Jo Cresswell, Marc Laniado, Andrew Sinclair , [...]
View All
Abstract
It has become customary that a session is held at the British Association of Urological Surgeons (BAUS) annual meeting, wherein the most important advances in the major urological sub-specialities are summarised by British opinion leaders for the benefit of the core of urologists. It gives us pleasure to present in this paper the topics covered at the BAUS meeting in June 2015, in Manchester, UK.
Research article
Restricted accessResearch articleFirst published July, 2016pp. 230-233
Adam W Nelson, Alastair D Lamb, Vincent J Gnanapragasam
Abstract
Objective: The process of writing a grant application can be challenging. In this article we summarise key aspects of the process including when to begin, whom to submit to and how to construct a research hypothesis. It is intended that this article will be a useful resource for individuals seeking to embark on research as part of a higher degree.
Research article
Restricted accessResearch articleFirst published July, 2016pp. 234-238
Recurrent urinary tract infections (UTIs) in women are common despite anatomically normal urinary tracts and are frequently referred to secondary care for further assessment.
Patients and methods:
Clinic letters and pathology reports of 244 women referred to our centre over a 2-year period with uncomplicated recurrent UTIs were reviewed to determine the investigations they underwent in both primary and secondary care.
Results:
A significant proportion of women do not meet the criteria for recurrent UTIs as their infections are not proven on culture. The majority of women undergo both renal tract ultrasound scan (USS) and flexible cystoscopy. Though USS was found to demonstrate relevant pathology, flexible cystoscopy, however, did not reveal any relevant pathology.
Conclusion:
Investigation of women with recurrent uncomplicated UTIs should be done with adequate cultures and renal tract USS.
Research article
Restricted accessResearch articleFirst published July, 2016pp. 239-243
Jack Donati-Bourne, Muhammad Idzwan Husaini, Praveen Pillai , [...]
View All
Abstract
Objective:
The objective of this article is to review the outcomes of our updated single-centre extended experience of an innovative enhanced recovery pathway to perform catheter- and drain-free laparoscopic pyeloplasties, achieving safe discharge within 23 hours of surgery.
Patients and methods:
We conducted a retrospective review of patients who underwent a standard trans-peritoneal laparoscopic pyeloplasty repair over an antegrade stent in our centre by a single surgeon, between 1 September 2007 and 1 February 2015.
Patients who had a urinary catheter and/or peri-nephric drain inserted intraoperatively and were not planned for day-case discharge were excluded.
Data were collected for duration of in-patient stay, readmission rates and reasons for these. Successful outcome was deemed both in subjective improvement of patient symptoms and/or objective improvement in post-operative MAG-3 renogram curve.
Results:
Fifty-eight patients were included. A total of 74% (n = 43) were successfully discharged as day-case, and four of these were readmitted. Fifteen patients required in-patient stay, of whom two were readmitted. Successful outcome was recorded in 93% (n = 54).
Conclusion:
The insertion of a drain and catheter are not essential in laparoscopic pyeloplasty. Avoidance of unnecessary tubes facilitates day-case surgery with no adverse effect on outcome.
At our institute all patients are now offered the enhanced recovery protocol for laparoscopic pyeloplasty with resulting benefits both to patients and the local health economy.
Research article
Restricted accessResearch articleFirst published July, 2016pp. 244-247
On-demand irrigation warmers are widely used to provide a convenient way of irrigating warmed fluids for endoscopic procedure. However, concern has been raised that flow rates via these devices are inadequate for safe operating. Holmium enucleation of prostate (HoLEP) requires significant volume and flow rate of irrigation. Poiseuille’s Law states the resistance of a tube will result in reduced flow and a reduction in pressure across the tube. The aim was to compare the irrigation rates provided by one such warming device compared to a standard giving set whilst simulating HoLEP and to monitor intravesical pressure.
