
Editorial
Select search scope: search across all journals or within the current journal
The incidence of ischemic stroke among young adults (aged 18–49 years) has risen over recent decades, particularly in high-income countries, contrasting with the decline seen in older populations. This trend represents a growing public health concern, as stroke at young age often leads to long-term psychosocial consequences and loss of productive life years. The increasing incidence may partly reflect a higher prevalence of traditional vascular risk factors, as well as the identification of non-traditional risk and trigger factors such as air pollution, sleep apnea, long working hours, vigorous exercise, and illicit drug use. Diagnostic evaluation in this young population is typically more extensive than in older patients, given the broad spectrum of potential underlying causes. A structured, multidisciplinary approach integrating vascular, hematologic, and cardiac assessment is essential for accurate etiological classification. Although functional outcomes are generally favorable, many young stroke survivors experience persistent psychosocial sequelae, including cognitive impairment, depression, anxiety, and fatigue, which significantly affect quality of life. Recurrence risk varies according to stroke etiology, with the lowest rates observed in patients with a cryptogenic stroke. These findings highlight the importance of more tailored secondary prevention strategies, as antiplatelet therapy is not without risks. Further research is needed to identify novel risk and trigger factors, refine prognostic tools, optimize secondary prevention, and develop interventions addressing the psychosocial recovery of young stroke survivors.
Although reductions in stroke incidence have been reported over recent decades particularly in high-income countries, there has been a worrying trend since the start of the 21st century: stroke incidence in younger individuals (<55 years) has not showed a similar decrease as at older ages. In high-income countries, several population-based studies have found an increase in the incidence of stroke at younger ages since 2000, reaching up to 90% in Oxfordshire, UK (2010–2018 vs 1981–1986) and 97% in Cincinnati, USA (2010 vs 1993–1994). A similar picture has also been documented in low- and middle-income countries, both in population-based studies (Joinville, Brazil, 35% increase in 2012–2013 vs 2005–2006) and in the Global Burden of Disease study. The exact reasons for this very different picture seen in younger individuals are unknown. One possibility is that traditional modifiable risk factors are increasingly prevalent and often undertreated at younger ages. However, studies have also found increases in the incidence of young-onset cryptogenic stroke and in people with no traditional modifiable risk factors, suggesting a role for emerging risk factors. Potential culprits might include air pollution, long working hours, psychosocial stress, prior autoimmune diseases, and illicit drug use, although further research is required to determine whether these emerging risk factors are causally related to stroke at younger ages. Without further intervention, the global burden of stroke at younger ages is projected to increase further in the coming years. Therefore, there is an urgent need to better understand the drivers of these time trends in incidence, to potentially alleviate the individual and societal impacts of stroke in the young. In this narrative review, we examine the recent global changes in stroke epidemiology at younger ages, their potential drivers, and their projected consequences.
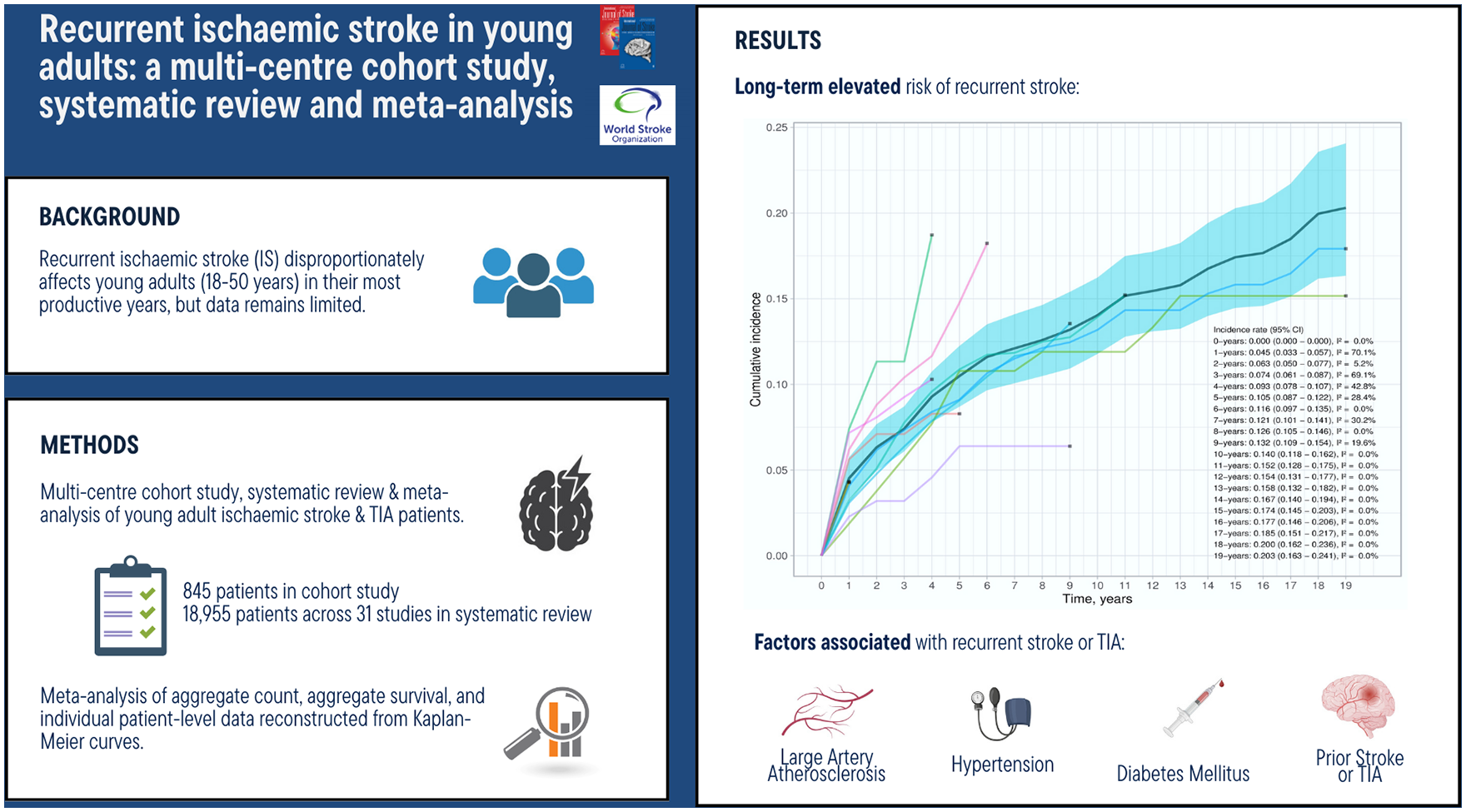
Recurrent ischemic stroke (IS) disproportionately affects individuals in their most productive years, contributing to significant morbidity and mortality. Despite its growing importance, data on this critical population remain limited.
The aim of the study is to characterize rates and factors associated with recurrent IS in young adults.
