
Editorial
Select search scope: search across all journals or within the current journal
Care teams and patients want to know what happens next, and researchers have put together a lot of tools, such as predictive models, to help them predict the future. While these researchers are well-intentioned, the tools they develop are not always helpful. Most researchers know enough to perform various tests of their predictive models, such as statistical tests that answer the question: “Are the predictions based on this model better than a coin flip?” We urge researchers to add another test to their existing lists: “Does this model tell care teams anything they don’t already know?”
Modality transitions are very common in patients undergoing peritoneal dialysis (PD); they can either occur before the initiation of PD, following its termination, or as a temporary interruption during PD treatment. Transfers to and from facility hemodialysis represent the majority of these transitions. In addition to their impact on the quality of life of patients and their caregivers, modality transitions are often linked with hospitalizations, mortality, and increased health expenditures. Yet, some of these transfers are unavoidable and should be considered as part of the “dialysis life plan” for patients receiving PD. In this review, we will present the epidemiology, risk factors, and clinical impacts of the most frequent transitions that PD patients experience. We will also discuss strategies to optimize the outcomes of patients undergoing modality transfers. Finally, we will review the evidence underlying the integrated home dialysis paradigm, in which patients transition from PD to home hemodialysis.
Peritoneal dialysis (PD) offers comparable survival for acute kidney injury (AKI) as other kidney replacement therapies, but concerns about rigid catheter complications like peritonitis persist. This study evaluated outcomes of acute PD using rigid catheters in critically ill children, including peritonitis rates and mechanical complications.
This retrospective study analyzed data from consecutive pediatric patients (aged <18 years) admitted to our tertiary-level pediatric intensive care unit, who underwent acute PD using either rigid or improvised catheters, with each PD session limited to 72 h followed by re-insertion after 24 h if indicated. Data on primary diagnosis, PD indication, and laboratory parameters were collected from patient records and dialysis registers. Outcome measures, such as peritonitis rates and mechanical complications, were assessed.
Over a 10-year span (January 2014–September 2023), 202 children, 57% males, with a median age of 11 (3.6, 30) months, underwent PD. PD was initiated for fluid overload in 65 (32%), persistent anuria in 51 (25.2%), and refractory hyperkalemia in 47 (23.3%). In 13 (6.4%) patients, PD was initiated for metabolic crisis in the absence of AKI. The median estimated glomerular filtration rate at PD initiation was 21.4 (13.2, 46.5) mL/1.73m2/min. A total of 250 PD sessions/catheter insertions were performed on 202 children, for a median duration of 72 (24, 72) hours. Fourteen (6.9%) children developed peritonitis. Among children who received PD for ≤ 72 h (
