
Abstract
Objective:
Unilateral nostril breathing (UNB) is a yogic pranayama technique that has been shown to improve verbal and spatial cognition in neurologically intact individuals. Early study of UNB in healthy individuals has shown benefits for attention and memory. This preliminary study explored whether UNB influenced various measures of attention, language, spatial abilities, depression, and anxiety in post-stroke individuals, both with and without aphasia.
Design:
A within-subjects repeated-measures design was used to determine whether UNB improved cognitive, linguistic, and affect variables in post-stroke individuals. Within-subjects comparisons determined UNB's effects over time, and between-subjects comparison was used to determine whether changes in these variables differed between post-stroke individuals with and without aphasia.
Setting:
Athens and Atlanta, Georgia.
Participants:
Eleven post-stroke individuals participated in a 10-week UNB program. Five individuals had stroke-induced left hemisphere damage with no diagnosis of aphasia (left hemisphere damage control group; LHD), and six individuals experienced left hemisphere damage with a diagnosis of aphasia (individuals with aphasia group; IWA).
Measures:
Individuals were assessed on measures of attention, language, spatial abilities, depression, and anxiety before, during, and after UNB treatment.
Results:
UNB significantly decreased levels of anxiety for individuals in both groups. Performance on language measures increased for the individuals with aphasia.
Conclusions:
Significant findings for language and affect measures indicate that further investigation regarding duration of UNB treatment and use of UNB treatment alongside traditional speech-language therapy in post-stroke individuals is warranted.
Introduction
A
The increase in stroke survival rates and the healthcare costs incurred during rehabilitation highlight the need for low-cost interventions for stroke-related cognitive and linguistic deficits, depression, and anxiety. To combat rising healthcare costs, complementary and alternative therapies are low-cost techniques that can be used as adjunct interventions. Certain approaches improve mood 5 and cognition 6,7 and may be implemented as adjunct treatments without the need for additional healthcare and/or disability costs. One approach that may be a beneficial adjunct treatment for post-stroke individuals is unilateral nostril breathing (UNB).
UNB is a type of pranayama, a group of breathing practices described in ancient texts of yoga. 7 –9 The practice of UNB requires an individual to occlude one nostril while inhaling and exhaling through the other. Through controlling that which is involuntary, the ancient texts argue that mental activity and prana (life force or vital energy) can be balanced. 8,9 For centuries, people have used controlled pranayama as a way to control or change prana. 7,8,10 In addition to potentially influencing prana, controlled yogic breathing has been found to positively alter physiology, mood, and cognition, 6,7,11 –13 and thus has been studied for its therapeutic benefits. Yogic breathing has been used as an adjunct treatment for clinical disorders, such as stress, anxiety, depression, asthma, and heart rate variability. 7,14,15
Although there is evidence that pranayama can help other clinical disorders, empirical evidence in aphasia is limited. 16 –19 There are several potential theories as to how UNB may benefit individuals with aphasia (IWA). For example, UNB has been linked to improvements in verbal and spatial abilities, cognition, and autonomic nervous system functioning. 11,12,20 –22 Previous research findings indicate UNB produces differences in cerebral hemisphere dominance and that the voluntary control of breathing patterns in practices such as UNB can influence neural activity. Werntz et al. 22 found that UNB alters electroencephalographic (EEG) amplitudes in the brain's hemispheres. Cycles of nasal dominance occur naturally, and EEG activity is greater in the hemisphere contralateral to the dominant nostril. 22 This naturally occurring dominance has been found to be related to verbal or spatial abilities, with unobstructed nasal dominance linked to cognitive performance in the contralateral hemisphere. 23 Further research supports that EEG activity and hemispheric dominance shift contralaterally with changes in nasal dominance, 13 and changes in hemispheric dominance can be induced when an individual engages in UNB. 22 These changes in hemisphere dominance may improve spatial memory, problem-solving skills, and emotions. 11,12,22
Others have found support for this idea of increased EEG activity over contralateral hemispheres demonstrated by changes in behavioral performance after UNB practice. For example, increased spatial memory has been observed in non–brain-damaged individuals after left UNB. 11,22,24 Changes in verbal skills have not consistently demonstrated significant change, which potentially could be due to the measures used in previous studies. 20,21,25,26 If hemispheric dominance is altered through UNB, as suggested by Werntz et al., 22 and this in turn alters behavior, 11,22,24 this particular pranayama practice may help strengthen the function of the damaged hemisphere following stroke.
Although UNB may lead to both cognitive and neural changes, the mechanism of action is not clear. One potential explanation is that behavioral changes could be linked to the physiologic alterations associated with breath and its control of the autonomic nervous system. Breathing is voluntarily and involuntarily regulated by an intricate feedback system composed of autonomic visceral networks, brain stem nuclei, the limbic system, cortical areas, and the neuroendocrine system. 6,7 The voluntary control of breathing patterns is argued to influence autonomic nervous system functions, including heart rate variability, expiratory rate, and cardiac vagal tone. 14,27 –29 For example, a study found that after 3 months of slow-breathing pranayama, individuals had significantly improved heart rate response to standing (a measure of autonomic system function) as well as decreased basal heart rate (a parasympathetic measure). 30 Similar changes were not observed for individuals who completed fast-breathing pranayama; this finding therefore suggests that it is not only the control of the breath that is important but also the way in which it is controlled. The slow-breathing practice of right UNB in healthy individuals significantly increased systolic blood pressure and increased oxygen consumption, which may be beneficial for individuals following a stroke. 31 However, findings in the literature are inconsistent regarding autonomic functions. 26
Breathing patterns may also influence emotional regulation, which may benefit those with post-stroke depression. Brown and Gerbarg described UNB as a way to reduce the effects of psychological and stress-related disorders in an imbalanced autonomic system. 6,7 Brown and Gerbarg 6 argued for a final effect on the peripheral nervous system beginning at the stretch receptors in the respiratory system, activating the vagal system, ultimately sending information to the brainstem and higher-level central nervous system structures. These inputs into the brain are thought to influence various areas, such as mood, cognition, and behavior. 6,7 It has been argued that through regulating movement of the respiratory system, the autonomic nervous system can be modified, 8 and that increased parasympathetic activity can lead to cognitive change. 32
Decreased stress and anxiety (increased parasympathetic activity) may also increase the available cognitive processing space available for language. 33 The reduction in negative emotions (i.e., anxiety, frustration, and tension) could increase resource allocation for language processing, subsequently increasing performance on linguistic tasks. 17 For example, Cahana-Amitay et al. 34 presented the concept of “linguistic anxiety” for adults with aphasia. Research in aphasia has suggested that language tasks produce additional stress for adults with aphasia. 35 If stress affects cognitive and linguistic function for individuals with aphasia 17, 33 and UNB increases activity of the parasympathetic system, 36 it is also possible that UNB could affect cognitive and linguistic performance through a reduction in stress or linguistic anxiety.
