
Abstract
Introduction:
Insurance reimbursement for clinical services provided by complementary healthcare professionals in the United States likely differs by provider specialty. It is hypothesized that a lower likelihood of insurance reimbursement demonstrates that complementary healthcare services are not utilized to an optimal level and are not financially accessible to all who may need or want these services. The purpose of this project was to evaluate the likelihood of insurance reimbursement for complementary healthcare services compared with other complementary services and with conventional primary care medical services in New Hampshire.
Methods:
The authors studied health claims for services provided in a nonemergent outpatient setting in New Hampshire in 2014. The study population consisted of New Hampshire residents aged 18–99 years with claims for selected clinical services commonly provided by complementary healthcare providers. The authors modeled the proportion of reimbursed claims by specialty of complementary healthcare service provider, compared with the reimbursement rate for primary care physicians' claims. The authors modeled first for the proportion of reimbursement for any selected clinical service, next for any evaluation and management (E&M) service, and finally for the most commonly used E&M procedure code, current procedural terminology (CPT) 99213 (reevaluation of established patient).
Results:
Compared with primary care physicians, the likelihood of reimbursement for any service was 69% lower for acupuncturists, 71% lower for doctors of chiropractic medicine, and 62% lower for doctors of naturopathic medicine. For any E&M service, likelihood of reimbursement was 69% lower for acupuncturists, 78% lower for doctors of chiropractic medicine, and 60% lower for doctors of naturopathic medicine. With further restriction to CPT 99213 only, likelihood of reimbursement was 34% lower for acupuncturists, 77% lower for doctors of chiropractic medicine, and 60% lower for doctors of naturopathic medicine.
Conclusions:
In New Hampshire, the likelihood of health insurance reimbursement for certain clinical services differs significantly by provider specialty. More research is needed to evaluate the extent and cause of such differences and the effect of such differences on the utilization of complementary healthcare services in the United States.
Introduction
E
All U.S. states license doctors of chiropractic medicine, and ∼85% of states license other types of complementary healthcare practitioners, including doctors of naturopathic medicine, acupuncturists, and massage therapists. 3 The costs of many complementary healthcare services are not reimbursed by health insurance plans and therefore the costs of care are often paid out of pocket by those who wish to receive such services. 4 In 2012, 60% of U.S. adult recipients of chiropractic care had insurance coverage for the services they received, compared with a 25% rate of coverage for recipients of acupuncture and a 15% rate of coverage for recipients of massage therapy. 5
The effect of differences in insurance reimbursement on the utilization of complementary healthcare services in the United States is largely unknown. In the state of Washington, which requires private health insurers to cover the services of licensed complementary healthcare providers, a cross-sectional analysis of health claims revealed that compared with national utilization rates, Washington state residents had fewer claims for massage therapy, a similar proportion of claims for acupuncture, and a greater proportion of claims for naturopathic and chiropractic care. 3 Secondary analysis of data from a randomized controlled trial of the effect of cost sharing on utilization of healthcare services revealed that utilization of chiropractic care is very sensitive to consumer costs. 6
It is possible that lower likelihood of insurance reimbursement could discourage utilization and lead to disparities in access to complementary healthcare services that patients need and want. However, little is known about the occurrence of differences in insurance reimbursement for complementary healthcare services compared with conventional medical services.
The purpose of this project was to evaluate the likelihood of insurance reimbursement for complementary healthcare services in New Hampshire, a suitable venue for this study, because the state licenses several types of complementary healthcare providers and is one of the few U.S. states that systematically collect data derived from health claims and release those data for research purposes. The results of this study will inform the efforts of healthcare consumers, providers, payers, and policy makers engaged in monitoring progress toward the achievement of equity in patient access to complementary healthcare services.
Methods
The authors conducted a retrospective study of commercial health system claims data. They reviewed claims by selected current procedural terminology (CPT)® code; diagnoses were not considered in the quantitative evaluation. They evaluated services provided by both complementary healthcare providers and conventional primary care medical physicians in nonemergent outpatient settings in New Hampshire during 2014. Points of service included office visits, walk-in retail health clinics, urgent care facilities, birthing centers, community health centers, and public health or rural health clinics.
