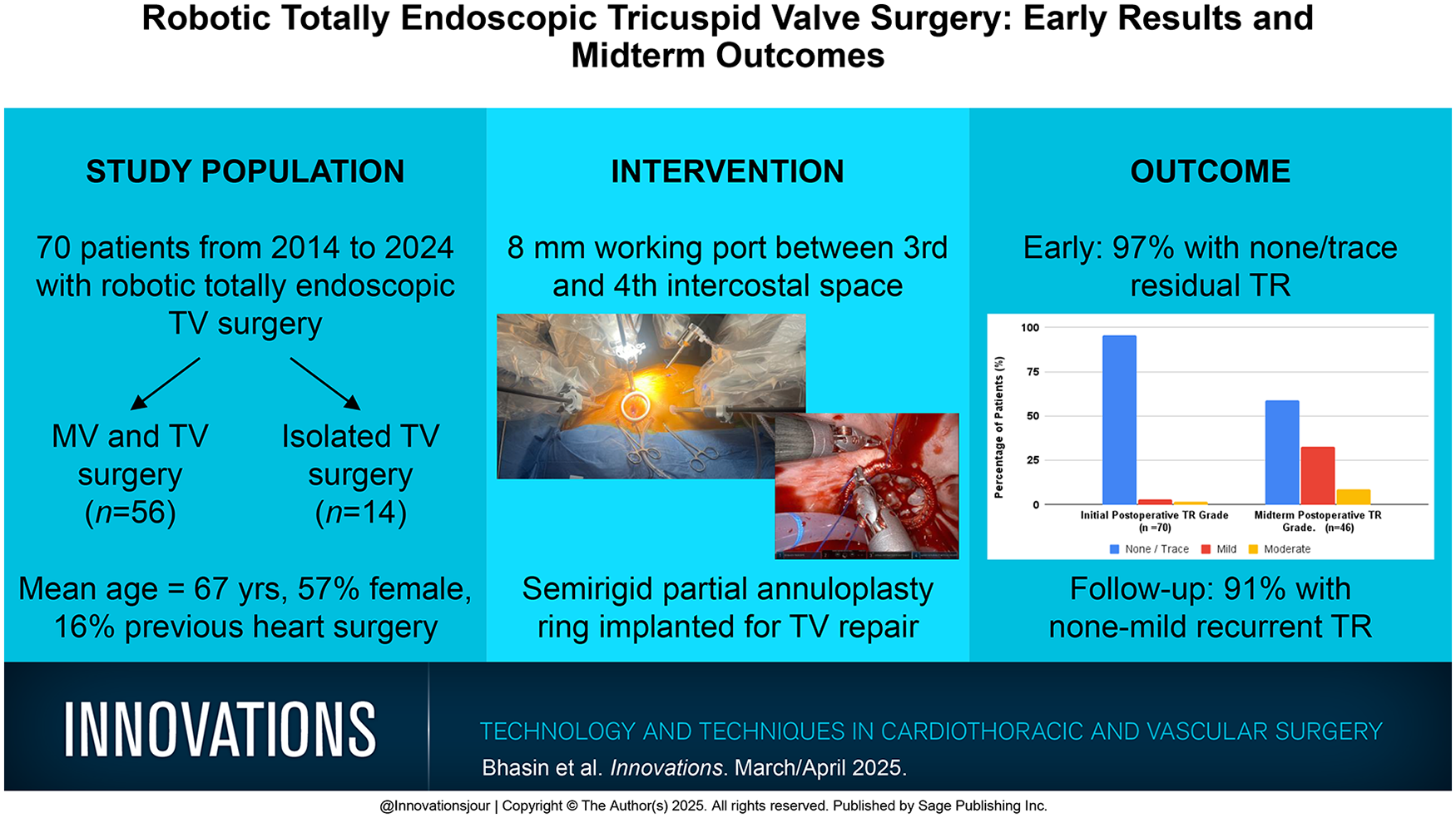
Although robotic cardiac surgery is becoming more widely adopted for mitral valve procedures, robot-assisted tricuspid valve (TV) surgery is less common. We describe clinical and echocardiographic outcomes for 70 isolated and concomitant TV repair (TVr) cases.