We performed a retrospective multicentre cohort study of consecutive acute IS patients aged 18–50 years from three tertiary hospitals in Singapore and Christchurch, New Zealand. We characterized rates and prognostic factors associated with recurrent IS over 1-year follow-up using univariate and multivariable Cox Proportional Hazards models. We then performed a systematic review and meta-analysis of PubMed, Embase, Scopus and Cochrane databases for all studies from January 2000 to July 2024 evaluating recurrent stroke or transient ischemic attack (TIA) following an index IS or TIA. We meta-analyzed rates and factors associated with recurrent cerebrovascular events based on aggregate count, aggregate survival, and individual patient-level survival data reconstructed from Kaplan–Meier curves.
The cohort study of 845 patients showed a 3.41% (95% confidence interval (CI) = 2.16–4.64) recurrence rate over 1-year follow-up. Patients with diabetes mellitus and prior stroke/TIA had significantly higher rates of recurrent IS. The systematic review and meta-analysis of 18,955 patients across 31 studies yielded a recurrence rate of 4.5–7.3% at 1 year, 10.5–12.8% at 5 years, and 14.0–20.3% at >10 years. Large artery atherosclerosis (LAA) etiology, hypertension, diabetes mellitus, and prior stroke/TIA were significantly associated with recurrent stroke or TIA.
Young adults with IS face a long-term risk of recurrent cerebrovascular events. More prospective studies are warranted to better characterize long-term prognosis for these patients.
The long-term non-motor outcome of young adults with ischemic stroke (IS) or transient ischemic attack (TIA) is poorly understood.
Therefore, in this observational cohort study, we explored the prevalence of impairment and factors influencing clinical and neuropsychological outcomes and return-to-work a decade post-stroke.
After a median follow-up duration of 10.4 years, 163 patients (median age at index event: 46.0 years, 44.8% female, 121 IS and 42 TIA) of the “Stroke in Young Fabry Patients study” attended an in-person follow-up in three European centers. We assessed clinical, neuropsychological, and return-to-work data.
A decade post-stroke, most patients (74.8%) showed excellent outcome, scoring 0–1 on the modified Rankin Scale (mRS) and 68.0% had returned to work. However, at follow-up, 27.2% of patients showed cognitive impairment and 27.6% suffered from fatigue. Anxiety and depression were reported by 38.0% and 18.5%, respectively. Even among patients with excellent functional outcome (mRS 0–1), 24.6% showed cognitive problems, 37.7% suffered from anxiety, 22.1% from fatigue, and 12.4% from depression. Female patients had higher rates of anxiety (52.1% vs. 26.7%), fatigue (37.0% vs. 20.0%), and depression (27.4% vs. 11.2%), compared to male patients.
In linear regression, female sex was associated with a higher likelihood for anxiety (odds ratio (OR = 2.89, 95% confidence interval (CI) = 0.62-5.16), fatigue (OR = 3.23, CI = 1.52-4.93), and depression (OR = 2.86, CI = 1.12-4.59). Hypertension at follow-up (52.1%) was associated with worse functional outcome (OR = 3.03, CI = 1.32-6.95), while patients smoking at follow-up (20.2%) had higher rates of anxiety (OR = 4.09, CI = 1.21-6.97) and depression (OR = 3.40, CI = 0.87-5.21).
Despite excellent functional outcome, many young stroke patients experience neuropsychological impairment, highlighting the need for targeted screening and treatment. Particularly young women are at higher risk for post-stroke depression, anxiety, and fatigue. Hypertension and smoking were modifiable risk factors contributing to worse outcomes in this young stroke cohort.
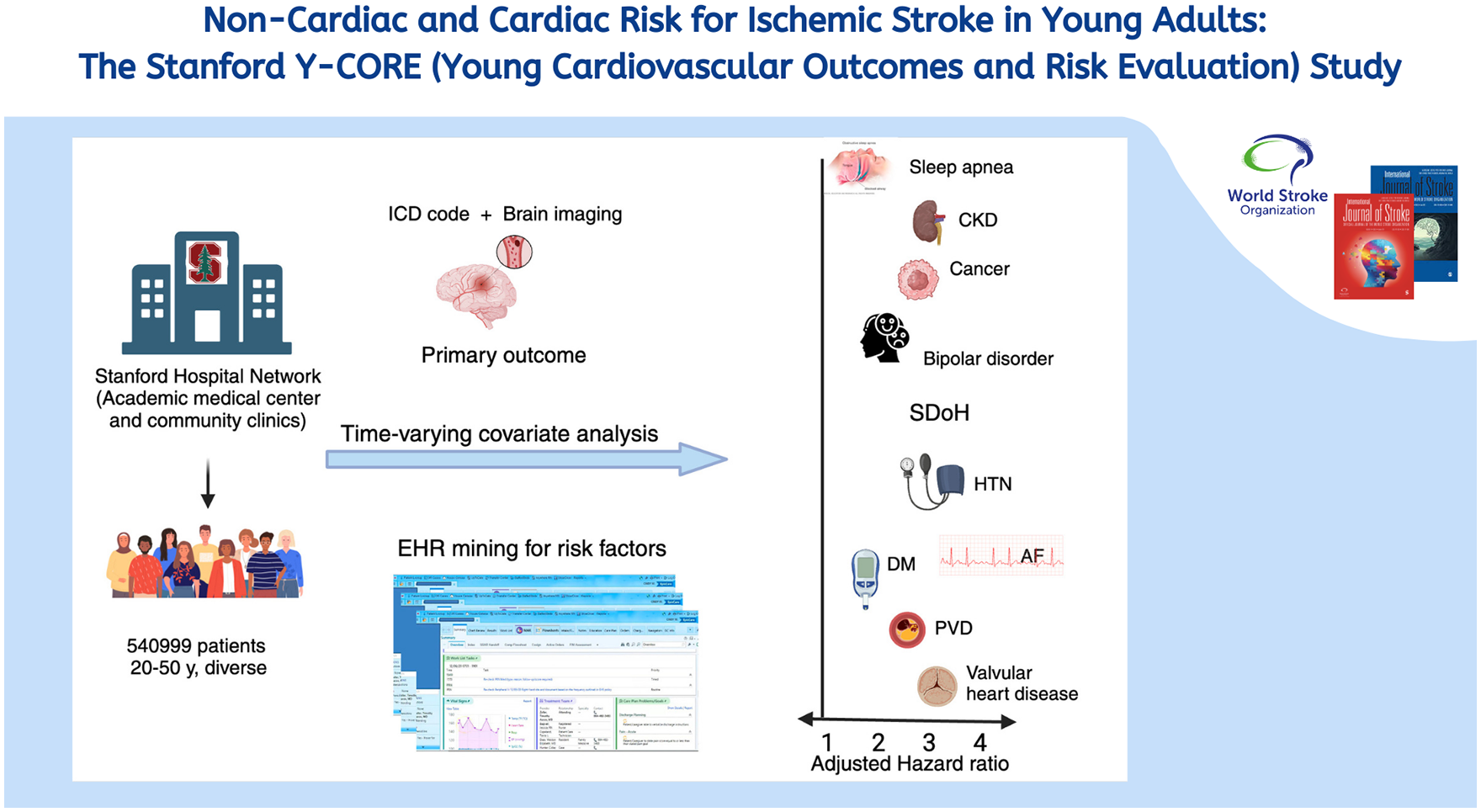
The incidence of stroke is increasing in young to middle-aged adults. Assessing risk factors is important in this large population whose comorbidities may differ from older adults.