UNB could potentially influence language performance for adults with aphasia, given the possible mechanisms it may affect. It has been suggested that attention and memory are important for linguistic performance for adults with aphasia. 37 –39 Furthermore, preliminary findings indicate that UNB may improve the linguistic abilities and attention that supports linguistic processing. 19,40 Pilot data presented by Marshall and Panico 40 found that UNB increased fluency and attention and decreased mood and anxiety in healthy individuals. Individuals completed a 10-week UNB instruction with significant improvements on the Beck Depression Inventory-2, Beck Anxiety Inventory, Controlled Oral Word Association Test (verbal fluency), and Conner's Continuous Performance Task-II (attention). Therefore, UNB may be a viable adjunct treatment option for improving linguistic and attention skills in those with aphasia. Alterations observed in other studies regarding hemispheric EEG patterns, hemispheric dominance, changes in systolic blood pressure, increased oxygen consumption, decreased depression, decreased stress, and increased attention following UNB suggest potential benefits for adults with aphasia. 13,19,22,31,36, 40, 41
It was hypothesized that UNB would improve attention and language as well as decrease anxiety and depression. Changes in attention would be expected because of the focused attention component of UNB, given previous literature that has specifically reported changes in hemisphericity. 22 It could be argued that UNB would also decrease anxiety and therefore increase an individual's attention abilities; language would therefore benefit from the increased ability to attend. 17,39 Spatial abilities were not hypothesized to increase, as previous research indicated that left UNB alters spatial abilities and right UNB was conducted in this study. Furthermore, depression is common after stroke, 2 and because of the language loss experienced in aphasia, IWA are at an increased risk for depression. 42 Pranayama has demonstrated alterations in depression and anxiety in various populations. 43 It was hypothesized that as a result of the guided nature, a majority of benefits would be observed during the initial training period, with maintenance and potential continued improvement as a result of extended practice.
Methods and Materials
Experimental design
A within-subjects repeated-measures design was used to study the effects of UNB on attention, language, spatial abilities, depression, and anxiety in IWA and individuals with left hemisphere damage without aphasia (LHD). A within-subjects repeated-measures design with appropriate correlation structures allowed for observation of UNB's effects over time, while between-subjects comparisons allowed for comparisons between the IWA and LHD groups. All research procedures were approved by the University of Georgia Institutional Review Board, Athens, Georgia.
Participants
Eleven individuals with brain damage age 31–74 years were recruited for this study. Six of these individuals received a diagnosis of aphasia by a certified speech-language pathologist. The remaining five individuals experienced left hemisphere stroke but did not have co-occurring aphasia (LHD group). Nine of the individuals were male (five IWA and four with LHD). All participants were native English speakers. Mean ages were 58.2 years for the IWA group and 52.4 years for the LHD group. All participants consented to participate in the study. Participants with aphasia were administered the Aphasia Diagnostic Profiles (ADP) 44 to determine the type and severity of aphasia, as well as to obtain repeated measures of these participants' language abilities over the course of treatment. Table 1 summarizes participant characteristics.
A, individual with aphasia group; L, left hemisphere damage group; NA, not applicable; TPO, time post onset; ADP, Aphasia Diagnostic Profiles.
Procedures
Participants were assessed for baseline performance before beginning the UNB instruction program. The 10-week program was divided into a 4-week guided instruction and practice followed by 6 weeks of individual UNB practice on the basis of findings of physiologic changes after 4 weeks of UNB. 31,45 Much of the UNB literature concerning healthy populations used a single training session (ranging from 5 to 40 minutes 22,46 ) with a few exceptions of extended trainings (10 days 11 and 15 days 30,47 ). During the first phase, individuals met in a group for 1 hour once per week to receive UNB instruction. Individuals were instructed to practice UNB 6 of 7 days per week, beginning with 5 minutes of practice and working up to 40 minutes.
UNB training sessions began with 1–2 minutes of three-part breathing as led by the instructor, which then led to guided UNB. For UNB, the participant was asked to close the left nostril using whichever hand was unaffected by the stroke or was more comfortable. Participants were encouraged to work toward extending the exhalation to twice as long as the inhalation, with a ratio of 1:2. All participants were judged to be able to complete the UNB practice during the initial training sessions, with no limb apraxia observed. Handouts outlining the practice and CDs with different lengths of guided UNB were provided, and adequate time was provided for questions and answers with a trained instructor.
At the end of the 4-week instruction period, participants were administered the same battery of assessments to determine whether attention, language, spatial abilities, depression, or anxiety changed during the 4-week guided breathing practice. Assessments were conducted again after the 6 weeks of independent UNB practice to determine whether change continued throughout the course of the 10 weeks. All participants reported compliance with practicing during the study.
Measures
Assessments were chosen to measure language, attention, spatial abilities, depression, and anxiety. These assessments included the Aphasia Diagnostic Profiles (ADP), the Benton Controlled Oral Word Association Test (COWAT), 48 the Revised Token Test (RTT), 49 Conners' Continuous Performance Test II (CPT), 50 the Benton Judgment of Line Orientation Test (BJLOT), 51 the Beck Depression Inventory (BDI-II), 52 and the Beck Anxiety Inventory (BAI). 53
Three measures of language were used: ADP, RTT, and COWAT. The ADP assesses language abilities among aphasic patients and was used as an overall measure of language for the IWA group. It has nine subtests to provide information regarding the type and severity of aphasia as well as information on the modality of communication. The RTT assesses deficits in auditory processing of individuals with aphasia, brain injury, and various language and learning disabilities. This sensitive and descriptive assessment includes 10 subtests that incorporate tasks using colored token pieces to assess auditory comprehension. The COWAT assesses verbal fluency in individuals with brain damage by requiring participants to verbally produce as many words beginning with F, A, and S as they can in 3 minutes. The CPT is a computerized assessment designed to assess attention, inhibition, and impulsivity. Participants are required to press the space bar for every letter shown on a computer monitor except X. It has been normed on both healthy and neurologic populations and has the ability to detect clinical attention problems. The BJLOT is a standardized nonverbal assessment of spatial orientation and perception in which an individual judges whether lines are at similar orientations. The BDI-II and BAI are both self-report forms used to assess depression and anxiety, respectively. The BDI-II is a clinically sensitive test that detects the presence and severity of depression. The BAI can differentiate between anxious and nonanxious groups. Both the BDI and the BAI were read to or with patients, using any compensatory methods necessary in order to maximize understanding.
