
Abstract
Select search scope: search across all journals or within the current journal
This study outlines methods for modeling disability-adjusted life-years (DALYs) in common decision-modeling frameworks. Recognizing the wide spectrum of experience and programming comfort level among practitioners, we outline 2 approaches for modeling DALYs in its constituent parts: years of life lost to disease (YLL) and years of life lived with disability (YLD). Our beginner approach draws on the Markov trace, while the intermediate approach facilitates more efficient estimation by incorporating non-Markovian tracking elements into the transition probability matrix. Drawing on an existing disease progression discrete time Markov cohort model, we demonstrate the equivalence of DALY estimates and cost-effectiveness analysis results across our methods and show that other commonly used “shortcuts” for estimating DALYs will not, in general, yield accurate estimates of DALY levels nor incremental cost-effectiveness ratios in a modeled population.
This study introduces 2 DALY estimation methods—beginner and intermediate approaches—that produce similar results, expanding the toolkit available to decision modelers.
These methods can be adapted to estimate other outcomes (e.g., QALYs, life-years) and applied to other common decision-modeling frameworks, including microsimulation models with patient-level attributes and discrete event simulations that estimate YLDs and YLLs based on time to death and disease duration.
Our findings further reveal that commonly used shortcut methods for DALY calculations may lead to differing results, particularly for DALY levels and incremental cost-effectiveness ratios.
Icon arrays, which visually depict frequencies, are commonly recommended for communicating risk information such as survival rates. However, they have been found to be ineffective at buffering against motivated reasoning that can lead to undue optimism. To determine whether the impersonal frequency format of icon arrays (reporting a number affected out of a reference class) makes them vulnerable to motivated reasoning, a novel intervention is tested as a means for reducing undue optimism.
Female US participants from Amazon’s MTurk (
People’s gut-level beliefs about their infant’s chances of survival were optimistically biased; the intervention did not reduce this. These gut-level beliefs, rather than the objective survival rate information conveyed through icon arrays, were predictive of subsequent treatment choices.
The results suggest that the inability of icon arrays to buffer against motivated reasoning is not due to their frequency format. Moreover, the findings highlight the usefulness of measuring gut-level interpretations of likelihood, which can reveal significant insights into the psychological mechanisms driving patient-treatment choices.
Icon arrays, which visually depict frequencies, are commonly recommended as best-practice for communicating risk information in health contexts.
However, recent work has found that they are ineffective at reducing the extent to which people engage in motivated reasoning when processing likelihood information.
We find that the frequency format of icon arrays—depicting a rate for outcomes in a group of people rather than a case-specific probability—is not a primary reason why they are ineffective at reducing optimism bias
We also find that measures of gut-level beliefs of likelihood are particularly well suited for detecting optimism bias, yet also predict subsequent treatment decisions.
This study explores patient and clinician perceptions of a patient decision aid, focusing on 2 features that are often absent: a health-literate approach (e.g., using plain language, encouraging question asking) and a tool that explicitly shows how treatment options align with patient values. The aim was to gather qualitative feedback from patients and clinicians to better understand how such features might be useful in guiding future decision aid development.
We present a secondary analysis of data collected during the development of a decision aid for patients considering surgery for sciatica (20 patients with sciatica or low-back pain; 20 clinicians). Patient and clinician feedback on the design was collected via semi-structured interviews with a think-aloud protocol. Transcripts were analyzed using framework analysis.
Theme 1 explored designs that reinforced key messages about personal autonomy, including an interactive values-clarification tool. Theme 2 explored how participants valued encouragement and scaffolding to ask questions. Theme 3 described how patients preferred information they felt was complete, balanced, and understandable.
Further experimental and observational research is needed to quantitatively evaluate these decision aid features including evaluation among patients with and without low health literacy.
A health-literate approach to decision aid design and embedding an interactive values-clarification tool may be useful strategies for increasing patient capacity to engage in key aspects of shared decision making. These features may support patients in developing an understanding of personal autonomy in the choice at hand and confidence to ask questions.
