
Abstract
It is increasingly common to produce physical anatomical medical models using high-fidelity multiproperty 3D printing to assist doctor–patient communication, presurgical planning, and surgical simulation. Currently, most medical models are created using image thresholding and traditional mesh-based segmentation techniques to produce mono-material boundaries (STL file formats) of anatomical features. Existing medical modeling manufacturing methods restrict shape specification to one material or density, which result in anatomically simple 3D printed medical models with no gradated material qualities. Currently, available high-resolution functionally graded multimaterial 3D printed medical models are rigid and do not represent biomechanical movement. To bypass the identified limitations of current 3D printing medical modeling workflows, we present a bitmap-based “voxel” multimaterial additive manufacturing workflow for the production of highly realistic and flexible anatomical models of the neonatal lower limb using computed tomographic (“CT”) data. By interpolating and re-slicing a biomedical volumetric data set at the native 3D printer z resolution of 27 μm and using CT scan attenuation properties (Hounsfield units) to guide material mixing ratios, producing highly realistic models of the neonatal lower limb at a significantly faster rate than other manufacturing methods. The presented medical modeling workflow has considerable potential to improve medical modeling manufacturing methods by translating medical data directly into 3D printing files aiding in anatomical education and surgical simulation practices, especially in neonatal research and clinical training.

Introduction
History
Scientists, physicians, artists, engineers, criminals, and martyrs were all instrumental in laying the foundation for the progression of anatomical imaging and, subsequently, medical modeling.1–3 Seeking to replicate the human body at a high fidelity has been central to the progression of present-day anatomical knowledge. Despite the wealth of knowledge available about the human body, it is still difficult to communicate life beneath the skin's surface—especially on a case-by-case basis.
Historically, anatomy has been taught through textbooks and cadaver dissection. Although a valuable tool, cadaver dissection has been criticized for its cost, limited availability, lack of portability, no patient-specific anatomy, health risks (such as disease transmission), and because of cultural and ethical concerns.4–9 A high-fidelity patient-specific medical model holds much of the same experience and knowledge, without the ethical and practical concerns and without disadvantaging students.
Current medical modeling applications
A plethora of literature suggests that high-fidelity medical modeling using additive manufacturing (“AM”) techniques provides ample benefits for surgical simulation, preoperative planning, doctor–patient communication, product testing, didactic instruction, prosthesis, or biomechanical research purposes. 7 Three-dimensional printed medical models are often used to provide a complimentary educational experience to cadaveric dissection. High-fidelity medical models have considerable potential to serve as a valuable tool for clinicians, surgeons, and medical students, eventually being an “essential component” in surgical training programs and a “prerequisite requirement for performing procedures on live patients.”10(p10)
Three-dimensional printed models produced from patient-specific biomedical imaging data is a process referred to as medical modeling. Additively manufactured medical models allow for the repeated replication of tangible patient-specific anatomical geometries, tailoring to the full variation of the human body and individual patient circumstances. 11
Application and fidelity
The use of 3D printing has a growing importance in the medical industry, with studies quantifying the value of medical models in health care environments. For example, using medical models during the doctor–patient consultation process before surgery was associated with higher patient satisfaction, involvement, and reassurance.12–14 Three-dimensional printed models used to communicate anatomy and physiology, illness characteristics, surgical procedures, and surgical risks to a patient before surgery were associated with better patient comprehension for informed decision making during the consultation process.12–14 Another study suggested that students who learnt anatomy on a synthetic model retained more correct information about anatomy compared with students who learnt anatomy on cadaveric material. 6
Three-dimensional printed medical models are also used to test medical devices both inside and outside the body. Testing devices and tools on medical models means that device limitations, failures, and successes can be identified and solved before clinical trials begin, decreasing overall expenses and safety threats for patients. 15 The production of patient-specific biomedical devices, including implants and prosthetics, can be custom-made for each patient.16–18
Medical models have been utilized to teach medical skills to improve technical skill competency in areas such as such as suturing, phlebotomy, hardware sizing, placement and intubation, allowing medical students to practice and learn from their mistakes without risking patient safety and increasing procedure risk.19,20 Operating strategy can be determined before surgery in complex patient cases where relationships between anatomical features are hard to visualize through virtual mediums.21–23
Surgical simulation with high-fidelity medical models has come to the foreground as a method of practicing, preparing, and teaching surgical procedures. High-fidelity simulation models can immerse a trainee into a realistic and hands-on training situation, allowing trainees to practice in a safe environment while receiving valuable feedback, decreasing patient risk and overall operating time and cost.7,24–27
Studies have indicated that pediatric and perinatal acute care may benefit from simulators, especially in the areas of surgical models for trainee education, open surgery, and planning.28–30 Adequate training can help mitigate risks associated with complex pediatric intervention contributing to the success of a procedure, improving surgical and life quality. 29 Pediatric and neonatal surgery are fields with limited access to high-fidelity simulation tools that accurately reflect individual neonatal and pediatric anatomy.28,31 This could be due to factors such as limited availability of pediatric cadavers donated to medical research and accommodating for different stages of infant growth. 8
The available medical models are of low fidelity and the materials do not reflect the complexities and intricacies of pediatric anatomy—confusing even experienced surgeons and clinicians.30,31 Since the inception of 3D printing in the 1980s, computer automated design (“CAD”) software and 3D printers have been designed and developed to produce mechanical prototypes, benefiting industries such as aerospace, automotive, military, and architecture.32,33 Despite the wealth of different 3D printing techniques and 3D printers, there has been limited research into developing 3D printing workflows to suit the cellular and anisotropic makeup of the human body.
