
Abstract
The objective of this study was to evaluate and compare the filling ability of various root canal obturation techniques on the internal root resorption (IRR) cavities of replicated tooth samples manufactured using computer software and a three-dimensional (3D) printer. Orthographic images and root structures of a healthy upper maxilla central incisor in determined volumes and sizes were drawn as a prototype with the aid of computer software. Using the same software, an IRR defect was also modeled. These two images were then transferred to the AutoDesk Fusion 360 3D modeling program (AutoDesk, San Rafael, CA) for meshing. Afterward, the tooth model was transferred to a 3D modeling and prototyping program (RhinoCeros 3D; Robert McNells & Assoc., New York) and printed on a 3D printer. Eighty replicas with IRR were manufactured and divided into four groups (n = 20 per group) according to the obturating techniques as follows: Group 1: Cold lateral compaction (CLC), Group 2: Core Carrier System (GuttaCore), Group 3: Injectable Cold Filling (GuttaFlow® BioSeal), and Group 4: Continuous Wave Obturation System (Elements Free). After root canal filling, replicas were scanned with a high-resolution micro-computed tomography system (SkyScan 1172; Bruker-microCT, Kontich, Belgium), data regarding voids (unobturated areas) inside the IRR defects were statistically analyzed using nonparametric Kruskal–Wallis tests. A pairwise comparison between the tested groups showed that Groups 3 and 4 had significantly fewer voids compared with Groups 1 and 2 in IRR defects (p < 0.05). Group 1/Group 2 and Group 3/Group 4 had similar results in terms of voids and there were no statistically significant differences (p > 0.05). The injectable cold filling system (GuttaFlow BioSeal) and the injectable continuous wave obturation system (Elements Free) successfully obturated the pathological IRR irregularities when compared with CLC and core carrier (GuttaCore) systems.
Introduction
The main goals of root canal treatment is to complete disinfection. Hermetically filling the root canals after mechanical shaping is also an another important issue. 1 Any pathology and irregularity within the root canal can make this process difficult. 2 Internal root resorption (IRR) is also a challenging pathological process that is difficult to clean, disinfect, and obturate hermetically. 3 IRR may occur as a result of chronic irreversible changes in any part of the root canal. 4 In turn, the mechanical shaping, disinfection, and root canal filling procedures of these teeth become very difficult due to the irregular structures of the dentin.4,5 Inflamed pulpal and granulation tissues may bleed during mechanical shaping, which might impair visibility, and the geometry of the IRR defect might negatively affect the mechanical instrumentation due to the complex irregularities of the root canal walls. 4
There is no clear information about which root canal filling materials used today will obturate this defect in a leak-proof manner. 6 Cold lateral compaction (CLC), the GuttaCore System with a gutta-percha (GP) carrier, continuous wave condensation and injectable cold filling techniques have different dynamics, but it is not yet known which of these will fill the root canal containing a resorptive cavity in an ideal manner.
Using CLC, master GP cone is inserted through the working length of the root canal covered with root canal sealer and discrepancies of the root canal is obturated with a large number of accessory GP cones having different diameters apically. 2 In this technique, since all material used is in solid form, irregular structures such as the IRR may not be completely obturated. 5 CLC forms a cold-welded nonuniform mass of GP, namely in different thirds of the root canal. 7 Using thermoplastic filling techniques, such as warm injectable GP and continuous wave condensation methods, for obturating irregular structures in the root canal have shown success with respect to their ability to obturate the defects more successfully when compared with the CLC, in terms of increased GP density, which leads to fewer voids, in view of flowing GP.6–9 In some cases, using different root canal filling techniques and materials together to provide a hermetically acceptable root canal filling has been suggested. 2
Previously published studies on shaping and obturation of the IRR have not been successful in standardizing the IRR cavities.2,5,8 In these studies, for creating artificial IRR, the roots of extracted maxillary central incisors were sectioned horizontally with a fine diamond disk 7–8 mm from the apex. Semicircular cavities were created using a low speed no. 6 round diamond bur around the periphery of the opening of the root canal of each section. Afterward the sections were cemented together using glue on the dentine surface around the cavities. In these ex vivo studies,2,5 none of the samples were physically dissimilar to each other. According to the hand sensitivity of the clinician who prepares the semicircular cavities using handheld instruments, it may not always be possible to create the same cavity size, which may produce a lack of standardization of the samples. 10 Therefore, with the development of three-dimensional (3D) printing and resin replica production technology, it is now possible to create replicas that physically resemble the sample tooth.11,12 For this purpose, high-resolution 3D software technologies have been used. 13 Replicas can be obtained in sufficient numbers for research, without restriction, and when it comes to ensuring standardization, each replica has the same physical characteristics as the other. 13 In addition, tooth modeling with the desired pathology can be performed in the computer environment software and replicas of this solid model can be produced using a plastic filament as a printing material. 14
To the best of our knowledge, this is the first research that has created replicas with an IRR model that provides complete standardization using remodeling of the tooth by a computer software and 3D printing.