Data analysis
Repeated-measures analyses of variance were conducted using SAS 9.3 software (SAS, Cary, NC) to determine if UNB instruction improved affect, attention, spatial orientation, and language abilities in the IWA and LHD groups and if changes for the two groups were similar. Correlation structures, typically compound symmetry or unstructured correlation, were used because exploratory analyses indicated they were necessary; several measurements were natural log transformed to meet the normal distribution assumption of the tests.
Results
Repeated-measures analyses of variance were used to determine the effect that UNB training had on each of the cognitive and affect variables for each group. Both groups were assessed with the CPT, BAI, BDI-II, COWAT, BJLOT, and the RTT. Table 2 summarizes the statistical significance for each of these test measures. Significance is recorded for the time of the measurement (baseline, 4-week, and 10-week measurements), the group, and the interaction of time and group (whether the changes over time were different for the IWA and LHD groups).
Average scores for each assessment at each time point, including significant effects.
Significant at 0.05 level.
Significant at 0.01 level.
Significant at 0.001 level.
BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; BJLOT, Benton Judgment of Line Orientation; COWA, Controlled Oral Word Association; CPT, Continuous Performance Test; LFD, left hemisphere damage; Hit RT, the mean response time for all target responses; ISI, Interstimulus Interval; IWA, individual with aphasia; RT, reaction time; RTTAV, revised token test average.
Significant results from the CPT measurements included log-transformed hit reaction time standard error (the IWA were found to have greater variability in hit reaction time; mean difference [MD]=0.3240, p=0.0048), log-transformed percentage omissions (the IWA were found to have more omissions than the LHD group; MD=0.5149, p=0.0225), and variability of hit reaction time standard error. This last measure was significantly greater for the IWA (MD=20.9623, p=0.0043), and particular to the UNB practice, both groups decreased from the baseline measurement to the 4-week measurement (MD=11.5348, Tukey HSD P=0.0063).
Log-transformed BAI scores indicated that for both groups, anxiety was less after 4 weeks of guided practice than at baseline (MD=0.6996, Tukey honestly significant difference test [HSD], p=0.0069). The average score of all participants (in original scale) at baseline was 10.5, and the average score after 4 weeks was 6.1. There was no interaction of group and time, indicating that this change is statistically similar for both groups. After 6 weeks of independent practice, the average BAI score for all participants was 6.9, which was not significantly different from either the baseline or the 4-week measurement. Figure 1 shows changes in BAI scores for both groups over the course of the study. For the BDI, there were no significant differences between the two groups of individuals or over the course of the breathing practice (Figure 2).
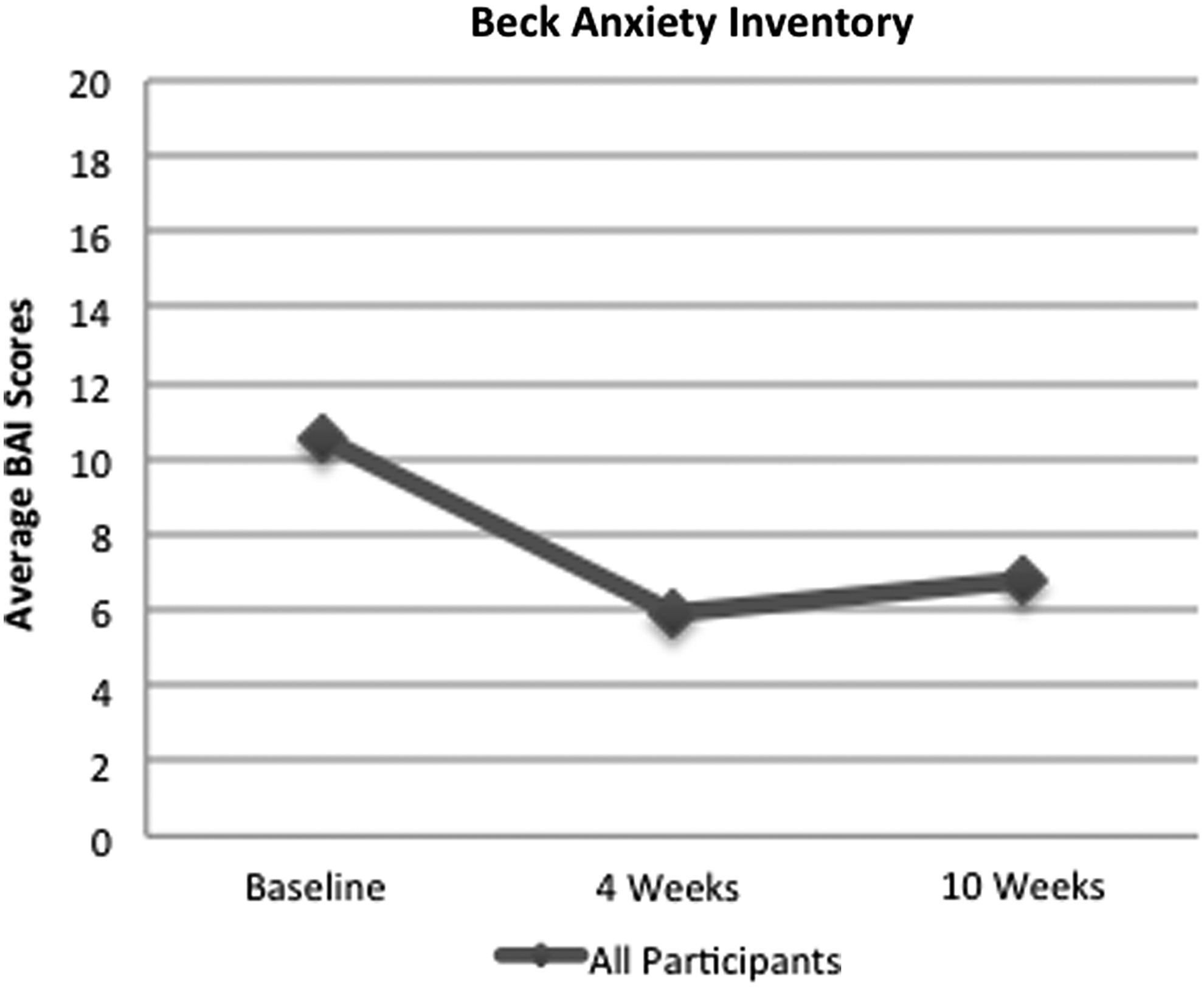
Average scores on the Beck Anxiety Inventory (BAI) for all participants.

