Other
Select search scope: search across all journals or within the current journal
Since 2011, otolaryngologists have been required to complete a 1-year fellowship in sleep medicine in order to be eligible for the ABOto Sleep Medicine Certification Examination (ASMCE). Resultantly, the number of sleep medicine board-certified otolaryngologists has plunged since that time. This push toward extinction comes at a time when otolaryngologists have been cast into the spotlight for the diagnosis and treatment of obstructive sleep apnea, the prevailing disorder in sleep medicine. To reverse the trajectory of this subspecialty, 2 changes need to occur: increase the exposure to sleep medicine/surgery during residency and improve access to sleep medicine fellowships featuring a strong otolaryngology presence.
A systematic review and meta-analysis of the evidence on balloon Eustachian tuboplasty (BET) as a treatment modality for Eustachian tube dysfunction (ETD). We followed the PRISMA guideline and registered with PROSPERO No. CRD42014009461.
We searched 12 databases including PubMed and Embase from January 1, 2010, to April 7, 2014, for studies of BET. Endpoints: change in symptoms, middle ear pathology, eardrum status, Eustachian tube function tests, hearing, adverse events, complications, and health-related quality of life.
Study quality was assessed using the modified Delphi technique quality appraisal tool for case series studies. Risk of bias was assessed using the Cochrane Collaboration’s tool for assessing risk of bias.
Nine case series studies with 443 patients (642 tubes) were included. Population size n = 4 (7 tubes) to n = 210 (320 tubes). All studies were of poor quality and featured a high risk of bias. We found reduction of patient symptoms in ETD questionnaire (
The evidence of BET is poor and biased. No firm conclusions can be made to identify patients who will benefit from the procedure or to accurately predict surgical results. Randomized controlled trials or case-control trials are needed.
To perform a systematic review evaluating the association between sensorineural hearing loss and (1) nonsteroidal anti-inflammatory drugs (NSAIDs) as a class, (2) NSAIDs available over the counter, (3) NSAIDs in short intravenous courses, (4) prescription NSAIDs utilized by patients without systemic inflammatory conditions, (5) prescription NSAIDs in patients with arthritides, and (6) acetaminophen with and without concomitant narcotic usage.
Computerized searches of PubMed, EMBASE, and the Cochrane Library were updated through May 2014, along with manual searches and inquiries to topic experts.
The systematic review was performed according to an a priori protocol. Data extraction was performed by 2 independent investigators, and it focused on relevant audiologic measurements, methodological elements related to risk of bias, and potential confounders.
The 23 criterion-meeting studies included a total of 92,532 participants, with mixed results. Sulindac was the only specific agent to have been studied with formal audiometry in a randomized double-blind placebo-controlled trial in which hearing was the reported primary outcome: Although an effect was seen in the unadjusted analysis (pure tone threshold > 15 dB, 9.3% vs 2.9%; relative risk [RR], 3.2; confidence interval [CI], 1.09-9.55;
Data are varied regarding the impact of NSAIDs and acetaminophen on population hearing health.
The last few years have seen significant increase in the number of available clinical trials in head and neck cancer. It has been difficult to stay abreast of these efforts because multiple cooperative groups and institutions are engaged in their recruitment. This review presents the state of the art of available clinical trials organized around major research themes.
Published literature, published cooperative group monographs, expert review.
Initial themes in head and neck cancer clinical trial development were first identified along with examples. Opinions from an international panel of multidisciplinary experts were then solicited.
Current major themes of head and neck clinical trials centered on 5 major themes: (1) recognition of human papillomavirus oropharynx cancer and optimal treatment strategies, (2) defining the role of transoral surgery in head and neck cancer treatment, (3) improving postoperative adjuvant treatment, (4) investigation of rare malignancies, and (5) the importance of biomarker-driven, innovative, and targeted therapy investigation.
A number of exciting clinical trials are currently in development or accrual with the potential for tremendous impact and improvement of the treatment of head and neck cancer.
Awareness by practicing otolaryngologists and trainees of these current themes will be essential for study accrual, success, and improvement in the care of head and neck cancer.
To assess recent trends in the prevalence and quality of reporting of randomized controlled trials (RCTs) in 4 otolaryngology journals.
Methodology and reporting analysis.
Randomized controlled trials in 4 otolaryngology journals.
All RCTs published from 2011 to 2013 in 4 major otolaryngology journals were examined for characteristics of study design, quality of design and reporting, and funding.