The objectives of this study are as follows:
To create a tooth model with IRR on computer software and use a 3D printer to manufacture replicas with the same physical properties. To evaluate and compare the filling quality of the IRR defects when the root canals were obturated using CLC, the core carrier system (GuttaCore), an injectable cold filling (GuttaFlow® BioSeal), and a continuous wave obturation system (Elements Free).
The null hypothesis tested was that there would be no significant difference regarding voids produced by the mentioned techniques.
Materials and Methods
Data from a previous study 12 were used to calculate the required minimum sample size for this study by using the G*Power v.3.1.9.2 program (Heinrich Heine, University of Düsseldorf, Düsseldorf, Germany). An α-type error of 0.05 and a beta power of 0.80 were specified and calculated based on these parameters. Thus, the minimum estimated sample size for each group was 19. To increase the statistical power and considering the potential sample loss, we decided to have 20 samples per group. Therefore, a total of 80 samples were included in this study. Since this research does not involve any human or animal participants or content, ethical approval is not required for the present study.
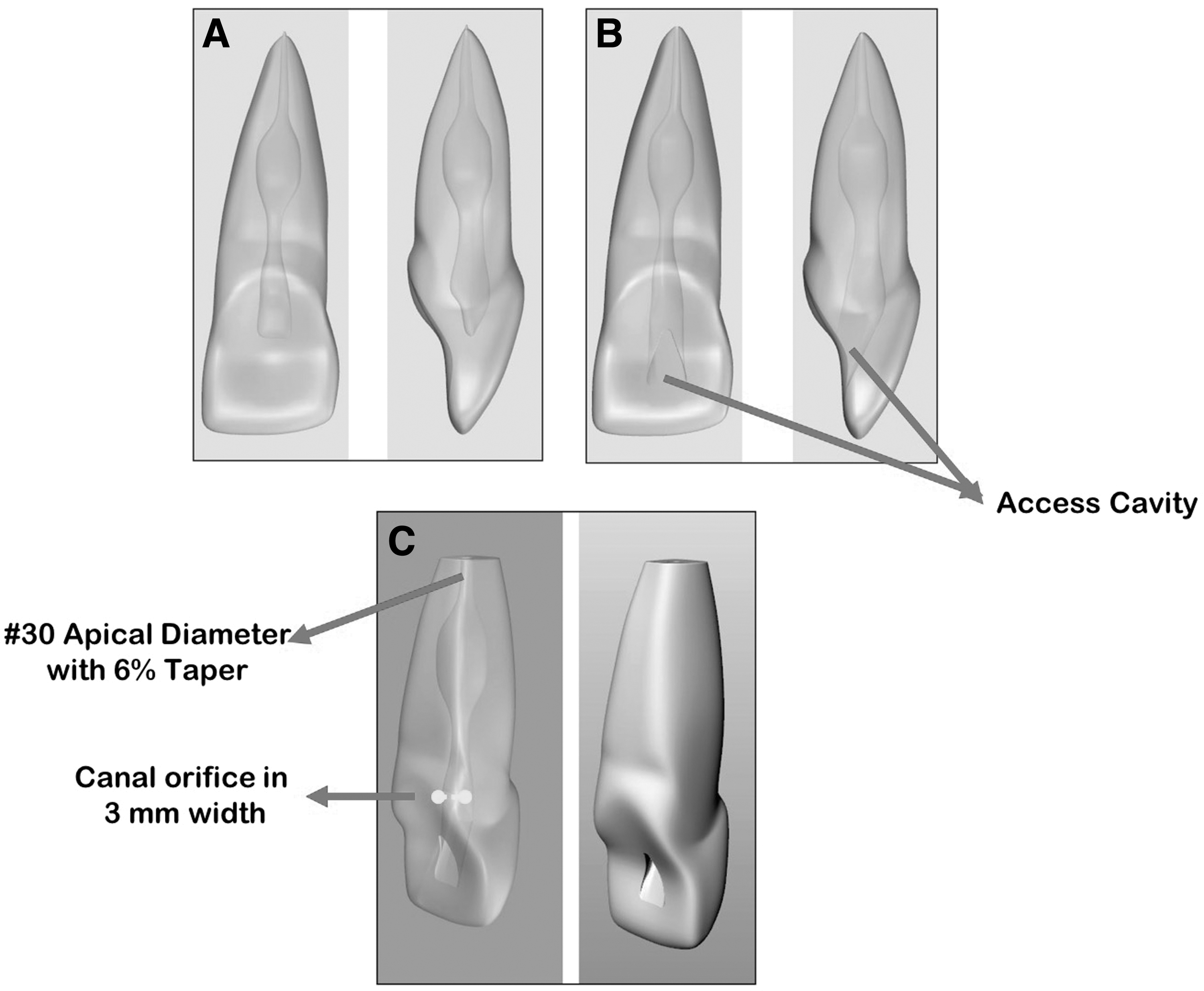
Orthographic images and root structures of the healthy upper maxilla central incisor in determined volumes and sizes were drawn as a prototype with the aid of a computer using AutoDesk Fusion 360 3D modeling program (AutoDesk, San Rafael, CA) (Fig. 1A, B). These images were then created for product design and transferred using the same AutoDesk Fusion 360 3D modeling program, which is a cloud-based software. After meshing, a healthy human tooth solid model was created 14 (Fig. 1A, B). As