
Abstract
Background and Objective:
Appendicitis is the most common cause of severe abdominal pain in the world, and the associated postsurgical pain, as occurs with other surgical procedures, is one of the most common problems. Today, there is a growing tendency toward nondrug methods and alternative medicine to reduce the adverse effects of drugs. Reflexology involves applying pressure on certain areas of the palms, feet, and ears in order to reduce stress and pain in certain areas of the body. The aim of this study was to determine the effect of reflexology massage on pain relief after appendectomy.
Methods:
This clinical trial was conducted at the surgical emergency unit of Imam Reza Hospital of Mashhad, Iran, in 2013. Pain intensity and analgesic consumption were compared between 105 patients before and immediately, 1 hour, 6 hours, and 24 hours after the intervention in three groups of intervention, control, and placebo. Patients in all three groups received analgesics, as required. The experimental group received pressure on a defined area of the right foot for about 10 minutes and the Shen Men point of the ear for 1 minute. This pressure in the placebo group was applied on the left foot and the left earlobe. Patients in the control group received routine care only. The results were evaluated at a 95% confidence level, and data were analyzed using SPSS software version 12 (SPSS, Inc., Chicago, IL).
Results:
At the beginning of the study, the mean pain intensity in different groups according to analysis of variance was not significantly different (p = 0.439); however, there was a notable difference in pain intensity between the intervention and other groups after reflexology therapy. In addition, methadone consumption was significantly lower in the reflexology group than in the other two groups (p ≤ 0.001).
Conclusion:
Reflexology is effective for reducing pain after appendectomy surgery.
Introduction
S
Today, despite the increasing awareness of pain physiology, the availability of new medications and prescribing practices, pain management after surgery is still unsatisfactory and insufficient. Previous studies reveal that 30%–40% of patients who undergo an abdominal procedure experience moderate to severe pain after surgery, and approximately 70% of patients experience severe pain on the first postoperative day. 5 –7
Typically, the pain lasts for 24–48 hours, sometimes longer. 8 From the perspective of patients, the major problem after surgery is pain at the incision site. 7 Annually, 23 million patients in the United States undergo surgeries, and a large number of them have acute postsurgical pain. 9 It is estimated that this experience will cost U.S. society $79 million annually. 10 A study has shown that effective postoperative pain management accelerates recovery, shortens hospital stay, and reduces costs. 11 Today, different methods are being used to reduce pain after surgery. Systemic opiate and nonsteroidal analgesics are among the most common medical interventions to relieve pain, and each is followed by specific health consequences. 12,13
Therefore, it is essential to use available, inexpensive, and less risky methods for postoperative pain management. Reflexology is a nonpharmacologic pain control method. Today, it is considered one of the six most popular alternative therapies in the United States. 14 Reflexologists believe that blocking the energy channels or chi may lead to declining health. They believe that foot manipulation and applying pressure on specific parts of the foot can reduce tension, improve blood flow and regional function, and, therefore, reduce pain in these areas. 15
Although several studies have evaluated the effect of foot reflexology on cancer-related pain, 16 –18 less attention is paid to the associated effects on postsurgical pain. Currently, given nurses' lack of time 19 and conflicting evidence on the effects of reflexology, 20 –22 this method is rarely used. Existing challenges in relation to the effectiveness of alternative medicine lead to inefficient application of such medical care; therefore, further research is needed in this area.
This study examined the effects of safe and noninvasive methods of reflexology 23 on pain intensity and analgesic consumption after appendectomy in three groups of patients: control, intervention, and placebo.
Materials and Methods
This randomized clinical trial was conducted on patients with appendicitis at Imam Reza Hospital in Mashhad, Iran, in 2013. In this double-blind study, the reflexologist differed from the person who completed the pain-level checklist. The analyzer had no information on the patient's treatment group or the type of massage. In addition, the intervention and placebo patients were not aware of their treatment group.
Ethical considerations
After the research ethics committee approved the study and the authorities of Imam Reza Hospital (AS) provided permission, the patients were informed about the study and randomly assigned to a group. Finally, after providing informed consent, the patients were included in the study.
Sampling
According to previous studies, a pilot study with a sample size of 10 patients in each group was performed to determine the initial estimate of the sample size. After 30 pilot samples were obtained, a total number of 105 patients was considered as the final statistical estimate.