Methods:
Patients who underwent robotic totally endoscopic TV surgery at our institution were retrospectively reviewed. The da Vinci Si or Xi robot (Intuitive Surgical, Sunnyvale, CA, USA) was used for all cases, employing an 8 to 10 mm working port and using cardiopulmonary bypass on a beating heart. Early and midterm outcomes were reviewed, along with echocardiogram results when available.
Results:
Between 2014 and 2024, 70 patients underwent TVr. Fourteen cases were isolated TV procedures and 56 were concomitant with mitral surgery. The mean patient age was 67 ± 14.4 years, 57% were female, and 11 patients (16%) had previous heart surgery. TVr with an annuloplasty band occurred in 97% of patients, 1 patient had a tissue valve replacement, and there were no conversions to sternotomy. Early mortality occurred in 1 patient (1.4%) with an observed to expected ratio of 0.4. Early postoperative echocardiography revealed none to mild residual tricuspid regurgitation (TR) in 65 patients (93%). Clinical follow-up was completed in 97% of patients. All-cause mortality occurred in 14 patients (20%), 11 of which were noncardiac, including cancer, gastrointestinal bleed, end-stage renal disease, SARS-CoV-2 infection, and drug overdose. Follow-up echocardiography results were available for 46 patients (66%) at a mean of 45 months, showing moderate or more recurrent TR in 6 patients (9%).
Conclusions:
Robot-assisted totally endoscopic TV surgery, for both isolated and concomitant TV disease, is a safe and effective approach. The sternal-sparing nature allows for rapid recovery and positive midterm outcomes.
Research article
Restricted accessResearch articleFirst published March, 2025pp. 194-200
Marc W. Gerdisch, Chanice Johns, Manesh Parikshak , [...]
View All
Abstract
Objective:
We initiated a cardiac enhanced recovery after cardiac surgery (ERAS) program in early 2019, protocolized it and applied it to all patients in 2020, and added the use of active chest tube clearance (ATC) in 2022. Prospective data collection of ATC patients was compared with historical controls to determine the impact of the device on outcomes.
Methods:
The study comprised 1,334 patients with 650 in the control group (group 1) and 684 in the ATC intervention group (group 2). Group 1 (historical control) consisted of 650 patients from January 1, 2020, to October 31, 2020, and January 1, 2021, to October 31, 2021. From October 31, 2021, to December 31, 2021, we introduced ATC use per protocol. Group 2 (ATC) consisted of 684 patients treated consecutively from January 1, 2022, to August 31, 2023, with ATC. The preoperative characteristics and operative procedures between groups were similar.
Results:
Patients in the ATC intervention (group 2) experienced a 41% reduction in the composite of retained blood syndrome (8.2% in group 1 vs 4.8% in group 2, P = 0.014). Postoperative atrial fibrillation was 17% reduced for group 2 (178 [33.8%] in group 1 vs 158 [28.1%] in group 2, P = 0.049). Group 2 had a 30% reduction in median intensive care unit (ICU) hours (51.6 [30.1 to 76.9] h in group 1 vs 36.3 [20.7 to 687] h in group 2, P < 0.001). Twenty-one patients (3.2%) were readmitted to the ICU after initial discharge to the step-down unit in group 1 and only 8 (1.17%) in group 2 (P = 0.013).
Conclusions:
The addition of the ATC intervention to an established ERAS program in a high-volume private practice setting decreased complications, improved outcomes, and decreased resource utilization.
Research article
Restricted accessResearch articleFirst published March, 2025pp. 201-204
Acute type A aortic dissection is a fatal condition that presents with arch vessel dissection necessitating emergency surgical intervention and reconstruction. During surgical treatment of acute type A aortic dissection, thorough analysis is required to prevent complications while reconstructing these fragile dissected arch vessels. This study describes the surgical treatment of 8 patients with dissected arch vessels who underwent reinforcement technique for anastomosis mediated by Hydrofit® (Sanyo Chemical Industries, Kyoto, Japan). The arch vessels were anastomosed with a prosthetic graft. Following the application of Hydrofit to the suture line on the adventitia, no intraoperative bleeding was detected at the reconstruction site of the dissected arch vessels. Postoperative computed tomography revealed no new anastomotic tear or pseudoaneurysm. We highly recommend the use of this reinforcement technique with Hydrofit for the management and reconstruction of vessels involved in acute type A aortic dissection. We observed a fast and uneventful recovery, suggesting promising postoperative results.
Brief report
Restricted accessBrief reportFirst published March, 2025pp. 205-206