with creating the healthy tooth model, a circular-like IRR solid pathology was also designed in the same manner using the meshing programme (AutoDesk; Fig. 1C, D). These two solid creations (tooth and IRR pathology) were then transferred to a 3D modeling and prototyping program (RhinoCeros 3D; Robert McNells & Assoc., New York) in non-uniform rational basis spline modeling software (Fig. 2A–C). Afterward, the tooth model and IRR were exported in a 3ds file format. After bunching the two images to each other using the same software (RhinoCeros), an access cavity design was performed (Fig. 2B). The root canal was designed and modeled to a diameter of #30 in the apical third with a 6% taper (Fig. 2C). The orifice of the root canal was modeled as if a ProTaper SX file (Dentsply Maillefer, Ballaiguea, Switzerland) was used with circumferential filing to a diameter of 3 mm, and the designed tooth model was ready for root canal filling on the software. When bunching was completed for every image, the solid tooth design was saved and exported in a 3ds file format (Fig. 2C).

Data from anatomical structures of a maxillary central incisor tooth were transferred into a modeling program using software (AutoDesk)
For manufacturing the replica, a bioplastic, based on corn starch material, polylactic acid (PLA) PLUS filament (FK Filament, Giresun, Turkey) was used with the 4GenPro 2R 3D printer (3D4E Design, Ankara, Turkey). PLA Plus, which was preferred due to its rigid and durable structure, was printed with a precision of 200 μm in a printer adjusted to 75°C and a 210°C nozzle temperature. 15 Owing to the volume and amorphous structure of the dental prototype, it was decided to print the filament slower to prevent the collapse of the layers, and each replica was printed in ∼16 min.