Of 5279 articles published in 4 leading otolaryngology journals from 2011 to 2013, 189 (3.3%) were RCTs. The majority of RCTs were clinical studies (86%), with the largest proportion consisting of sinonasal topics (31%). Most interventions were medical (46%), followed by surgical (38%) and mixed (16%). In terms of quality, randomization method was reported in 54% of RCTs, blinding in 33%, and adverse events in 65%. Intention-to-treat analysis was used in 32%;
Based on review of 4 otolaryngology journals, RCTs are still a small proportion of all published studies in the field of otolaryngology. There seem to be trends toward improvement in quality of design and reporting of RCTs, although many quality features remain suboptimal. Practitioners both designing and interpreting RCTs should critically evaluate RCTs for quality.
To assess the role of preoperative serum 25 hydroxyvitamin D as predictor of hypocalcemia after total thyroidectomy.
Retrospective cohort study.
University teaching hospital.
All consecutively performed total and completion thyroidectomies from February 2007 to December 2013 were reviewed through a hospital database and patient charts. The relationship between postthyroidectomy laboratory hypocalcemia (serum calcium ≤2 mmol/L), clinical hypocalcemia, and preoperative serum 25 hydroxyvitamin D level was evaluated.
Two hundred thirteen patients were analyzed. The incidence of postoperative laboratory and clinical hypocalcemia was 19.7% and 17.8%, respectively. The incidence of laboratory and clinical hypocalcemia among severely deficient (<25 nmol/L), deficient (<50 nmol/L), insufficient (<75 nmol/L), and sufficient (≥75 nmol/L) serum 25 hydroxyvitamin D levels was 54% versus 33.9%, 10% versus 18%, 2.9% versus 11.6%, and 3.1% versus 0%, respectively. Multiple logistic regression analysis revealed preoperative severe vitamin D deficiency as a significant independent predictor of postoperative hypocalcemia (odds ratio [OR], 7.3; 95% confidence interval [CI], 2.3-22.9;
Postoperative clinical and laboratory hypocalcemia is significantly associated with low levels of serum 25 hydroxyvitamin D. Our findings identify severe vitamin D deficiency (<25 nmol/L) as an independent predictor of postoperative laboratory hypocalcemia. Early identification and management of patients at risk may reduce morbidity and costs.
To evaluate the association between modifiable patient risk factors including tobacco use, alcohol consumption, body mass index (BMI), and thyroid cancer.
Retrospective study with chart review.
Midwest university hospital.
Retrospective study comparing Midwest patients with thyroid cancer from our Thyroid Tumor and Cancer Registry with Midwest controls without a personal history of cancer. Descriptive statistics were created from patient questionnaires and chart reviews. Odds ratios (ORs) were reported for significant associations.
There were 467 patients with cancer and 255 controls. The thyroid cancer group included 404 papillary, 47 follicular, 13 medullary, and 3 anaplastic cancers. When comparing all patients with cancer with controls, smoking more than 100 lifetime cigarettes was associated with a reduced cancer risk (OR, 0.68; 95% confidence interval [CI], 0.50-0.94). Secondhand smoke exposure did not show a statistically significant relationship to thyroid cancer. Compared with never drinking, current drinking was associated with a reduced cancer risk (OR, 0.46; 95% CI, 0.29-0.73) as was consuming 1 to 2 drinks daily compared to drinking <1 drink daily (OR, 0.58; 95% CI, 0.34-0.89). There was no difference between median BMI at age 20 years, lifetime maximum BMI, or current BMI between patients with cancer and controls.
Our data showed no positive correlation between tobacco use, alcohol consumption, or obesity and thyroid cancer risk. Our data suggest that tobacco use and mild alcohol consumption may be associated with a slightly reduced risk of thyroid cancer. There was no association between BMI and thyroid cancer in our study population.
The present study was designed to evaluate 4D computerized tomography (CT) as a means of localizing abnormal parathyroid glands in primary hyperparathyroidism (HPT).
Case series with expertized image review.
Tertiary care hospital.
A total of 38 patients were recruited for study, all of whom had undergone focused parathyroidectomy for single-lesion primary HPT between June 2011 and September 2013. In each patient, 3 imaging procedures were performed: cervical ultrasonography (US), 99mTc-sestamibi SPECT/CT (SeS), and 4D CT. Collective imaging data were blindly reviewed and compared.
4D CT outperformed US and SeS in terms of sensitivity (
4D CT proved helpful in localizing target parathyroid glands of primary HPT that were missed by traditional imaging.
Septal spurs are exceedingly common structural deformities that contribute to nasal obstruction and often require surgical correction. The posterior extension of the quadrangular cartilage (PEQC) and its relationship with septal spurs have not been previously examined. We seek to examine the anatomic and histologic relationship of the PEQC and concurrent septal spurs in patients undergoing septoplasty.
Prospective cohort study.
Facial plastic and rhinology center in tertiary hospital setting.