Acute PD with a rigid catheter limited to 72 h appears safe and feasible in resource-constrained settings where soft Tenckhoff PD catheters are not easily available, though peritonitis rates increase with increasing cumulative duration on PD.
This is a visual representation of the abstract.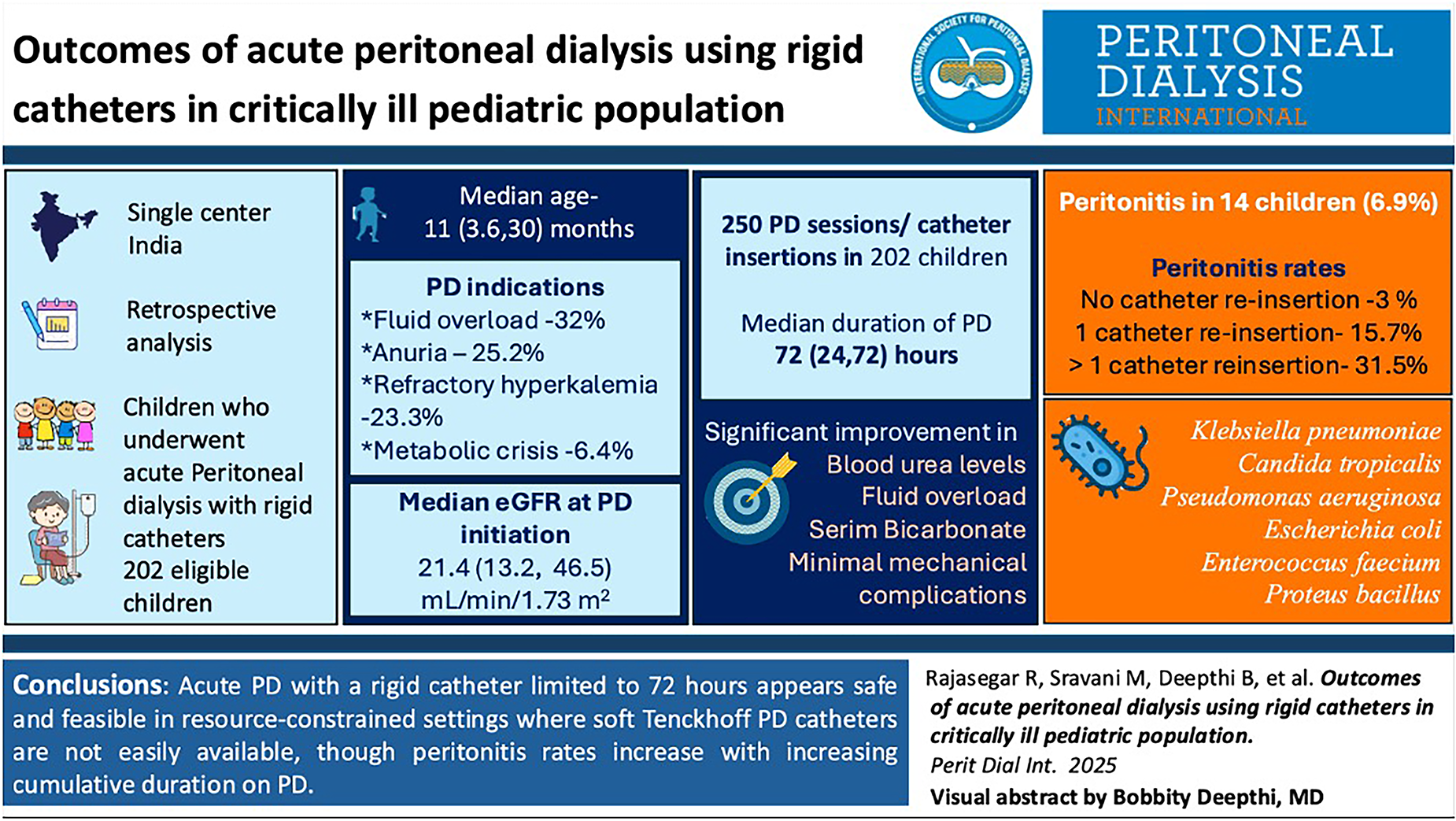
There are several indices to predict survival at dialysis start but tools to predict mortality for prevalent patients are lacking. This study provides evidence for external validity of the Cohen model to assess 6-, 12-, and 18-months survival of prevalent peritoneal dialysis (PD) patients.
Prospective cohort study of 464 PD patients in a university-based program between 2015 and 2019. Survival probabilities were compared to observed survival. Discrimination and calibration were assessed through predicted risk-stratified observed survival, cumulative area under the curve, Somer's Dxy, and a calibration slope estimate.
Discrimination performance was moderate with c-statistic of 0.73 to 0.74 for all 3 time points. The model over predicted mortality risk with the best predictive accuracy for 6-month survival. The difference between observed and mean predicted survival at 6, 12, and 18 months was 3.1%, 5.5%, and 11.0%. Kaplan-Meier curves showed good discrimination between low- and high-risk patients with hazard ratios [95% confidence interval (CI)]: C4 vs C1 32.0 [4.3–236.5]. Miscalibration of the model was the greatest for the highest risk patient group in whom 12 and 18 months predicted survival was 15% and 28% lower than observed survival.
The Cohen prognostic model can identify PD patients at high risk for death over 6, 12, and 18 months. Given it overestimates mortality risk for the highest risk patients, care must be taken to not use predictions to withhold treatment but rather to risk stratify and identify those who may benefit from enhanced kidney supportive care. This miscalibration provides an imperative to refine the tool for PD patients.
Peritoneal dialysis (PD) is being promoted because it is cost-effective and has equivalent outcomes to facility-based hemodialysis (HD). Determining PD eligibility is critical but subjective, with high variability among renal programs. This study aimed to establish a predictive model for PD eligibility among individuals who started treatment with HD. A secondary objective was to identify predictors of PD eligibility and determine if eligible patients went on to receive PD.
This retrospective cohort study included individuals starting HD at multiple hospitals in Alberta, Canada, as part of the START program between 1 October 2016 and 31 March 2018. Twenty-seven predictors, including patient characteristics, laboratory values, and comorbidities, were considered in logistic regression modeling. The outcome variable was PD eligibility, as determined by a standardized interdisciplinary assessment. The model selection was based on the Akaike information criterion. The confusion matrix was used for each model to compare the predicted versus observed eligibility. The final model was calibrated and presented.