In this retrospective cohort analysis of adults aged between 20 and 50 presenting to the Stanford Healthcare system from 1 January 2000 through 31 December 2021, with no prior history of stroke or transient ischemic attack, we studied the effects of 30 risk factors on the primary endpoint of incident ischemic stroke, defined by the presence of the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) codes for stroke and confirmed by brain imaging. The secondary endpoint was incident cerebrovascular events defined by the presence of ICD-10 codes for stroke or transient ischemic attacks (TIAs). Associations were measured with time-varying multivariable survival regression.
From an overall population of 1.3 million, we identified 540,999 individuals aged 20–50 years. Over the study period, 802 experienced the primary endpoint and 5734 the secondary endpoint. On multivariable analysis, non-cardiovascular risk factors were independently associated with the primary endpoint, adjusting for established cardiovascular risk factors, including sleep apnea [1.44, (1.19, 1.74)], bipolar disorder [1.88, (1.23, 2.86)], cancer [2.07 (1.71, 2.51)], and chronic kidney disease (CKD) [2.2, (1.73, 2.81)]. Other non-cardiovascular associations included ethno-racial subgroups of Black [2.05, (1.60, 2.64)], Pacific Islander [2.56, (1.70, 3.84)], and Hispanic [1.71, (1.37, 2.15)] versus white non-Hispanics. Combining non-cardiovascular risk factors significant on multivariable analysis with established cardiovascular factors significantly improved the C-index for de novo stroke to 0.814 over that obtained in either group alone (
In this large population of young adults, several non-cardiovascular factors conferred risk for incident stroke independent of known cardiovascular risk factors and, in combination, significantly improved the prediction of incident stroke over those based on either group of factors alone. These findings may have implications for assessing risk in younger patients with distinct comorbidities.
Stroke is associated with substantial mortality among children and adolescents, yet evidence on the death burden of stroke in this group in China is scarce.
To assess the trends of mortality and years of life lost (YLL) due to stroke in children and adolescents in China.
We estimated the number and age-standardized rate of death and YLL caused by stroke and its subtypes among children and adolescents aged 0–19 years in China and its provinces from 2005 to 2020, utilizing data from National Mortality Surveillance System.
In China, the age-standardized mortality rate due to stroke among children and adolescents aged 0–19 years decreased from 1.40/100,000 to 0.51/100,000 during 2005–2020, and the YLL rate decreased from 116.28/100,000 to 38.79/100,000. During 2005–2020, intracerebral hemorrhage (ICH) consistently showed significantly higher age-standardized mortality rate than ischemic stroke (IS) and subarachnoid hemorrhage (SAH). In 2020, the mortality rate of ICH was 11.35-fold and 4.96-fold greater than that of IS and SAH, respectively (ICH 0.40/100,000, IS 0.04/100,000, SAH 0.08/100,000). Overall, males among children and adolescents exhibited higher age-standardized mortality and YLL rate due to stroke compared to females. Notably, the stroke mortality rate in 15–19 years age group increased by 16.10% during 2005–2020, primarily attributed to the significant increases in mortality rate of ICH and SAH among males in this age group (ICH males 25.51%, SAH males 107.83%). In 2020, Yunnan (1.56/100,000), Tibet (1.54/100,000), and Henan (1.47/100,000) had the highest age-standardized mortality rate of stroke among children and adolescents, while Shanghai, Fujian and Jiangsu had the lowest rates. In addition, a negative association was observed between the age-standardized YLL rates of stroke among individuals aged 0–19 years and the socio-demographic index across 31 provinces in China from 2005 to 2020.
In China, the death burden of ICH among children and adolescents was considerably heavier than that of SAH and IS. The rising mortality rate of ICH and SAH among males aged 15–19 years requires greater emphasis. Targeted interventions for stroke in children and adolescents should be expedited to reduce the disease burden in this particular population.
Young adults account for up to 15% of all ischemic strokes, yet data from Latin America remain scarce. Understanding their clinical profile and outcomes is essential to inform targeted interventions and public health strategies. We aimed to characterize demographics, vascular risk factors, stroke etiology, access to acute reperfusion therapies, and 90-day outcomes in Argentine patients aged 18–50 years with ischemic stroke.
We conducted a retrospective multicenter cohort study including consecutive patients aged 18–50 years with ischemic stroke, enrolled between January 2015 and December 2023 across 26 centers in Argentina. Primary outcomes were functional dependence (modified Rankin scale (mRS) 3–5), stroke recurrence, and all-cause mortality at 90 days.
Among 18,934 ischemic stroke patients, 1422 (7.5%) were young adults. Median age was 43 years (interquartile range (IQR) 36–47), and 53.7% (n = 763) were male. The most prevalent risk factors were hypertension (31.0% (n = 441)), smoking (29.3% (n = 417)), and obesity (18.8% (n = 267)). Median National Institute of Health Stroke Scale (NIHSS) on admission was 3 (IQR 1–8). Acute reperfusion therapy was administered in 18.9% (n = 269). Stroke etiology remained undetermined in 50.4% (n = 717) of cases; within this group, 26.1% (n = 312) fulfilled criteria for embolic stroke of undetermined source (ESUS), and 17.8% (n = 198) were cryptogenic strokes associated with patent foramen ovale. Arterial dissection accounted for 56.6% (n = 193) of other determined causes. At 90 days, functional dependence was observed in 12.1% (n = 110), stroke recurrence in 3.9% (n = 37), and mortality in 4.8% (n = 44).
In Argentina, nearly 1 in 13 ischemic strokes occurs in young adults. Despite generally mild presentations, functional dependence and mortality remain substantial. The high rate of undetermined etiology underscores the need for standardized diagnostic protocols in this population, whose strokes carry a disproportionate individual and societal burden due to their early onset.