This study used an easy nonprobability sampling size. 24,25 The parameters that were used for sample size calculation were a power of 80%, confidence level of 95%, and standard deviation of 2.2.
One researcher visited the emergency surgical department and selected patients who had been diagnosed with positive appendicitis and were eligible for the study (i.e., met the inclusion criteria); he allocated the patients to the intervention, placebo, or control group. Sampling was performed using random permuted blocks.
After clinical examination, routine laboratory tests, and ultrasound diagnosis, study-eligible patients with confirmed appendicitis were informed about study method and objectives before going to the operation room; informed consent was obtained from all participants. The patients were taught how to use the numeric pain scale. After surgery, if the patient was under general anesthesia and no postoperative complications were observed, he or she was included in the study. After the patient regained partial consciousness, the pain level was measured. If the pain was severe and unbearable, an analgesic was administered before the intervention and the patient was excluded from the study.
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) age 15–60 years; (2) appendectomy by a surgeon; (3) no history of surgery; (4) no addiction, sensory disorders, diabetes, or mental disorders; (5) lack of spinal anesthesia during surgery; (6) no history of the use of reflexology massage; (7) no chronic pain in other body areas; (8) lack of sensitivity to touching or massage; (9) no fever or skin diseases, (10) no pregnancy; (10) lack of severe postsurgical complications or hearing impairment; (11) consciousness; and (12) healthy feet and ears.
The exclusion criteria were as follows: (1) receipt of painkillers before the intervention, (2) receipt of any type of painkillers except methadone, (3) patient's death, and (4) hospital discharge before 24 hours of hospitalization.
Research skills
Before sampling, the researcher underwent two sessions of theoretical and two sessions of practical reflexology training in the presence of a professional instructor. Afterwards, reflexology was performed on seven people at the office. Finally, after the specialist's approval, the researcher started sampling. Pilot sampling was conducted with the participation of specialists.
Tools
For foot reflexology, a special device called a “stick,” which was designed for reflexology therapy and described in earlier reports, 14 was used (Fig. 1) For ear reflexology, special Chinese ear adhesive tape was used (Fig. 2). Use of this adhesive tape is safer and easier than other methods (such as ear acupuncture) and is considered more comfortable by patients as well. These tapes have also been used in other studies. 26,27 These devices were obtained from Beijing, China.

Reflexology stick.

Ear adhesive tape.
To measure the intensity of pain, a visual analogue scale (VAS) was used. This VAS is a horizontal line, divided into increments ranging 0 to 10, that measures the intensity of pain; 0 indicates lack of pain and 10 refers to severe pain. This scale has been examined in numerous studies 28 –30 and is one of the prominent grading scales used today.
Intervention
The Shen Men (TF4) point for ear reflexology lies in or close to the tip of the fossa triangularis (between the upper and lower legs of the antihelix). It diminishes stress, pain, tension, anxiety, depression, and sleeplessness. In operations where acupuncture anaesthetic is used, Shen Men (Fig. 3) is one of the most important points. 27

Shen Men point.
The tape was attached on the Shen Men point of the right ear of patients in the intervention group, who received ear reflexology therapy for 1 minute; then the tape was removed. The tape was squeezed 60 times during 1 minute. Previous investigations suggest that this leads to a calming effect on the brain. 31 Foot reflexology was applied with a stick for 10 minutes in the specified region of the right foot, which was related to the appendix and intestine area. 14
To investigate the specific effect of reflexology on the appendix and to avoid the effect of other reflexology points on the results, only the appendix point was stimulated; no relaxation procedures were used.
Reflexology for patients in the placebo group was performed by supporting the patient's left foot with the right hand and moving the stick under the toe fingers in a horizontal line from little toe to third toe; a very gentle pressure that lasted 10 minutes was applied. Accordingly, for ear reflexology, the ball was removed from the adhesive tape and the adhesive was put on the right earlobe and removed after 1 minute.