Methods:
A simulated apparatus was set up to replicate HoLEP surgery. Simulated design rather than ‘real-life’ apparatus was used to allow for repeated testing in a more controlled environment and to avoid other variables due to operative differences. Comparison of irrigation rate and pressure difference was measured whilst using a standard irrigation set (Fresenius Kabi) with pre-warmed fluid and the Ranger irrigation warming system (3M). Pressure was measured using a pressure line passed via the working channel of the laser resectoscope.
Results:
The standard giving set demonstrated lower resistance and higher irrigation rates. The irrigation rate was 31% higher (7.2 vs 5.5 ml/s). A lower change in pressure across the standard giving set was found (20 vs 38 cm H2O). The resistance therefore is much higher in the Ranger irrigation system, which gave a much slower flow and greater drop in pressure.
Conclusion:
This unique demonstration has led to a quantitative assessment of commonly used giving sets and has shown irrigation rates via a standard giving set are 31% greater than through the Ranger irrigation warming system. On-demand fluid warmers are felt to result in poor intraoperative vision and pose a potential risk to patient safety during HoLEP and other urological procedures requiring high fluid volumes.
Research article
Restricted accessResearch articleFirst published July, 2016pp. 248-251
Hamid Abboudi, Michael Mikhail, Mohammed Ghazal-Aswad , [...]
View All
Abstract
Objective:
YouTubeTM has provided a platform that is utilised by millions. Patients are increasingly utilising this source of information. We set out to systematically analyse the quality of ureteroscopy videos.
Materials and methods:
YouTubeTM was searched using the term ‘ureteroscopy’. Content was assessed using the British Association of Urological Surgeons website criteria. Information relating to management options, procedural description, stent insertion, recovery and complications was rated. An overall rating was given. Videos were also analysed in terms of country of origin, view count, likes, dislikes, source and technical quality. The kappa statistic was used.
Results:
A total of 59 videos were analysed. The total number of viewings was 557,896 (range: 42– 121,943), with an average number of 9456 viewings per video. The information content was either poor or average in 98% (n = 58) of videos, with only 2% (n=1) rated as good and 0% achieving an excellent rating. Technical quality was rated as poor in 28 videos, average in 22 and good in nine videos. Most videos were broadcast by surgeons or surgical institutes (48/59).
Conclusion:
The quality of videos is variable. Patients should not be encouraged to use this for education. Opportunity has arisen for the endourology community to produce high quality video broadcasts to optimise patient understanding.
Research article
Restricted accessResearch articleFirst published July, 2016pp. 252-255
The objective of this study was to review the effectiveness and safety of a one stop urology clinic led by a consultant diagnostic urologist.
Methods:
Data were collected prospectively on all patients seen by a single consultant diagnostic urologist from February 2007 to February 2008. In 2013, patient records were reviewed and cross-referenced to identify if any patients had been re-referred to the urology service and why.
Results:
From 889 referrals, 799 patients attended, of these 689 (86%) were discharged after a single visit with 110 (14%) booked follow-up appointments. Ninety patients were re-referred, only two of these had a significant diagnosis. Thirty-four (38%) had a new referral reason.
Conclusion:
The one stop method of consultation is effective and efficient across a range of presenting complaints in urology. It is safe for patients and leads to a high discharge rate with a low re-referral rate without missing clinically significant diagnoses.
Research article
Restricted accessResearch articleFirst published July, 2016pp. 256-261
The efficacy of intravesical botulinum toxin-A (BTX-A) for the treatment of idiopathic detrusor overactivity (IDO) is well-established and evidence-based. The optimal regime in terms of dose, distribution, depth of injection and number of injections has not been determined and there is still considerable variation throughout clinical practice. We aim to establish the optimum template for bladder injections.
Patients and methods:
All patients had urodynamically-proven IDO which had failed conservative and medical management. AbobotulinumtoxinA (250 units) was injected into the detrusor and sub-urothelium in one of five injection templates under general anaesthetic. An Overactive Bladder Symptom Score (OABSS) and International Prostate Symptoms Score (IPSS)-Likert quality of life (QoL) score was completed pre-operatively and at six weeks post-operatively. In those who underwent repeat treatments the time to re-commencement of pharmacological therapy was recorded.
