
Article commentary
Early innovation to avoid late peritonitis-related complications
Muthana Al SahlawiORCID
Select search scope: search across all journals or within the current journal
Effective treatment of infections is a growing challenge owing to antimicrobial resistance. Peritoneal dialysis (PD) patients experience more frequent hospitalisations than the general population and have greater exposure to antibiotics, making them particularly vulnerable to this threat. Over the last decade, we have noted a surge in cases of complicated peritoneal dialysis–associated peritonitis (PD peritonitis) caused by antimicrobial-resistant organisms, including extended-spectrum beta-lactamase (ESBL), AmpC beta-lactamase-producing Enterobacterales,
Periplex® is a rapid point-of-care test based on the detection of interleukin-6 (IL-6) or matrix metalloproteinase-8 (MMP-8) to diagnose peritonitis in peritoneal dialysis (PD) patients.
This single-centre study was conducted in Singapore General Hospital from 2019 to 2022. The study recruited PD patients suspected of having peritonitis. Periplex was performed at the presentation and recovery of peritonitis. Primary outcomes were sensitivity and specificity of Periplex at presentation. The positive and negative predictive values of tests were also performed.
A total of 120 patients were included in the study. The mean age was 60.9 ± 14.9 years, 53% were male, 79% were Chinese and 47.5% had diabetes mellitus. Periplex was positive in all patients with peritonitis (
Periplex had high sensitivity, and positive and negative predictive values in the diagnosis of peritonitis can be considered as a screening tool for peritonitis. Given its high specificity and negative predictive value, it may also be used to document the resolution of peritonitis.
The risk of peritonitis has limited wider adoption of peritoneal dialysis (PD) in the United States. We developed a prototype bedside dialysate turbidity monitoring system, aiming to improve diagnostic accuracy relative to conventional approaches which depend on visual inspection and reporting of insensitive and non-specific symptoms.
The prototype system was tested in a single-centre, proof-of-principle clinical study in patients receiving intermittent PD. We obtained multiple effluent dialysate samples from each consenting participant. We compared turbidity measurements with diagnostic criteria endorsed by the International Society of Peritoneal Dialysis (ISPD).
Overall, we analysed 983 specimens from 65 patients, including 105 samples from patients with peritonitis and 878 samples from patients without peritonitis. An operating point derived from a previous in vitro study yielded an unadjusted sensitivity and specificity of 95.2% and 91.5%, respectively. The majority of samples that did not meet ISPD diagnostic criteria were either cases detected before criteria were met or were related to active peritonitis treatment and resolution.
This proof-of-principle study demonstrates the feasibility and diagnostic accuracy of a prototype dialysate turbidity monitoring system for peritonitis surveillance.
Cat ownership is common in peritoneal dialysis (PD) patients, even with recent guidelines recommending avoiding domestic animals during PD exchanges to limit the risk of peritonitis due to pet contamination. We analysed the outcomes of patients who experienced cat-related peritonitis compared with those who experienced peritonitis due to other causes.
This retrospective study based on the Registre de Dialyse Peritoneale de Langue Française data analysed the outcomes of 52 patients experiencing cat-related peritonitis from the beginning of the database (1986) until 21 June 2022 compared with those of 208 matched patients experiencing peritonitis due to other causes. A Cox regression model examined the association between cat-related peritonitis and the composite end point of death in PD or transfer to haemodialysis (HD), death in PD and transfer to HD.
Among patients with an episode of cat-related peritonitis, 11 (21.1%) died, 19 (36.5%) were transferred to HD and 11 (21.1%) were transplanted. In the group with other causes of peritonitis, these numbers were 67 (32%), 81 (39%) and 26 (12.5%), respectively. In multivariate survival analysis, age (hazard ratio (HR): 1.39; 95% confidence interval (CI): 1.13–1.70) and use of assisted PD (HR: 4.07; 95% CI: 2.11–7.86) were associated with the risk of death. Having experienced cat-related peritonitis was not significantly associated with any of the three outcomes (death, transfer to HD or PD cessation).
Patients on PD should be aware that cats may cause a peritoneal infection, which results in similar consequences to those of other causes of peritonitis. However, pets at home should not be considered a contraindication to PD.
Intraperitoneal antibiotics may be required daily for up to three weeks to treat peritoneal dialysis (PD)-related peritonitis. In some jurisdictions, antibiotic-admixed PD solutions are required to be used within 24 h due to concerns regarding microbial contamination and growth. This requires patients to attend the PD unit daily or alternatively for staff to perform home delivery with associated transport, staffing and cost implications.
The aim of this study was to determine if significant microbial growth occurs in PD solutions following their injection with antibiotic or sterile water.
Twelve PD solution bags were admixed with cefazolin sodium 1 g, diluted in 10 mL sterile water, while a further 12 PD solution bags were admixed with 10 mL sterile water using aseptic technique (AT) under supervision. All bags were stored at room temperature. Three bags from each experimental group were sampled for microbiologic culture at 0-, 24-, 48- and 72-h intervals.