Patients in the control group received only routine care (checking of vital sign and methadone if necessary). Pain intensity and analgesic dose for placebo and intervention groups were measured and recorded before and immediately, 1hour, 6 hours, and 24 hours after the intervention by a person unaware of the treatment group. In the control group, pain was measured immediately, 1 hour, 6 hours, and 24 hours after patient achieved partial consciousness. Patients in all three group were receiving routine analgesics (methadone, 5 mg), as required, after the intervention.
Data collection and analysis
After collection and importing of the data into SPSS software, version 12 (SPSS, Inc., Chicago, IL), charts, statistical tables and indices, central tendency, and distribution were used to describe the data. Chi-square, analysis of variance, and the Tukey post hoc test were used. In all calculations, a p-value < 0.05 was considered to represent statistically significant differences. The data analyzer was not aware of any patient's treatment group.
Results
Of 105 patients with appendicitis, 39 patients (37.1%) were female and 66 (62.9%) were male. Of the 35 patients in each treatment group, 20 patients (57.1%) in the intervention group, 21 patients (60.0%) in the placebo group, and 25 patients (71.4%) in the control group were male and the rest were female; the male-to-female ratio did not bear any meaningful differences (p = 0.425).
At the beginning of the study, the mean pain intensity, based on VAS scores, was 8.14 ± 2.24 for the intervention group, 8.23 ± 2.81 for the control group, and 8.86 ± 2.52 for the placebo group, which did not show a statistically significant difference (p = 0.439). In all three groups, decline of pain intensity during treatment was evident (p ≤ 0.001). Pain intensity during treatments was different in the treatment groups (p ≤ 0.001). The difference in pain intensity was significant between the intervention and control groups (p ≤ 0.001) and between the intervention and placebo groups (p ≤ 0.001); the difference between the placebo and control groups was not statistically significant (p = 0.979). (Figure 4 and Table 1 show the general trend of changes in pain in treatment groups during the study.)
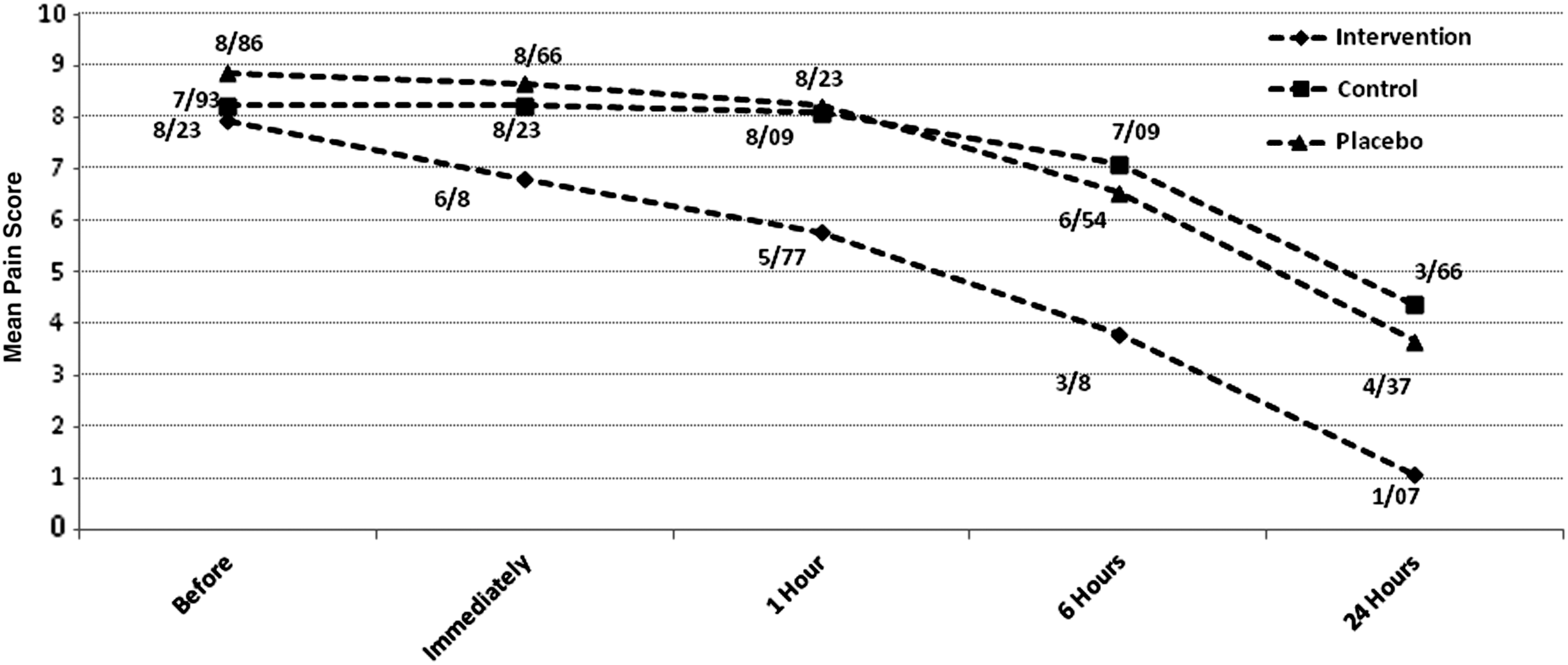
Changes in pain intensity among different treatment groups during the study period.