Thirty patients with septal deviation are described in this series. The quadrangular cartilage and associated septal spur were removed en bloc from patients undergoing septoplasty. The length of the PEQC, the side of spur deviation, and the relationship of the PEQC to the spur (ipsilateral vs contralateral) were recorded.
The mean length of the PEQC, beyond the bony-cartilaginous junction, was 30.06 ± 6.06 mm. The PEQC was present on the ipsilateral side of the spur deviation in all 30 patients (100%).
At sites of septal spur formation, the quadrangular cartilage possesses an average 3-cm extension beyond its junction with the bony components of the septum. This cartilaginous extension is exclusively found on the same side of spur deviation. These findings have implications on our understanding of the ontogeny of commonly found septal spurs and deviations, as well as treatment strategies and cartilage graft harvesting.
To characterize patterns of utilization and outcomes following transfusion in head and neck patients undergoing free flap reconstruction.
Case series with chart review.
Tertiary academic medical center.
Two hundred eighty-two head and neck patients undergoing free flap reconstruction from 2011 to 2013. Outcome parameters included post-transfusion hematocrit increase, length of stay (LOS), flap survival, and perioperative complications.
Of all head and neck free flap patients, 48.9% received blood transfusions. Average pretransfusion hametocrit (Hct) was 24.7% ± 0.2% with 2.5 ± 0.1 units of blood transfused. Transfused patients were more likely to have been taken back to the operating room. Rates of transfusion were similar between flap types, although anterolateral thigh (ALT) and fibular free flap (FFF) patients had higher transfusion requirements compared to radial forearm free flap (RFFF) patients. Further, FFF patients trended toward receiving transfusions earlier. Transfusion did not influence flap survival but was associated with wound dehiscence, myocardial infarction, congestive heart failure, respiratory distress, and pneumonia. Subset analyses by flap type revealed that differences were significant among the RFFF and FFF cohorts but not ALT patients. When comparing patients who were transfused for Hct <21 to those transfused for Hct <27, there were no differences in LOS, flap survival, or postsurgical complications.
Among the different types of flaps, FFF and ALT are associated with higher transfusion requirements. Transfusion in patients undergoing free flap reconstruction does not significantly affect flap survival but was associated with perioperative complications. Our data support consideration of a restrictive transfusion policy in free flap patients.
“The Match” has become the accepted selection process for graduate medical education. Otomatch.com has provided an online forum for Otolaryngology–Head and Neck Surgery (OHNS) Match-related questions for over a decade. Herein, we aim to delineate the type of posts on Otomatch to better understand the perspective of medical students applying for OHNS residency.
Retrospective review of an OHNS Match-related online forum.
Subjects were contributors to an OHNS Match-related online forum. Posts on Otomatch between December 2001 and April 2014 were reviewed. The title of each thread and number of views were recorded for quantitative analysis. Each thread was organized into 1 of 6 major categories and 1 of 18 subcategories. National Resident Matching Program (NRMP) data were utilized for comparison.
We identified 1921 threads corresponding to over 2 million page views. Over 40% of threads were related to questions about specific programs, and 27% were discussions about interviews. Views, a surrogate measure for popularity, reflected different trends. The majority of individuals viewed posts on interviews (42%), program-specific questions (20%), and how to rank programs (11%). There was an increase in viewership tracked with a rise in applicant numbers based on NRMP data.
Our study provides an in-depth analysis of a popular discussion forum for medical students interested in the OHNS Match process. The most viewed posts are about interview dates and questions regarding specific programs. We provide suggestions to address unmet needs for medical students and potentially improve the Match process.
To determine the trend of number of tracheotomies performed by otolaryngologists.
Case series with chart review.
Tertiary referral center in central Pennsylvania.
All patients undergoing tracheotomy between 2000 and 2013.
Data were gathered from billing records and operative reports to determine the service performing the tracheotomy. In addition, the surgical technique and indication for surgery were recorded. Negative binomial regressions were conducted to examine the number of tracheotomies performed by each specialty as a function of year.
In 2000, 44% of tracheotomies were being performed by the otolaryngology service, compared with only 25% in 2013. This is a decline of 22% over time. Since 2000, general surgery steadily increased the number of tracheotomies performed in comparison to the steady decrease performed by otolaryngology. Since 2008, general surgeons have significantly increased the number of percutaneous tracheotomies they perform (76% per year). Over the same period, the number of tracheotomies performed by the cardiothoracic surgery service has steadily increased by 26% per year. Most of the tracheotomies performed by cardiothoracic surgery are percutaneous tracheotomies.
