
Abstract

INTRODUCTION
average TAT for routine morning specimens of 95 minutes, and average TAT for stat specimens of 69 minutes (1);
interlaboratory median order-to-report TATs of 36 and 50 minutes in the fastest 10% of laboratories for potassium and hemoglobin tests, respectively in the 1993 College of American Pathologists Q-probes study on emergency department TAT (2);
10.6% of outliers (tests reported in excess of 70 minutes from the time the test was ordered) out of 218,551 tests, with causes of delay equally distributed among test ordering, collection of specimen, analytic phase (3)
TATs evaluated on a monthly basis do not identify daily problems. The “freckle plot” (4) displays different symbols for reports within TAT's limits, reports within 10 minutes beyond that limit, and reports well outside the limit.
OBJECTIVES
Our fully computerized clinical laboratory works in a 850 bed Hospital with no HIS network yet. The lab has been organized in departments: three of them (hematology, coagulation and chemistry), work as an emergency department both for routine and for STAT tests. Diagnostic profiles have been agreed upon with most wards, with these goals:
Reduction of clerical work of ward nurses for better utilization of their skills
Reduction of tests per patient in order to reduce costs and shorten analytical TAT
Analyzing routine as emergency (not vice-versa) in order to have same instruments, same technicians, same need for skills, same analytical TAT, reduction of replicate requests (emergency and routine)
Giving the possibility of requesting a large number of tests 24 hours a day in order to reduce venipunctures and requests to the same patient for emergency and routine tests
Reduction of brain to brain TAT for shorter hospitalization and faster clinical diagnosis.
MATERIALS AND METHODS
LIS is by Metafora Informatica (Milano, Italy).
Chemistry is composed by three Vitros 950 and two Vitros 250 by Ortho Clinical Diagnostics (Rochester, NY).
Coagulation is composed by two STA Systems by Roche Diagnostic Systems (Branchburg, NJ).
Hematology is composed by two Sysmex SE-9000 by TOA Medical Electronics (Kobe, Japan).
Request forms go through two optical readers, with priority given to emergencies.
Tube caps differenciate STAT tests. Both routine and emergency reports are automatically printed every 5 minutes.
Tests which can be requested 24 hours a day are: CBC, differential, prothrombin time and INR, partial thromboplastin time, fibrinogen, D-dimer, glucose, BUN, creatinine, uric acid, total and direct bilirubin, total protein, Na, K, total Ca, Mg, inorganic phosphorus, AST, ALT, GGT, alkaline phosphatase, amylase, lipase, cholesterol, triglycerides. 75,000 stat tests and 103,000 routine tests have been performed and analyzed for TAT, also according to time of the day.
RESULTS
We have evidence of higher comfort and satisfaction of ward nurses in order compilation.
Number of tests per patient has been reduced by about 20%.