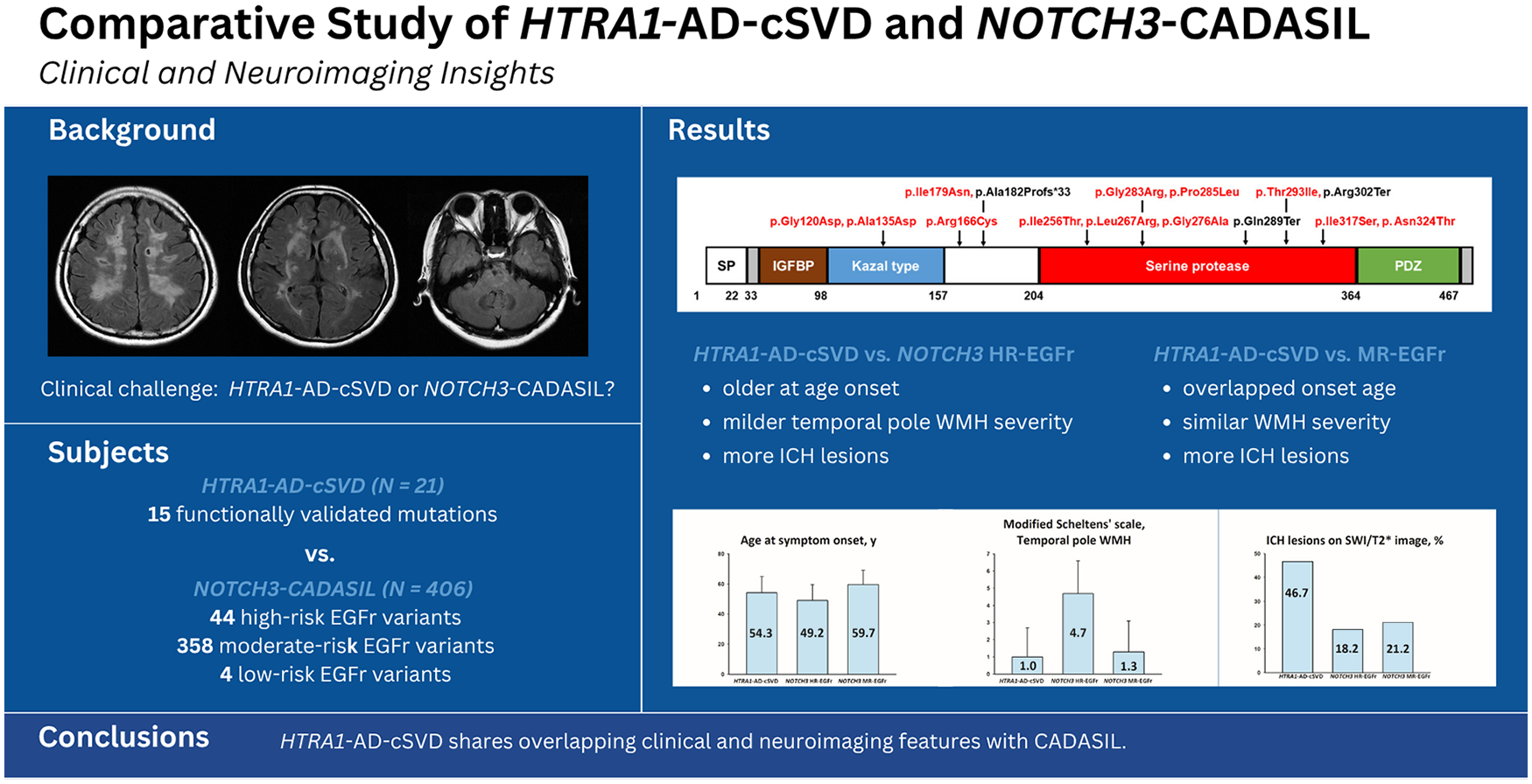
Heterozygous
This retrospective study aims to characterize and compare the clinical and neuroimaging features of
We identified 21 unrelated Taiwanese subjects carrying 15 heterozygous
Stroke occurred in 81.0% of
Data are available upon reasonable request from third parties.
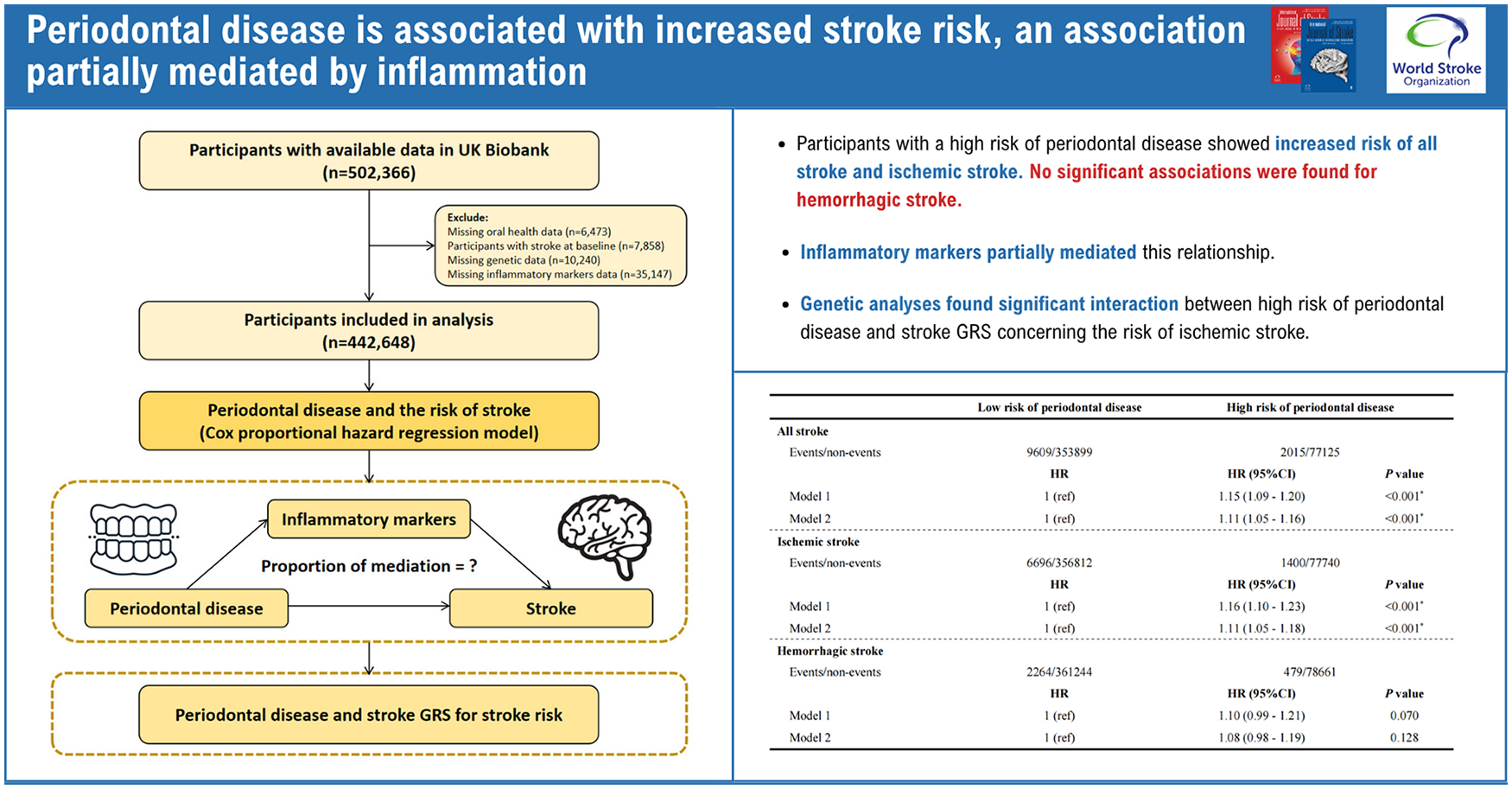
Despite evidence linking periodontal disease to stroke risk, research investigating the potential mediating role of inflammatory markers and the modifying influence of genetic susceptibility in this relationship remains limited.