This study illustrates that otolaryngologists at our institution are performing fewer tracheotomies over time. If this trend continues, the experience of our trainees may become diluted through reduction in surgical volume. While multi-institutional studies are warranted, this review provides a summary of data collected at a tertiary care institution, which may reflect national trends.
The discovery of carbon monoxide (CO) and hydrogen sulfide (H2S) as pathogenic signaling molecules in airway-related diseases has led to significant insights into the pathophysiologic mechanisms underlying the development of allergic rhinitis (AR). The potential crosstalk between CO and H2S signaling pathways in AR has not been adequately investigated. This study was performed to elucidate the mechanistic relationship between CO and H2S in AR.
Experimental prospective animal study.
Animal laboratory of Tongji Hospital, Tongji University, Shanghai, China.
A well-established model of AR was used whereby guinea pigs (N = 24) were randomly divided into 4 treatment groups (n = 6 for each group): The first group received ovalbumin only; the second group was administered exogenous hemin, a CO-binding metalloporphyrin; the third group received zinc protoporphyrin, an inhibitor of heme oxygenase-1. A control group was challenged using only saline. Symptoms of AR were recorded, and quantitation of plasma CO and H2S levels was performed. Expression of heme oxygenase-1 and H2S-generating enzyme cystathionine-γ-lyase (CSE) were measured from nasal mucosa.
Plasma CO and heme oxygenase-1 expression levels of nasal mucosa were significantly increased in the AR group compared to controls, whereas H2S concentrations were significantly decreased. Exogenous administration of CO exacerbated allergic symptoms, resulting in higher levels of both CO and heme oxygenase-1 expression, and a further reduction in H2S levels and CSE expression. Zinc protoporphyrin decreased CO concentrations and increased levels of both H2S and CSE expression.
Results indicated an inverse relationship between H2S levels and CO in the pathogenesis of AR.
To determine if the manner in which a tuning fork is activated affects its vibrational response.
Diagnostic test assessment.
Hearing Center of Excellence laboratory.
A Polytec OFV-5000 scanning vibrometer was used to measure the vibrational response of 256-Hz, 512-Hz, and 1024-Hz tuning forks after activation. The tuning forks were activated to varying intensities by striking 4 unique surfaces: the head, palm, a metal surface, and a wood table.
The fundamental frequency of the individual tuning fork was the dominant observed frequency in all testing scenarios. Additional nonharmonic frequencies were noted when the 256-Hz and 512-Hz tuning forks were struck off metal and wooden surfaces.
Additional nonfundamental sound frequencies produced secondary to striking a tuning fork off a metal object or a wooden table could affect clinical tuning fork examination and complicate decisions regarding surgical candidacy.
To investigate the association between perioperative patient characteristics and treatment modalities (eg, vasopressor use and volume of fluid administration) with complications and failure rates in patients undergoing head and neck free tissue transfer (FTT).
A retrospective review of medical records.
Perioperative hospitalization for head and neck FTT at 1 tertiary care medical center between January 1, 2009, and October 31, 2011.
Consecutive patients (N = 235) who underwent head and neck FTT. Demographic, patient characteristic, and intraoperative data were extracted from medical records. Complication and failure rates within the first 30 days were collected
In a multivariate analysis controlling for age, sex, ethnicity, reason for receiving flap, and type and volume of fluid given, perioperative complication was significantly associated with surgical blood loss (
FTT complications were associated with surgical blood loss but not the use of vasoactive drugs. For patients undergoing FTT, judicious monitoring of blood loss may help stratify the risk of complication and failure.
Complaints of dysphagia for solids lead to speech-language pathology (SLP) referral. Yet many of these patients are later diagnosed with esophageal rather than oropharyngeal dysphagia. Fluoroscopic screening involving the oropharynx alone fails to identify these patients. The aim of this study was to investigate the prevalence of esophageal abnormalities in an SLP-led videofluoroscopic study of swallowing (VFSS) clinic.
Prospective, observational study.
Radiology suite, public hospital.
In total, 111 consecutive mixed-etiology patients referred to the clinic by otorhinolaryngology (ORL) (59) or by a speech-language pathologist (52) were recruited. A VFSS was performed according to protocol, and at completion, esophageal visualization (in anterior-posterior plane) was performed by administration of a large liquid barium bolus and a barium capsule. All VFSS recordings were analyzed using objective digital measures of timing and displacement.
Sixty-eight percent of patients had an abnormal esophageal transit. One-third of those referred presented exclusively with esophageal abnormalities, while one-third had both oropharyngeal and esophageal abnormalities. Oral abnormalities, reduced pharyngoesophageal segment maximum opening (PESmax), and increasing age were significantly associated with esophageal abnormalities.