Current medical modeling workflows
Literature suggests that current medical modeling workflows are limited as shape specification is inherently linked with one material quality—limiting the production of material gradients.34,35 Mesh-based 3D printing workflows borrowed from industrial applications are inapt for 3D printing complex material topologies (such as human tissue) and production methods currently overlook the design potential of heterogeneous material distributions.34,36–39
Current limiting factors of typical 3D printed medical models include the lack of soft tissue realism, low-fidelity detail due to segmentation techniques, the capability of only printing with one 3D printed rigid material, and the processing time involved in traditional mesh-based segmentation methods.10,17,35 Current CAD programs accommodate traditional mesh-based segmentation manufacturing workflows, which can be time-consuming and result in anatomically inaccurate 3D prints caused by data loss, segmentation artefacts, and multiple postprocessing steps using different software packages.34–36,40
Voxel 3D printing
The ambit of 3D printing has expanded to include many different fabrication methods and 3D printer types, ranging from relatively cheap to highly sophisticated machines that can 3D print with voxels. 41 Research is currently being conducted into adapting traditional mesh-based 3D printing workflows to processes that are better suited to mimicking the fidelities of human anatomy. 34 Data-driven bitmap-based AM—also referred to in literature as voxel printing,36,39 bitmap printing,34,38 or error diffusion halftoning 42 —can translate information from various data sets into heterogeneous physical forms by translating on-screen pixels into 3D printed voxels. Each voxel is a homogenous and isotropic 27-μm material droplet.
Previous studies have shown that the GrabCAD Voxel Print Utility and multimaterial 3D printers can produce 3D prints with heterogeneous material compositions, allowing the designer to engineer object functionality into the 3D printed materials, including anisotropic, color, and density property gradients. 38 The Stratasys J850™ 3D Printer can produce smoother surfaces at higher resolutions, allowing for control over internal and external structures and every Stratasys J850 3D Printer voxel. The Stratasys J850 3D Printer is a multimaterial Polyjet 3D Printer that works by simultaneously and sequentially depositing microdroplets (voxels) of different ultraviolet (“UV”)-cured resins in 14-μm layers (in high-quality mode) or in 27-μm layers (in high mix and high-speed mode), producing 3D models with varied translucency, density, and color qualities.36,38
A bitmap-based medial modeling workflow allows translation of DICOM cross-sectional bitmap image stacks to be used as direct 3D printer inputs, rather than using mesh-based files. These images are 3D printed sequentially on top of each other at the 3D printer's native z resolution. Each image sent to a 3D printer contains a pixel matrix containing colors indicative of the native 3D printer materials (CMYK) inspired by error-diffusion algorithms from 2D printing 42 and, therefore, gradients are produced through 2D printing halftoning principles.36–39,42 Each pixel within a matrix defines the material placement and specifications of the 3D printed voxel, which are then fused together, differing in their physical and chemical properties, completely bypassing traditional mesh-based segmentation methods and file formats. 37
A limited amount of studies have explored bitmap-based 3D printing workflows for medical modeling purposes, concluding that more research should be conducted into exploring the most accurate and feasible way of converting voxel-based DICOM data into 3D printed medical models. Studies acknowledge that the strengths of bitmap-based 3D printing lie in its accuracy, limitless manufacturing possibilities, and the production of complex material combinations at a microscale.36–39,42 Bitmap-based 3D printing is currently novel and has not been explored in depth for its application in medical modeling, leaving considerable gaps in knowledge, especially regarding the ability to mimic anatomical dynamics.