The study aimed to assess the association between self-reported high risk of periodontal disease and stroke, while exploring the potential mediating effects of inflammatory markers and the modifying influence of genetic susceptibility.
Using UK Biobank data, we investigated the association between high risk of periodontal disease and incident stroke using Cox proportional hazards regression models. Participants were classified as having a high risk of periodontal disease if they reported experiencing any of painful gums, bleeding gums, and/or loose teeth. We explored the potential mediating role of inflammatory markers in the observed association through mediation analyses. For genetic analyses, we calculated a genetic risk score (GRS) for stroke using 32 single nucleotide polymorphisms, stratified participants into tertiles, and conducted interaction analyses between GRS and periodontal disease risk with respect to both all stroke and ischemic stroke.
The study included 442,648 participants, followed up for a median of 13.7 years. Participants with a high risk of periodontal disease showed significantly increased risk of all stroke (HR = 1.11, 95% CI: 1.05–1.16) and ischemic stroke (HR = 1.11, 95% CI: 1.05–1.18) after adjusting for confounders, but no significant associations were found for hemorrhagic stroke (HR = 1.08, 95% CI: 0.98–1.19). Mediation analyses showed that inflammatory markers partially mediated this relationship, with mediation effects ranging from 0.86% to 8.41% for all stroke and 1.03% to 9.58% for ischemic stroke. Genetic analyses revealed no significant interaction between high risk of periodontal disease and stroke GRS concerning the all stroke risk, but a significant interaction was found for ischemic stroke, with participants having both periodontal disease risk and a high GRS showing the highest risk (HR = 1.19, 95% CI: 1.07–1.32).
This study demonstrates a significant association between high periodontal disease risk and increased stroke risk, particularly ischemic stroke, with partial mediation by inflammatory markers and interaction with genetic risk factors.
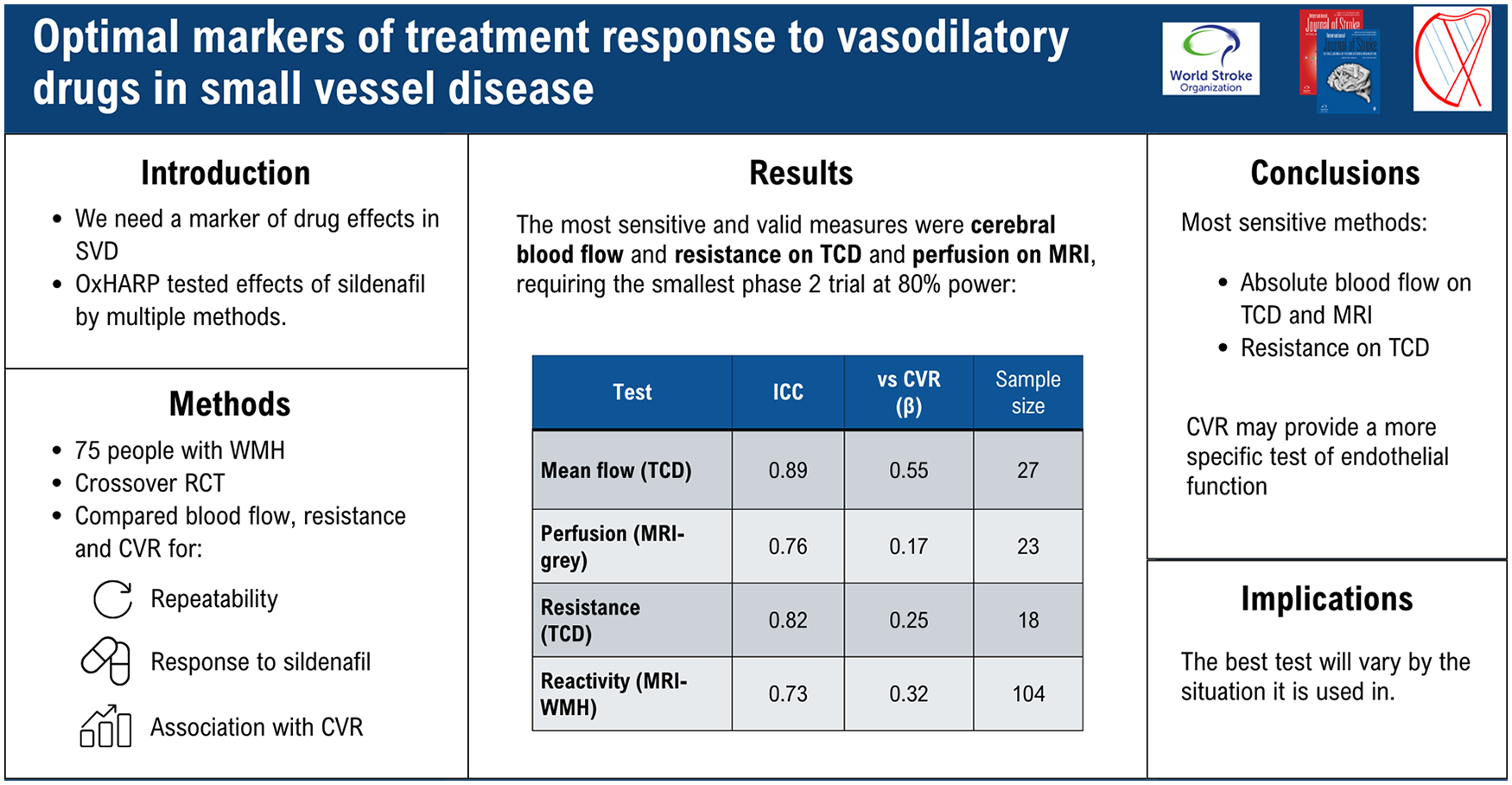
Vasodilating drugs targeting the endothelium could reduce long-term harms due to cerebral small vessel disease (cSVD) but there are no commonly accepted methods to measure short-term disease activity or drug response. In the OxHARP clinical trial, we determined the most sensitive physiological markers of treatment response to sildenafil versus placebo on either transcranial ultrasound (TCD) or magnetic resonance imaging (MRI), and their validity compared to disease severity and other measures of other physiological mechanisms.
