
Abstract
Background/Objective:
Atopic dermatitis comprises a group of chronic, relapsing inflammatory conditions. Topical steroids (TS) can ameliorate atopic dermatitis but induce skin atrophy and secondary infection. Tzu-Yun ointment (TYO) was used widely for skin ulcers and pus discharges. This study sought to determine whether TYO can replace TS therapy for atopic dermatitis.
Methods:
This preliminary, randomized, controlled, open-label design compared the therapeutic effects of TS and TYO in patients with atopic dermatitis; 33 patients were randomly assigned to the TS group (17 patients) and the TYO group (16 patients). All patients received an 8-week TS or TYO treatment. Primary outcome measures were assessed by using the Eczema Area and Severity Index (EASI) and Three Item Severity (TIS) before the treatment (baseline, week 0) and 1 week (week 1), 2 weeks (week 2), 4 weeks (week 4), and 8 weeks (week 8) after initiation of the treatment.
Results:
Of the 33 enrolled patients, 31 (16 in the TS group and 15 in the TYO group) completed the study. Patients in both groups showed decreased EASI and TIS scores, with no significant difference at weeks 0, 1, 2, 4, and 8.
Conclusion:
TYO may be as effective as TS therapy for atopic dermatitis and has potential as an alternative treatment for this condition.
Introduction
E
Tzu-Yun ointment (TYO) is a Traditional Chinese Medicine (TCM)–based formula described in Waikezhengzong (i.e., TCM writing). TYO consists of sesame oil (Ma you), Angelica sinensis (Oliv.) Diels (Dong qi), Lithospermum erythrorhizon (Tzu tsao), and yellow wax (Huang la) and is clinically used for skin ulcers and pus discharge. TYO is used to treat several skin disorders, such as bed sores, eczema, and ulcers. The ointment is widely used in Asian countries, including Taiwan. Shikonin, an active component extracted from L. erythrorhizon, exhibits anti-inflammatory and antimicrobacterial properties and can be used to treat eczema, carbuncle, and burns. 5
Although TYO is widely used in Asia to treat skin disorders, it is yet to be scientifically assessed. Therefore, a randomized, controlled, preliminary, open-label trial was conducted to investigate the therapeutic efficacy of TYO in eczema/atopic dermatitis.
Materials and Methods
Drug preparation
The TYO was manufactured by Sun Ten Pharmaceutical Co. Ltd., Taiwan, a good manufacturing practice factory (license number: 013198). In this study, each gram of TYO contained Arnebia euchroma (120 mg), cera flava (300 mg), A. sinensis (60 mg), and sesame oil (quantum sufficit). The TYO was analyzed by using a high-performance liquid chromatography system with ferulic acid and ligustilide for a marker substance for A. sinensis, and shikonin, β-hydroxisovaleryshikonin, acetyshikonin, deoxyshikonin, (β, β-dimethylacryl) shikonin, and 2-methy-n-butyryl shikonin for A. euchroma (Fig. 1). A cream containing 0.6 mg/g of betamethasone valerate (Shionogi & Co., Ltd., Osaka, Japan; license number: 010577) was used as the control drug.

Fingerprint of Tzu-Yun ointment obtained by using a high-performance liquid chromatography system analysis.
Participants
Patients diagnosed with atopic dermatitis by dermatologists at least 5 years before the study were included. The inclusion criteria were as follows: (1) female or male, 2) age between 18 and 65 years (inclusive), (3) ability to apply the topical drug twice daily on their own, and (4) agreement to participate in the trial and completion of signed informed consent. The exclusion criteria were as follows: (1) pregnancy or lactation, (2) overt bacterial infection, (3) systemic treatment with steroids, antibiotics, phototherapy, or immunomodulator drugs in the 8 weeks before the study, and (5) allergy to TYO or betamethasone valerate.
The Institutional Ethics Committee of the Veterans General Hospital, Taichung, Taiwan (IRB TCVGH number: CF13038), approved the study. All participants provided written informed consent. The following demographic and clinical characteristics were recorded: age; sex; duration of atopic dermatitis; Eczema Area and Severity Index (EASI) and Three Item Severity (TIS) scores before the treatment; IgE levels; and a history of diabetes mellitus, hypertension, autoimmune disorders, and hyperlipidemia.