One sterile water admixed bag sampled at 24 h yielded a
Antibiotic-admixed PD solutions prepared using AT and stored at room temperature remained sterile for up to 72 h. This suggests that patients can be safely issued with a supply of antibiotic-admixed PD bags for up to three days at a time.
Intraperitoneal (IP) aminoglycosides (AGs) continue to be the cornerstone of empiric management of peritonitis. AG dosing during automated peritoneal dialysis (APD), however, has not been well studied in patients with peritonitis. We sought to identify differences in AG exposure in the peritoneum and plasma for two different dosing regimens with little supporting evidence in patients on APD with peritonitis.
A retrospective design that utilised the peritoneal and plasma concentration–time data from a prior study of 18 continuous ambulatory peritoneal dialysis (CAPD) patients with peritonitis to generate an in silico peritoneal and plasma PK model. This model was then used to compare via simulation using Phoenix© WinNonlin Software with IP AG dosing for a loading-dose regimen (1.5 mg/kg first dose) versus a fixed-dose regimen (0.6 mg/kg/d) in patients on APD with peritonitis.
Outcome measures were (1) percentage of time where peritoneal peak concentrations/minimal inhibitory concentration (MIC) ratio >10, (2) AUC/MIC > 74 and (3) plasma Cmin concentrations. Both regimens resulted in > 90% optimal peak/MIC ratio and AUC/MIC ratios on days 1 and 5 of the dose protocol. The loading-dose regimen resulted in IP exposures that were 2.5 times greater in the peritoneal compartment on day 1. By day 5, both protocols resulted in similar accumulation of AG plasma Cmin concentrations of 2.5–3.4 mg/L versus 2.4–3.3 mg/L, respectively, for the loading-dose regimen versus fixed-dose regimen.
The current international guidelines for the treatment of peritoneal dialysis-associated peritonitis can continue to recommend the fixed-dose regimen for those on APD with the addition of plasma Cmin monitoring after 3 days to assess for drug accumulation.
Acute kidney injury (AKI) occurs frequently in the neurocritical intensive care unit and is associated with greater morbidity and mortality. AKI and its treatment, including acute kidney replacement therapy, can expose patients to a secondary greater brain injury. This study aimed to explore the role of peritoneal dialysis (PD) in neurocritical AKI patients in relation to metabolic and fluid control, complications related to PD and outcome.
Neurocritical AKI patients were treated by PD (prescribed Kt/V = 0.40/session) using a flexible catheter and a cycler and lactate as a buffer.
A total of 58 patients were included. The mean age was 61.8 ± 13.2 years, 65.5% were in the intensive care unit, 68.5% needed intravenous inotropic agents, 72.4% were on mechanical ventilation, APACHE II was 16 ± 6.67 and the main neurological diagnoses were stroke (25.9%) and intracerebral haemorrhage (31%). Ischaemic acute tubular necrosis (iATN) was the most common cause of AKI (51.7%), followed by nephrotoxic ATN AKI (25.8%). The main dialysis indications were uraemia and hypervolemia. Blood urea and creatinine levels stabilised after four sessions at around 48 ± 11 mg/dL and 2.9 ± 0.4 mg/dL, respectively. Negative fluid balance and ultrafiltration increased progressively and stabilised around 2.1 ± 0.4 L /day. Weekly delivered Kt/V was 2.6 ± 0.31. The median number of high-volume PD sessions was 6 (4–10). Peritonitis and mechanical complications were not frequent (8.6% and 10.3%, respectively). Mortality rate was 58.6%. Logistic regression identified as factors associated with death in neurocritical AKI patients: age (odds ratio (OR) = 1.14, 95% confidence interval (CI) = 1.09–2.16,
Our study suggests that careful prescription may contribute to providing adequate treatment for most neurocritical AKI patients without contraindications for PD use, allowing adequate metabolic and fluid control, with no increase in the number of infectious, mechanical and metabolic complications. Mechanical ventilation, positive fluid balance and intracerebral haemorrhage were factors associated with mortality, while patients with nephrotoxic AKI had lower odds of mortality compared to those with septic and ischaemic AKI. Further studies are needed to investigate better the role of PD in neurocritical patients with AKI.