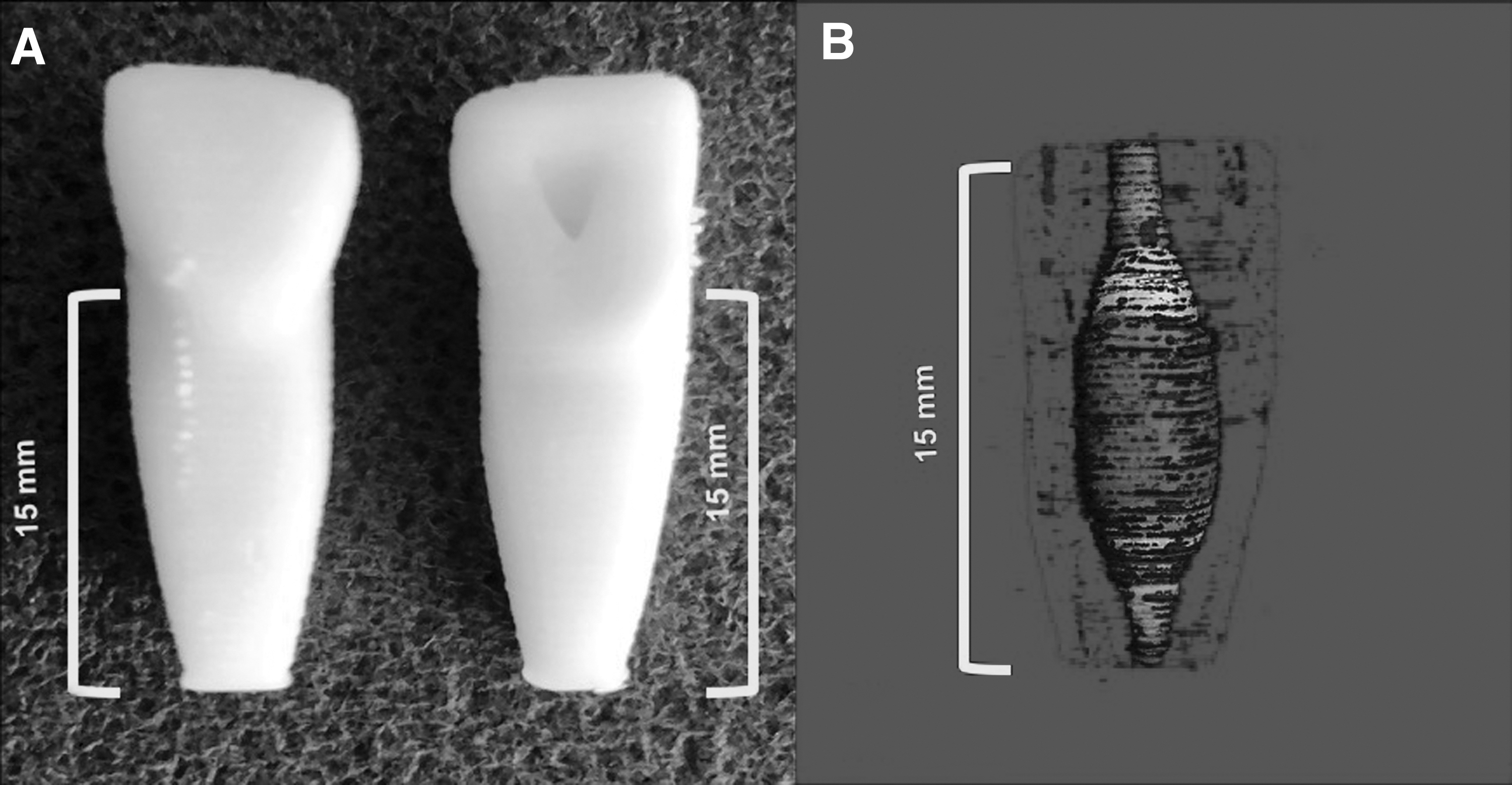
Eighty replicas (Fig. 3A) produced with PLA, and duplicates of each other, were assigned to four groups of 20 replicas each. The IRR cavities within the replicas (Fig. 3B) were obturated using four different root canal filling techniques as follows:
Group 1. CLC: a standardized #30/.02 GP cone (Diadent, Cheongju, Korea) coated with AH Plus (Dentsply Maillefer) was fitted as a master cone within 0.5 mm of the working length. Freshly mixed root canal sealer was applied to the root canal walls using GP in a counterclockwise rotation. Lateral compaction was achieved using standardized finger spreaders (Dentsply Maillefer) using #25, #20, and #15, respectively. When the spreader was unable to penetrate beyond the coronal third of the root canal, the canal was considered adequately obturated. Approximately 15–20 lateral GP points were used for each replica. The remaining GP residues were removed using a heated hand plugger (Buchanan Hand Plugger; SybronEndo, Peterborough, UK).