Among the 598 participants, 391 (65.4%) were considered eligible for PD. The logistic regression model achieved a modest performance in discriminating patients who were eligible for PD, with a high sensitivity of 91.3%, an accuracy of 0.68 (95% CI, 0.65–0.72), and an area under the receiver operating characteristic curve ranging from 0.69 to 0.71. Age (OR = 0.98; 95% CI, 0.97–0.99), body mass index (OR = 0.95; 95% CI, 0.93–0.97), starting dialysis in intensive care unit (OR = 0.53; 95% CI, 0.31–0.92), and polycystic kidney disease (OR = 0.37; 95% CI, 0.13–0.99) were statistically significant factors associated with a lower likelihood of being considered eligible for PD. Out of the 391 eligible PD patients, 87 (22.3%) received PD treatment within 6 months of starting HD.
The majority of patients starting HD were considered eligible for PD. Our model exhibits a high level of sensitivity and could serve as a valuable tool for screening potential candidates following the commencement of HD.
Assisted peritoneal dialysis (PD), where trained health care providers assist individuals with PD in their home, allows individuals, who would otherwise be ineligible, to pursue home dialysis. Alberta Kidney Care South started an assisted PD program in 2011 using licensed practical nurses (LPNs) and switched to health care aids (HCA) July 2018.
A retrospective chart review to describe characteristics of assisted PD patients and their outcomes for each of the models of health care. The primary outcome was the duration of assisted PD from initiation to exit. Secondary outcomes included reasons for exit and the proportion of patients who performed independent PD.
A total of 135 patients received assisted PD, mean age 70.7 ± 11.2 years and 44.4% (60/135) women. The average time to exit from assisted PD was 366.2 ± 378.1 days. There was no difference between time in PD between LPN (1.89 [1.02, 3.85] years) and HCA (2.09 [0.89, 3.26] years),
Assisted PD allows patients to maintain independence in the community and facilitates the uptake of independent PD in a significant proportion. Utilizing an HCA model offers a cost-effective alternative while still providing high-quality care.
Few studies have evaluated the predictive capability of equations for residual kidney function (RKF) in patients undergoing peritoneal dialysis (PD). Moreover, the applicability of each equation remains unclear. Therefore, we aimed to evaluate the performances of the estimated RKF (eRKF) equations of Shafi, Steubl, and Jaques in Chinese patients undergoing continuous ambulatory peritoneal dialysis (CAPD).
This was a retrospective study. We enrolled patients who underwent CAPD and RKF measurements (via 24-h urine collection) in our hospital between November 2021 and May 2022. Using the measured RKF (mRKF) as the reference, we derived the bias, precision and accuracy of each equation.
We enrolled 174 participants. The mean β2-microglobulin and median mRKF were 29.00 ± 8.69 mg/L and 2.94 (1.26, 4.65) mL/min/1.73 m2, respectively. The Steubl equation had the least bias (MD [95% confidence interval, CI]: −0.52 [−0.77 to −0.38]), higher precision (interquartile range: 1.43 [1.16, 1.76]), and highest accuracy (83%). It also had a high diagnostic accuracy for identifying patients with an mRKF of > 2.5 mL/min/1.73 m2, area under the curve of 0.936 95% CI [0.903–0.970],
Although no equation was fully accurate, the Steubl equation identified patients suitable for an incremental PD prescription more accurately than the Shafi and Jaques versions. It may be useful for monitoring the RKF of Chinese patients undergoing CAPD who are unable to reliably collect urine.
Local and systemic side effects of glucose remain major limitations of peritoneal dialysis (PD). Glucose transport during PD is thought to occur via inter-endothelial pathways, but recent results show that phloretin, a general blocker of facilitative glucose channels (glucose transporters [GLUTs]), markedly reduced glucose diffusion capacity indicating that some glucose may be transferred via facilitative glucose channels (GLUTs). Whether such transport mainly occurs into (absorption), or across (trans-cellular) peritoneal cells is as yet unresolved.
Here we sought to elucidate whether diffusion of radiolabeled 18F-deoxyglucose ([18F]-DG) in the opposite direction (plasma → dialysate) is also affected by GLUT inhibition. During GLUT inhibition, such transport may either be increased or unaltered (favors absorption hypothesis) or decreased (favors transcellular hypothesis). Effects on the transport of solutes other than [18F]-DG (or glucose) during GLUT inhibition indicate effects on paracellular transport (between cells) rather than via GLUTs.
GLUT inhibition using phloretin markedly reduced [18F]-DG diffusion capacity, improved ultrafiltration (UF) rates and enhanced the sodium dip. No other solutes were significantly affected with the exception of urea and bicarbonate.