Digital anisotropy is a term coined by the authors to denote the ability of the designer to strategically control the density and directionality of material substance in the generation of form. 43 Available literature has explored bitmap-based 3D printing creating gradient in color and opacities, but limited exploration has been conducted into the gradation of bitmap-based 3D printed material densities. Past bitmap-based 3D printing studies have focused on the process of converting bioimaging medical data into 3D printing files and physical models34,36 but do not address the replication of accurate anatomical color and densities. This research focused on understanding how medical imaging data could translate into a bitmap based voxel 3D printing file, producing a flexible 3D print.
Research scope
A flexible 3D print within the scope of this research is defined as a 3D print that is capable of being flexed in an attempt to mimic human biomechanics. The hierarchical, functional, and material complexities that can be attained through AM produce an unparalleled level of detail in physical objects that may begin to emulate the fidelities of human anatomy to the highest degree of realism. Neonatal simulators with higher levels of realism and physical fidelity have been shown to help advanced learners develop technical skills. 28
Simulators with functional fidelity can optimize skill transfer by suspending disbelief, helping with remaining focused and improving cognitive and psychomotor aspects of skill acquisition.24,31 Therefore, there is value in exploring a sustainable and streamlined medical modeling workflow that can create flexible patient-specific models from biomedical imaging data to a high degree of realism. Material properties created through bitmap-based 3D printing have potential to emulate bioinspired material qualities, including movement, inherent in human anatomy.
Specialists capture anatomical images using scanning modalities such as computed tomography (CT). If the distance between axial images in known, software can interpolate the distances between the cross-sectional tomographic images to create volume reconstructions with smooth surfaces, creating a voxel representation of the human body.26(p170) CT images are divided into grayscale pixel matrixes. Each shade of gray is indicative of the density of tissue at that location. Density is quantified using the Hounsfield unit (“H.U.”) scale ranging from a value of −1000 (air) to a value of +700 to +3000 (bone).44,45(p8)
A feasibility study was performed in which a representative range of material compositions and densities (Polyjet shore hardness scale) were distributed over a series of 3D printed medical imaging test and calibration phantoms to investigate if scanned materials mimic the photon attenuation properties (density) of human tissues and bone. Proof of principle of the phantom design was successfully demonstrated, VeroWhite™ showed different attenuation properties to Tango+™ and there is an obvious change in materials are they become less “dense.” 46
Owing to the gap in knowledge around neonatal anatomy and the low-fidelity physical simulators available,30,31 we present a bitmap-based 3D printing workflow to produce flexible medical models using tomographic biomedical imaging data of the neonatal lower limb. Cross-sectional images through the human body can generate 3D reconstructions of anatomy.
Materials and Methods
Methodology
The methodology is focused on developing a successful workflow for converting CT imaging data into flexible bitmap-based 3D prints of the neonatal lower limb that mimic biomechanical movement.
Three-dimensional printed neonatal lower limb tests were also conducted using traditional mesh-based STL segmentation workflows to use as a comparison with the bitmap-based 3D print process.
Medical data acquisition
The data set used in this research was an anonymized high-resolution CT scan of a 6-month-old neonate obtained under the research protocol entitled, “Clinical anatomy of the infant: Correlation with clinical landmarks using imaging, digitization and 3D modelling.”
The neonatal lower limb was selected as it includes varying tissue densities and biomechanical movements of the foot can be early indicators of conditions such as cerebral palsy and equinovarus (commonly known as “clubfoot”) which develop in neonates.47,48
Medical data processing
After acquiring a volumetric tomographic data set, the data were processed through open-sourced medical imaging software 3D Slicer software. 49 A volumetric visualization of the neonatal lower limb, where thresholding values (window/level) were used to control the appearance of the anatomical part, see Figures 1 and 2. The Gradient Anisotropic Diffusion module was utilized to reduce scan noise and eliminate unwanted scan detail. Depending on how the thresholding values have been adjusted, materials can be assigned to different grayscale ranges (“H.U.” ranges). These grayscale values were assigned with the native Stratasys J850 3D Printer materials. For example, the lowest H.U. value within the anatomical part was assigned with the RGB values indicative of the softest 3D printing material available and the highest H.U. value was assigned with the RGB values indicative of the most rigid material.