Group 2. Core carrier system (GuttaCore): the root canal diameter in the apical third was verified using the #30 GuttaCore (GC) Size Verifier (Denstply, Sirona, OK). A #30 GC obturator (Denstply) was then placed in the GuttaCore Heater Obturator Oven (Dentsply, Sirona). The obturator was heated for a minimum of 15 s in accordance with the manufacturer's recommendations. Meanwhile, AH Plus was applied on the root canal walls using #30/.06 paper points. The heated obturator was slowly inserted into the canal within 0.5 mm of the working length. When the GP cooled down, the obturator was twisted into two parts, whereas retaining the main core inside the root canal. The remaining GP residues were removed using a heated hand plugger.
Group 3. Injectable cold filling (GuttaFlow BioSeal): GuttaFlow BioSeal (Coltene, Whaledent AG, Altstatten, Switzerland) was applied 3 mm shorter than the working length using an automatic mixing tip from the apical to the coronal regions. During the procedure, the mixing tip was not withdrawn from the root canal; rather, the tip was allowed to rise spontaneously toward the coronal region. AH Plus was not used as a root canal sealer in this group.
Group 4. Continuous wave obturation system (Elements Free): A #30/.06 master GP was covered with AH Plus and inserted into the canal, down-packed as a 3–4 mm apical filling with the Buchanan Heat Plugger (SybronEndo). The Elements GP Cartridge (SybronEndo, Kerr Endodontics, Orange, CA) attached to the backfill unit was heated to 160°C and injected into the root canal in one attempt. The remaining GP residues were removed using a heated hand plugger.
Replicas were stored for 1 week at 37°C and in 100% humidity to allow the sealer to set completely before micro-computed tomography (CT) scanning. All root canal obturations were performed by a single operator.
Micro-CT analysis
Replicas were scanned with a high-resolution micro-CT system (SkyScan 1172; Bruker-microCT, Kontich, Belgium). The X-ray source was operated with a 0.5 mm Al+Cu filter at 85 kV and 118 μA with 13.68 μm pixel resolution. Each replica was scanned for 60 min and the raw data were reconstructed into images using NRecon v.1.6.3 software (Bruker-microCT). The voids (unobturated areas) inside the region of interest, where the root canals were not obturated by the filling material, were then analyzed using the micro-CT. The apical and the coronal thirds of the root canals were out of interest.
Statistical analysis
IBM SPSS statistics software (version 25.0; SPSS Inc., Chicago, IL) was used for the data analysis. The data were not normally distributed according to the Lilliefors-corrected Kolmogorov–Smirnov test. Therefore, nonparametric Kruskal–Wallis H tests were used to evaluate the differences between the groups (p < 0.05). A pairwise comparisons module in the SPSS program was used for the binary comparisons (α = 0.05).
Results
According to the results of 3D micro-CT imaging analysis (Table 1; Fig. 5), the best quality in root canal obturation was formed using Group 3, the injectable cold filling, and Group 4, the continuous wave obturation system, where compressions of the filling material toward the cavity walls were nearly flawless (Fig. 2C, D).
The Mean, Standard Deviation, Median, and Minimum and Maximum Values of Unobturated Areas within Internal Root Resorption Defects for Each Group
CLC, cold lateral compaction; SD, standard deviation.
The amount of unobturated area was quite low (Table 1; Figs. 4C, D and 5). This degree of harmony and quality was not seen in Group 1 or Group 2. Neither root canal sealers nor canal obturation materials were able to hermetically seal IRR areas (Fig. 4A, B).

MicroCT images of the replicas filled by different obturation techniques.