Treatment groups and interventions
Participants were randomly assigned to the TYO group (intervention: local application of TYO twice a day) or the TS group (intervention: topical application of betamethasone valerate cream twice a day). The study period was 8 weeks; however, the treatment could be stopped when all lesions were completely clear. All participants received an oral antihistamine drug (cetirizine, 10 mg/d) to prevent itching. The treatment would be immediately stopped upon noticing any adverse effects, such as allergy, that were possibly associated with the treatment (Fig. 2).
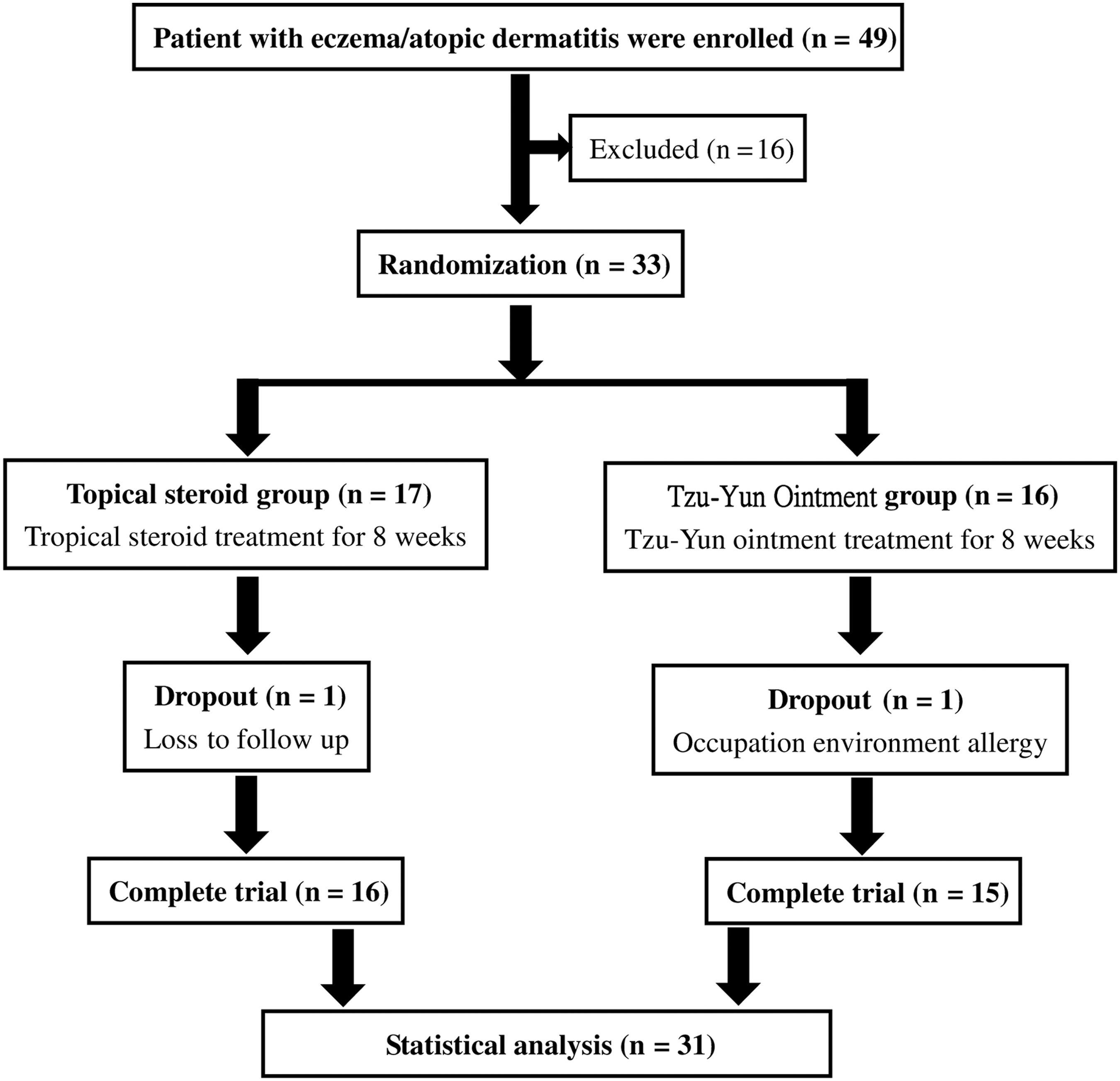
Flowchart of screening and enrollment.