A process flow outline of a bitmap-based voxel 3D printing workflow for medical modeling applications (steps 1 and 2).

A process flow outline of a bitmap-based voxel 3D printing workflow for medical modeling applications (step 3).
By re-slicing and interpolating the data set, the volumetric visualization of the anatomical part (including the thresholding, color, and cropping adjustments) exported as a cross-sectional image stack at 0.027 mm intervals to match the Stratasys J850 3D Printer native z resolution. Owing to the feasibility of this research, 14-μm layer resolution (high quality) was out of scope and the research focused on 27-μm layers (high mix and high-speed mode).
The interpolation algorithm filled in missing scan slices using 3D Slicer's inbuilt SlicerFab Bitmap Generator module 50 to produce a cross-sectional image stack of the anatomical part.
Image processing
Automated batch processing was conducted using Adobe® Creative Cloud® Photoshop 51 to prepare the exported images for 3D printing. The images were scaled to match the Stratasys J850 3D Printer XY resolution by stretching the X-axis by 200% (600 × 300 dpi).
Two-dimensional digital halftoning principles were used to assign the 3D Printer materials to each image. The images were digitally halftoned using the 3D Printer's native materials, including VeroCyan-V™, VeroMagenta-V™, VeroYellow-V™, VeroPureWhite™, VeroBlackPlus™, VeroClear™, Vero UltraClear™, and Agilus30™ to generate a stack of bitmap images comprising a pixel matrix made up of up to six colors indicative of each material.
This was achieved by creating a GrabCAD Voxel Printing-specific custom color panel using the Color Table dialog box. The image pixels were arranged using Adobe Photoshop's inbuilt Index Colour image mode, a Local (Perceptual) palette, and an error-diffusion halftoning method (modified Floyd–Steinberg algorithm) with 30% diffusion. A stack of dithered and 8 bits per channel PNG images are exported as singular PNG images including up to six colors per materials. White pixels (with an RGB value of red = 255, green = 255, and blue = 255) are areas with no assigned material (this is filled with the automatically generated support material SUP706™).
Three-dimensional printing
The resulting tomographic image stack is processed through the GrabCAD Print software using the Voxel Print Utility feature to produce a voxel .gcvf file for 3D printing on the multimaterial polyjet Stratasys J850 3D Printer range (Stratasys, Rehovot, Israel) see Figure 3. The Stratasys J850 3D Printer simultaneously and sequentially deposits droplets (voxels) of different UV-cured resins in 27-μm layers (High Mix mode) producing 3D models with smooth gradients and varied translucency, density, and color qualities. The bitmap-based 3D printed models were produced on the Stratasys J850 3D Printer using the Voxel Print Utility feature. Six materials out of VeroCyan-V, VeroMagenta-V, VeroYellow-V, VeroPureWhite, VeroBlackPlus, VeroClear, Vero UltraClear, and Agilus30 were selected throughout the research to produce the resulting 3D prints.