This project was conducted subject to the terms of data user agreement between the investigator and the state of New Hampshire. The research methods were reviewed and approved by the institutional review board of the investigator's university. All statistical analyses were performed using SAS (SAS Institute, Cary, NC).
The data source was the all-payer claims database administered by the Department of Health and Human Services of the state of New Hampshire, which aggregates health claims data submitted by 26 private and public third-party payers, including preferred provider organizations, health maintenance organizations, and indemnity insurance plans. No Medicare or Medicaid claims were included in the database.
The authors employed a cross-sectional design to analyze data for one calendar year (2014). The study population consisted of residents of New Hampshire aged 18–99 years, insured under a health plan regulated by the state of New Hampshire, with claims for specified clinical services provided in New Hampshire by clinicians in certain provider specialty categories.
The clinicians were categorized according to self-reported specialty, as recorded in the provider metadata file of the health claims database. The provider specialty category, Primary Care Physicians, included physicians with self-reported specialty of Family Medicine, Internal Medicine, or General Practice. The provider specialty category, Complementary Healthcare Professionals, included clinicians with self-reported specialization in one of the five licensed complementary health disciplines with a federally recognized accrediting agency: acupuncture, chiropractic, direct entry midwifery, massage therapy, and naturopathic medicine. 7
The authors analyzed by CPT codes for selected clinical services commonly provided by complementary healthcare providers (including acupuncture, biofeedback, evaluation and management (E&M) services, manipulative therapy, manual therapies, nutritional therapy, physical therapy, and wellness and prevention services) and compared the following outcomes by provider and payer categories: utilization of clinical services, spending on clinical services, and proportion of reimbursed claims for clinical services. The fundamental unit of analysis was the claim line, which equates with a single clinical service, defined by CPT code.
For evaluation of the utilization of clinical services and spending on clinical services, the authors restricted the analyses to claims for E&M services. E&M procedures are key features of the clinical practices of all healthcare professionals, both conventional and complementary, and are the most commonly performed clinical services among all categories of providers. The authors evaluated by provider specialty category for providers of E&M services per 10,000 unique patients, utilization (E&M services per 10,000 unique patients), and spending (expenditures for E&M services per patient).
The authors modeled the likelihood of reimbursed claims for clinical services by specialty of complementary healthcare service provider, compared with the likelihood of reimbursement for primary care physicians' claims. Reimbursement was defined as health insurance claim payment greater than zero dollars.
A generalized estimating equation model was used to account for within-person correlations among the separate claim reimbursement indicators for individuals used in the analysis, using an exchangeable working covariance structure among claims for the same individual. All calculations were performed with SAS PROC GENMOD. 8 The authors modeled first for the proportion of reimbursement for any selected clinical service, next for any E&M service, and finally for the most commonly used E&M procedure code, CPT 99213 (reevaluation of established patient).
Results
A total of 1277 healthcare professionals, including 910 primary care physicians, 425 doctors of chiropractic medicine, 28 doctors of naturopathic medicine, 19 acupuncturists, and one direct entry midwife, provided E&M services to 130,227 unique patients. Payers included preferred provider organizations (covering 49% of beneficiaries), health maintenance organizations (28%), indemnity insurance plans (7%), and other payer types (16%).
Services provided by primary care physicians accounted for 98% of all E&M reimbursement dollars. Of the remaining 2%, 63% went to doctors of chiropractic medicine, 34% to doctors of naturopathic medicine, 2% to acupuncturists, and <1% to direct entry midwives. The authors found no reimbursed claims for E&M services rendered by massage therapists (Fig. 1). Conventional primary care physicians also dominated statistics on utilization and per-patient spending for E&M services (Table 1).