Fluoroscopic evaluation of the pharynx alone, without esophageal review, risks incomplete diagnosis of patients with esophageal disorders. Using esophageal visualization allows timely referral for further investigation by appropriate medical specialties, avoiding incomplete management of patients with dysphagia.
This randomized trial investigated voice rest and supplemental text-to-speech communication versus voice rest alone on visual analog scale measures of communication effectiveness and magnitude of voice use.
Randomized clinical trial.
Multicenter outpatient voice clinics.
Thirty-seven patients undergoing phonomicrosurgery.
Patients undergoing phonomicrosurgery were randomized to voice rest and supplemental text-to-speech communication or voice rest alone. The primary outcome measure was the impact of voice rest on ability to communicate effectively over a 7-day period. Pre- and postoperative magnitude of voice use was also measured as an observational outcome.
Patients randomized to voice rest and supplemental text-to-speech communication reported higher median communication effectiveness on each postoperative day compared to those randomized to voice rest alone, with significantly higher median communication effectiveness on postoperative days 3 (
Supplemental text-to-speech communication increased patient-perceived communication effectiveness on postoperative days 3 and 5 over voice rest alone. With the prevalence of smartphones and the widespread use of text messaging, supplemental text-to-speech communication may provide an accessible and cost-effective communication option for patients on vocal restrictions.
The titanium stapes footplate prosthesis (FPP) was designed to ensure a stable connection of a total ossicular replacement prosthesis (TORP) to the stapes footplate and maximize acoustic coupling by centering the footplate on the oval window. Our goal was to assess the impact of the FPP on TORP ossiculoplasty outcomes.
Case series with chart review.
Tertiary care center.
Adult patients undergoing TORP ossiculoplasty with (n = 53) or without (n = 108) a stapes FPP.
Rate of prosthesis displacement and audiologic outcomes were tabulated for statistical analysis.
A lower rate of prosthesis displacement and statistically better audiologic outcomes were seen in FPP patients. The pure-tone average air-bone gap (PTA-ABG) was closed to <20 dB in 69.8% (37/53) of patients in the study arm and 44.4% (48/108) of patients in the control arm (
Use of the titanium stapes FPP during TORP ossiculoplasty provides a statistically significant advantage in short-term PTA-ABG closure and a higher rate of successful rehabilitation of conductive hearing loss. Further studies are necessary to assess any long-term advantages a FPP may offer.
This study describes the presentation of first branchial cleft anomalies and compares outcomes of first branchial cleft with other branchial cleft anomalies with attention to otologic findings.
Case series with chart review.
Pediatric tertiary care facility.
Surgical databases were queried to identify children with branchial cleft anomalies. Descriptive analysis defined sample characteristics. Risk estimates were calculated using Fisher’s exact test.
Queries identified 126 subjects: 27 (21.4%) had first branchial cleft anomalies, 80 (63.4%) had second, and 19 (15.1%) had third or fourth. Children with first anomalies often presented with otologic complications, including otorrhea (22.2%), otitis media (25.9%), and cholesteatoma (14.8%). Of 80 children with second branchial cleft anomalies, only 3 (3.8%) had otitis. Compared with children with second anomalies, children with first anomalies had a greater risk of requiring primary incision and drainage: 16 (59.3%) vs 2 (2.5%) (relative risk [RR], 3.5; 95% confidence interval [CI], 2.4-5;
Children with first branchial cleft anomalies often present with otologic complaints. They are at increased risk of persistent disease, particularly if anomalies lie medial to the facial nerve. They may require ear-specific surgery such as tympanoplasty.
To assess for the presence of human herpesvirus (HHV) using immunohistochemical and polymerase chain reaction (PCR) assay in surgically excised vestibular schwannoma (VS) samples.
Cross-sectional study.
A retrospective laboratory-based study of tumors from patients with vestibular schwannoma.
Tissue microarrays (TMAs) representing sporadic and NF2-associated VS from 121 patients, as well as appropriate positive and negative controls, were studied. TMA sections were immunostained using antibodies directed against HHV-1, HHV-2, HHV-3, HHV-4, HHV-5, and HHV-8. PCR was used for the detection of all 8 known human herpesviruses.
There was no detectable HHV (HHV-1, HHV-2, HHV-3, HHV-4, HHV-5, HHV-8) by immunohistochemistry in any of the 121 cases of sporadic and NF2 cases analyzed. These data were further validated by DNA sequence analyses using PCR in a subset of the VS samples, all of which were found to be negative for all HHV.
The data offer no support for an association between HHV and the development of sporadic or NF2-associated VS in humans.
A consistent management algorithm for subjective tinnitus remains to be elucidated. Chronic tinnitus yields approximately US$2110 in annual health care costs per patient. However, it is unclear whether spending more in the management of tinnitus equates with greater patient satisfaction. Thus, the aim of this study is to correlate patient satisfaction with patient demographics, provider recommendations, and total health care–related expenditures.