The present results indicate that part of glucose is transported via the transcellular route across cells in the peritoneal membrane. Regardless of the channel(s) involved, inhibitors of facilitative GLUTs may be promising agents to improve UF efficacy in patients treated with PD.
Peritoneal dialysis (PD)-related pleuroperitoneal communication is strongly associated with PD discontinuation. Video-assisted thoracoscopic surgery (VATS) has emerged as a promising therapeutic approach. However, there are still challenges in detecting diaphragmatic defects under conventional thoracoscopy, and the repair methods vary significantly.
We have developed an intervention protocol for pleuroperitoneal communication that includes single-port VATS utilizing near-infrared fluorescence with indocyanine green, as well as the management of perioperative kidney care and PD reinitiation. Patients who underwent VATS for pleuroperitoneal communication repair from September 2022 to March 2024 were identified at a single center. The procedures and outcomes were evaluated, and the success rate of PD resumption was compared with that of a historical cohort treated with non-surgical therapies.
A total of 6 patients underwent VATS. The age was 48.7 ± 11.8 years, 2 were female, and the PD vintage was 8.7 (2.0–28.4) months. Non-dialysis therapy (
The minimally invasive VATS integrating fluorescence with indocyanine green and pleurodesis with multiple mechanical reinforcements, along with appropriate perioperative care and an incremental approach to resume PD, was a reliable treatment for PD-related pleuroperitoneal communication.
Iron deficiency and anaemia are prevalent in people undergoing peritoneal dialysis (PD), necessitating effective iron supplementation. While oral iron is often preferred for its accessibility and cost, it may be insufficient or poorly tolerated. Intravenous (IV) iron is generally well tolerated and associated with improved haemoglobin response and reduced erythropoiesis-stimulating agent requirements, yet optimal dosing, administration intervals, and haematological targets remain under-researched, particularly in PD populations. Current prescribing practices vary significantly, reflecting gaps in evidence and consensus. This study aimed to evaluate UK clinical practices for iron therapy in PD and estimate patient eligibility for a future randomised controlled trial (RCT).
A cross-sectional survey was conducted among UK-based kidney clinicians using a structured 9-item questionnaire distributed electronically via the UK Kidney Association. The survey explored iron repletion strategies, diagnostic thresholds, and circumstances for withholding therapy. Responses were analysed using descriptive statistics for quantitative data and thematic analysis for free-text responses.
A total of 41 clinicians from 23 dialysis units participated, including consultants (73.2%), registrars (17.1%), and specialist nurses (9.7%). High-dose IV iron (≥500 mg per visit) was the preferred strategy for 65.9% of respondents, while none used oral iron alone. Most clinicians initiated iron therapy when serum ferritin was <200 µg/L (53.7%) or transferrin saturation (TSAT) was <20% (78.1%). Diagnostic measures beyond serum ferritin and TSAT, such as reticulocyte haemoglobin content, were rarely used (14.6%). The majority avoided iron therapy in the presence of active infection (90.2%) or IV iron allergy (92.7%). Estimates of trial eligibility indicated that 6–10% of people receiving PD might not meet inclusion criteria, largely due to elevated C-reactive protein, ferritin, or TSAT levels.
This survey highlights significant variability in iron therapy practices for people receiving PD in the UK. Most clinicians favour high-dose IV iron, reflecting its practical advantages in outpatient settings. However, diagnostic and safety concerns remain, with limited use of advanced biomarkers and inconsistent thresholds for therapy initiation. These findings underscore the need for a robust RCT to address gaps in evidence, establish optimal iron repletion strategies, and ensure safe and effective anaemia management in PD populations.
The impact of incremental peritoneal dialysis (PD) on outcomes is poorly understood, and there is a paucity of evidence informing best practices regarding the dialysis dose at the commencement of PD. This international prospective cohort study aimed to compare PD prescription practices at dialysis commencement and their subsequent association with clinical outcomes.
Adult patients who started PD for less than three months at the time of enrolment in the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS) between 1 January 2014 and 31 December 2017 were included. Patients were defined as initiating incremental PD if prescribed a total of <4 exchanges/day for continuous ambulatory peritoneal dialysis (CAPD) or, with dry days or having PD less than seven days per week for automated peritoneal dialysis (APD). All other prescriptions were considered standard PD. The primary outcome was the transfer to haemodialysis (HD). Secondary outcomes included peritonitis rate, time to first peritonitis and mortality. Logistic regression analysed PD uptake and the Cox proportional hazards regression model analysed HD transfer, peritonitis and patient survival.