Values are expressed as mean ± standard deviation.
Chi-square results showed no significant difference between the placebo and control groups in terms of methadone consumption; however, the intake in the intervention group was significantly less than in the other two groups. (Figure 5 and Table 2 show the methadone consumption in different groups during the study period.)

Patients' methadone consumption in different groups during the study period.
The results of a generalized estimation equation (an alternative to the likelihood-based generalized linear mixed model used for analysis of longitudinal data) showed that the possibility of pain reduction in the intervention group was 7.24 times higher than in the placebo group (p < 0.001). In addition, the possibility of pain increase in the control group was 1.03 times higher than in the placebo group (p = 0. 947).
Moreover, the results showed that the possibility of reduction in drug consumption in the intervention group was 3.22 times higher than in the placebo group (p < 0.001). Also, the possibility of increased drug use in the control group was 2.73 times higher than in the placebo group (p < 0.001).
Discussion
The results of this study showed that reflexology can reduce pain and analgesic consumption in patients after appendectomy. Although none of the previous studies have examined the effect of reflexology on reducing pain after appendectomy in patients, several studies have measured the effects of foot reflexology under different conditions, and some of them have been effective in reducing pain. For instance, the positive effect of foot reflexology, over 1 week, was confirmed in 40 cases of lumbosacral herniation. 32 In addition, on the basis of the research conducted on women undergoing cesarean delivery and breast surgery, successful application of this massage reduced pain. 32 –35 Moreover, various studies showed the positive effect of foot reflexology on sternotomy pain after coronary artery bypass graft surgery. 35,36
In other studies, foot reflexology and ear acupuncture reduced pain and analgesic consumption in the days after surgery. 37,38 It is still unclear that how reflexology affects physiologic and biochemical parameters, 39 but some studies pointed out that reflexology can help reduce pain through the release of endorphins and enkephalins. 40 In fact, the release of these neurotransmitters can cause sedation and analgesic effects, which may be the reason that patients go to sleep during the intervention. On the other hand, pain reduction may result from pressure on specific reflex points and the prevention of pain transmission through gate control mechanism. 41
However, some studies rejected the analgesic effect of reflexology massage on surgeries such as total knee replacement and abdominal surgery (due to gynecologic reasons). 42,43 In the study conducted on patients undergoing total knee replacement surgery, despite the lack of change in pain intensity in the intervention group, use of analgesics in this group of patients was significantly lower than in the placebo group. 42,43 Lack of a control group was a limitation of that research that has been resolved in the current study. In addition, performing only ear reflexology and prolonged interference time can lead to the variation in the results of this study and the current study.
It can be inferred from previous studies that ear reflexology can also cause endocrinologic and neuroendocrinologic responses and can affect people in this way. 44 However, the analgesic effect of ear acupuncture on patients after knee surgery in Usichenko study was rejected. In that study, the needle was placed on the ears and remained there until the next day. Knee joint, Shen Men, and lung were three acupuncture points used in that study. The results of that study indicate that pain intensity remained the same after the intervention in both groups. The difference in pain reduction in that study may be due to different effects of acupuncture compared with ear reflexology; it is recommended that it be addressed in additional studies. Furthermore, lack of a control group and needle insertion in other parts of the ear in the placebo group (which can have similar effects according to other studies 45 ) are among the limitations of that study. 46 This problem was curbed in the current study by including a control group.