A retrospective chart review and a patient satisfaction questionnaire.
All data were collected from a large Midwestern hospital.
Patients were included who presented to the tinnitus clinic during the year 2011 and were between the ages of 18 and 89 years. They were excluded with diagnoses of Ménière’s disease, pulsatile tinnitus, acoustic neuromas, or autoimmune inner ear diseases. The retrospective data and satisfaction surveys were entered by 3 of the authors. Responses were based on Likert scales.
Of the 692 patients included, 230 completed and returned the satisfaction questionnaire (33.2% response rate), yielding an overall mean of $662.60 charges. The frequency of intervention recommendations per patients ranged from 0 to 13, with a median of 4. Spearman’s correlations did not result in significant correlations between patient satisfaction and number of clinic visits (
Given that the variability among provider recommendations, the high overall mean of tinnitus-related charges, and patient satisfaction was not related to costs, further research is needed examining patient preference in the treatment of tinnitus.
(1) To describe outcomes from and modifications to the hybrid laryngotracheal reconstruction (LTR) technique and (2) to compare this technique to traditional single- and double-stage LTR (ssLTR/dsLTR).
Chart review with case series.
Tertiary care otolaryngology specialty hospital.
All patients under 18 years of age who underwent LTR by a single surgeon from July 1, 2009, to December 31, 2013.
Charts were assessed for age, gender, etiology of stenosis, type of reconstruction, comorbidities, length of stay, complications, and tracheostomy status. Analysis was performed using Kruskal-Wallis and Wilcoxon rank sum analysis.
Forty-four patients were identified, with 13 hybrid LTRs, 27 ssLTRs, and 4 dsLTRs. Of the hybrid LTRs, an overall decannulation rate of 76.9% was noted, comparable to those for dsLTR. The hybrid LTR technique offered a significantly shorter period of narcotic use when compared to ssLTR (median 15 vs 21 days,
The hybrid LTR technique is well tolerated and useful in patients of all ages. Narcotics can be weaned more quickly due to the presence of a secure airway at all times via the existing tracheostomy. Use of a long stent prevents formation of granulation tissue that may be seen with a suprastomal stent. This technique should be considered in patients with high-grade stenosis with a preexisting tracheostomy.
To compare local infiltration of dexamethasone to intravenous injection for postoperative pain and recovery after tonsillectomy.
Prospective, randomized study.
Second Affiliated Hospital of Harbin Medical University.
Children (n = 240, American Society of Anesthesiologists [ASA] classes I-II, aged 5-10 y) scheduled for tonsillectomy were randomly and equally assigned to 3 groups: DEX-IV, for intravenous injection of dexamethasone (0.5 mg/kg, maximum dose 24 mg); DEX-INF, given the same amount of dexamethasone by local infiltration to the upper middle and lower poles of the tonsils; and a control group not given dexamethasone. Postoperative pain was scored at intervals from 30 minutes to 24 hours. The time to first administration of analgesic and average consumption of analgesic, times to first oral water and solid food intake, and incidence rates of nausea and vomiting were evaluated.
From postoperative 1 to 16 hours, the DEX-INF group had significantly lower pain scores than did the DEX-IV group, and the time to first analgesic and average consumption of analgesic were also significantly lower. The times to first oral water and food intake in the DEX-INF group were significantly shorter than in the DEX-IV group. The incidence of nausea and vomiting in the DEX-INF group was higher than that of the DEX-IV group.
Local infiltration of dexamethasone was more effective than systemic administration to decrease pain and time to food intake, but the antiemetic effect was less.
Clinical trials registration number: ChiCTR-TRC-13003535.
Sinonasal disease is a common condition treated by otolaryngologists. Malpractice in this area is the most common litigation faced by otolaryngologists. This study analyzes malpractice in the treatment of sinonasal disease.
Case series, review of legal records.
Legal databases.
Using 2 different computerized legal databases, the phrase
Chronic sinusitis (42%) was the most common presenting symptom. Many cases included multiple types of alleged malpractice, with the most common being negligent technique (38%) and lack of informed consent (27%). The most common alleged injuries included cerebrospinal fluid leak, meningitis, nasal obstruction, and orbital trauma. Defendants prevailed in 13 of 18 cases in which outcomes were known, with mean award of $225,000 and mean settlement of $212,500. The cases won by plaintiffs were all in a private practice setting.
Otolaryngologists should be aware of the causes of malpractice litigation as it relates to treatment of sinonasal disease. Lack of informed consent continues to be a common allegation, and surgeons should ensure complete informed consent is obtained and well documented. A unified and complete database of medical malpractice cases is needed to allow for further analysis of specialty-related claims.