Findings presented here were specific to the clinical context but provide generalizable practical insights for decision aid developers. This study provides insight into potential future areas of research for decision aid design.
This qualitative study explored clinician and patient perceptions of health literacy features and an interactive values-clarification task within a decision aid for patients considering surgery for sciatica.
The first theme described how patients and clinicians appreciated sections of the decision aid that reinforced the importance of personal choice. Patients and clinicians thought the interactive values-clarification task would help patients reflect on their values and support shared decision-making discussions.
The second theme described how patients and clinicians appreciated strategies to encourage patients to ask questions of the surgeon.
The third theme described patients’ preference for information that they felt was complete, balanced, and understandable.
Lung cancer is especially prevalent among US veterans, and lung cancer mortality can be reduced through lung cancer screening (LCS). LCS guidelines recommend shared decision making (SDM) to help patients weigh the benefits and harms of LCS and make informed, values-based decisions about screening. Yet some question whether SDM affects patient outcomes. This study evaluated US veterans’ perceptions of LCS SDM quality and its relationship with satisfaction in LCS decisions.
We administered surveys via mail and phone to veterans in the VA New England Healthcare Network after recent LCS conversations. SDM quality was measured using CollaboRATE, with top scores indicating high quality. Decision satisfaction was assessed using the Satisfaction with Decision scale. Generalized linear models analyzed associations between perceived SDM quality and decision satisfaction, adjusting for demographics, health, and overall care satisfaction.
Among 1,033 patients who received surveys, 320 responded (31.0%), with 220 recalling the LCS conversation. Among those who answered the CollaboRATE questions, 34.0% (73/215) perceived SDM to be high quality (“top scorers”). Perceived high-quality SDM was significantly associated with greater decision satisfaction compared with lower perceived SDM quality (adjusted mean satisfaction on a 30-point scale = 26.75 v. 24.23;
The sample was primarily White, male, and all US veterans, limiting generalizability to other LCS-eligible cohorts. The cross-sectional design prevents causal inferences and long-term follow-up.
Higher perceived SDM quality was associated with greater patient satisfaction with the LCS decision. Improving SDM processes can enhance patient engagement and may improve LCS adherence and health outcomes.
Higher perceived shared decision making (SDM) quality in lung cancer screening (LCS) discussions leads to greater patient satisfaction with screening decisions.
While the use of patient education materials was linked to higher perceived SDM quality, less than half of patients who received materials rated SDM as high quality. There remains room for improved design and delivery to ensure materials effectively support the SDM process and guidance to providers on how to effectively incorporate patient educational materials to support, rather than replace, high-quality SDM conversations.
Enhancing SDM processes and aligning them with patient preferences can support patient satisfaction with their decision, which may have downstream benefits to patient engagement, adherence, and improved outcomes.
Patients are increasingly involved in decision making by their clinicians. Yet, there are concerns that involvement in decision making may cause emotional distress in patients. Little research has examined the nature of the burden experienced by patients confronted with a life-changing treatment decision. Therefore, we explored the nature and manifestations of burden experienced by patients with early-stage breast and prostate cancer regarding their involvement in decision making. We further aimed to identify patient-perceived causes and potential solutions for their experienced burden.
We used semi-structured interviews to explore the perspectives of patients with early-stage breast and prostate cancer. Patients (
Patients described being burdened by the decision in various ways and at various moments in the decision-making process. Patients attributed their decision-related burden mainly to uncertainty, fear of making the wrong decision, insufficient guidance by their clinician, and feeling an overwhelming sense of responsibility for their treatment decision. Patients indicated various factors that mitigated their burden or facilitated decision making, including having sufficient time, the opportunity to discuss the choice with experts and/or family, and receiving advice or confirmation from family or the clinician.
These findings suggest that decision-related burden could be caused by the uncertainty and anxiety patients experience and by a nonpreferred division of roles within the decision-making process.
Accordingly, acknowledging patients’ feelings by discussing the presence of uncertainty and distress might normalize the burden for patients. Moreover, clinicians could explore and adjust to patients’ role preference in decision making and discuss what would facilitate the decision process for patients.
