
Abstract
Background:
The purpose of this study was to examine the effectiveness of aromatherapy with ginger essential oil on nausea and vomiting in abdominal surgery patients.
Method:
This was a quasi-experimental study with a nonequivalent control group and repeated measures. The experimental group (n = 30) received ginger essential oil inhalation. The placebo control group (n = 30) received normal saline inhalation. The level of postoperative nausea and vomiting was measured using a Korean version of the Index of Nausea, Vomiting, and Retching (INVR) at baseline and at 6, 12, and 24 h after aromatherapy administration. The data were collected from July 23 to August 22, 2012.
Results:
Nausea and vomiting scores were significantly lower in the experimental group with ginger essential oil inhalation than those in the placebo control group with normal saline. In the experimental group, the nausea and vomiting scores decreased considerably in the first 6 h after inhaled aromatherapy with ginger essential oil.
Conclusion:
Findings indicate that ginger essential oil inhalation has implications for alleviating postoperative nausea and vomiting in abdominal surgery patients.
Introduction
P
Considering complex and multifactorial nature of PONV, several guidelines with the recommendation of a multimodal approach based on evidence have been developed in recent years. Furthermore, non-pharmacological techniques such as aromatherapy have been considered in the management of PONV, along with conventional management that includes hydration and anti-emetic treatment. 1,14 –18
Among popular complementary and alternative interventions, aromatherapy is the therapeutic use of essential oils from fragrant plants such as rose and peppermint through inhalation or topical application. 19,20 A systematic review of studies on aromatherapy with peppermint or ginger essential oils for nausea and vomiting demonstrated that the use of inhaled aromatherapy with these essential oils could be an effective treatment to reduce not only the incidence of nausea and vomiting but also the need for anti-emetic treatment. 21 –23 In particular, ginger (Zingiber officinale) has been used in ancient medicine as an important medicinal remedy to alleviate digestive problems such as nausea and vomiting. 24 –26
The use and effectiveness of this herb for the management of PONV have been evaluated in several clinical studies. 15,27 –30 Findings from a meta-analysis of five randomized trials (a total of 363 patients) on the effectiveness of ginger for PONV indicated that a prophylactic administration of at least 1 g of powered ginger root can significantly reduce PONV occurrence in the first 24 h among patients who received gynecologic or lower extremity surgeries. 15 However, relatively few researchers to date have investigated aromatherapy with ginger essential oil as a treatment for PONV. In a controlled clinical trial with adult patients at high risk for PONV, a 5% solution of ginger essential oil applied to both wrists as well as below the nose prior to surgery was found to be significantly effective in the prevention of PONV. 27 In another randomized trial, changes in both nausea level and the number of requests for anti-emetic medication were found to be significant for aromatherapy with ginger essential oil or an essential oil blend of ginger, spearmint, peppermint, and cardamom compared with normal saline. The number of anti-emetic medications requested after aromatherapy was also significantly reduced with ginger or blend aromatherapy versus saline. 29 Yet, little has been studied on the effectiveness of such use of aromatherapy in Korea. Therefore, the purpose of the study was to investigate the effectiveness of aromatherapy with ginger essential oil for PONV in Korean adult patients who received major abdominal surgery.
This study investigated the effectiveness of aromatherapy with ginger essential oil for the treatment of PONV, as well as the efficacy over a longer period as measured with the level of PONV three times at 6, 12, and 24 h after aromatherapy administration. The findings that inhaled aromatherapy using ginger essential oil reduces nausea and vomiting after major abdominal surgery provide additional support that ginger essential oil is helpful to treat later-stage PONV. Aromatherapy with ginger essential oil can serve as a promising treatment option to prevent and manage nausea and vomiting after surgery.