Average scores on the Beck Depression Inventory (BDI) for all participants.
An analysis of COWAT scores indicated that overall, the individuals with LHD had significantly higher scores than the IWA (MD=8.7356, p=0.0003). The average score of the individuals with LHD over the course of the breathing practice was 13.1060, and the average score for the IWA group was 4.3704. This indicates the level of language loss typical with individuals with aphasia. There was a significant interaction of group and time; Tukey HSD comparisons indicate a significant increase in COWAT scores from the baseline to the end of the 10-week study for the individuals with LHD only (MD=1.2558, p=0.0001). Figure 3 shows changes in COWAT scores for both groups.
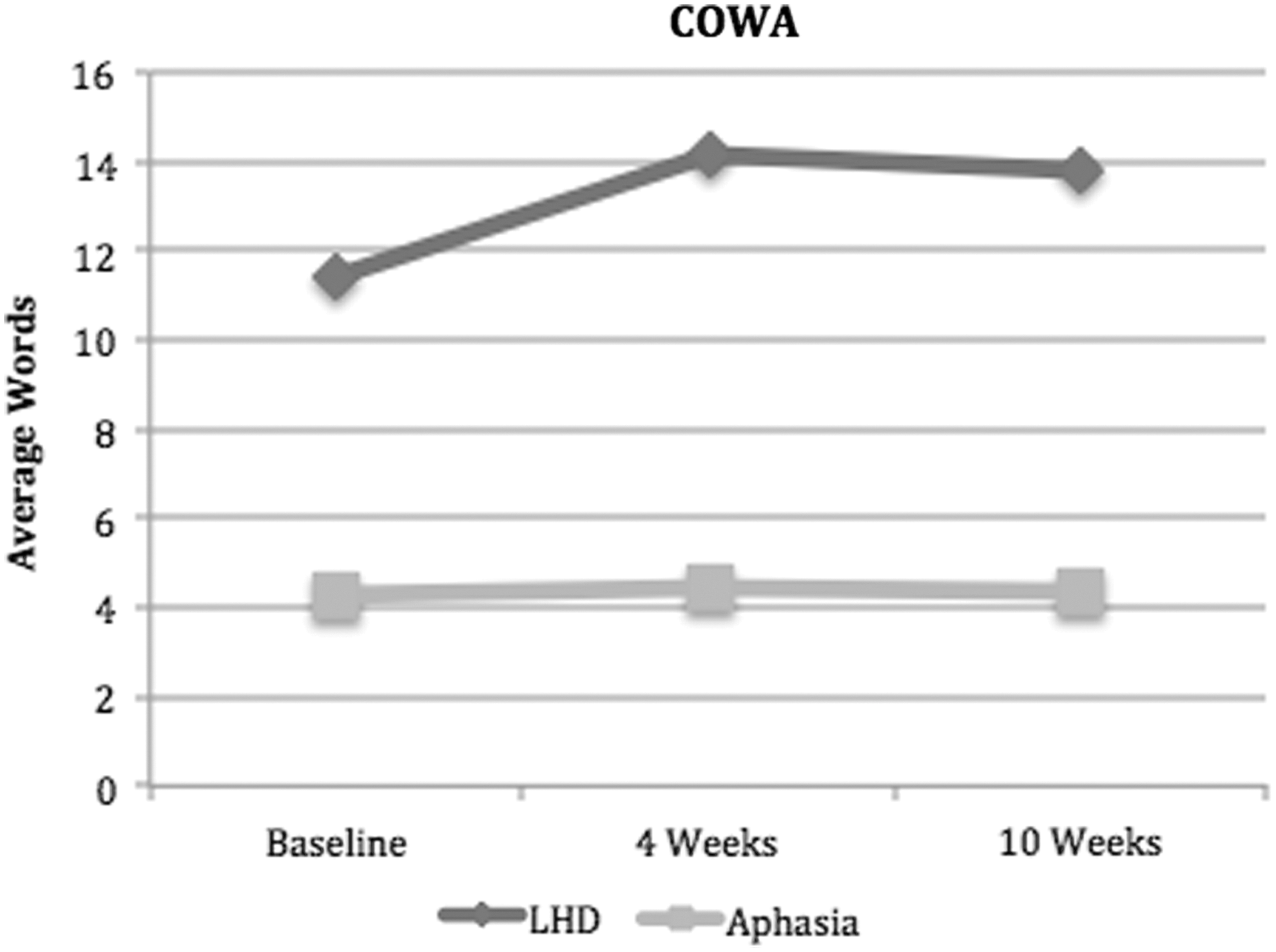
Average scores on the Benton Controlled Oral Word Association (COWA) Test for all participants.
Of the two other measures taken on all participants (BJLOT and RTT), neither the LHD group nor the IWA group showed significant changes over the course of the study. BJLOT scores were significantly higher on average for the LHD group than the IWA group (MD=8.3222, p=0.0370), as were average RTT scores (MD=1.9390, p=0.0088).
The ADP was administered only to individuals with aphasia. Table 3 summarizes statistical significance among the ADP measures. The following ADP subtests demonstrated significant positive changes from baseline to the measurement after 4 weeks of guided practice: lexical retrieval, alternative communication, personal information, information units, phrase length, and ADP severity. Scores that were found to be significantly higher after the 4-week guided practice tended to decrease somewhat during the 6-week independent breathing practice (Figures 4 –10), indicating that improvements in language abilities did not remain significantly greater than baseline through the 6 weeks of independent breathing practice. No effect of UNB treatment was found to last through week 10 of the study, with the exception of the Gestures subtest.