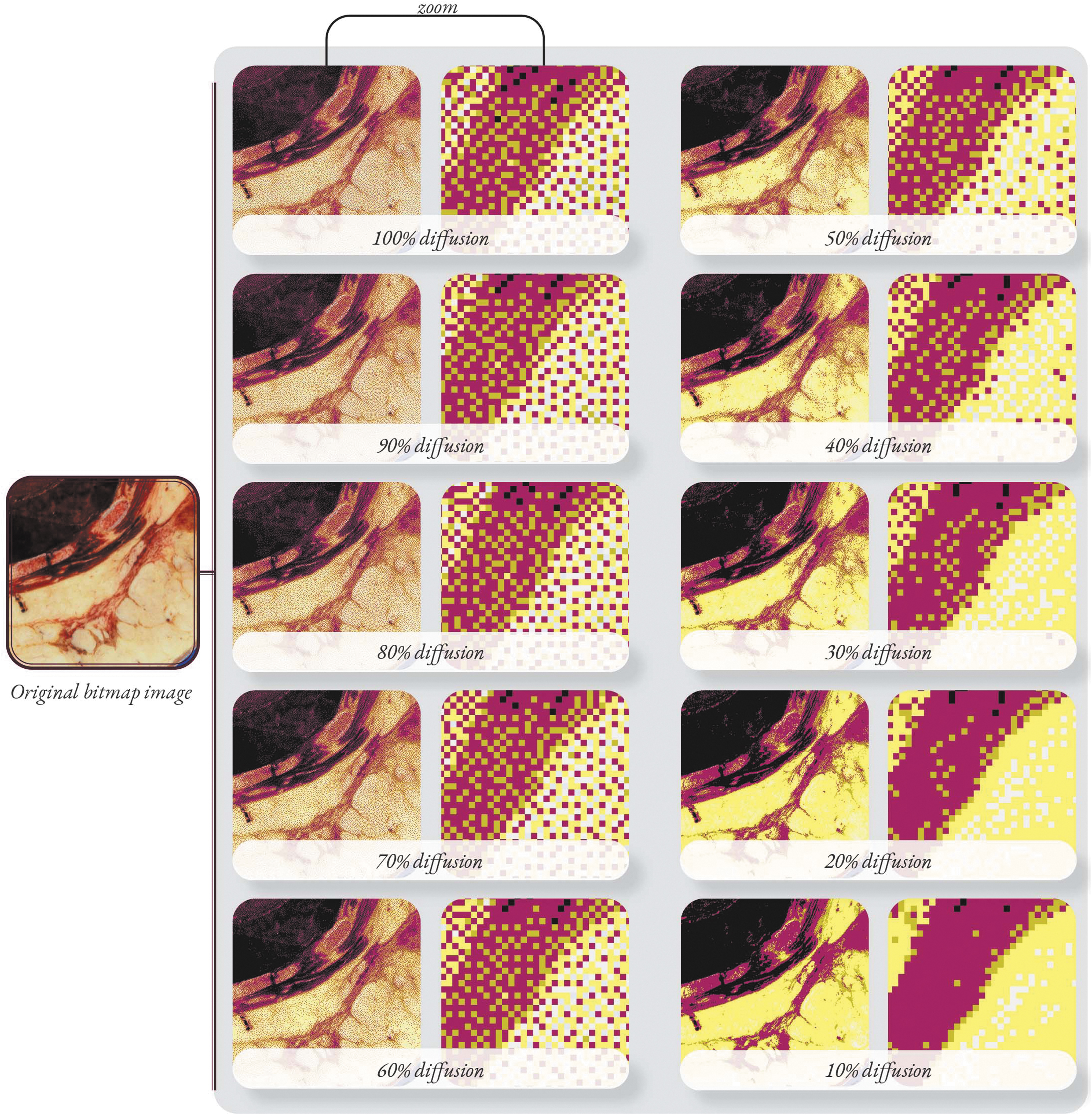
Error-diffusion halftoning using Adobe Photoshop's “Index Colour” image mode, a Local (Perceptual) palette, and a modified Floyd–Steinberg algorithm resulting in different pixel distributions (ranging from 100% to 10% diffusion of pixels).
Note: The benchmark mesh-based STL models were produced using the Stratasys J750™ Digital Anatomy™ 3D Printer with new Digital Anatomy materials, including TissueMatrix™, BoneMatrix,™ and Gel Matrix™. Currently, the commercially available Stratasys J750 Digital Anatomy 3D Printer does not include a Voxel Print Utility feature.
Results
Mesh-based medical modeling workflows have been criticized to be time-consuming, resulting in anatomically inaccurate 3D prints caused by data loss, segmentation artefacts, human error, and multiple postprocessing steps.
Mesh-based medical models include artificial boundaries between anatomical features. This means that each anatomical part that requires a different material quality must be segmented and created into a mesh-based geometry (STL file). Polyjet multimaterial 3D printing allows no geometry to overlap, meaning every mesh must be “cut out” of another to create “nestled” mesh-files. The process, referred to in many CAD programs as a Boolean function, can be a time-consuming complicated step in the modeling process, requiring large computer processing power to produce complex and detailed anatomical models with microstructures. Notably the mesh procedure fails to accommodate the material gradients that are inherently present within the human body.
Owing to the 3D printing material limitations and limited full color Agilus materials available, 3D print color and flexibility can be controlled through the assignation of appropriate halftoning diffusion percentages as displayed in Figure 3. The Diffusion percentage will control the pixel placement and the degree of interaction/mixing between Agilus and Vero materials.