Sample size
The study used a preliminary, randomized, controlled, open-label design. Because this trial was a preliminary study, statistical power and sample size were not calculated.
Assessment
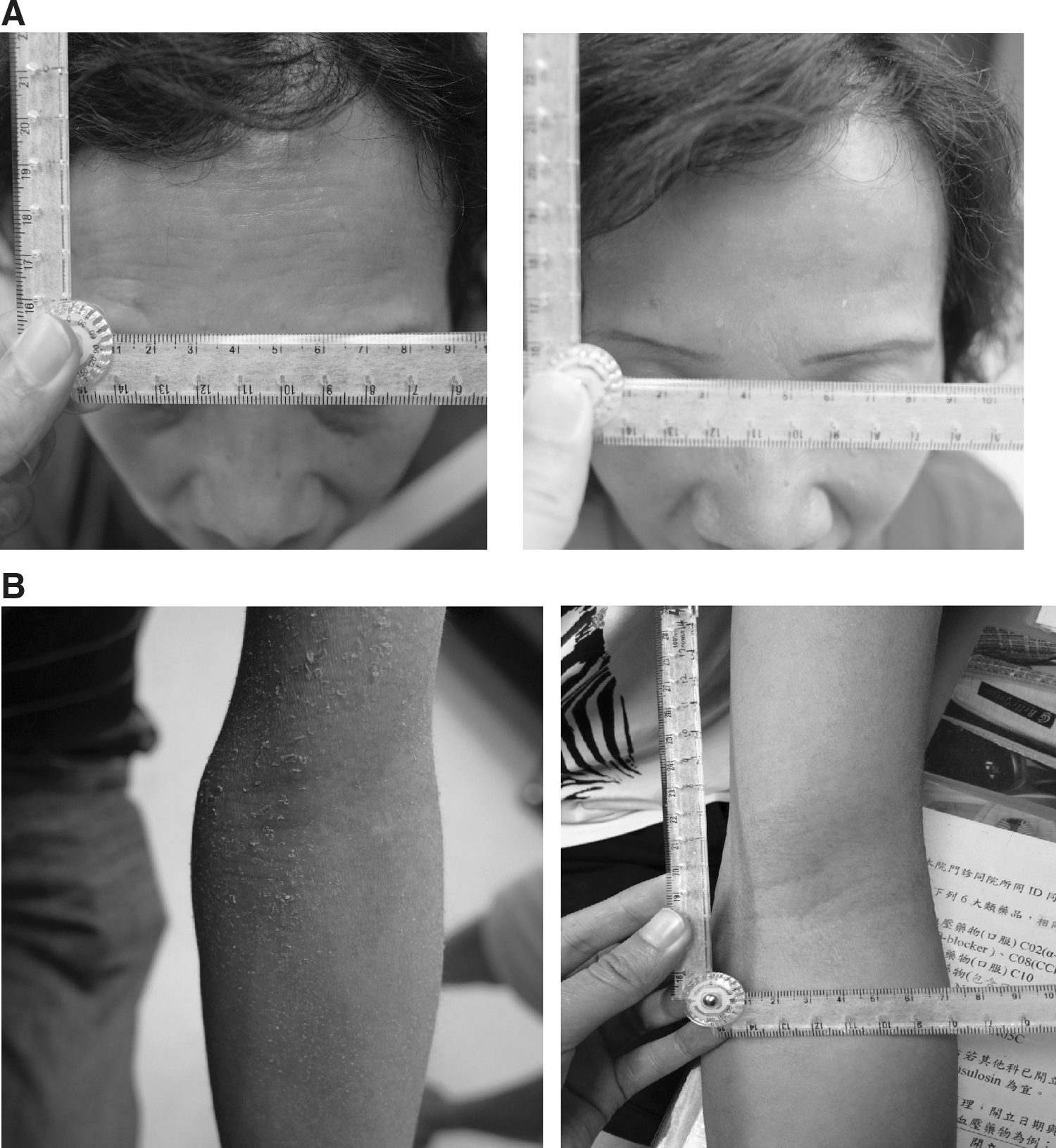
A well-trained nurse blinded to the groups assessed the ESAI and TIS scores before the treatment and at weeks 1, 2, 4, and 8 after the treatment was initiated. The skin lesions were photographed after each assessment.