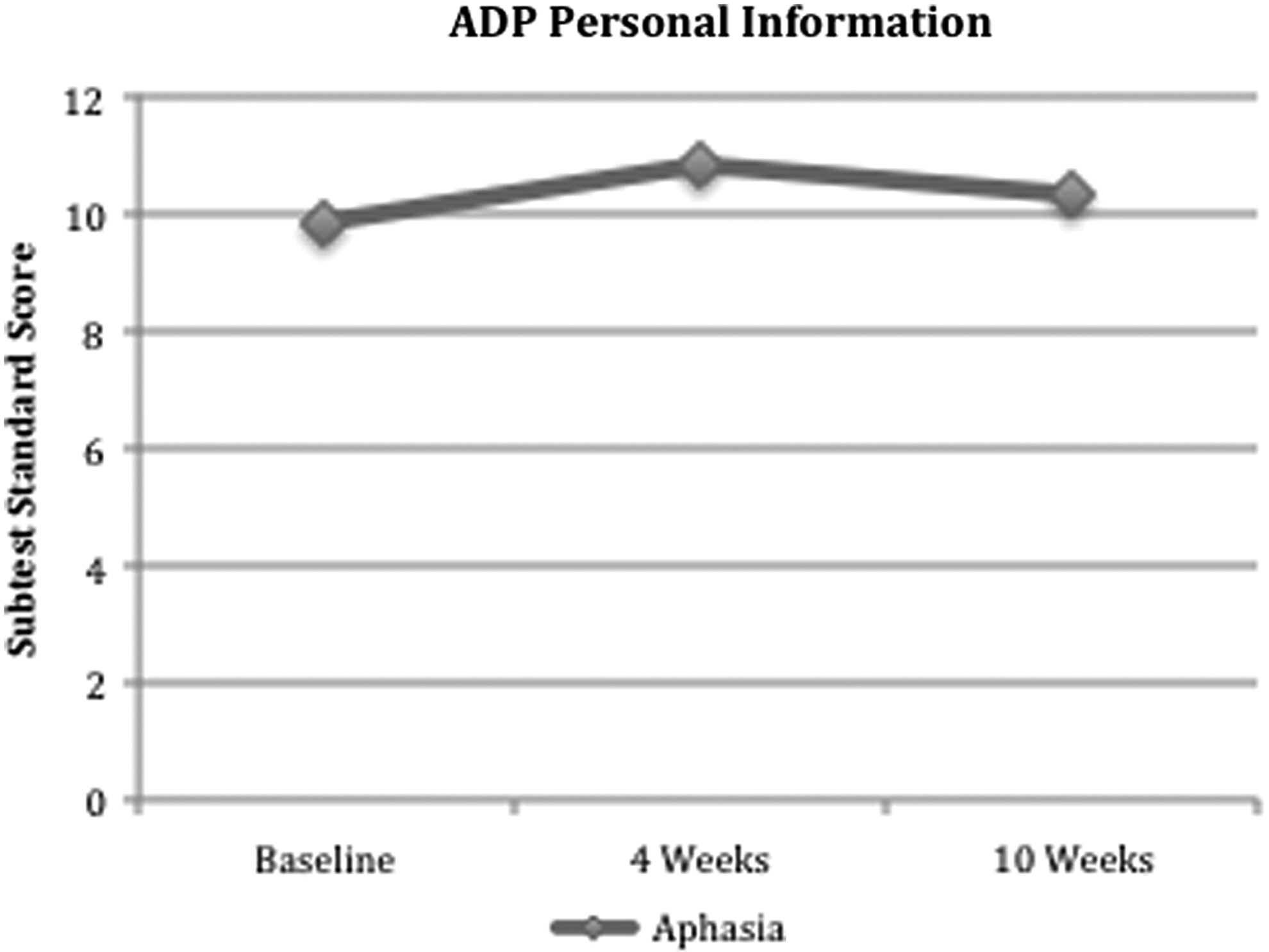
Average scores on the Personal Information subtest of the Aphasia Diagnostic Profiles (ADP) for individuals with aphasia.

Average Lexical Retrieval Standard Scores for individuals with aphasia.
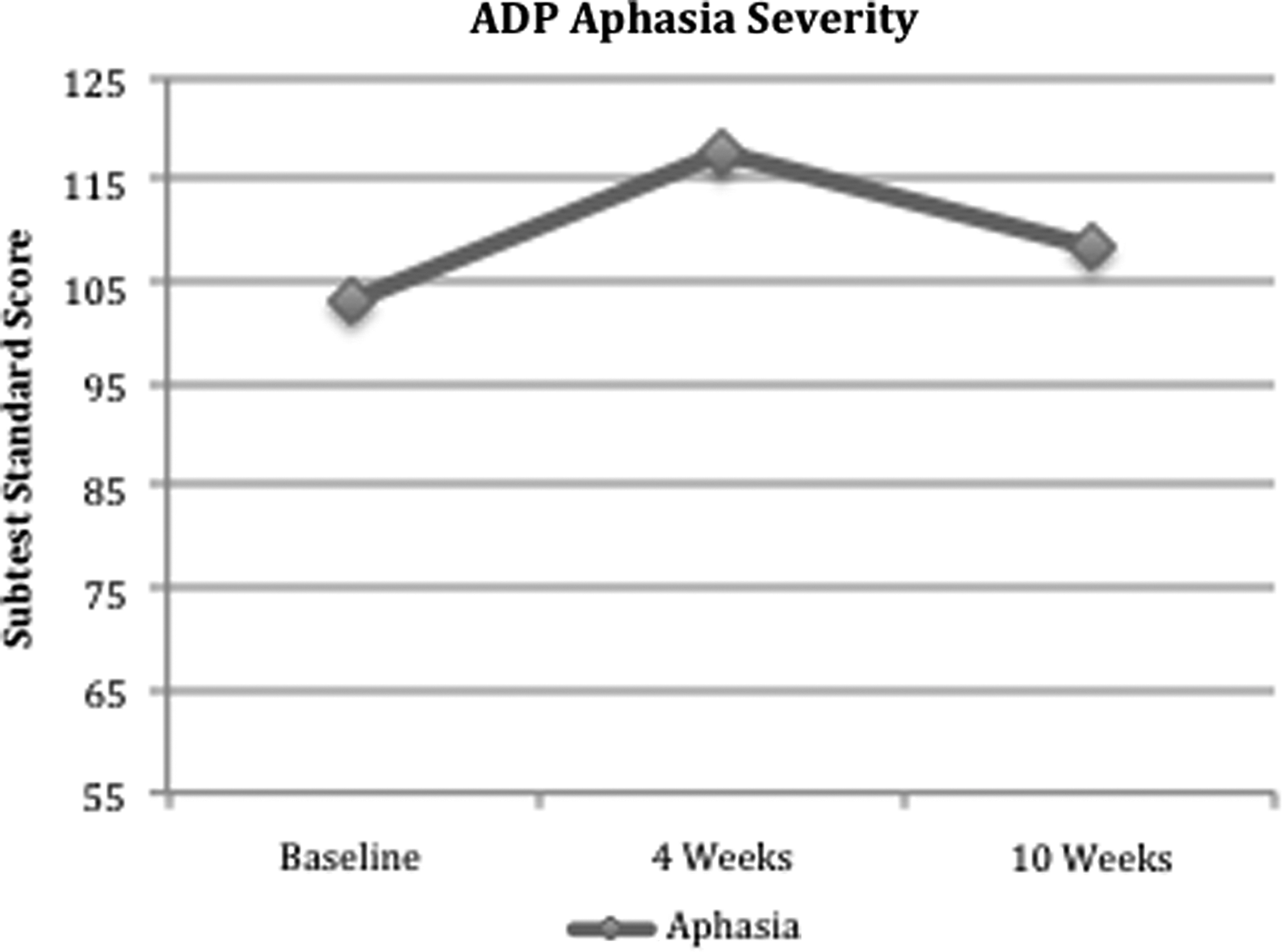
Average Aphasia Diagnostic Profiles Aphasia Severity Standard Scores for individuals with aphasia.