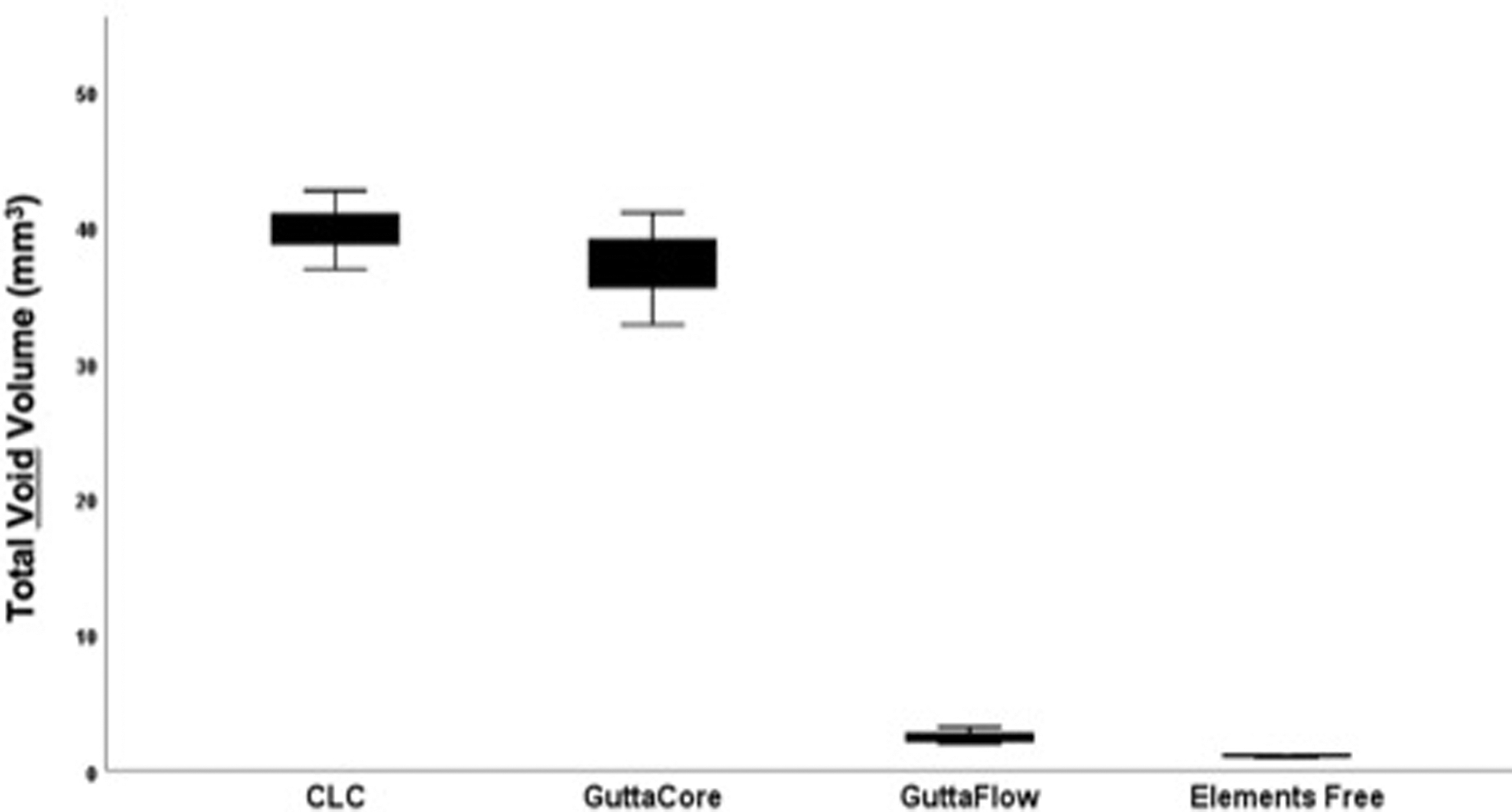
A BoxPlot graphic of the total void volume remaining in unobturated areas after root canal obturation.
According to the result of the Kruskal–Wallis test, there was a statistically significant difference between the tested groups in terms of void volume (p < 0.05). Data examined with the Bonferroni correction in multiple tests showed no significant difference between Group 1/Group 2 and Group 3/Group 4 in terms of voids (p > 0.05). However, the differences were significant between Groups 1/3, Groups 1/4, Groups 2/3, and Groups 2/4, respectively (p < 0.05).
Regarding the unobturated area, the least void was 13.4 mm3 in Group 4 and 27.6 mm3 in Group 3 (Table 1; Figs. 4C, D and 5). There was a huge volume of unobturated regions in Group 1 with 63.45 mm3 and Group 2 with 57.55 mm3 (Table 1; Figs. 4A, B and 5).