Patients experience emotional, cognitive, and physical burden from their involvement in decision making.
Some of the burden appears to result from the way clinicians involve patients in decision making.
In addition to information about options, benefits, and harms, patients require active support in their decision-making process.
Clinicians could aim to avoid overfocus on patient autonomy and instead establish authentic, shared decisions, with a role for some clinician control if needed.
In Ontario, Canada, the first cohorts who were offered school-based human papillomavirus (HPV) vaccination are now eligible for cervical screening. We determined which screening strategies for these populations would result in optimal harms–benefits ratios of screening.
We used the hybrid microsimulation model STDSIM- MISCAN-Cervix to determine the harms and cancers prevented of 309 different primary HPV screening strategies, varying by screening ages and triage methods. In addition, we performed an unstratified (i.e., uniform screening protocols) and stratified (i.e., screening protocols by vaccination status) analysis. Harms induced were quantified as a weighted combination of the number of primary HPV-based screens and colposcopy referrals at 1:10. A harms–benefit acceptability threshold of number of harms induced for each cancer prevented was set at the estimated ratio under current screening recommendations in unvaccinated cohorts in Ontario.
For the unstratified scenario, 5 lifetime screens with HPV16/18 genotyping was optimal. For the stratified scenario, the optimal scenario was 3 lifetime screens with HPV16/18/31/33/45/52/58 genotyping for vaccinated individuals versus 6 lifetime screens with HPV16/18 genotyping for unvaccinated individuals.
We determined the optimal cervical screening strategy in Ontario over the next decades. To maintain an optimal harms–benefits balance of screening, the Ontario Cervical Screening Program could adjust screening recommendations in the future to reduce the number of lifetime screens and extend screening intervals to account for vaccinated cohorts. Stratified screening by vaccination status could further improve this balance on an individual level.
People in cohorts who were offered HPV vaccination as part of Ontario’s school-based program may achieve a better harms–benefits balance if cervical screening recommendations are updated to a less intensive protocol in future. This holds for the cohorts as a whole (i.e., unstratified screening) as well as for both vaccinated and unvaccinated individuals in these cohorts.
Instead of using a cost-effectiveness threshold, it is possible to determine optimal screening protocols by calculating an acceptability threshold using alternative harms–benefits measures based on existing policy.
Using univariate harms measures such as primary HPV screening tests or colposcopies per 1,000 people can yield biases in optimizing cervical screening programs. Alternatively, combining both primary screens and colposcopy referrals could provide a more accurate harms measure and result in optimal strategies with a better balance between harms and benefits.
The 2023 American College of Physicians (ACP) guidelines for colorectal cancer (CRC) screening are at odds with the United States Preventive Task Force (USPSTF) guidelines, with the former recommending screening starting at age 50 y and the latter at age 45 y. This article “stress tests” CRC colonoscopy screening strategies to investigate their robustness to uncertainties stemming from the natural history of disease and sensitivity of colonoscopy.
This study uses the CRC-SPIN microsimulation model to project the life-years gained (LYG) under several colonoscopy CRC screening strategies. The model was extended to include birth cohort effects on adenoma risk. We estimated natural history parameters under 2 different assumptions about the youngest age of adenoma initiation. For each, we generated 500 parameter sets to reflect uncertainty in the natural history parameters. We simulated 26 colonoscopy screening strategies and examined 4 different colonoscopy sensitivity assumptions, encompassing the range of sensitivities consistent with prior tandem colonoscopy studies. Across this set of scenarios, we identify efficient screening strategies and report posterior credible intervals for benefits of screening (LYG), burden (number of colonoscopies), and incremental burden-effectiveness ratios.
Projected absolute screening benefits varied widely based on assumptions, but strategies starting at age 45 y were consistently in the efficiency frontier. Strategies in which screening starts at age 50 y with 10-y intervals were never efficient, saving fewer life-years than starting screening at age 45 y and performing colonoscopies every 15 y while requiring more colonoscopies per person.