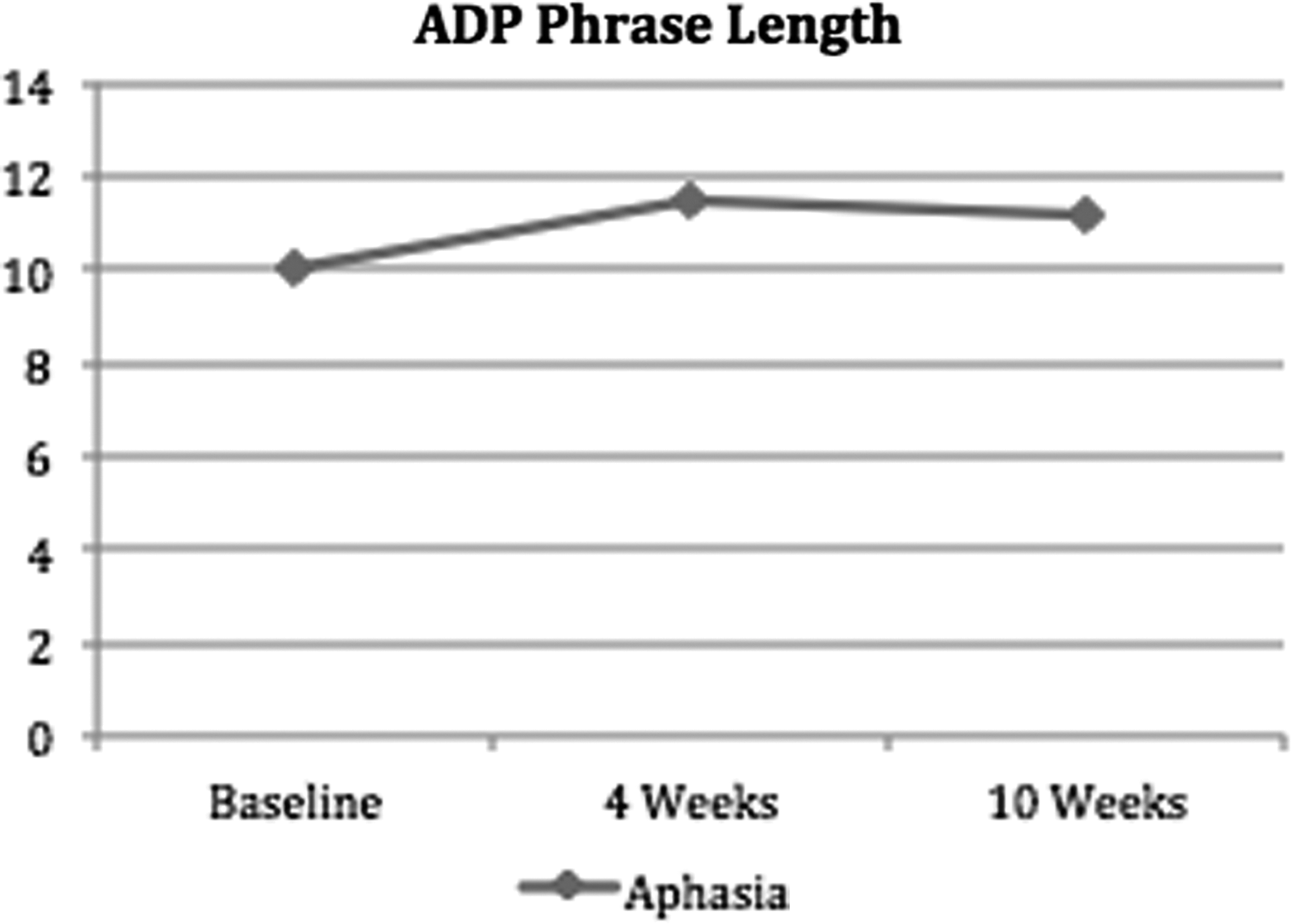
Average Aphasia Diagnostic Profiles Phrase Lengths for individuals with aphasia.
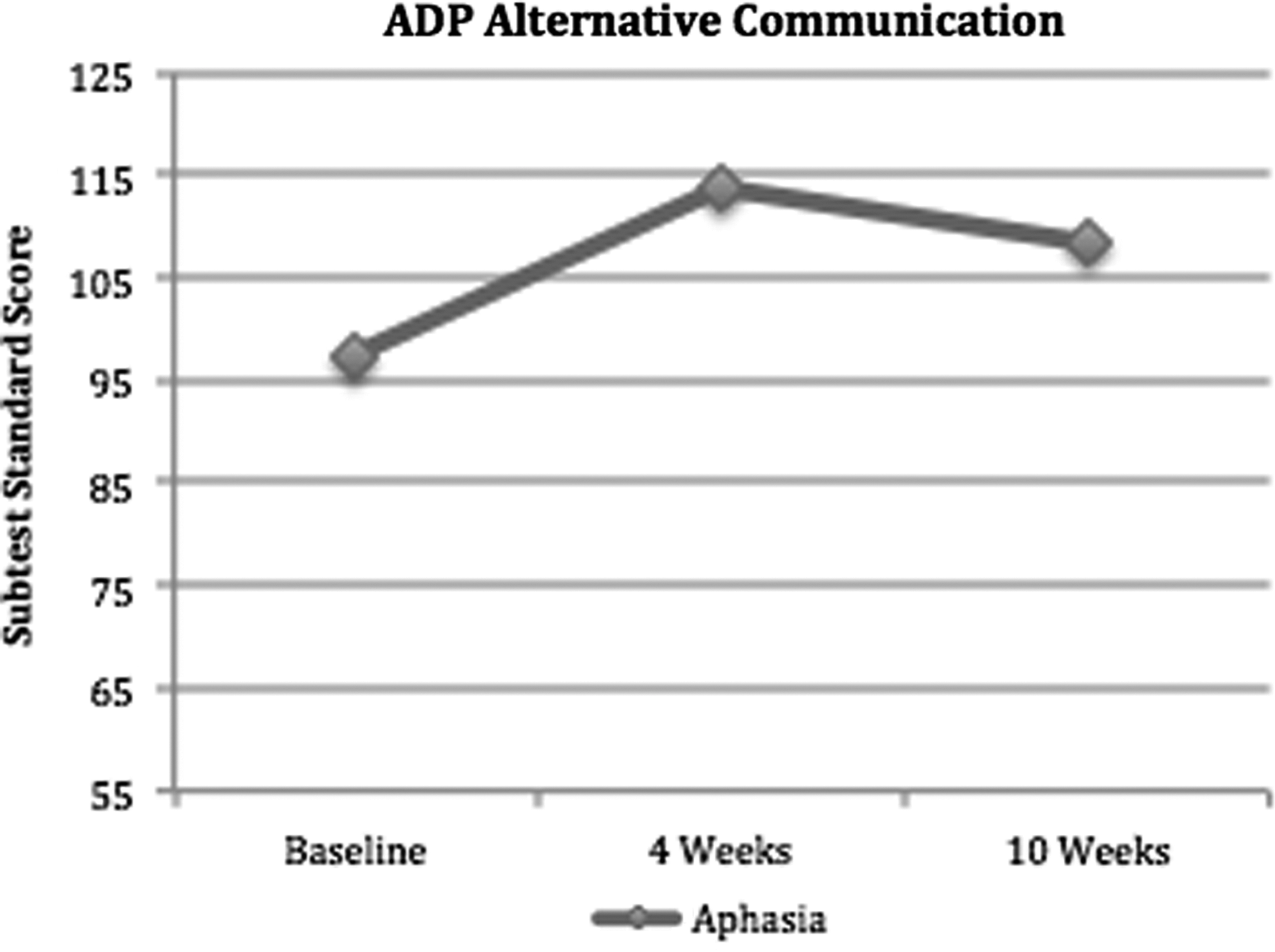
Average Alternative Communication Standard Scores for individuals with aphasia.