Allergic fungal rhinosinusitis (AFRS) may present with significant bone erosion of the orbital walls or cranial base. Although proptosis is fairly common, cranial neuropathies are rarely reported. The objectives of this study are to describe strategies for AFRS-induced neuropathies and evaluate ophthalmologic outcomes following endoscopic sinus surgery.
Case series with chart review.
Tertiary referral center.
A retrospective review identified 9 patients treated from 2008 to 2014 with AFRS-induced cranial neuropathies. Data regarding patient demographics, preoperative imaging, ophthalmologic symptoms, surgical intervention, histopathologic findings, and postoperative sinonasal and ophthalmologic outcomes were recorded.
Patients with AFRS (average age, 38 years) presented with optic neuropathy or abducens nerve palsy. Clinical presentation included unilateral visual loss secondary to optic nerve compression (n = 5), diplopia from unilateral (n = 2) or bilateral (n = 1) abducens nerve palsy, and bitemporal hemianopsia secondary to optic chiasm compression (n = 1). On average, the duration of ocular symptoms was 17 days. All patients underwent endoscopic surgical decompression of the sinuses and oral steroid therapy. Two individuals had an additional optic nerve decompression at the time of surgery. Seven patients had complete return of nerve function, whereas 2 had partial recovery at an average of 5 weeks following surgery.
Bone erosion of the sphenoid sinus walls by AFRS can lead to compression of surrounding neural structures producing cranial neuropathies. Identification of these symptoms and prompt surgical decompression and removal of disease, along with aggressive medical therapy, provided excellent outcomes in the current series of patients.
To evaluate the impact of early versus delayed endoscopic sinus surgery (ESS) in terms of postoperative health care utilization, using a patient cohort with chronic rhinosinusitis (CRS).
Retrospective administrative database analysis.
US-based primary and secondary sites of care.
CRS patients with ESS in 2010—with no other ESS before 2010 and with complete medical history from 2004 to 2012—were identified within the MarketScan database. Patients were characterized by time interval of first sinusitis or nasal polyposis diagnosis to ESS and grouped as following: group 1, < 1 year (n = 818); group 2, 1 to <2 years (n = 247); group 3, 2 to <3 years (n = 274); group 4, 3 to <4 years (n = 364); group 5, 4 to <5 years (n = 595); and group 6, ≥5 years (n = 535). Outpatient visits/procedures and prescriptions associated with sinusitis and/or nasal polyps were analyzed for 1 year preoperatively and 2 years postoperatively. Subanalyses were conducted on separate cohorts with or without asthma or polyps, within each group.
Patients in group 1 had significantly fewer visits and prescriptions than patients in group 6 (postoperative visits: group 1, 4.45 [95% CI, 4.06-4.84]; group 6, 6.70 [95% CI, 6.10-7.30; prescriptions: group 1, 4.54 [95% CI, 4.12-4.96]; group 6, 7.61 [95% CI, 6.92-8.31]). Gradual increases in utilization were observed from groups 1 to 6. Subanalysis of patients with and without asthma or polyps showed similar findings.
Early intervention after diagnoses of CRS, with or without asthma or polyps, is associated with lower health care utilization than intervention after many years of medical management.
To report improvements in childhood obstructive sleep apnea (OSA) and hypertension after adenotonsillectomy.
Case series with planned data collection.
Tertiary referral center.
Fifty consecutive patients (36 boys and 14 girls; median age, 7.0 years) who underwent plasma knife–assisted total tonsillectomy and adenoidectomy for OSA between January 2010 and March 2013 were assessed with the body mass index
The median follow-up period was 9.6 months. Postoperatively, the median AHI significantly reduced from 9.8 to 1.6 (
The decreased hypertension rate indicates that a reduction of the AHI is not all that matters after adenotonsillectomy in childhood OSA. However, patients with preoperative severe OSA and hypertension need careful management of their elevated BP despite surgical treatment.
To assess pediatric habitual snoring (PS) using home sleep test (HST) technology and attempt to correlate the objective components of PS to specific upper airway anatomy. In addition, the effects of adenotonsillectomy (± turbinoplasty) on objective measures of PS were evaluated.
Prospective cohort study.
Tertiary medical center.
Pediatric patients with a chief complaint of snoring and probable obstructive sleep apnea underwent an HST (SNAP Diagnostics, Wheeling, Illinois) with a detailed acoustical snoring analysis prior to adenotonsillectomy (± turbinoplasty). During surgery, detailed anatomical measurements were performed and correlated to snoring analysis results. After surgery, patients were offered another HST with snoring analysis. Data analysis was performed using descriptive statistics and statistical correlation with attention to the multiple-comparisons paradox.