Decennial colonoscopy screening initiation at age 45 y remained a robust recommendation. Colonoscopy screening with a 10-y interval starting at age 50 y did not result in an efficient use of colonoscopies in any of the scenarios evaluated.
Colorectal cancer colonoscopy screening strategies initiated at age 45 y were projected to yield more life-years gained while requiring the least number of colonoscopies across different model assumptions about disease natural history and colonoscopy sensitivity.
Colonoscopy screening starting at age 50 y with a 10-y interval consistently underperformed strategies that started at age 45 y.
Epidemiological models benefit from incorporating detailed time-to-event data to understand how disease risk evolves. For example, decompensation risk in liver cirrhosis depends on sojourn time spent with cirrhosis. Semi-Markov and related models capture these details by modeling time-to-event distributions based on published survival data. However, implementations of semi-Markov processes rely on Monte Carlo sampling methods, which increase computational requirements and introduce stochastic variability. Explicitly calculating the evolving transition likelihood can avoid these issues and provide fast, reliable estimates.
We present the sojourn time density framework for computing semi-Markov and related models by calculating the evolving sojourn time probability density as a system of partial differential equations. The framework is parametrized by commonly used hazard and models the distribution of current disease state and sojourn time. We describe the mathematical background, a numerical method for computation, and an example model of liver disease.
Models developed with the sojourn time density framework can directly incorporate time-to-event data and serial events in a deterministic system. This increases the level of potential model detail over Markov-type models, improves parameter identifiability, and reduces computational burden and stochastic uncertainty compared with Monte Carlo methods. The example model of liver disease was able to accurately reproduce targets without extensive calibration or fitting and required minimal computational burden.
Explicitly modeling sojourn time distribution allows us to represent semi-Markov systems using detailed survival data from epidemiological studies without requiring sampling, avoiding the need for calibration, reducing computational time, and allowing for more robust probabilistic sensitivity analyses.
Time-inhomogeneous semi-Markov models and other time-to-event–based modeling approaches can capture risks that evolve over time spent with a disease.