Materials and Methods
Design and participants
A quasi-experimental study design with a nonequivalent control group and repeated measures was employed for the study. All participants were recruited from three surgical units in a tertiary hospital in Seoul, Korea. Eligible patients were those scheduled for major abdominal surgery (e.g., liver, gallbladder, pancreas, appendix) under general anesthesia for a minimum of 60 min; aged between 20 and 70 years; alert and oriented in terms of time, place, person, and situation when admitted to the units; requesting patient-controlled analgesia (PCA) with fentanyl for postoperative pain control; and able to understand the study purpose. Patients were excluded if they had severe heart, lung, or kidney disease; were receiving chemotherapy treatment; had a history of drug allergies; had allergies to essential oils; or had sensitivity to ginger aroma.
The target sample size was 30 for each group. The sample size was determined using a power analysis program (G*POWER 3.0) 31 for a mixed-design analysis of variance (ANOVA) with an alpha of 0.05, medium effect size of 0.5, and a power of 0.8. The participants were not randomly assigned into two groups. To control for possible diffusion effects of the aromatherapy with ginger essential oil in this study, data collection was completed from the placebo control group patients before collecting data from the experimental group patients. No patients dropped out of the study, so the final sample size was 60 (30 in the experimental group and 30 in the placebo control group).
Research instruments
The level of PONV was measured using a Korean version of the Index of Nausea, Vomiting, and Retching (INVR). 32 The INVR consists of eight items with a five-point Likert-type scale response option that asked about the frequency and duration of nausea (three items), vomiting (three items), and retching (two items). The possible scores ranged from 0 to 32, and a higher score indicated a greater severity of PONV. This scale was chosen for ease of administration on patients who were recovering from anesthesia. Reliability and validity of the Korean version of the INVR have been established for use among Korean patients. 33 –35 In the current sample, the Cronbach's alpha was 0.94, indicating high reliability.
Intervention
For this study, 100% pure and certified organic ginger essential oil (La Drome Provencale, France) was used. Patients in the experimental group were given an aromatherapy necklace as soon as they arrived at the unit from the post-anesthesia recovery unit (PACU). This aromatherapy necklace contained 0.3 mL of ginger essential oil. For patients in the placebo control group, the same type of necklace with 0.3 mL of normal saline was given. All patients in the two groups were instructed to wear the necklace for 24 h and to inhale the aroma while naturally deep breathing. Analgesics provided to all patients in both the control group and the experimental group after the surgery were 30 mg of ketorolac tromethamine or 50 mg of tramadol hcl.
Data collection
The study was approved by the Institutional Review Board at the study hospital (IRB number: 2012-0420). Written informed consent was obtained from all patients who met all the criteria and agreed to participate in the study during a face-to-face interview with investigators. Data were collected by five research assistants (three in the PACU and two in the surgical units) for 4 weeks during July and August, 2012. All research assistants were trained regarding the study purpose and all aspects of the data collection procedure to minimize potential bias during data collection. Immediately before transfer to PACU, each patient was asked to assess their level of nausea and vomiting using the INVR scale. This self-assessment was then repeated at 6, 12, and 24 h after the initial aromatherapy administration.
Data analysis
To compare sample patient characteristics between the experimental group and the placebo control group, independent t tests were used for continuous variables and Pearson's chi-square tests for categorical variables with Fisher's exact test when the sample size in a cell was <5. A mixed design ANOVA (group × time) was used to examine the effects of aromatherapy with ginger essential oil on PONV. Included in the model were group (experimental and control), time (baseline, 6, 12, and 24 h), and the interaction between group and time. The level of significance for statistical tests was considered at p < 0.05. All analyses were performed using IBM SPSS v19 (IBM Corp, Armonk, NY).
Results
As shown in Table 1, no significant differences were found between the experimental group and the placebo control group with regard to demographics and other characteristics, including age, sex, history of nausea, and duration of anesthesia. In this study, patients in the experimental group used an average of 0.15 mL of ginger essential oil for the 24 h inhaled aromatherapy, and reported no side effects related to ginger essential oil. Table 2 shows the mean PONV scores with standard deviations for the two groups at baseline (before aromatherapy) and at 6, 12, and 24 h after aromatherapy administration. The mean PONV scores at baseline for the experimental group with ginger essential oil and the placebo control group with normal saline were 11.80 and 11.57, respectively, and no significant difference was found between the two groups.