Twenty-two patients (45% male; mean age, 5.4 years [range, 2.4-8.4 years]) completed the preoperative HST and operative measurements. Unlike typical adult snoring, only a minority of PS was from palatal flutter (mean palatal component, 24%; median, 10%). The resistance occurrence percentage (ROP, percentage of breathing events with snoring noise) was associated with body mass index (BMI; Spearman ρ = 0.55;
Pediatric snoring has different acoustical characteristics than adult snoring. Objective PS is associated with BMI, turbinate size, and palatal obstruction. Adenotonsillectomy (± turbinoplasty) may significantly reduce objective PS.


Advanced skin malignancies involving the temporal bone can involve the temporomandibular joint and glenoid fossa. Many of these tumors can be removed with a lateral temporal bone resection; however, extensive involvement of the glenoid fossa should include an en bloc resection of the temporal bone, glenoid fossa, and condyle. We describe a novel surgical approach that is an extension of a temporal bone resection that includes the glenoid fossa and condyle in an en bloc resection with the temporal bone. This procedure has been performed in 7 patients with advanced carcinoma of the temporal bone involving the glenoid fossa. There were no short-term complications as a result of the surgical approach. The addition of a middle fossa craniotomy and inclusion of the glenoid fossa and condyle as part of an en bloc resection of the temporal bone can be performed safely.
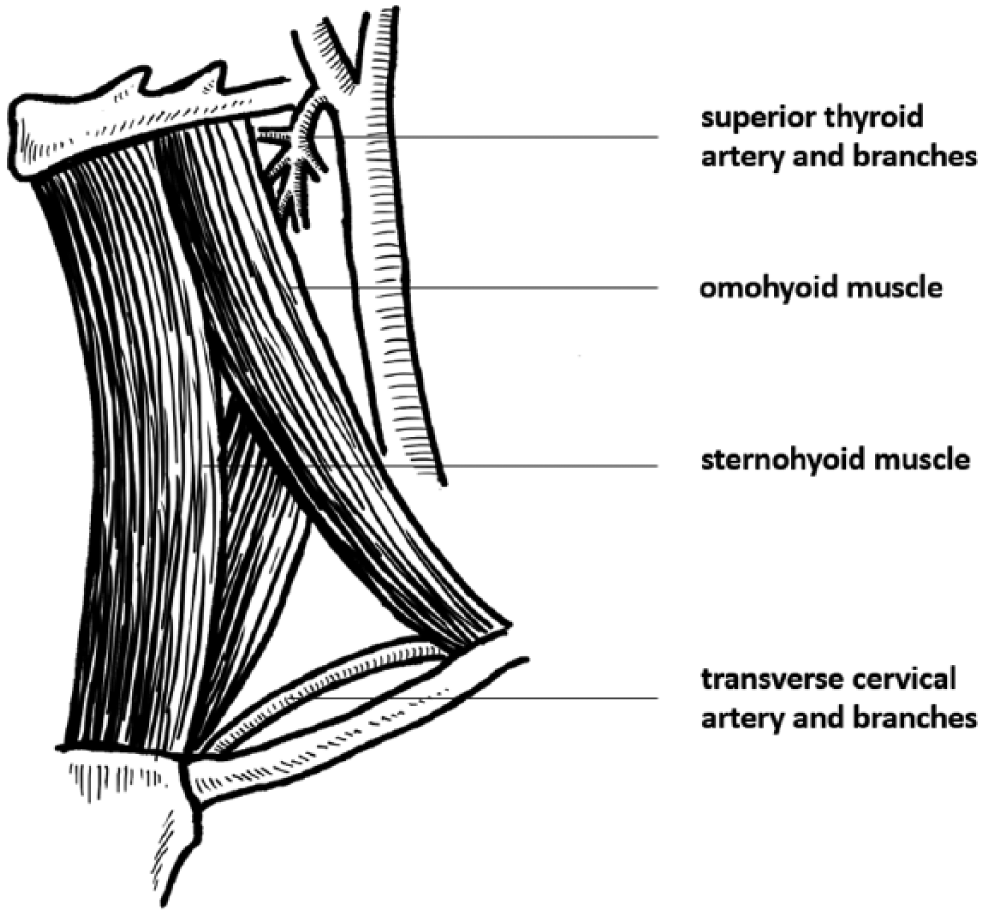
Yu Y, Wang X, Xu Z, Wu Y. Laryngeal reconstruction with a sternohyoid muscle flap after supracricoid laryngectomy: postoperative respiratory and swallowing evaluation.
In the above-mentioned article, the muscles in