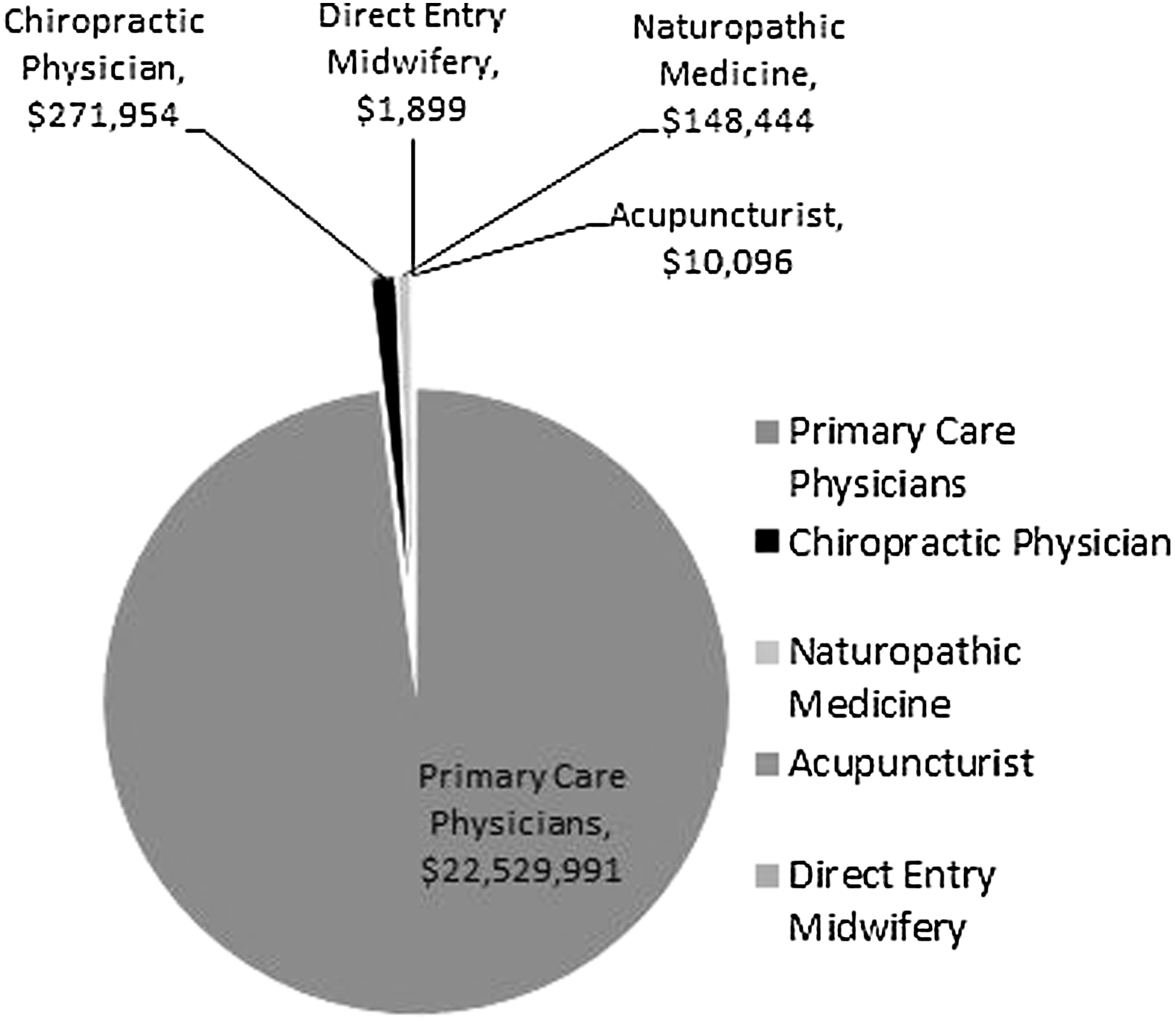
Spending on evaluation and management services in New Hampshire by selected provider specialty categories, 2014.
Availability = providers of E&M services per 10,000 patients.
Utilization = E&M services per 10,000 patients.
Spending = expenditures for E&M services per patient.
E&M, evaluation and management.