SD, standard deviation.
Results from a mixed-design ANOVA showed that there were significant main effects of group (F = 71.21, p < 0.001) and time (F = 73.87, p < 0.001) on the mean scores of PONV. Mean PONV scores in the experimental group were significantly lower than those in the placebo control counterpart at all three time points after aromatherapy. These scores significantly decreased in the two groups within 24 h after aromatherapy administration. The interaction effect between group and time was also found to be statistically significant (F = 26.85, p < 0.001), indicating that changes in the PONV scores were considerably different between the two groups over time. The mean PONV scores of the ginger essential oil inhalation group decreased significantly to an average of 1.14, while those of normal saline inhalation group did not change dramatically with an average of 8.91. Moreover, among the three different time points of PONV scores in the experimental group, a significant decrease in mean scores was found at 6 h after initial aromatherapy with ginger essential oil (see Fig. 1).
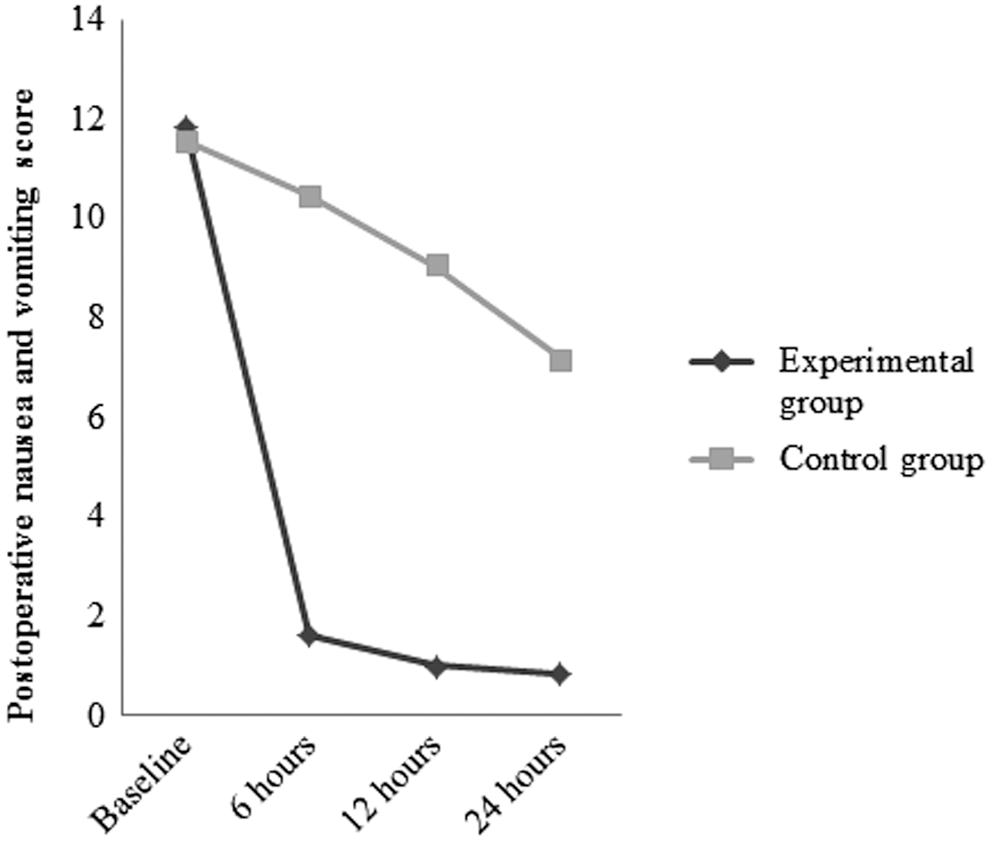
Postoperative nausea and vomiting scores in the experimental and control groups within 24 h after aromatherapy.