Discussion
It is almost impossible to mechanically shape the entire root canal walls affected by IRR, as there will be areas left untouched by the instruments. 4 Even if these areas are not cleaned, all irregularities should be obturated with root canal filling materials to ensure microbial control. 8 The main goal is to fill the resorption area with the least volume of canal sealer and the maximum volume of GP. The reason for this is because the sealant will shrink while polymerizing, thereby leaving undesirable gaps and voids that will occur between the paste and the walls over time, thus increasing the possibility of reinfection.16,17 Therefore, in light of our findings, we can state that an injectable root canal filling contains more GP by volume, adapts to irregular structures and fills the voids volumetrically. Since cold/warm injectable GP may better adapt to these irregularities, IRR cavities will be successfully and hermetically obturated using these materials.
Owing to its complex structure and irregular root canal wall structure, it is very difficult to complete the root canal filling in a leakproof manner in cases of IRR. In these cases, it is preferred to use thermoplastic GP filling techniques.16,18 Our results support these suggestions. Namely, considering the pathologies of the replicas, we determined we were successful with root canal fillings obturated by the injection techniques. Both warm and cold (GuttaFlow BioSeal and Elements Free, respectively) injection techniques successfully filled the resorption gaps with an average of 80 mm3. In contrast, this ratio was ∼40 mm3 in the CLC and GuttaCore systems; that is, Groups 3 and 4 were at least twice as successful as the other two groups. Although the GuttaCore in Group 2 was an obturation technique used by heating, the filling material was stripped from the GP-based carrier from the first moment it was placed through the access cavity and was not able to obturate the hollow space of the IRR (Fig. 2B). In addition, as stated previously by Goldberg et al. 19 and Agarwal et al., 20 Thermafill, which is also a core carrier-based system, was incapable of obturating resorptive cavities. Gençoğlu 21 evaluated the quality of root fillings in teeth with IRR and concluded that core carrier-based systems, such as Thermafill and Soft-Core, are less effective for filling resorptive cavities compared with MicroSeal and System B, which are both injectable. In another study of Gençoğlu et al., 2 effectiveness of different GP techniques was evaluated when filling experimental internal resorptive cavities and they also concluded that warm GP condensation technique was better than CLC and core carrier-based systems. Despite there is similarity with previous study and findings; they found the void ratio of CLC lesser than this study. One may explain the potential sources of this variability due to the specific geometry. In this study, an IRR defect, very close to real scenario, was designed and manufactured using the computer-based software and 3D printing technology. In this real scenario, the crown of the tooth was not removed, as in real in vivo cases. So, using CLC technique was sometimes difficult because root canal instrumentation size was not increased to a diameter of 0.60 mm as like Gençoğlu et al., 2 limiting it to a diameter of 0.30 mm, with a limited coronal flaring to protect the remaining dentine of the root canal. In addition, after root canal obturation, they only sectioned the root at 7 mm from the apex, took photograph and evaluated using a two-dimensional image processing system; however, in this study, voids were analyzed using a 3D volume processing system, micro-CT.
Considering that the overall distribution of voids (unobturated areas) were significantly different and higher in the comparison of CLC and GuttaCore compared with GuttaFlow BioSeal and Elements Free, our null hypothesis was rejected.
While evaluating the efficiency of root canal filling techniques compared with each other, it is important to provide similar, but preferably the same, physical standardizations on samples. This issue is particularly important in studies that focus on teeth, which may show many variations, such as IRR 5 or C-shaped canals.9,12 Thanks to technological developments, it is now possible to reproduce 3D root canal structures using models made with high-resolution 3D-printing out of thermoplastic or thermosetting polymers.11,15,22 Since the produced samples will be physically similar to each other, between-groups comparisons of the data will be more valid and will offer greater standardization. To ensure the reliability of the results in comparative studies, it is important to use teeth with the same anatomy as those produced by 3D printing technology.