The likelihood of reimbursement for clinical services of selected provider specialty categories may be viewed in Table 2. Compared with primary care physicians, the likelihood of reimbursement for any clinical service was 69% lower for acupuncturists, 71% lower for doctors of chiropractic medicine, and 62% lower for doctors of naturopathic medicine. When the authors restricted the analysis to any E&M service, likelihood of reimbursement was 69% lower for acupuncturists, 78% lower for doctors of chiropractic medicine, and 60% lower for doctors of naturopathic medicine. With further restriction to CPT 99213 only, likelihood of reimbursement was 34% lower for acupuncturists, 77% lower for doctors of chiropractic medicine, and 60% lower for doctors of naturopathic medicine. A paucity of claims data for services of direct entry midwives precluded analysis for likelihood of reimbursement.
CPT, current procedural terminology.
Discussion
Limitations
The authors caution that likelihood of reimbursement must be distinguished from amount of reimbursement; which often differs by specialty due to differences in relative value units. Because it is impossible from analysis of claims data to determine the percentage of services rendered for which claims were submitted, utilization may have been underestimated. Unmeasured factors may account for the observed differences in rates of reimbursement, including type of condition, (the specific International Classification of Diseases, 9th revision-defined conditions diagnosed in the set of 130,277 patients), scope of practice and training impacting ability of providers to accept patients, appropriateness of coding, and medical necessity of service.
The results may be associated with differences in provider credentialing: in the examination of the data, the authors noted the possibility of a positive correlation between lack of National Provider Identifier and low likelihood of reimbursement. If a provider submits a claim for reimbursement from an Health Maintenance Organization or other restricted health plan in which he or she is not enrolled, the insurer may justifiably deny payment. Complementary healthcare professionals who are new to health plan participation may be less skilled in obtaining insurance reimbursement than their more experienced medical colleagues.
Implications
Among the selected categories of healthcare providers in New Hampshire, the vast majority of claims for E&M services in nonemergent outpatient settings were accounted for by the services of conventional primary care physicians. Complementary healthcare professionals other than massage therapists did receive reimbursement for E&M services, but the likelihood of reimbursement was lower compared with primary care physicians.
The reported differences in reimbursement by provider specialty may have resulted from systematic differences in policy or payer practices. Systematic differences in health plan coverage are allowable under the Employees Retirement Income Security Act and federal health plans, including Medicare. Systematic differences in payer practices may take the form of benefit design features such as caps on the number of allowable visits per member per year or caps on total expenditures per member per year.
The Affordable Care Act (ACA) prohibits discrimination in insurance coverage by specialty of healthcare provider. Section 2706 of the ACA states, “A group health plan and a health insurance issuer offering group or individual health insurance coverage shall not discriminate with respect to participation under the plan or coverage against any health care provider who is acting within the scope of that provider's license or certification under applicable state law.” 9
The business practices of health insurers are regulated by the states, and differences between states in the implementation of Section 2706 have been reported. 10 Thus, differences by provider specialty in health insurance coverage and reimbursement may persist despite the nondiscrimination mandate of Section 2706. The licensed health professionals belonging to the specialties included in this study were all authorized in the state of New Hampshire to provide E&M services. 11 –15 The cause of the observed differences is therefore uncertain.
Regardless of the reason or mechanism by which differences in reimbursement occur, the lack of reliable health insurance reimbursement for services that people need and want may lead to inequitable healthcare access and higher costs. The authors recommend further research to evaluate for differences in reimbursement by provider specialty across various categories of services and variations across U.S. states, applying rigorous methods for unbiased identification of the causes of such differences, and testing the hypothesis that differences in health insurance reimbursement by provider specialty limit access to healthcare services that people need and want.
Conclusions
In New Hampshire, the likelihood of health insurance reimbursement for certain clinical services differs significantly by provider specialty. More research is needed to evaluate the extent and cause of such differences and the effect of such differences on the utilization of complementary healthcare services in the United States.
Footnotes
Acknowledgments
All analysis, conclusions, and recommendations reported in this article are solely those of the author.
Author Disclosure Statement
No competing financial interests exist.