Discussion
Aromatherapy has become an increasingly used adjunctive therapy in a variety of clinical settings, and has been investigated in the consideration of a treatment for PONV. Ginger is believed to be an effective option in the management of nausea and vomiting. This study investigated the effectiveness of aromatherapy with ginger essential oil for the treatment of PONV, as well as the efficacy over a longer period as measured by the level of PONV at 6, 12, and 24 h after aromatherapy administration. A significant difference in the level of PONV was found between the ginger essential oil and normal saline inhalation groups. It was also found that although overall PONV decreased over time in both groups, PONV was significantly reduced in the ginger essential oil aromatherapy group. Moreover, the notable change in the mean PONV scores in the experimental group was found at 6 h after aromatherapy administration, and the lower levels of PONV remained until the end of the 24 h aromatherapy with ginger essential oil. Findings from this study indicate that inhaled aromatherapy with ginger essential oil is effective in reducing nausea and vomiting within the first 24 h after surgery.
The result of this study supports the results of previous studies: inhaling ginger essence has a positive effect on postoperative nausea and vomiting by lowering the mean nausea intensity and the numbers of vomiting episodes. 35,36 The study of Hunt et al. showed that the ginger or blend aromatherapy significantly reduced the level of postoperative nausea and the number of anti-emetic medications requested. 29 In addition, the post-discharge nausea in patients undergoing outpatient abdominal surgery was decreased by the aromatherapy product QueaseEASE. 37
Though not an inhalation method, a previous study with 120 gynecologic surgery patients found significant decreases in PONV at 2 and 6 h after surgery when patients took two capsules of ginger (0.5 g of ginger powder) 1 h before surgery. 28 Findings from a previous randomized trial were consistent with those of the present study that patients who received aromatherapy with ginger essential oil reported significantly lower nausea compared with those receiving normal saline. 29 Because the subjects of this study were the patients who fasted after abdominal surgery, ginger essential oil was provided as an inhalation substance via a necklace instead of oral medication, so it is difficult to compare the effectiveness of ginger essential oil due to the different application methods. Therefore, more research is needed to provide substantial scientific evidence on the effectiveness of aromatherapy with ginger essential oil for the prevention and management of PONV.
This study has several limitations. The study findings cannot be generalized because the sample was limited to a hospital in Korea. The research design for this study is not ideal. Although it may not be possible to blind both researchers and patients completely because of the scent of the essential oil, further research with a better research design (e.g., randomized controlled trial) and a larger sample is needed. This study used a reliable and valid instrument to measure the level of PONV. However, data were collected by research assistants, which might lead to potential observation bias, even though they were all trained in the data-collection procedures. Although the research assistants checked patients every 2 h regarding all aspects of aromatherapy, including any side effects and patients' comfort levels, the first assessment of the level of PONV was done at 6 h after implementing the aromatherapy on the unit. It is unclear at what point ginger essential oil was effective within the first 6 h after inhaled aromatherapy administration. Further research is needed to develop more effective options for aromatherapy with ginger essential oil, including a shorter interval of measurements on PONV and different doses, duration, and types (blended or single oil) of ginger essential oil. Moreover, this study did not examine whether ginger essential oil would be effective in reducing nausea and vomiting during the recovery period in the PACU. Baseline data on the level of PONV were collected from patients immediately before transfer to their units. It was difficult to capture the actual initial levels of nausea and vomiting after surgery while patients were recovering from anesthesia.
Conclusions
Despite significant advances in the management of PONV, there is still no consensus on the optimal prevention and treatment. A multimodal approach has been strongly recommended, including both pharmacological and non-pharmacological treatments. The present findings that inhaled aromatherapy using ginger essential oil promotes reduced nausea and vomiting after major abdominal surgery provide additional support that ginger essential oil is helpful to treat PONV. In addition to its advantage as a noninvasive method of administration, ginger essential oil is relatively inexpensive and easy to administer, and has minimal known side effects. Aromatherapy with ginger essential oil can serve as a promising treatment option to prevent and manage nausea and vomiting after surgery.
Footnotes
Acknowledgments
The authors are grateful to all the participants from the Department of Stomach and Liver Surgery, ASAN Medical Center, Seoul, South Korea.
Author Disclosure Statement
All authors declare that they have no conflicts of interest.