However, these computer software-based canals, which are replicas of an IRR of the canal system, do not fully represent the clinical cases of root canals with IRR and, therefore, stand out as a limitation of this study. 9 In addition, regarding the surface difference for the adhesion of root canal sealer or the GP to resin 3D printing material, there may be slight differences in adhesion compared with human teeth, which could be considered as another limitation of this study. 8
Additive manufacturing (sometimes referred to as rapid prototyping or 3D printing) is a method of manufacture where layers of a material are built up to create a solid object. In general, dental models due to their unusual geometries are widely printed in high-resolution 3D printing systems, as like fused deposition modeling (FDM), stereolithography (SLA), or material jetting (MJ) systems. 23 FDM is the most widely used type of 3D printing at the consumer level because it is cost-effective, the lead times are short, easy to use, and a wide range of thermoplastic materials are available such as PLA, acrylonitrile butadiene styrene (ABS), polyethylene terephalate glycol (PETG), polycarbonate (PC), and polyetherimide (PEI). However, it has the lowest accuracy and resolution compared with other 3D printing systems. In addition, since FDM parts are likely to have visible layer lines, postprocessing may require smoothing. 24 Despite its disadvantages, FDM has a common layer height of 50–400 μm, which is suitable for our study. The advantages summarized earlier are the main factors for FDM to be preferred in this study. SLA 3D printers use a laser to cure liquid resin into hardened plastic and they are popular for their ability to produce high-accuracy, isotropic, with smooth surface finish, with a common layer height of 25–100 μm. SLA allows increased unsupported overhanging volumes and typically performs similar or better than filament printing. Several dental-grade SLA resins offer outstanding properties in comparison; however, due to its high cost, SLA was not preferred to use in this study. MJ is a polymer jetting process in which a printhead dispense droplets of a photosensitive material that solidify under ultraviolet light, building a part layer by layer. MJ has a common layer height of 16–32 μm, giving the most accurate 3D printing technology. MJ can be used with a variety of materials, including photosensitive polymers, metallic or ceramic suspensions, as well as biological formulations. MJ has great benefit in regard of high resolution, and its multijetting capability may deliver more realistic dental and general medical structure prototypes; however, similar to SLA, MJ also has a high cost and due to this disadvantage, MJ was not used in this study.
Advances in 3D printing technologies have made it possible to effectively create identical replicas of extracted human teeth that can be used for standardized preclinical endodontic training 25 and, more recently, for the evaluation of the obturation techniques in the endodontic field.12,26 Although the 3D printed teeth do not reflect the properties of the real teeth tissue, they provide optimum standardization for obturation comparison studies. Gok et al. 12 and Holmes et al. 26 used 3D printing technologies to compare different obturation techniques similar to this study. The results of these studies are not suitable for comparison with the results of our studies because this study only investigates the obturation quality of the IRR gaps. It is noteworthy that after the developments in this area, 3D printed teeth are frequently preferred in the studies related with the endodontic obturation techniques. In addition, 3D printed technology used in this study appears to be a practical and useful method and looks very promising in terms of dental research.
In our research, unlike studies using replicas, a maxillary central incisor tooth was modeled using computerized software and then an IRR pathology was created in this virtual tooth. A tooth model with IRR was created 3D using algorithms. To the best of our knowledge, this research is the first and only research using 3D software technology to model a solid tooth with IRR and produce many replicas with the same anatomy, which compares the obturation quality of four different root canal obturation materials in IRR cavities.
Conclusion
Limited to the findings of this research, the injectable cold filling system and the injectable continuous wave obturation system successfully filled the pathological irregularities in the presence of IRR. Based on these results, we can conclude that the obturation materials preferred by clinicians in cases of IRR should have a fluid consistency. The continuity of clinical research on this subject is advised, although these factors may not be easily quantitatively determined in vivo.
Modeling teeth using computer software may enable research on various cases. In comparative studies, similar to this study, it has been shown to be important to use teeth with the same anatomy as those produced by 3D printer technology to ensure the reliability of the results.
Footnotes
Authors' Contributions
Conceptualization, data curation, formal analysis, investigation, methodology, supervision, validation, writing—original draft, and writing—review and editing by S.Y.Ö. Data curation, formal analysis, investigation, methodology, validation, visualization, and writing—review and editing by H.D.Ö. Investigation, methodology, software, validation, visualization, and writing—review and editing by İ.O.
Author Disclosure Statement
The authors declare they have no conflict of interest. English grammar and spellings were checked under #723743 by Scribendi, according to the journal's guidelines.
Funding Information
This study was supported by the Scientific and Technological Research Council of Turkey (TÜBİTAK) Grant No. 1002-218S867. The foundation had no role in performing and publishing this study.