In the OxHARP double-blind, randomized, placebo-controlled crossover trial we measured aortic blood pressure, mean flow velocity (MFV), cerebral pulsatility, cerebrovascular conductance index (CVCi = MFV/aortic mean BP), cerebral perfusion (pcASL-MRI) and cerebrovascular reactivity to inhaled CO2 on TCD (CVR-TCD) and MRI in white (CVR-WM), gray (CVR-GM) and white matter hyperintensities (CVR-WMH). Effects of 3 weeks of sildenafil were compared to placebo. Validity of markers were determined by between-visit repeatability (intraclass correlation coefficient (ICC)); associations with CVR-TCD, CVR-WMH and CVR-GM; associations with other markers; the magnitude of response, and sensitivity, to sildenafil.
In 69 participants, repeatability was greatest for MFV, pulsatility, CVCi and CVR-WMH (ICC > 0.8), very good for CVR-TCD and GM-perfusion (ICC > 0.7), and good for CVR-GM (ICC > 0.6). CVR-TCD was associated with CVR on MRI (CVR-WMH: r2 = 0.12, p = 0.02; CVR-GM: r2 = 0.22, p = 0.001), while blood flow measures on TCD (MFV, CVCi) were associated with CVR-TCD and perfusion-MRI (all p < 0.05). All markers were associated with WMH volume and improved by sildenafil, but CVCi was most sensitive, requiring only 20 patients for a crossover trial at 80% power, compared to 26 for GM-perfusion or 84 for CVR-GM.
Multiple markers were associated with cSVD, but no single marker reflected all physiological drug effects. CVCi and gray matter perfusion on MRI were the most sensitive markers of disease activity and drug response, although CVR indices may be more specific for endothelial dysfunction.
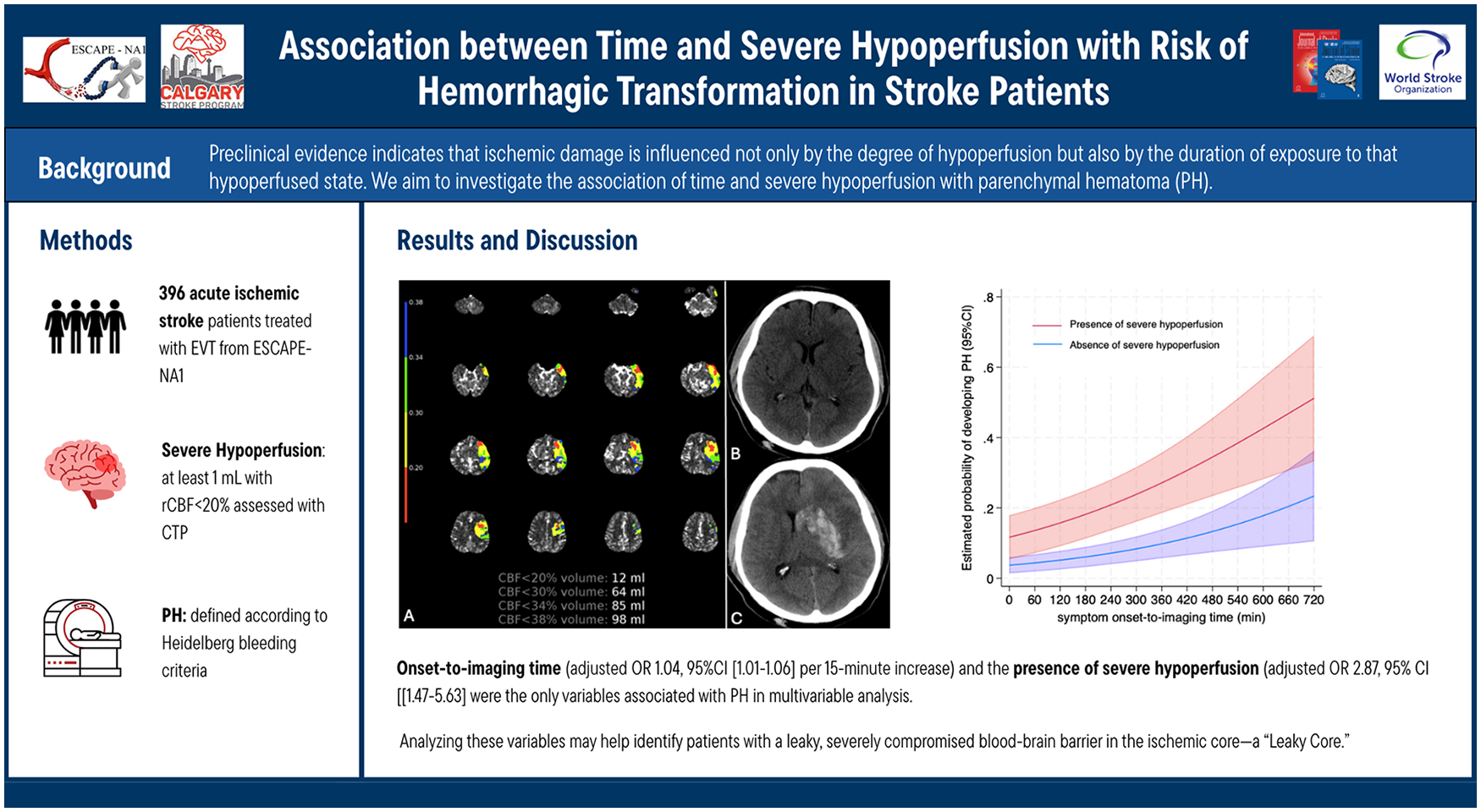
Perfusion imaging studies show a substantially increased risk of hemorrhagic transformation (HT) in severely hypoperfused tissue. Preclinical evidence indicates that ischemic damage is influenced not only by the degree of hypoperfusion but also by the duration of exposure to that hypoperfused state. We aim to investigate the association of time and severe hypoperfusion with parenchymal hematoma (PH) in ischemic stroke and explore whether there is a combined effect of the two variables on PH.
Data are from the ESCAPE-NA1 trial, which evaluated the effect of nerinetide in large vessel occlusion patients treated with thrombectomy. This study included patients with some degree of recanalization (expanded Thrombolysis in Cerebral Infarct [eTICI] > 0) and available baseline CT perfusion. Severe hypoperfusion was defined as at least 1 mL volume of relative cerebral blood flow (rCBF) <20%. We assess 24-h imaging for the presence of PH, according to Heidelberg bleeding criteria. Univariable and multivariable logistic regression analyses, including interaction terms, were used to assess the effect of time and severe hypoperfusion on outcomes.