Results:
In total 111 patients received 170 treatments. The average age of patients was 57 (range: 17–86) and the male: female ratio was 0.18:1. Overall there was a mean improvement in the OABSS by −3.7 points±4.29 (standard deviation (SD) (p<0.01) and an average change in the QoL score of −2.18±2.17 (SD) (p<0.01) with BTX-A treatment. When analysed by template subgroup there was no statistically significant difference in the magnitude of change for any template over the other four for either the OABSS (p=0.78) or QoL scores (p=0.56). Forty-one patients had multiple treatments and had data collected for the duration to treatment failure. The overall average time to treatment failure was 11.2±7.9 months. Subgroup analysis showed that there was no statistically significant (p=0.783) difference in time to treatment failure for any one of the injection distributions.
Conclusion:
This study has shown that altering the injection protocol of BTX-A did not affect the clinical outcome in terms of symptoms, QoL or in the time to treatment failure.
Research article
Restricted accessResearch articleFirst published July, 2016pp. 262-267
Ionising radiation is commonly used in urological practice in the form of fluoroscopy. To date there is a remarkable scarcity of information concerning patient exposure to ionising radiation during urological procedures and the potential risk of developing of a lethal malignancy due to excessive radiation exposure.
Objectives:
We aimed to determine the radiation exposure for a patient during the most commonly performed urological procedures, and to assess the potential risk of developing a fatal cancer as a result of endourological fluoroscopy.
Methods:
Data was collected prospectively in two institutions on endoscopic urological operations. Procedures were classified as retrographic, semi-rigid ureteroscopic and flexible ureterorenoscopic (FURS). Data collected included procedure type and difficulty, Dose Area Product [DAP (Gy*Cm2)]. The effective dose (ED) measured in millisievert (mSv) was determined from the DAP by using the Monte Carlo calculation.
Results:
In total 395 consecutive operations from two institutions were assessed. The mean ED for all procedures in this study was 0.394 mSv, IQR (0.1184–0.7583). The maximum ED was 5.93 mSv. The radiation exposure for all procedures was relatively small; for diagnostic retrographic procedures the median ED was 0.112 mSv. For retrograde procedures that involved stent insertion, the median ED was 0.438 mSv. The median ED for all ureteroscopic surgeries was 0.295 mSv, and the median ED for all FURS procedures was 0.491.
Conclusion:
The findings of this study are reassuring. Endoscopic urological procedures appear to expose patients to relatively small radiation compared with other procedures requiring fluoroscopy, thus conferring a very low lifetime risk of malignancy.
Research article
Restricted accessResearch articleFirst published July, 2016pp. 268-273
We present our experience using oral bicarbonate as a dissolution therapy for radiolucent kidney stones in the pre-dual energy CT era.
Methods:
A retrospective analysis of dissolution therapy was undertaken over a four-year period. Stones were diagnosed as radiolucent on conventional KUB X-ray in combination with either ultrasound or CT KUB. Oral bicarbonate was given at a dose of 2 g tds orally, increased to 2 g five times daily according to urinary pH. Patients monitored their own urine dipstick daily to achieve a pH of at least seven.
Results:
Altogether 27 patients were identified with radiolucent stones. Stone size varied from 4–40 mm. Average length of therapy was nine weeks. Of the patients, 17 had renal U/S and six had CT KUB as end point imaging. We found that 39% had complete dissolution, 18% had a partial response and 43% showed no response. A high serum uric acid level correlated with a higher incidence of dissolution. Cost-benefit analysis shows bicarbonate therapy to be more cost-effective than lithotripsy, ureteroscopy or nephrolithotomy.
Conclusions:
Bicarbonate therapy remains an attractive option for the treatment of radiolucent kidney stones. The presence of hyperuricaemia or hyperuricosuria appears to influence the success rate. Further prospective randomised studies are needed to identify the most tolerable and effective treatment regime as well as the optimal duration of treatment. Dual-energy CT may hold the key to identifying patients most likely to benefit from treatment.