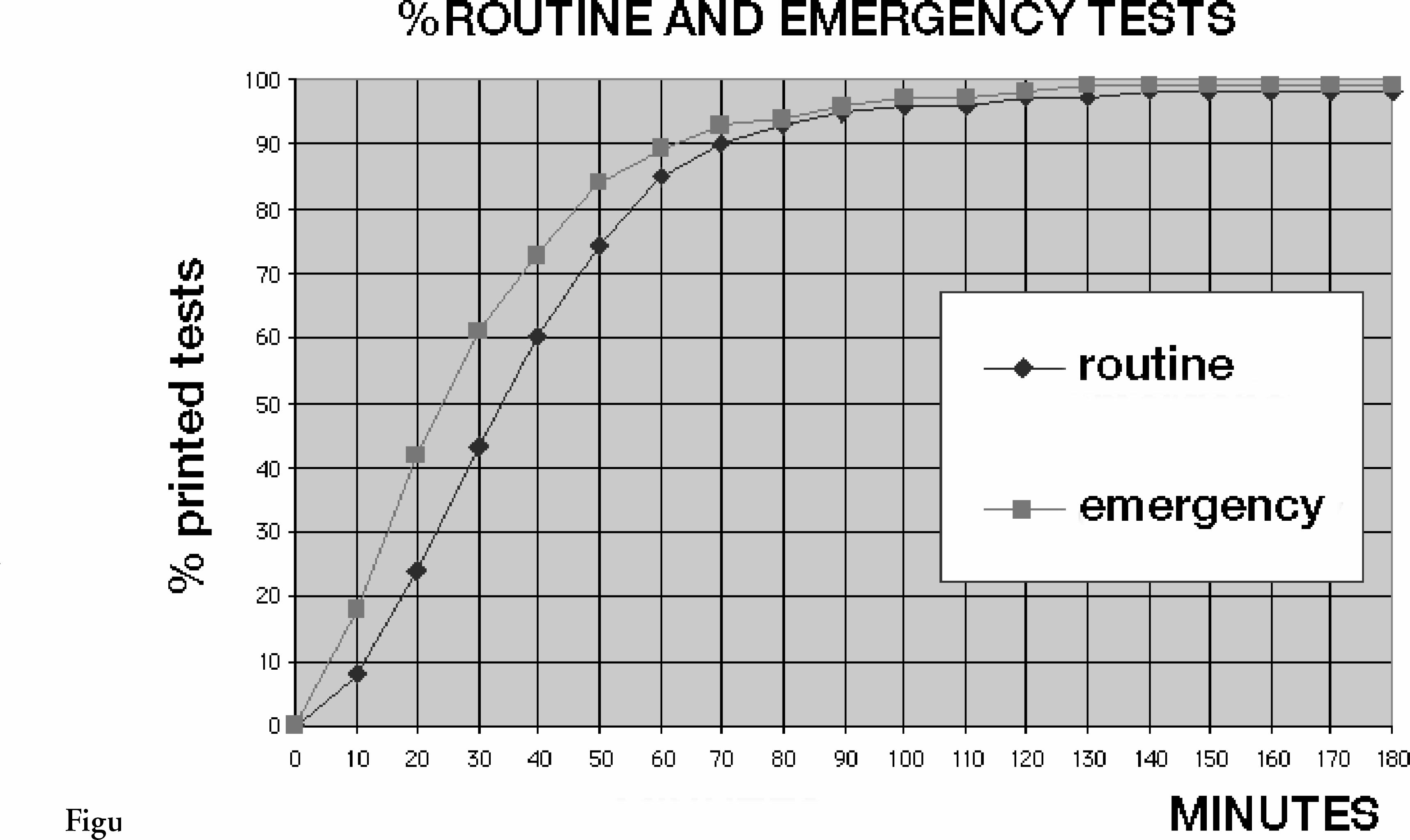
Mean TAT times are: 31' for emergencies, 41' for routine tests. 85–90% of tests are reported within one hour (
As can be seen both in figure 1 and 2, requests often do not differenciate between routine and STAT: routine tests are requested 24 hours a day. Probably a part of the 20% reduction of tests depends on reduction of replicates.
A study is now being carried out to look after preanalytical delays (from ward order to laboratory acceptance), and postanalytical delays (from result printing to ward receiving the results).
CONCLUSIONS
Too many emergencies is a problem of lab organization, not a clinical one. In our lab we don't have an emergency department, and mean global TAT is below 41' for 73% of the tests performed in the lab. Many tests can be requested 24 hours a day, even in excess of clinical necessity, so reducing replicate requests. Emergencies are treated with priority by the same technicians on the same instruments as routine tests.