Out of 1105 patients from ESCAPE-NA1, 396 (35.8%) were included. The median age was 70 years (IQR = 59.8–79.2), 202 (51%) were females, and 50 (12.6%) experienced PH. Onset-to-imaging time (adjusted OR 1.04 [95% CI = 1.01–1.06] per 15-min increase) and the presence of severe hypoperfusion (adjusted OR 2.87 [95% CI = 1.47–5.63]) were the only variables associated with PH in multivariable analysis. No significant interaction effect of time and severe hypoperfusion on PH was found. The presence of severe hypoperfusion had a negative predictive value of 98% and a positive predictive value of 39.4% for predicting PH in patients presenting within 3 h and after 6 h from symptom onset, respectively.
Both severe hypoperfusion and time affect the risk of hemorrhagic transformation. However, the interaction between these two variables was not statistically significant, indicating that their effects on hemorrhagic transformation risk are not dependent on each other. Analyzing these variables may help identify patients with a leaky, severely compromised blood-brain barrier in the ischemic core—a “leaky core.”
In Sub-Saharan Africa (SSA), most stroke epidemiological data comes from hospital-based registers, which are prone to selection bias, and data may be unrepresentative of stroke burden at the population level. The degree of incompleteness and bias in hospital-based registers has been assessed in high-income countries but not in an SSA country.
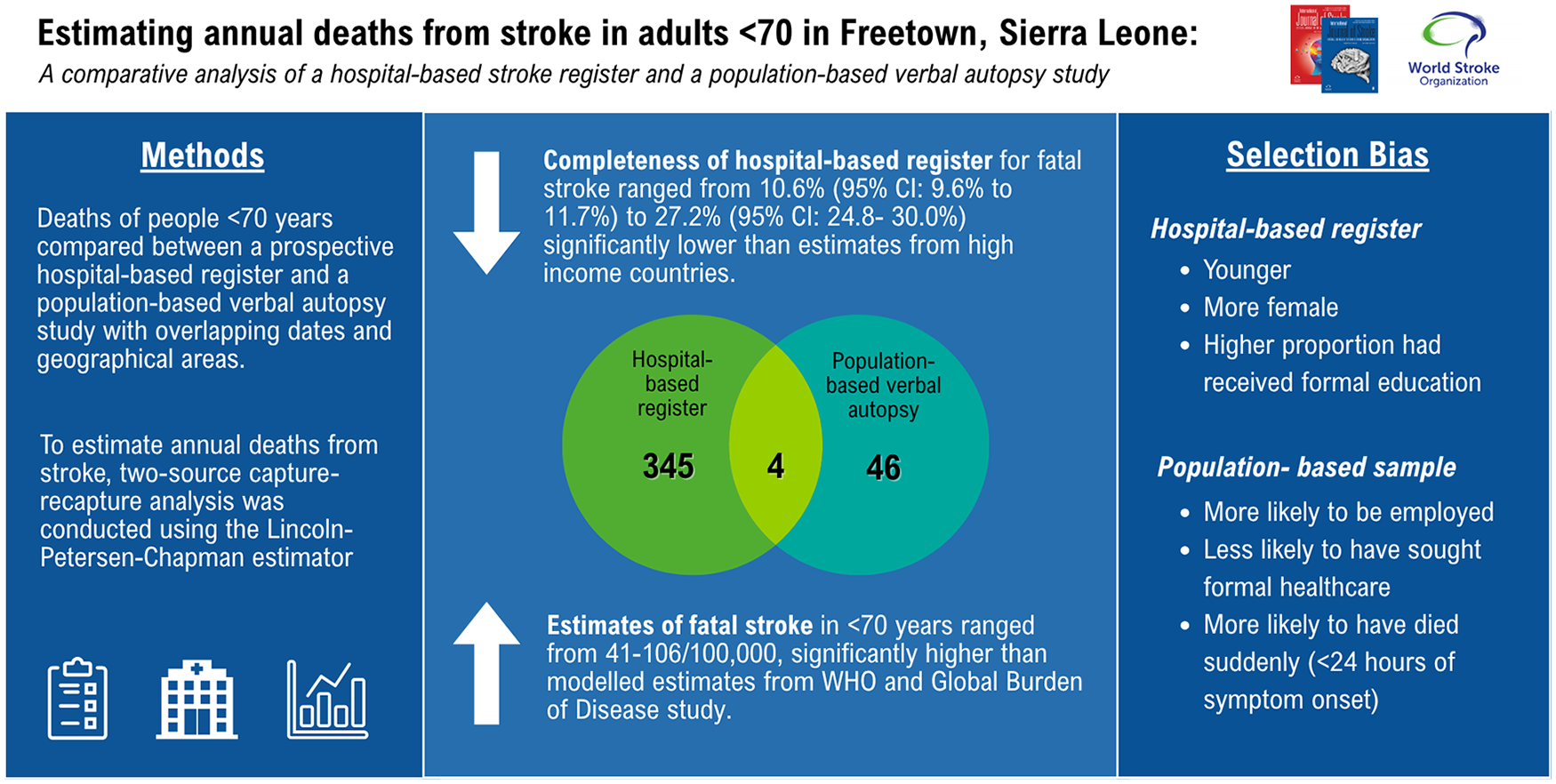
The study describes and compares estimates of annual deaths from stroke under 70 years of age, from a hospital-based stroke register and a population-based verbal autopsy (VA) study. We describe the sociodemographic and clinical differences between patients captured and those missed by a hospital-based register and estimate the completeness of a hospital-based register in Sierra Leone.
We compared people under 70 years of age who died from stroke in the Stroke in Sierra Leone (SISLE) prospective longitudinal hospital-based register to the Healthy Sierra Leone (HEAL-SL) population-based VA study which sampled 2.5% of households in the Western Area. We included participants from SISLE and HEAL-SL who died within the same dates (1st May 2019 until 30th September 2021) and geographical area. We conducted data linkage using probabilistic matching and manual clerical review by two authors. To assess selection bias, we used univariable analysis to identify variables associated with capture by the hospital register. To estimate annual deaths from stroke, two-source capture-recapture analysis was conducted using the Lincoln-Petersen-Chapman estimator. Estimates of completeness were adjusted for undermatching and for the positive predictive value of VA for stroke diagnosis. Deaths rates from stroke were calculated as deaths per 100,000 individuals, with population estimates sourced from the 2021 Mid-term Population and Housing Census.
A total of 345 participants were identified in the SISLE dataset, 46 in the VA dataset, and 4 in both datasets. Excluding individuals captured in both datasets, individuals identified by VA had a mean age of 58 years compared to 55 years in SISLE (
In this setting, a hospital-based stroke register underestimated deaths from stroke in adults younger than 70 years to a much greater degree than estimates from high-income country settings. For people who died from SISLE, employed people, people who did not seek formal healthcare, and people who died within 24 hours were less likely to be included in the hospital-based stroke register. Investment in routine death registration systems and population-based stroke surveillance is essential to provide accurate estimates of population-level stroke burden in our setting.