Primary outcome measures
Disease severity was analyzed by using EASI and TIS scores. Outcome measures were defined on the basis of body surface area and redness, swelling, lichenification, and scratches on the body. The intensity of severity was scored on a scale of 0 to 3 (none, mild, moderate, or severe). The total score was calculated as the sum of the maximal score of redness, swelling, lichenification, and scratch marks for each patient. In addition, the redness of a lesion was measured by using a spectrometer (Cortex Technology, Hadsund, Denmark).
Statistical analyses
All statistical analyses were performed using SPSS statistical software, version 22 (IBM, Chicago, IL). The chi-squared test, paired t test, Mann–Whitney U test, and analysis of variance were used, with the significance level set at p < 0.05.
Results
Of the 49 screened patients, 33 patients with atopic dermatitis were enrolled in this study; 17 patients were assigned to the TS group and 16 to the TYO group, and 31 of these patients (16 and 15 patients in the TS and TYO groups, respectively) completed the trial. Two patients were withdrawn from the study: A patient in the TYO group was withdrawn because of a progressing skin lesion owing to occupational and environmental allergies. He was treated with oral prednisolone therapy and a change in occupation and environment. Another patient in the TS group failed to follow up because of a busy work schedule (Fig. 2).
The demographic characteristics—sex, age, a history of diabetes mellitus, hypertension, autoimmune disorders, hyperlipidemia, duration of atopic dermatitis, IgE levels, and EASI and TIS scores before treatment—showed no significant difference between the TYO and TS groups (all p > 0.05; Table 1).
Values are expressed as number (percentage) or mean ± standard deviation. Analyses were conducted by using the Mann–Whitney U test.
TS, topical steroid; TYO, Tzu-Yun ointment; pre-EASI score, Eczema Area and Severity Index score before treatment; pre-TIS score, Three Item Severity score before treatment.
Patients in the TS group showed decreased EASI and TIS scores after 8 weeks (p = 0.001 and 0.000, respectively) (Table 2 and Fig. 3A). Patients in the TYO group showed decreased EASI and TIS scores after 8 weeks (p = 0.002 and 0.000, respectively) (Table 2; Fig. 3B). The recurrences of EASI and TIS scores between the two groups did not differ significantly (both p = 1.0) (Table 3). In addition, differences between EASI and TIS scores were calculated as ([the score at week 0 – the score at week 8]/[the score at week 0]). These values did not differ significantly between the two groups (p = 0.082 and 0.567, respectively) (Table 3).
Effect of Tzu-Yun ointment and topical steroid cream in patients with atopic dermatitis.
Data are expressed as mean ± standard deviation. Analyses were conducted by using the paired t test.
Compared with prescore.
Values are expressed as number (percentage) or mean ± standard deviation. Unless otherwise noted, analyses were conducted by using Mann–Whitney U test.
Fisher exact test.
Prescore, score before treatment; end score, score at end of treatment.
The EASI and TIS scores did not significantly differ between the two groups at weeks 0, 1, 2, 4, and 8 (all p > 0.05) (Fig. 4A, B). The redness scores between the two groups at weeks 0, 1, 2, 4, and 8 did not differ significantly (all p > 0.05) (Fig. 5). The redness scores at weeks 2, 4, and 8 were less than those at week 0 in the TS group (all p < 0.05) (Fig. 5).