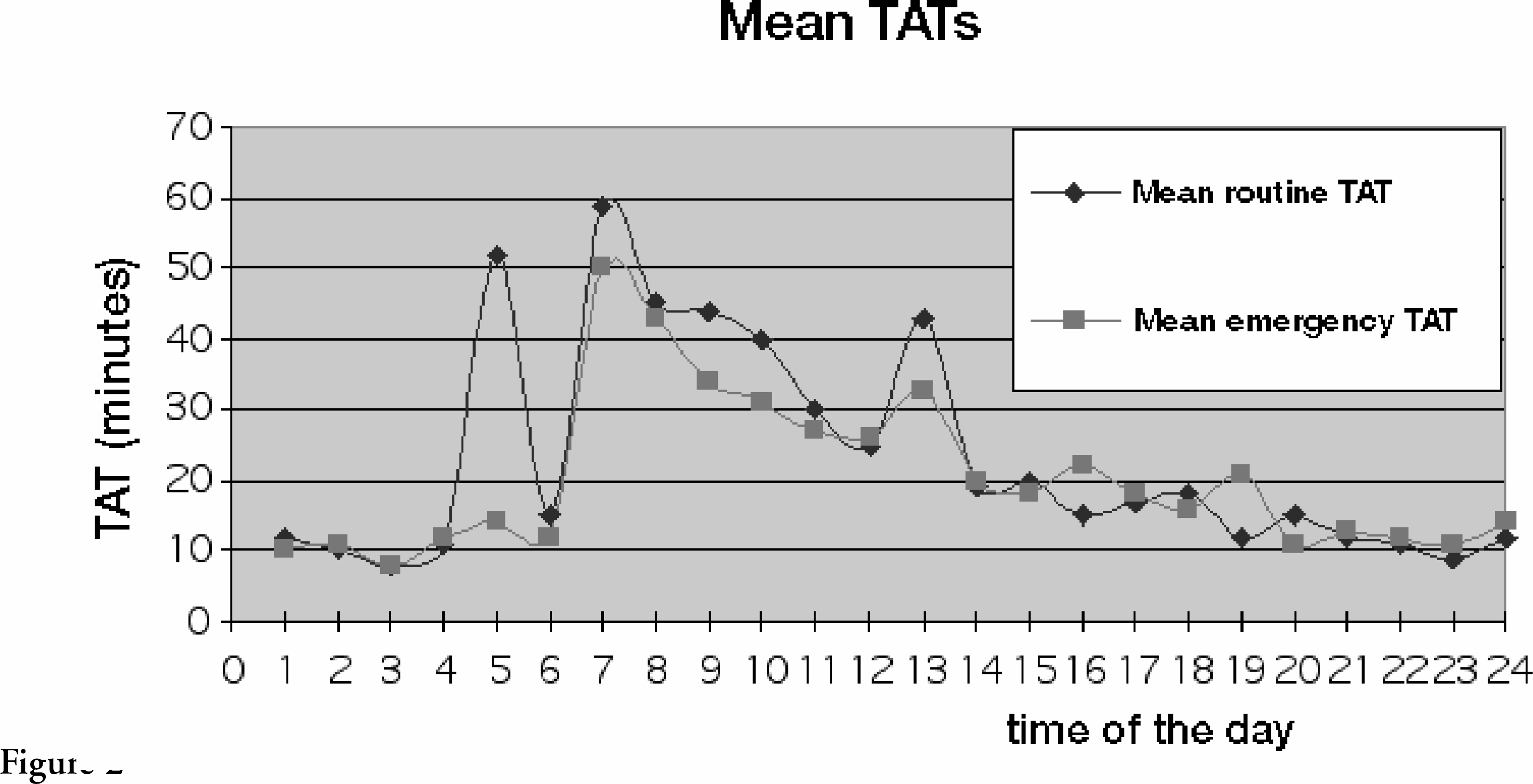
Long TATs have been demonstrated at 5 a.m., 7 a.m., and 1 p.m. (see figure 2): problems are probably related to shifts, but real causes still have to be looked for, and remedies found.
The presence of routine requests 24 hours a day demonstrates that the wards have understood there is almost no difference between routine and emergency TATs.
For the moment we have worked on analytical times: results are shown in figure 1. Pre- and post-analytical delays are next in our schedule of problems to be solved, with airtube and HIS network.
Footnotes
Acknowledgements
If you are interested in seeing more articles like this in JALA, please email