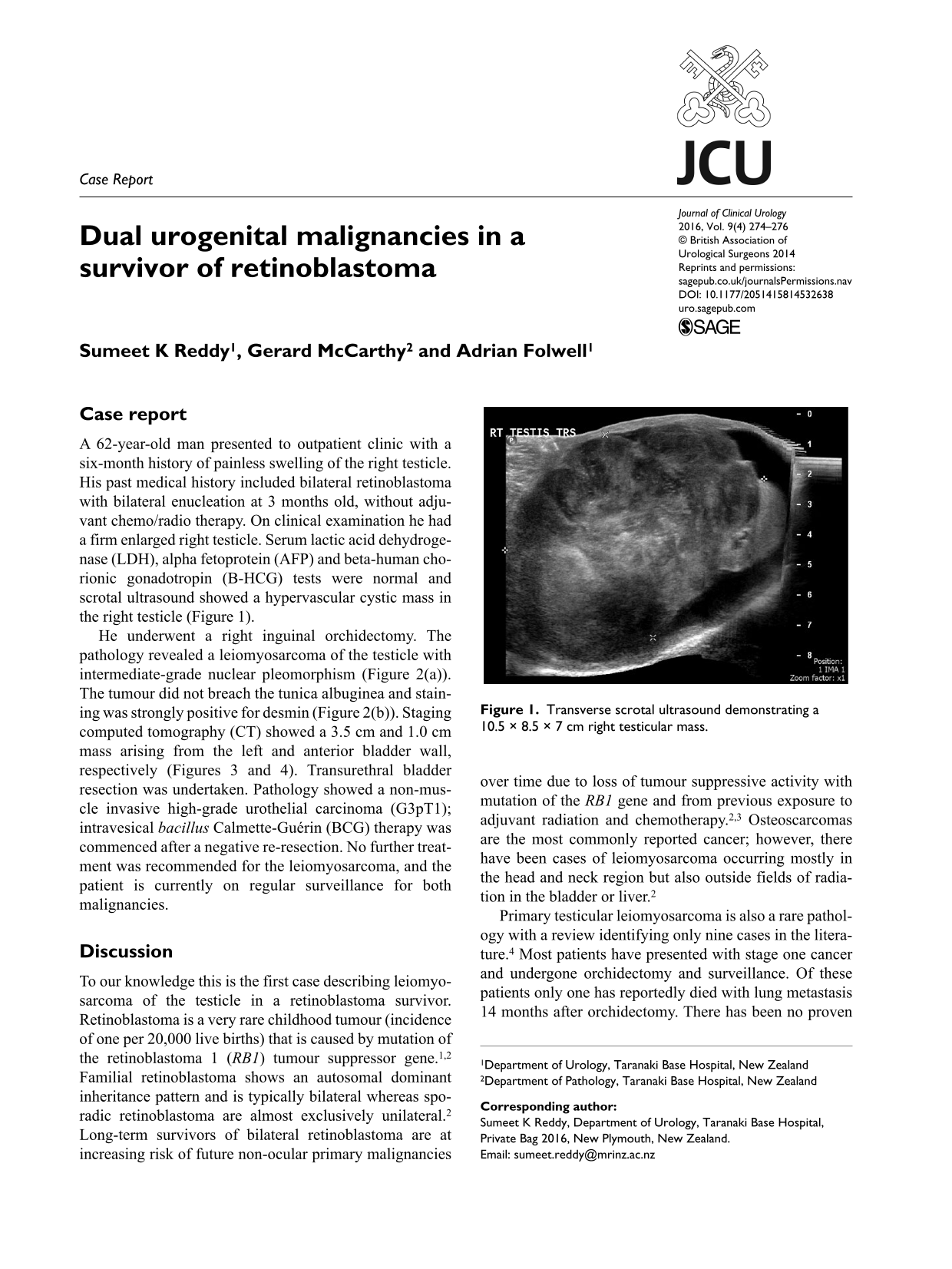
Case report
Restricted accessCase reportFirst published July, 2016pp. 274-276