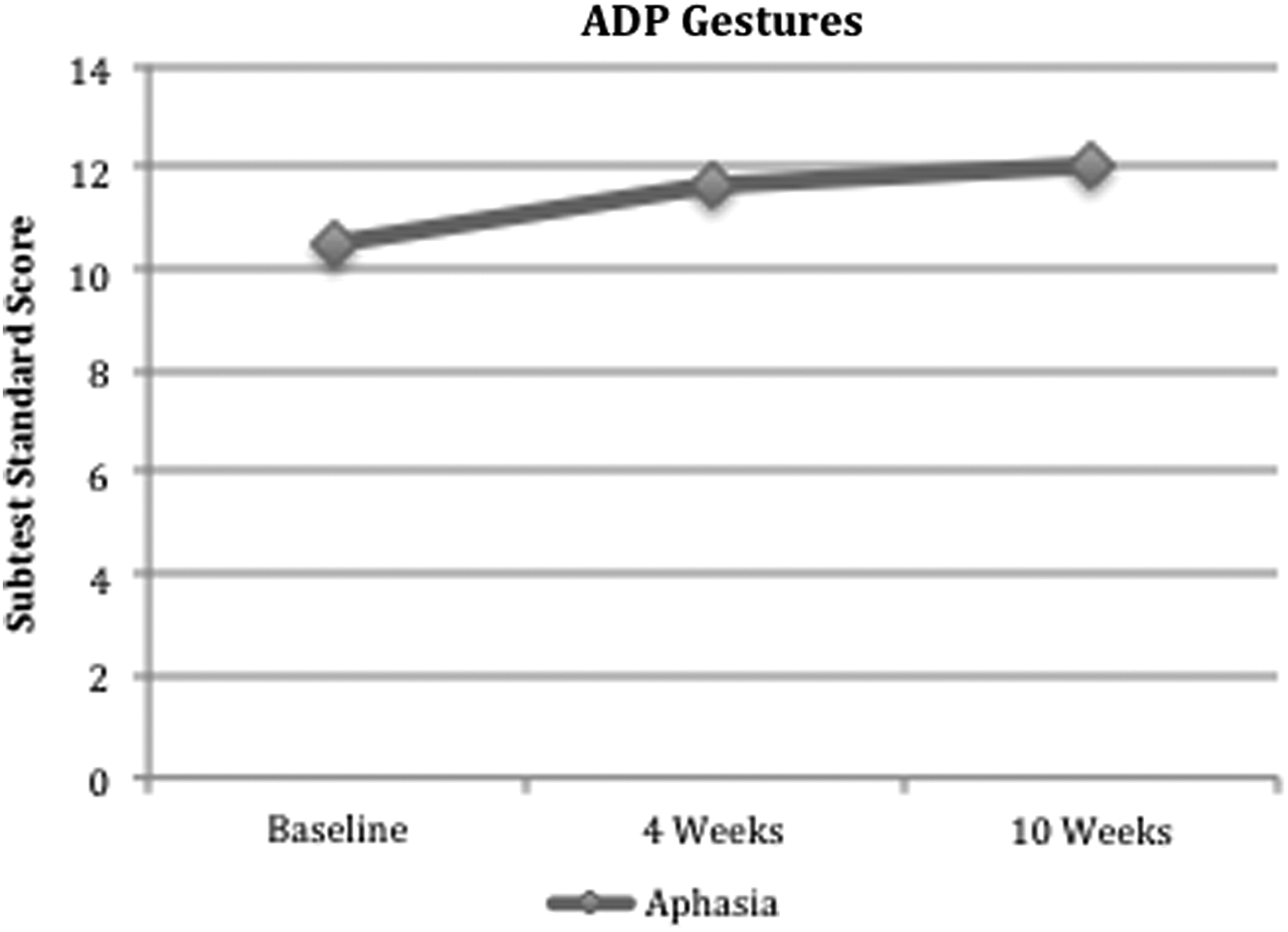
Average standard score for Gestures subtest for individuals with aphasia.

Average Aphasia Diagnostic Profiles Information Units for individuals with aphasia.
Significant at 0.05 level.
Significant at 0.01 level.
Significant at 0.001 level.
Mean Personal Information scores were 9.83 at baseline and increased to 10.83 after the 4-week guided treatment (MD=(1.0, p=0.0126). Scores did not remain significantly higher than baseline at the completion of the study, however, returning to an average of 10.33 at the completion of the study. Information Units averaged 12.33 at baseline and increased to 14.83 after 4 weeks of guided practice (MD=(2.5, p=0.049). Scores decreased to 11.83 at the completion of the study. Average Phrase Length scores were 10.0 at the beginning of the study and increased to 11.50 (standard deviation [SD], 4.3) after guided breathing practice (MD=(1.5, p=0.0298). Although scores did not significantly decrease at the completion of the study (mean,=11.17; SD,=4.4), no overall significant difference was noted in Phrase Length.