We describe an approach to computing these models that represents them as partial differential equations representing the evolution of the sojourn time probability density.
This sojourn time density framework incorporates complex data sources on competing risks and serial events while minimizing computational complexity.
This is a visual representation of the abstract.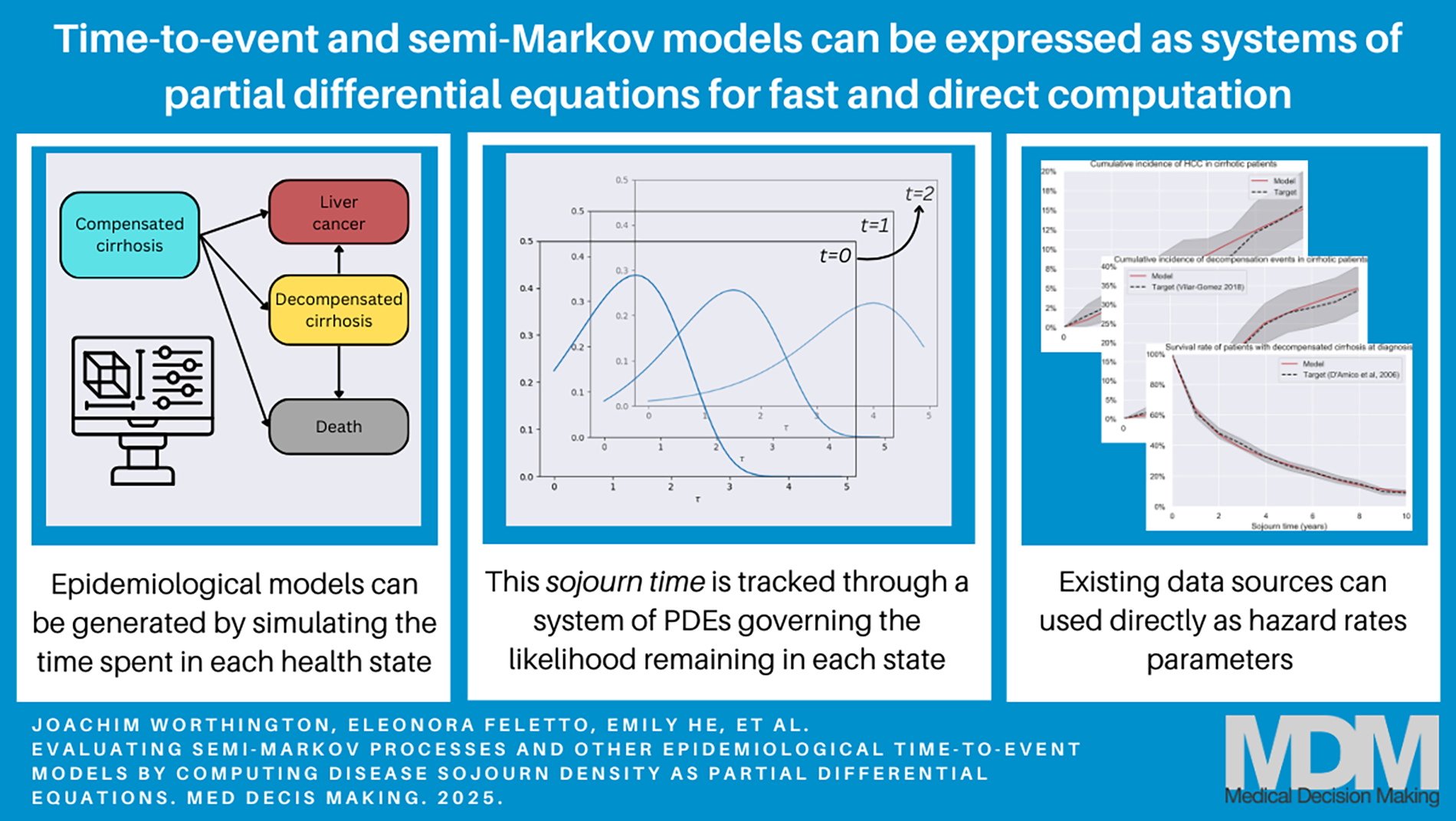
Intensive care unit (ICU) hospitalizations of very old patients with acute respiratory infection have risen. The decision-making process for ICU admission is multifaceted, and the prediction of long-term survival outcome is an important component. We hypothesized that data-driven algorithms could build long-term prediction by examining massive real-life data. Our objective was to assess machine learning (ML) algorithms to predict the 1-y survival of very old patients with severe respiratory infections.
A national 2011–2020 study of ICU patients ≥80 y with respiratory infection was carried out, using French hospital discharge databases. Data for the training cohort were collected from 2013 to 2016 to build the models, and the data of patients extracted in 2017 were used for external validation. Our proposed models were developed using random forest, logistic regression (LR), and XGBoost. The optimal model was selected based on its accuracy, sensitivity, specificity, Matthews coefficient correlation (MCC), receiver-operating characteristic curve (AUROC), and decision curve analysis (DCA). The local interpretable model-agnostic explanation (LIME) algorithm was used to analyze the contribution of individual features.
A total of 24,270 very old patients were hospitalized in the ICU for respiratory infection (2013–2017) with a known vital status at 1 y. The 1-y survival rate was 41.3% (median survival: 3 mo [2.7–3.3]). Of the 3 ML models tested, LR exhibited promising performance with an accuracy, sensitivity, specificity, MCC, and AUROC (95% confidence interval) of 0.65, 0.76, 0.60, 0.27, and 0.70 (0.69–0.72), respectively. LR achieved an AUROC of 0.70 (0.68–0.71) in external validation by temporal splitting. LR demonstrated higher net benefits across a range of threshold probability values in DCA. The LIME algorithm identified the 10 most influential features at an individual scale.
We demonstrated that a ML model has the potential to predict long-term outcomes for very old patients with acute respiratory infections. As a proof of concept, we proposed a program that acts as an “explainer” for the ML model. This work represents a step forward in translating ML models into practical, transparent, and reliable clinical tools to support medical decision making.