This is a visual representation of the abstract.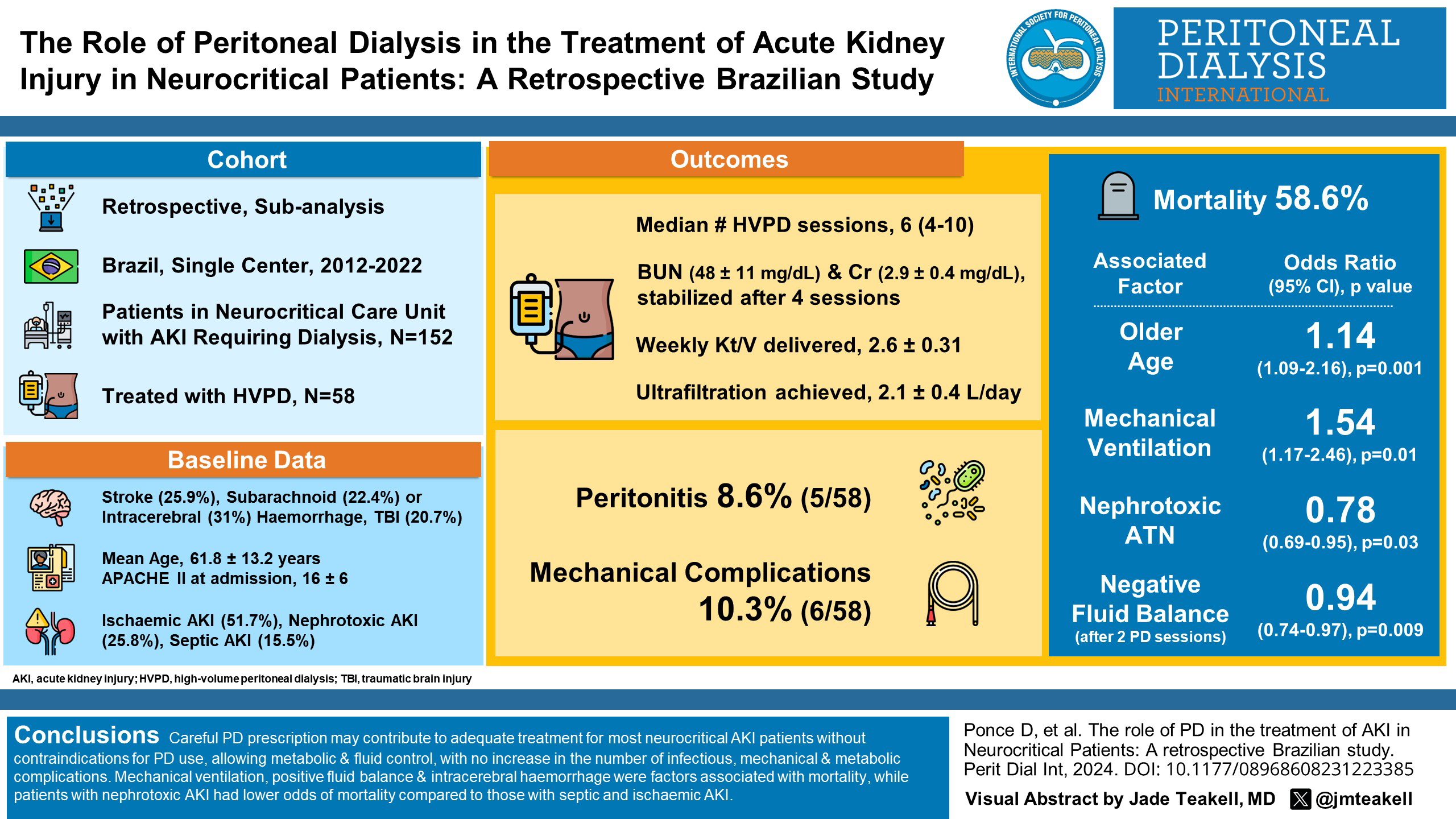
Peritoneal dialysis (PD) patients who undergo gastroendoscopy and colonoscopy are at increased risk of peritoneal dialysis-associated peritonitis (PD peritonitis) following the procedure (defined as occurring within 7 days of intervention). As per current International Society for PD (ISPD) guidelines, antibiotic prophylaxis is currently recommended pre-colonoscopy in PD patients given the risk of post-colonoscopy PD peritonitis. The risk of PD peritonitis in patients undergoing capsule endoscopy (CE) is unknown. This binational data-linkage study between the Australia and New Zealand Dialysis and Transplant Registry and all hospital admission data sets in Australia and New Zealand evaluated all patients with PD who underwent CE between 2006 and 2015. The objective of the study was to assess the risk of PD peritonitis in patients undergoing CE. Descriptive statistics were used to describe patient characteristics and clinical outcomes. Overall, 23 patients with PD underwent CE. Twelve patients underwent CE alone (i.e. no other concomitant procedures) and none of these patients experienced an episode of PD peritonitis. The remaining 11 patients underwent CE and other invasive endoscopic/abdominal surgical procedures, of whom 2 suffered PD peritonitis. CE is likely a relatively safe procedure in PD patients. PD patients undergoing CE may not require prior antibiotic prophylaxis. Given their relative safety, CE may be an appealing diagnostic tool in a select group of PD patients for the investigation of gastrointestinal disease.
Peritoneal dialysis (PD)-related infection rates have improved, but serious complications such as liver abscesses remain an issue, posing unique management challenges including safety of continuing PD versus early PD catheter removal. Current literature describing this is unfortunately limited. This study aims to describe the characteristics, management and outcomes of liver abscesses in PD patients from a retrospective review of prevalent PD patients on follow-up at Tan Tock Seng Hospital between 1st January 2016 and 30th June 2021. A total of 11/383 PD patients (2.9%) were treated for liver abscesses. Most were diabetic (
Catheter-related tunnel infection may lead to peritonitis and discontinuation of performing high-quality peritoneal dialysis (PD). Tunnel infection is commonly caused by