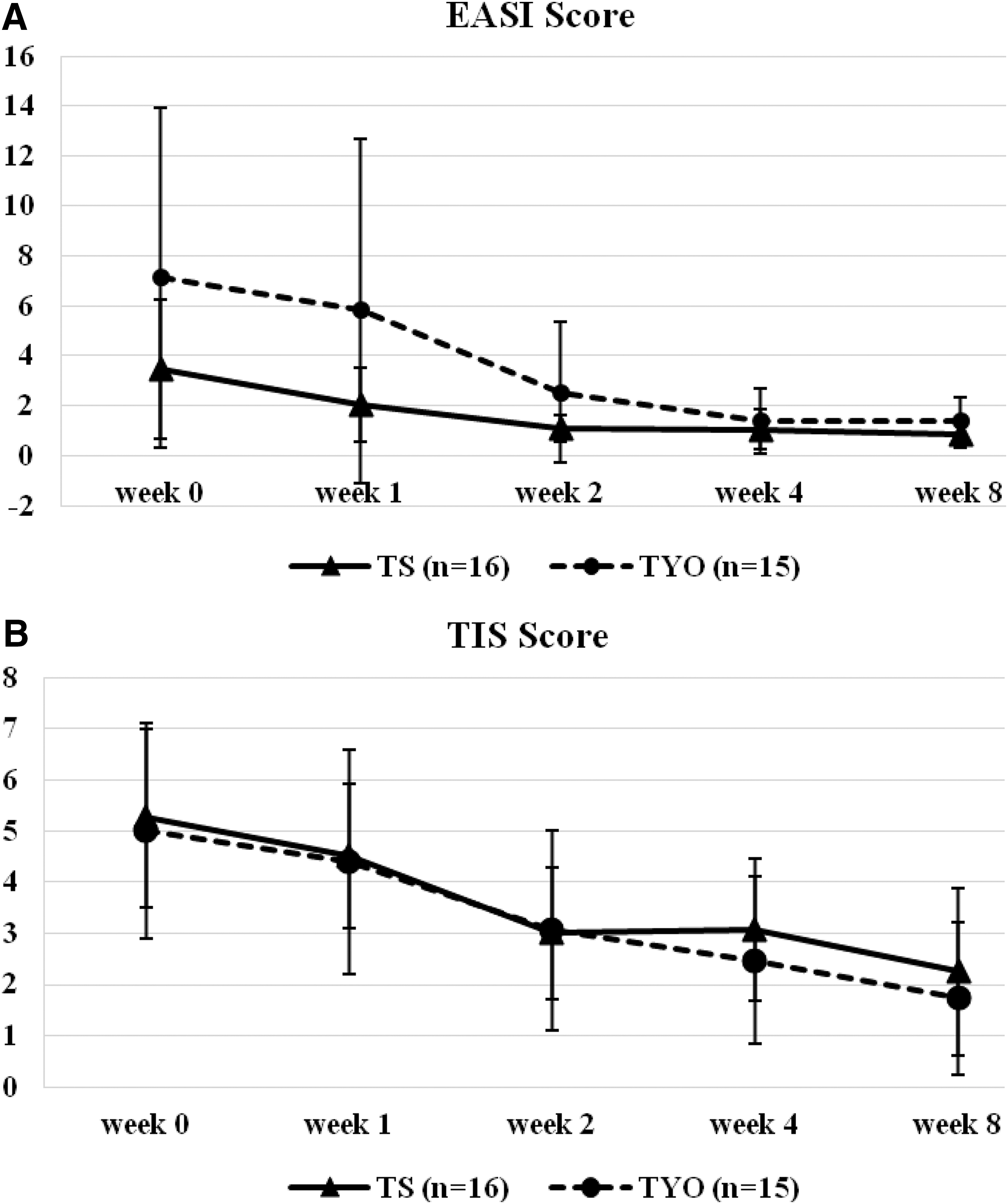
Effect of Tzu-Yun ointment (TYO) and topical steroid (TS) cream on Eczema Area and Severity Index (EASI) and Three Item Severity (TIS) scores in patients with atopic dermatitis as the study progressed. Depicted are changes in EASI
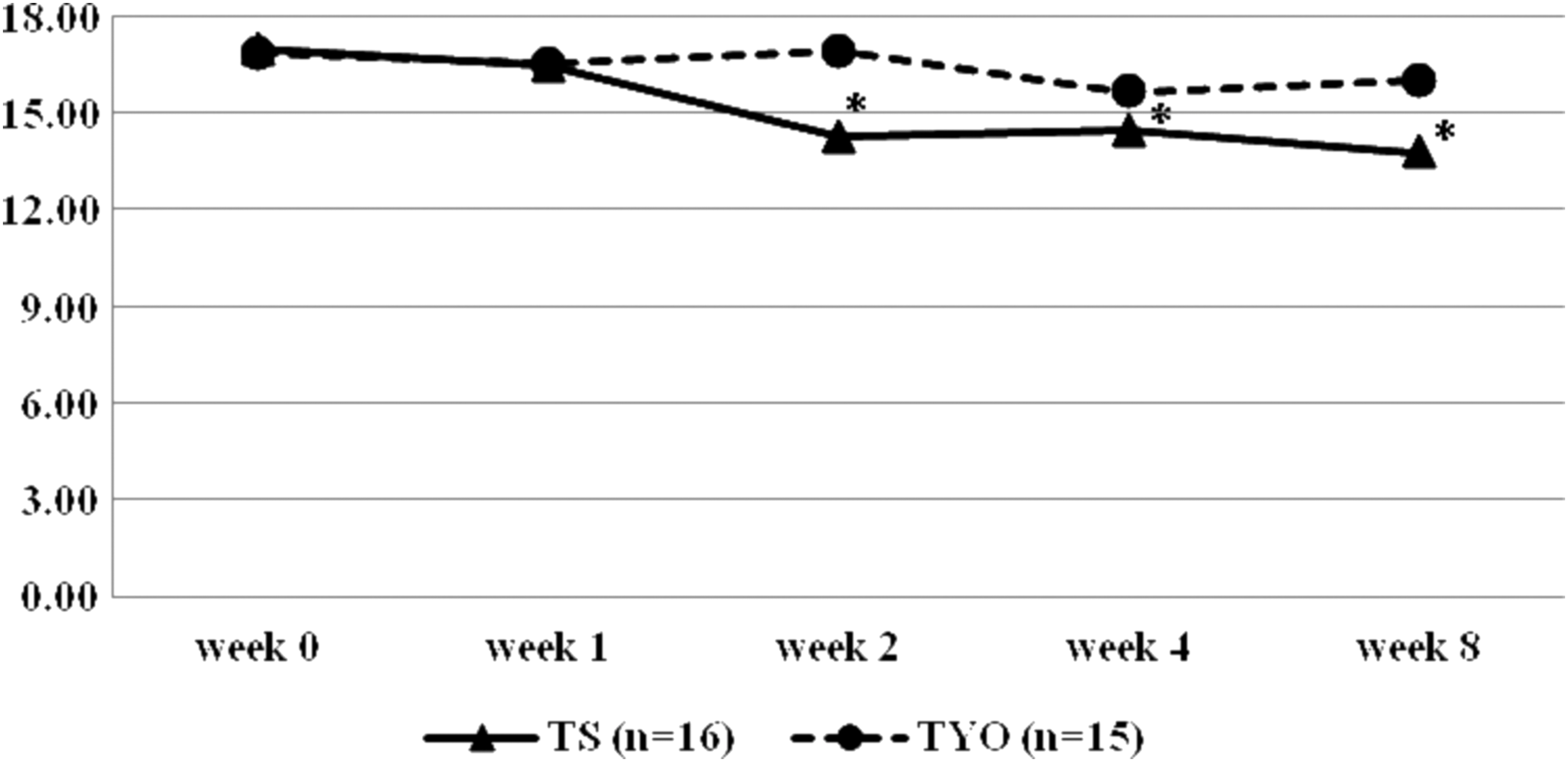
Effect of TYO and TS cream on erythema scores measured by using a spectrometer in patients with atopic dermatitis as the study progressed. *p < 0.05 compared with the score at week 0.
All patients showed improvements in the symptoms of pruritus after the treatment. One patient reported a hypopigmentation ring and a poor response to a previous TS therapy; the hypopigmentation ring gradually improved after the TYO treatment. Two patients (one each in the TS and TYO groups) experienced a stinging sensation at the beginning of the treatment, but this was resolved within 2 days. Three patients in the TYO group reported that TYO stained their clothes. Two patients in the TYO group and two in the TS group had a recurrence within 4 weeks.