The decision to admit a very old patient to the ICU is one of the most complex challenges faced by intensivists, often relying on subjective judgment.
In this study, we evaluated the efficacy of machine learning algorithms in predicting the 1-y survival rate of critically ill very old patients (≥80 y) with severe respiratory infections, using data available prior to the admission decision.
Our findings demonstrate that machine learning can effectively predict long-term outcomes in very old patients. We used an innovative approach that aims to support medical decision making about admission in ICU.
This is a visual representation of the abstract.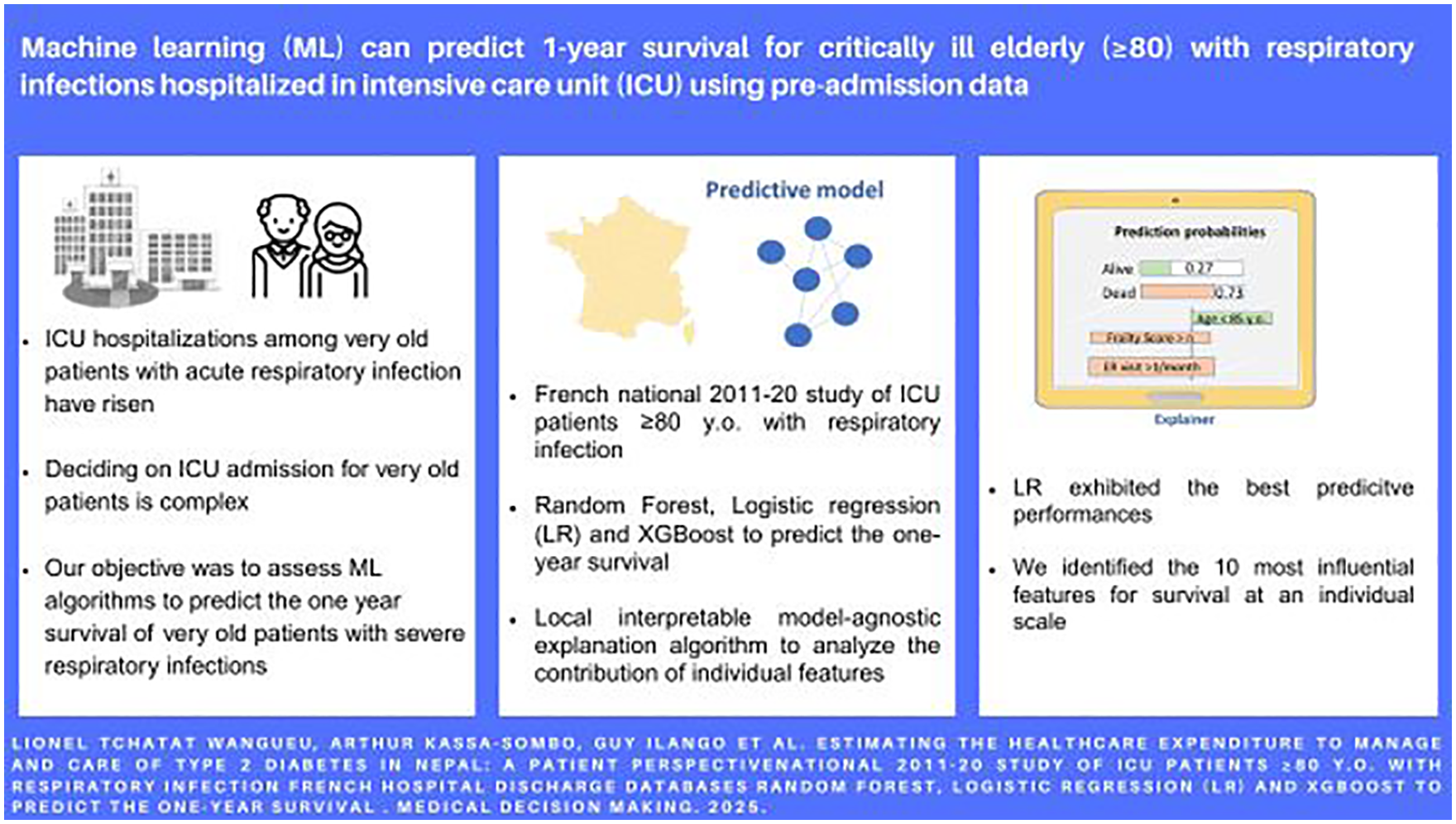
While structured expert elicitation (SEE) is gaining traction in health technology assessment in situations in which data are scarce, its application in practice remains limited. Co-designing a practical and fit-for-purpose SEE with experts could enhance its acceptability and feasibility in clinical research.