Results of this study were successful in converting biomedical imaging data into 3D printed models. However, results indicated that 3D printing materials available on the Stratasys 8750 3D Printer were not soft enough to mimic anatomical density and biomechanics to the highest degree of realism based on factors such as flexion and joint articulation. Other factors that can influence the degree of 3D printing difficulty include the resolution of the biomedical imaging data and material elasticity (“softness”).
Rapid developments in the 3D printing field include the development of Stratasys J750 Digital Anatomy 3D Printer. A combination (mixing ratios) of the six materials available for 3D printing at one time on the Stratasys J750 Digital Anatomy 3D Printer can produce a range of “Digital Anatomy” materials such as the “Myocardium.” These materials used in combination have the potential to provide an unprecedented level of realism in medical models where Digital Anatomy myocardium showed promising comparisons with porcine myocardium. For compliance testing, the Digital Anatomy was either within the same range as the porcine myocardium or stiffer. 20
Figure 4 shows a coupon of swatches of all present material combinations (shore hardness scale) available for printing of J850™ 3D Printer and the Stratasys J750 Digital Anatomy 3D Printer. Interestingly, the relationship between Agilus and Vero materials is nonlinear. 46 An example of this nonlinearity is shown in Figure 4D, a voxel 3D printed swatch covering the range of Stratasys J850 shore hardness scale (blending Agilus30™ with Vero™). When Agilus30 is dispersed within a 3D print, 3D printed color fades substantially. Moreover, when Vero is combined with Agilus30, Vero works as a hardening agent and when even a small amount is added to Agilus30, the 3D print hardens. This had significance in relation to the overall study because the least dense areas of anatomy had to sacrifice color pigmentation to maintain flexibility.

Material swatches (coupons) from the Stratasys J750™ Digital Anatomy™ 3D Printer and the Stratasys J850™ 3D Printer.
To illustrate the value of bitmap-based 3D printing, this research presents two neonatal 3D printed feet created by using a single data set and two different 3D printing methods (Fig. 5). Using a bitmap-based medical modeling workflow, there was a mean reduction time of 138 min when compared with traditional mesh-based segmentation methods per model. Bypassing the traditional segmentation conversion process streamlines the medical modeling workflow, decreasing time and, subsequently, the costs associated with model production. Differences in 3D print surfaces was also observed because bitmap-based 3D printing workflows preserve the CT scan boundaries and no postprocessing smoothing of geometry occurs, unlike mesh-based medical models (Appendix Fig. A1).

Three-dimensional printed models of a neonatal foot (without fat) using the same CT bioimaging data set.
The bitmap-based 3D printed neonatal foot was produced by processing 1494 cross-sectional tomographic images into a GCVF file using the workflow presented in Figures 1 and 2. Each of these cross-sectional bitmap images comprised a pixel matrix containing 1,483,524 pixels (1,483,524 3D printed voxels) and the memory size per image was 70,128 bytes (74 KB on disk). The full 3D printed foot was constructed from 2216, 384, 856 voxels (1,483,524 pixels × 1494 images). The ability to control the placement and materials assignation of every voxel allows for higher fidelity models than mesh-based segmentation workflows (Appendix Fig. A2).
Note: All 3D prints are cleaned of SUP706 support materials using a chemical bath and manual cleaning methods.
Gradients in both color and density is impossible to achieve through mesh-based 3D printed medical models. Gradients in density, which are indicated in CT imagery by attenuation properties and, subsequently, the grayscale value and H.U. readings, can be mimicked within bitmap-based 3D printed models. By using CT imagery bitmap images to guide the material mixing ratios, the relative gradients in density can be preserved and mirrored within the 3D printed model due to the 27-μm resolution control of material mixing properties, where the lowest H.U. value is indicative of the softest polyjet 3D printing material (Agilus30) and the highest H.U. value is indicative of the hardest polyjet 3D printing material (Vero). Control over these mixing ratios meant that the relative (not absolute) grayscale value was produced from black:white pixel ratios and diffusion properties.
During the refined prototyping stage of the research, bitmap-based 3D prints were produced of the neonate's foot, knee, and hip using the same process. Sample images of these 3D prints are presented in Figures 6 and 7.

Bitmap-based voxel 3D printed neonatal knee (without fat) using 30% diffusion.

Bitmap-based voxel 3D printed neonatal foot (with fat and skin) using 30% diffusion.