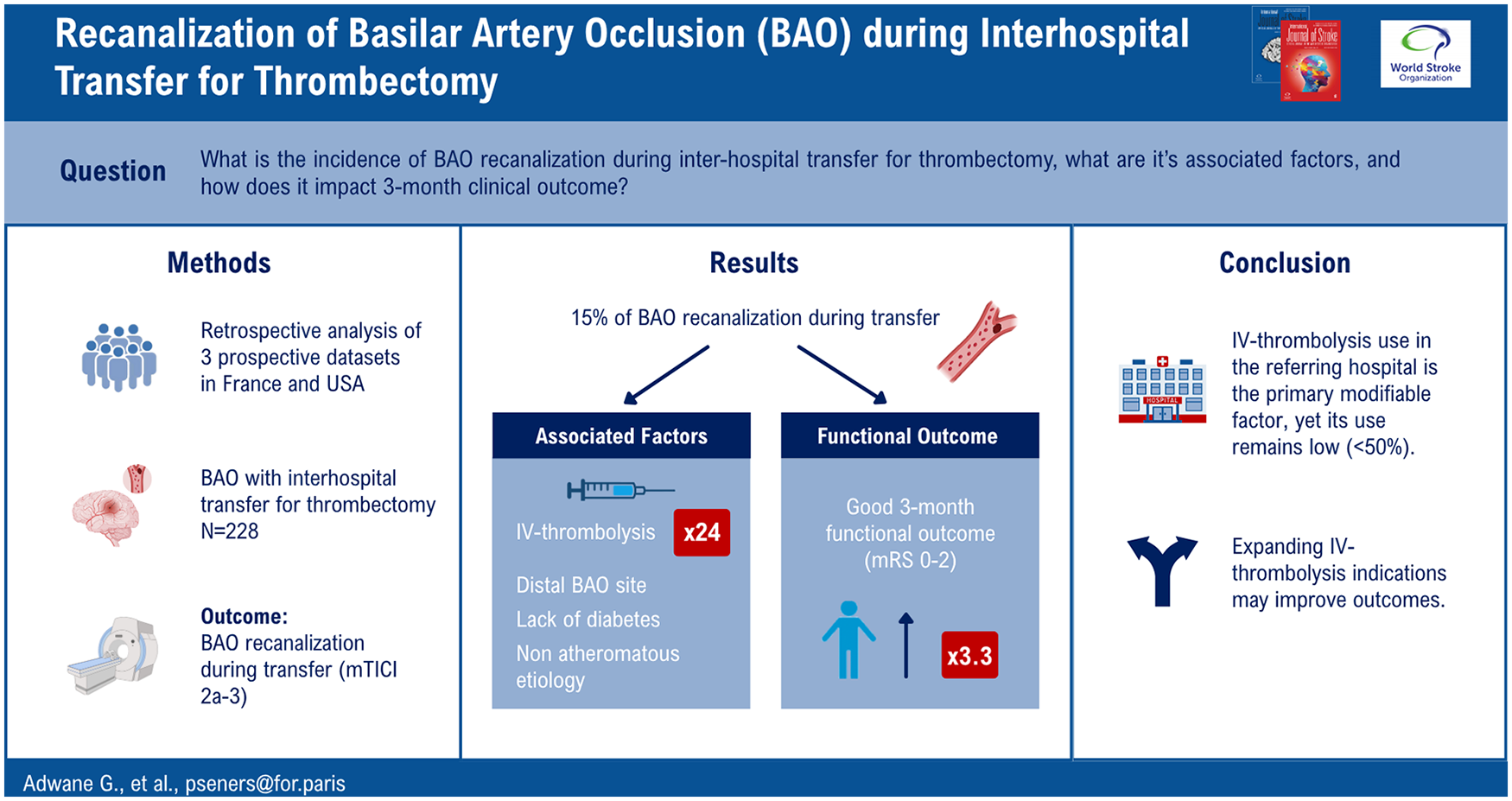
Patients with acute ischemic stroke and a large vessel occlusion admitted to non-endovascular capable centers frequently require inter-hospital transfer to a comprehensive stroke center (CSC) for thrombectomy. Data regarding arterial recanalization of patients with basilar artery occlusion (BAO) during transfer are lacking.
We analyzed prospectively collected data of acute stroke patients with BAO transferred for consideration of thrombectomy to three CSCs (Rothschild Hospital, France; Montpellier Hospital, France; Stanford Hospital, USA) between 2016 and 2024, with arterial imaging at the referring hospital and on CSC arrival. Inter-hospital recanalization was assessed by comparison of the baseline and post-transfer arterial imaging and was defined as 2a-3 on the modified Thrombolysis In Cerebral Infarction (mTICI) scale. Independent predictors of inter-hospital recanalization were assessed using multivariable logistic regression analysis.
Overall, 228 patients were included: median age 71 years, the National Institutes of Health Stroke Scale (NIHSS) of 14, transfer time of 3.5 h, and 39% of patients received intravenous thrombolysis (IVT) before transfer. The primary reason for withholding IVT was late presentation. Inter-hospital BAO recanalization occurred in 15% of patients. Variables independently associated with inter-hospital BAO recanalization were IVT use (adjusted odds ratio (aOR) = 24.3, 95% confidence interval (CI) = 6.9-85.5,
BAO recanalization during inter-hospital transfer for thrombectomy occurred in 15% of patients and was associated with a favorable 3-month outcome. IVT use in the referring center was the primary modifiable factor associated with recanalization, yet its use remains low. Expanding IVT indications in primary stroke centers and developing new therapies that increase recanalization may improve outcomes.
Hyperglycemia is common in ischemic stroke. Admission glucose modifies the effect of endovascular therapy (EVT) in patients with ischemic stroke of the anterior circulation, who are treated 0 to 6 hours since onset. Whether this also applies for late-window EVT (6–24 hours since symptom onset or last known well) is unknown. In this study, we assessed whether admission glucose level and/or hyperglycemia modifies the EVT effect in patients with ischemic stroke of the anterior circulation in the late time window.
We used data from the MR CLEAN LATE trial. The primary outcome measure was the modified Rankin Scale (mRS) score at 90 days. Secondary outcome measures were symptomatic intracranial hemorrhage and mortality at 90 days. Treatment effect modification of EVT by either glucose or hyperglycemia on admission was assessed by multiplicative interaction factors with logistic regression analysis and adjusted for potential confounders. Hyperglycemia was defined as glucose level >7.8 mmol/L on admission.
On admission, median glucose was 7.0 mmol/L (IQR 6.0–8.3 mmol/L), and 147 patients (32%) were hyperglycemic. We found no interaction of either hyperglycemia or serum glucose on admission with treatment effect on functional outcome (p = 0.76 and p = 0.79, respectively), symptomatic intracranial hemorrhage (p = 0.29 for hyperglycemia; p = 0.57 for glucose on admission), and for mortality (p = 0.52 for hyperglycemia; p = 0.69 for glucose on admission).
We found no evidence for effect modification of EVT by admission glucose level or hyperglycemia in patients with acute ischemic stroke and large-vessel occlusion of the anterior circulation in the late treatment window.