An SEE was co-designed with clinicians to elicit expert opinions on 3 uncertain quantities of interest (QoIs) for a decision-analytic model in exercise oncology.
A series of co-design meetings was convened to design 6 elicitation stages. Individual elicitation was conducted using the variable interval method (VIM), via videoconferencing. Linear pooling was adopted to generate group estimates. Semi-structured interviews were conducted after the elicitation exercise to gather the experts’ first-hand experience of the elicitation process and to identify areas for improvement. Qualitative data were transcribed and content analyzed.
Twelve experts participated in the co-designed SEE. Three beta distributions were derived and estimated from the experts’ responses: the relative risk reduction of cardiovascular events of exercise for women who survived early-stage endometrial cancer (Mean: 0.362, SD: 0.15), the probability that a clinician would refer a patient to the exercise program (Mean: 0.457, SD: 0.218), and the probability that a cancer patient would use such a health service upon referral (Mean: 0.446, SD: 0.203). Most of the experts’ first-hand experience of the co-designed SEE was positive. The qualitative feedback highlighted critical aspects of the elicitation process that should be designed and executed with caution when targeting clinicians with no prior experience of SEE.
This is the first expert elicitation conducted in exercise oncology. Engaging diverse stakeholders through co-design meetings and incorporating qualitative feedback proved effective and practical in introducing expert elicitation into clinical research.
Recent SEE guidelines aim to facilitate the conduct of expert elicitation in model-based economic evaluation, but its application in practice remains limited.
Engaging experts in the design of SEE could enhance its acceptability and feasibility in clinical research.
This is the first co-designed expert elicitation involving clinicians in the field of exercise oncology.
This practical approach to conducting SEE could promote a wider adoption to inform health care policy decisions when the evidence is lacking or uncertain.
Health interventions affect people’s welfare directly by impacting people’s health but also indirectly via a change in consumption and leisure time caused by the change in health. This study discusses 2 ongoing issues in the economic evaluation of health interventions. The first is how to value a change in the amount of leisure time of a patient. The second issue concerns the valuation of a change in production.
We present a theoretical model that assumes that individual utility depends on health, consumption, and leisure time. We assume that the total stock of time consists of 3 components: leisure time, working time, and recovery time. The model takes a societal perspective and assumes that individuals optimize their utility, conditional on time and budget restrictions.
For the first issue, the model indicates that the value of a change in the stock of time available for leisure and work has to be added to the direct effects of a health intervention, instead of only a change in work hours. For the second issue, the model indicates that in case of a change in longevity, only the change in taxes paid may be counted because the income change is included in the value of the change in quality-adjusted life-years. A numerical example shows that this approach may counterbalance the potential overestimation of the welfare effects of treatments with the human capital method and underestimation related to the friction cost method.
We propose a new method that includes the welfare effects of health interventions due to a change in the amount of leisure time and avoids double counting of welfare changes, which are included in the direct effects.
We present a theoretical model and use it to analyze 2 issues in the economic evaluation of health interventions: the inclusion of leisure time and the valuation of production.
The model indicates that the effects of health changes on the amount of both work and leisure hours need to be taken into account in economic evaluation.
As to the valuation of production, the model indicates that in case of a change in longevity, only the change in taxes may be counted.
We propose the “stock of time” method to value changes in working hours and leisure hours, which may counterbalance potential overestimates and underestimates in established methods.