Discussion
The demographic characteristics, namely sex, age, a history of diabetes mellitus, hypertension, autoimmune diseases, and hyperlipidemia, duration of eczema/atopic dermatitis, IgE levels, and EASI and TIS scores before the treatment, did not differ significantly between the two groups. Therefore, the results are comparable. Both EASI and TIS scores in the patients with eczema/atopic dermatitis decreased after the 8-week treatment of TS or TYO. In addition, no significant differences in TSAI and TIS scores of patients in both groups were observed, suggesting that the efficacies of betamethasone cream and TYO were similar in patients with atopic dermatitis. The atopic dermatitis results from a dysregulation between Th1 and Th2 lymphocyte-mediated immunity, which causes Th2-mediated inflammation, resulting in a dysfunction of the skin barrier, 6 particularly in a primary skin barrier, causing secondary inflammation. 7
Topical corticosteroid therapy is a first-line treatment for eczema/atopic dermatitis, 6 but it reduces host immunity and increases the rate of bacterial infection. Some bacterial toxins deteriorate atopic dermatitis. Some patients with atopic dermatitis have allergic antibodies, such as IgE for the Staphylococcus toxin. 8
L. erythrorhizon is a main component of TYO. Shikonin, an active component of L. erythrorhizon, activates the anti-inflammatory process by suppressing mast cell degranulation and inhibition of leukotriene B4 biosynthesis, cyclooxygenase-2 transcription, and nuclear factor-κB activation. 8,9 Sesame oil acts as a moisture base for the patient's skin and enriches it with omega-3 fatty acids, which are highly effective anti-inflammatory agents. 10 Ferulic acid, a component of A. sinensis (Oliv.) Diels, has anti-inflammatory and analgesic effects. 11 TS ameliorates the symptoms and signs of eczema/atopic dermatitis, possibly through its immunosuppressive effects, whereas TYO essentially produces anti-inflammatory activities.
Although these results indicated that the erythema scores calculated from week 0 to week 8 did not differ significantly between the two groups, scores at weeks 2, 4, and 8 were less than that at week 0 in the TS group. No similar results were observed in the TYO group. These results suggest that TS more effectively reduced erythema than did TYO did and that the color of TYO made differentiating between the color of a lesion and the color of the ointment difficult. Three patients in the TYO group reported that TYO stained their clothes.
Two patients (one each in the TS and TYO groups) experienced a stinging sensation, which suggests that TS and TYO imparted stimulant properties to the inflammatory lesion; however, the patients did not withdraw, indicating that the effect was tolerable. Several studies have shown that TS may induce several adverse effects, including metabolic effects (such as skin atrophy, acne, skin atrophy, and skin striae) and immunosuppressant effects (such as bacterial, viral, and fungal infections). 12 Other adverse effects include hypopigmenation, 13 osteoporosis, hyperglycemia, glaucoma, and adrenal insufficiency. 12 TYO has been used for the past several hundred years in Asian countries, particularly for wound healing, and no severe adverse effects have been reported. In addition, evidence that TYO reduces host immunity is lacking. In severe atopic dermatitis, excoriation wounds and crusts are produced easily, and the subsequent inflammation can be suitably treated by using TYO. A drawback of TYO is the discomfort in applying the ointment on the face and its tendency to stain clothing dark purple.
This study has some limitations. First, this was a preliminary, small-sample study. A large-sample, double-blinded, randomized, controlled trial is necessary to support the authenticity of these results. Second, although no adverse effects were observed with the TYO treatment except for staining of clothes and sting sensation, the safety of TYO must be assessed with a longer follow-up study.
Conclusion
An 8-week treatment of both TS and TYO successfully lowered EASI and TIS scores in patients with atopic dermatitis, and changes in both the scores did not differ significantly between the two groups. The results suggest that TYO has potential as an alternative treatment for eczema/atopic dermatitis and is as effective as TS therapy is. Future product refinement and research will be needed to reduce a stinging sensation in some patients and staining of clothes.
Footnotes
Acknowledgments
This study was supported by a grant from Chinese Medicine Research Center, China Medical University (Ministry of Education, The Aim for the Top University Plan) and also is supported in part by the Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW105-TDU-B-212-133019).
The authors thank the Biostatistics Task Force of Taichung Veterans General Hospital, Taichung, Taiwan, Republic of China, for analyses.
C.-Y.Y. designed the protocol, performed the trial, and wrote the manuscript; C.-L.H. was an advisor, participated in designing the protocol, and helped revise the manuscript.
Author Disclosure Statement
No competing financial interests exist.