Overall, 1365 PD patients from 128 facilities across seven countries were included. Fewer individuals started on incremental PD than standard PD (37% vs 63%,
Incremental PD start was prescribed in approximately one-third of patients and, in low certainty evidence, was associated with comparable risks of HD transfer, peritonitis and death.
Peritoneal dialysis (PD) catheter placement is considered a controversial procedure in patients with a history of abdominal surgeries or peritonitis. In these subjects, video laparoscopic (VLS)-assisted placement under general anesthesia (GA) is the gold standard procedure. However, older multimorbid patients are at high risk for complications in GA. In our opinion, thoracic spinal anesthesia (TSA) instead of GA could also be used in older multimorbid patients undergoing PD. Here, we report five cases of older multimorbid end-stage kidney disease (ESKD) patients aged 79.6 ± 3.5 years with a history of abdominal surgery or peritonitis needing renal replacement therapy. Overall comorbidity was high (Cumulative Illness Rating Scale (CIRS) comorbidity index 4.0 ± 1.2 and CIRS severity index 2.1 ± 0.5). We placed the PD catheter in these patients using the VLS-assisted placement under TSA. All subjects underwent TSA performed at the T9-T10 thoracic level, obtaining optimal pain control and no periprocedural side effects. This is the first attempt to utilize the TSA in PD catheter VLS placement in very old multimorbid patients. Further studies could be useful to confirm whether TSA can be successfully used in VLS-assisted PD catheter placement, especially in subjects ineligible for GA such as older frailty patients.
Pleuroperitoneal communication affects 1.6%–10% of continuous ambulatory peritoneal dialysis (PD) patients and often leads to discontinuation of peritoneal dialysis. In pleuroperitoneal communication, an important aspect is not only the diagnosis but also the detection of the diaphragmatic defect. Traditional methods have often failed to detect small defects, which contributes to the recurrence of pleuroperitoneal communication. We present three cases of intractable diaphragmatic defects in pleuroperitoneal communication, successfully localized and treated using indocyanine green (ICG) fluorescence staining of peritoneal dialysate, visualized with an infrared camera. After detecting the defect, surgical repair involved defect plication and the application of talc for pleural adhesion. This approach enabled immediate and successful on-site repair, allowing all patients to resume peritoneal dialysis post-surgery. Even the smallest diaphragmatic defects were accurately identified using ICG fluorescence dye dissolved in peritoneal dialysate. This case series demonstrates that ICG fluorescence staining enhances the diagnosis and treatment of pleuroperitoneal communication by improving defect localization. Our protocol shows promise in increasing diagnostic accuracy, reducing recurrence rates, and helping patients maintain their preferred dialysis modality.
Anorexia nervosa (AN) is an eating disorder characterized by restriction of energy intake leading to a significantly low body weight, and intense fear of gaining weight. Severe electrolyte changes such as hypokalemia and hypophosphatemia; and alterations in water metabolism such as hyponatremia and edema, can occur in patients with AN. Hypokalemia and chronic volume depletion may lead to acute kidney injury (AKI) and chronic kidney disease (CKD). There are few reports of patients with AN who require maintenance dialysis. Therefore, it is unclear whether hemodialysis (HD) or peritoneal dialysis (PD) is suitable for such patients. We report a case of kidney failure that developed in the patient with AN who received successful psychiatric treatment aimed at weight gain while performing PD. The safety of PD may be improved in patients who also undergo cognitive behavioral psychotherapeutic intervention.

Peritoneal dialysis (PD)-associated peritonitis commonly arises from touch contamination events, however, it is important to be mindful of alternative etiologies and to take a detailed history and perform a root cause analysis for each episode. In fact, the PD effluent can be a window into intra-abdominal pathologies which may require surgical management. We present an unusual case of secondary enteric peritonitis due to foreign body bowel perforation from ingestion of a fish bone.
Peritoneal dialysis-associated peritonitis (peritoneal dialysis (PD) peritonitis) is a common complication of peritoneal dialysis associated with adverse events and mortality. Outcomes are poorer when two or more organisms are isolated in the dialysis effluent culture, known as polymicrobial PD peritonitis, which can be caused by an underlying secondary process, such as gastrointestinal tract pathology and, rarely, a foreign body. Here, we report a case of polymicrobial PD peritonitis due to a vegetable matter foreign body perforating the colon. The patient was conservatively managed with antibiotic treatment and subsequent colonoscopic removal of the foreign body without the need for peritoneal dialysis catheter removal. She continues to remain on peritoneal dialysis 18 months after the PD peritonitis episode.