A full-scale neonatal lower limb was produced using a bitmap-based medical modeling workflow. The decision was made to 3D print the neonatal lower limb without the fat and skin. The 1:1 scale flexible bitmap-based 3D printed neonatal lower limb is presented in Figure 8.

1:1 scale flexible bitmap-based 3D printed neonatal lower limb.
Discussion
These research results suggest that bitmap-based 3D printing files for medical modeling (GCVF files) require a significantly less time to generate than complex mesh-based files (STL files) due to the automated nature of the workflow and the synonymity between CT imaging data sets and bitmap-based 3D printing files. Using a bitmap-based medical modeling workflow and CT imaging data a 1:1 scale model of a neonatal lower limb was produced with integrated biomechanics. This process allows a closer emulation of anatomical qualities and in conjunction with soft materials a rudimentary dynamic model.
The results of this study build on previous literature and the body of evidence that bitmap-based 3D printing can create models with unprecedented material qualities due to the production of functional material gradients in both color and density at a 27-μm voxel resolution. Control over every 27-μm material voxel presents advantages over mesh-based medical models because models are not restricted to the assembly of mono-material geometric boundary meshes—meaning that 3D prints can integrate gradients in density, mimicking the anisotropic nature of human anatomy to a higher degree of realism.
Bitmap-based 3D printing not only bypasses the thresholding and mesh-based file production used in traditional segmentation methods, it also reduces the amount of computer processing power needed to create multimaterial 3D prints. Bypassing the traditional segmentation conversion process streamlines the medical modeling workflow decreases model production and operating time and, subsequently, the costs associated with model production and operating room time.
Time and cost reduction of bitmap-based AM workflow is primarily due to its semiautomated nature and mitigating the time constraints surrounding manual processing steps that can be influenced by human error and computer processing power. The application of artificial intelligence and machine learning has grown in virtually every discipline, including medicine.
The semiautomated production of high-fidelity medical models using a bitmap-based AM workflow means that highly realistic models can be produced at a quicker rate than mesh-based models. This opens a discussion about the potential impact of bitmap-based medical modeling workflows to create models for simulation, informed decision making, and preoperative planning applications, including the potential for pediatric education and patient-specific cases.
Software designed to accommodate a bitmap-based medical modeling workflow would advance the efficiency of bitmap-based modeling.
Conclusion
Physical patient-specific models have considerable potential to overcome cultural and language barriers, as well as helping patients with deficiencies in hearing and sight to understand a diagnosis. This may democratize important information about patient-specific health that cannot always be understood through 2D or virtual forms of medical communication.
Study limitations and recommendations
It was beyond the scope of the research to quantify the value of the results and the complete accuracy of 3D printed density gradients in a clinical research setting. Material qualities, including density gradients, should be evaluated in a clinical setting to quantify their likeness to human anatomy. To quantify the value of a bitmap-based AM workflow to produce medical models with integrated biomechanics, research should be conducted into the validity, efficiency, and accuracy of this technique for reproducing movement. This would include understanding shrinkage and expansion allowances required for voxel 3D printing.
Further research could address this concern by conducting a time-based shrinkage/expansion study to understand if there is a statistically significant shift in dimensional measurements for a set period of time. If the shrinkage/expansion is statistically significant relative to the anatomical specification (biomedical imaging dimensions), it is recommended that researchers derive process limits (scale the 3D model up or down) to accommodate for the dimensional shift over time.
Further research could test bitmap-based medical modeling using the Stratasys J850 Digital Anatomy 3D Printer and the newly available anatomical materials, and could consider the potential of creating bespoke materials for medical modeling.
Footnotes
Acknowledgments
The authors are very grateful to the following who critically reviewed the study proposal and provided advisory support: Ross Stevens and Professor Simon Fraser of Victoria University of Wellington; Dr Merryn Tawhai, FRSNZ, Deputy Director Auckland Bioengineering Institute and Dr Alys Clark, Associate Director Postgraduate, Auckland Bioengineering Institute, The University of Auckland.
Note: This article is based on Morris' (author) thesis submitted in partial fulfilment of the requirements for Master of Design Innovation at the School of Design Innovation, Victoria University of Wellington. 1
Ethical Approval
Ethics approval for use of data was granted through Dr. Ali Mirjalili (Senior Lecturer at the University of Auckland, New Zealand).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors wish to acknowledge funding support from the The MedTech Centre of Research Excellence New Zealand and the Tertiary Education Commission of New Zealand (Grant 1032-70996).