Simultaneous application of reflexology for the ear and foot can be another possible reason for the reduction of pain in the current study, compared to other similar studies. Pain reduction in the intervention group led to a decrease in methadone intake compared with the control and placebo groups.
Korhan and colleagues reduced the intake of analgesics in patients undergoing ventilation by doing 30 minutes of foot, hand, and ear reflexology each day for 5 days. 47 In addition, Grammel et al. reduced opioid intake (a combination of tilidine and pethidine) by up to 75% with ear acupuncture in 20 patients undergoing total hip arthroplasty. However, lack of randomization and blinding and the small number of samples may be the reason behind the significant analgesic effect in the study. 47,48
In the present study, analgesic consumption in the intervention group was significantly lower than in the other two groups of patients. On the other hand, although the mean pain reduction in the control and placebo groups was not significantly different, the amount of methadone intake among patients in the placebo group decreased compared with the control group; these results indicate the placebo effect of this massage. Hence, further research should be done in three treatment groups (control, placebo, and intervention) to compare the obtained results in the placebo group with those of the control and intervention groups and focus on the placebo effect of this massage.
Another possible reason for variations in pain intensity reduction in different experiments on reflexology can be due to different effects of reflexology on various diseases and people. As Ernst and colleagues demonstrated in a systematic study on the effect of reflexology on specific diseases and conditions, reflexology can be effective for patients with diabetes, premenstrual syndrome, cancer, multiple sclerosis, unknown detrusor overactivity, and forgetfulness; however, it was not effective for other diseases. Therefore, reflexology may not be effective in all conditions and medical problems, 49 and it is recommended that further research be performed on the effects of massage on patients with various physical and mental conditions.
Reflexology is a safe, simple, and cost-effective method that can be applied by patients themselves after discharge from the hospital to control the pain. This research was conducted on the basis of experts' opinions in order to evaluate the use of complementary and alternative therapies for the reduction of pain, analgesic consumption, and adverse effects of medications after surgery. The double-blind nature of the study (data collector and analyzer of the treatment group were blinded to the study groups) and patients' lack of awareness of the type of massage therapy in the placebo and intervention groups minimize the bias and increase the credibility and reliability of the results.
In addition, the increased number of participants in this study compared with other related research and inclusion of three groups (control, intervention, and placebo) are strengths of the current study that some other studies neglected.
The theory of meridians is another explanation for reflexology, especially ear reflexology. According to this theory, meridians are a complex system that consist of 12 primary meridians, 12 divergent meridians, 8 extraordinary vessels, and 15 collaterals. It also includes numerous minute collaterals, superficial collaterals, and vessels. 50
It is very difficult to determine which part of the body is not affected by these meridians and branches. Because of the high density of these meridians in the ear, stimulating each of the areas can lead to similar effects. 45
Therefore, the current study evaluated the effect of reflexology on true and false regions and compared it with those seen in patients in the control group. To minimize the effect of pressure for placebo patients, the ear ball glue was removed and foot reflexology was performed with minimal pressure.
This study has some limitations. The research was conducted in a single hospital setting, and the effectiveness of environment and personnel-patient interactions could not be evaluated. Moreover, patients who had undergone appendectomy were discharged after 1 day; thus, the long-term effects of reflexology could not be assessed. Further research on the long-term effects of this complementary therapy should be performed.
In conclusion, the findings suggested the positive effect of foot and ear reflexology for reduction of pain and analgesic use after appendectomy. Therefore, it is suggested that nurses employ this method to reduce pain and analgesic intake in patients undergoing appendectomy, given its simple application and cost-effectiveness. Results of this study could pave the way for the use of nonpharmacologic methods and increase patient satisfaction and quality of medical hospital care. In fact, it should be a priority for personnel and health programs.
Footnotes
Acknowledgments
The authors would like to thank the emergency department personnel of Imam Reza Hospital, who cooperated with the study. The study was supported financially by the Vice Chancellery of Research of Sabzevar University of Medical Sciences with the approval number 392025002.
Author Disclosure Statement
No competing financial interests exist.