ADP Lexical Retrieval scores are a composite of the Personal Information, Information Units, and Naming scores. Mean Lexical retrieval scores were 10.33 at baseline and increased to 12.33 after the 4-week guided treatment (MD=(2, p=0.0084). At the end of the 6-week independent breathing portion of the study, lexical retrieval scores decreased significantly to 10.67, resulting in a statistically insignificant change in overall lexical retrieval abilities from baseline to week 10. A significant improvement in Information Units and Personal Information scores appears to underlie the improvement in overall Lexical Retrieval, as there was no change in Naming abilities throughout the study.
Alternative Communication scores were significantly higher after the 4-week guided practice. These scores averaged 97.5 at baseline and rose to 113.67 after the 4-week group treatment (MD=(16.17, p=0.0264). At week 10, the average Alternative Communication score decreased insignificantly from the 4-week assessments, yielding an average Alternative Communication score of 108.5 at the completion of the study. Although average Alternative Communication scores increased from baseline, this overall change was not statistically significant at the end of the 10-week program.
Aphasia Severity scores are a composite of Auditory Comprehension and Repetition abilities. There was no significant change in Auditory Comprehension or Repetition. Mean scores for Auditory Comprehension were 10.67 (standard error of the mean [SEM], 0.84) at baseline, 11.83 (SEM, 0.6) after guided treatment, and 12.33 (SEM, 1.29) at the completion of the study. Mean scores for Repetition were 9.17 (SEM, 1.47) at baseline, 9.83 (SEM, 1.83) after guided practice, and 9.83 (SEM, 2.63) at the completion of the study. Average Aphasia Severity Scores were 103 (SD,=5.329) at baseline, improved to 117.5 (SD, 15.947) after guided breathing treatment (MD=(14.5, p=.0429), and then decreased to 108.17 (SD, 9.97) at week 10.
The only ADP score to show a significant improvement from baseline to completion of the study was Gestures. Average Gesture scores were 10.5 (SEM, 0.34) at baseline, increased to 11.67 (SEM, 0.62) after guided practice, and rose to 12 (SEM, 0.37) at the completion of the study (overall MD=1.5, p=0.0026).
Overall, for both groups, performance for the BJLOT, CPT, or RTT did not significantly change during the study. However, for the LHD group, guided UNB training had a positive effect on anxiety and on COWAT scores. For the IWA group, language abilities on some of the ADP subtests and anxiety improved significantly, although these changes did not remain stable after the 4 weeks of guided breathing.
Discussion
The current study provided preliminary evidence for the benefits of UNB in a group of individuals who have experienced a stroke that may or may not have resulted in aphasia. On the basis of changes in measures of language for the individuals with aphasia (i.e., various ADP subtests), UNB may be an effective adjunct treatment strategy to use with traditional speech-language therapy. In addition, the LHD group's improvements on the COWAT scores provide further information that right UNB may improve functions of the contralateral hemisphere 54 and that verbal improvements may follow with UNB practice. 20
For both groups it appears that UNB may be a successful strategy for improving anxiety. BAI scores indicated significantly decreased levels of anxiety for both the individuals with LHD and the IWA after 4 weeks of guided practice when compared with baseline, but this was not found at the final testing after 6 weeks of independent practice. However, many of the participants in the LHD group reported that they were not as anxious, had an easier time sleeping and relaxing, and were better able to manage moods. A follow-up analysis was conducted to examine anxiety and language performance. A linear repeated measures model with unstructured covariance was used. The predictor was ADP Severity, and the response was performance on BAI. Within individuals, the BAI score tended to decrease by an average of 0.2483 point for every one-point increase in the ADP Severity score (F[1,5]=20.25, p=0.0064). This suggests that as anxiety decreases, language abilities increase in IWA, which is an interesting finding relevant to the theory of “linguistic anxiety.” 34
Attention level did not significantly change throughout the study, as measured by the CPT. Nevertheless, significant improvements in measures of anxiety (both LHD and IWA groups) and language (IWA group) indicate that changes in attention may not be contributing to the improvements observed.
Group treatments for IWA have been proven beneficial for language and psychosocial wellbeing; 55 however, the positive effects found for the language measures during the 4-week guided practice may not have been solely related to socialization in the group setting. A study by Elman and Bernstein-Ellis 56 found that IWA who engaged in social activities did not show significant improvements on language measures when compared with a group that engaged in communication treatment. Therefore, socialization in a group setting alone may not be the mechanism of change. 56 Rather, reductions in anxiety may have positively affected language abilities during the 4-week guided practice by freeing cognitive resources to allocate for language 17,33 and executive functioning. 57 For example, increased executive functioning may be responsible for improvements in ADP Gestures seen over the course of study. 58
It is also possible that the chosen assessments were not sensitive enough to detect changes that may have occurred throughout the study or that linguistic deficits precluded reliable responses from participants for some of the measures. In a review, Robinson and Spalletta 59 concluded that there is currently no reliable method of assessing depression in post-stroke individuals with comprehension deficits. Individuals with aphasia are often excluded from studies investigating post-stroke depression, 59 and in a review, Townend and colleagues found that many studies consider language-based methods of assessing depression best for individuals with mild aphasia. 60 There may also be problems with use of self-report rating scales to assess anxiety and depression in IWA (for review and discussion, see Cahana-Amitay et al. 34 ).
Although significant differences were found in this study even with the small number of participants, it is possible that a larger sample size would have allowed for additional significant findings for the measures assessed. Future studies with a greater sample size may reveal significant changes in additional variables. Further, measuring physiologic changes in addition to the behavioral changes would allow for exploration of additional potential mechanisms. It is noteworthy that improvements observed after the 4-week guided breathing practice did not remain after the full course of the 10-week breathing program. Individuals may need a longer period of guided breathing practice before practicing independently in order to continue improving affective or linguistic abilities.
Conclusion
Preliminary evidence for improved affect and language, along with participant self-report of UNB benefits, indicates that UNB may be a low-cost adjunct strategy to consider using for ameliorating certain post-stroke effects. Further research regarding a longer-duration and more focused guided UNB treatment sessions may demonstrate greater benefits for the variables measured in the current study. The use of complementary treatments has been suggested for individuals in need of post-stroke language rehabilitation, 17,18 and, therefore, future study regarding treatments such as UNB should continue for IWA.
Footnotes
Acknowledgments
Special thanks to Dr. Richard Panico and the Athens Regional Mind Body Institute for space in order to conduct this research. Additional gratitude is extended to the participants for their time and to the speech-language pathologists and graduate students who helped with recruitment, assessment, and scoring.
Disclosure Statement
No competing financial interests exist.