
Abstract
Introduction:
Acupuncture as one of the alternative therapies for insomnia is widely used in Asia and increasingly employed in western countries.
Objectives:
To provide updated evidence from randomized controlled trials (RCTs) on the effectiveness and safety of acupuncture for primary insomnia.
Methods:
A comprehensive literature search in 11 databases was conducted from January 2008 to October 2017. Two authors independently extracted data and assessed risk of bias independently. Statistical analysis was performed using RevMan 5.3 software. According to predefined protocol, we combined data in meta-analysis and performed trial sequential analysis when appropriate. Grading of Recommendations Assessment, Development, and Evaluation was also conducted to assess the quality of evidence.
Results:
A total of 73 RCTs involving 5533 participants were analyzed. The pooled results showed better effect from real acupuncture than no treatment (mean difference [MD] −5.58, 95% confidence interval [CI] −6.85 to −4.31, I 2 = 0%, p < 0.00001, 2 trials, fixed effect model, 105 participants) on reducing Pittsburgh Sleep Quality Index (PSQI) scores with “very low quality” evidence. Acupuncture plus drugs showed better improvement than drugs alone on decreasing the PSQI total scores (MD −3.17, 95% CI −4.74 to −1.61, I2 = 72%, 4 trials, random-effects model (REM), p < 0.0001, 253 participants, low quality). Similar benefit favored acupuncture compared with no treatment (MD −8.46, 95% CI −9.59 to −7.33, I2 = 0%, p < 0.00001, 2 trials, 65 participants). Acupuncture showed more benefit than estazolam on PSQI (with enough statistical power). Athens Insomnia Scale (MD −1.64, 95% CI −2.40 to −0.89, I2 = 0%, p < 0.0001, 3 trials, fixed-effects model, 180 participants) or SPIEGEL (MD −2.86, 95% CI −3.54 to −2.18, p < 0.00001, I2 = 0%, 5 trials, fixed-effects model, 326 participants) with “very low-quality” evidence. Furthermore, low-quality evidence showed less adverse events from acupuncture than western medications (risk ratio 0.23, 95% CI 0.11–0.48, I2 = 56%, p < 0.0001, 11 trials, REM, 914 participants). Publication bias was likely present based on the PSQI total scores.
Conclusions:
The summary estimates indicate that acupuncture might result in improvement than no treatment on PSQI scores and appears safe. However, the quality of the evidence is varied from very low to low due to the potential risk of bias and inconsistency among included trials. Further large sample size and rigorously designed RCTs are still needed.
Introduction
Insomnia is a subjective experience characterized by impairment of the ability to initiate or maintain sleep and result in significant impairment in daily function. 1,2 Approximately 35%–50% of adults experience unsatisfactory sleep, 3 and 12%–20% of these individuals suffer from insomnia disorder. 4,5 In China, insomnia affects about 42.5% adults. 6
Insomnia treatments include cognitive behavioral therapy (CBT) and medication treatment. 7 CBT, as a multicomponent behavioral intervention, which provides sleep education, stimulus control (strengthening associations between bed and sleep), and therapy for anxiety-provoking beliefs about sleep, is now commonly recommended as a first-line treatment for chronic insomnia disorder (Grading of Recommendations Assessment, Development, and Evaluation [GRADE]: strong recommendation, moderate-quality evidence), since CBT produces sleep improvements that are sustained over time. 8,9 Pharmacologic interventions are often prescribed for insomnia disorder, including benzodiazepines and other nonbenzodiazepine hypnotics.
Although CBT and medications may help to alleviate symptoms, both of them have limitations. Since insomnia is a chronic condition, CBT is not accepted by patients completely in the long run and also not readily available in most clinical settings. Medications may cause undesirable adverse effects, including morning sedation, anterograde amnesia, anxiety, or other cognitive and behavioral changes, such as sleepwalking, sleep-related eating, etc. 7,10 Thus, more and more patients seek for alternative therapies.
Acupuncture treatment for insomnia was widely applied and reported. 11 –15 The potential mechanism of acupuncture is difficult to scientifically understand or measure, such as the invisible energy of chi in the body. Preliminary evidence based on experimental studies suggests that acupuncture works in many cases, has theorized that the energy meridians are actually part of the nervous system, and that acupuncture improves insomnia by cholinergic activation, stimulation of the opioidergic neurons to increase the concentrations of β-endorphin, and the involvement of the μ-opioid receptors. 16 Although the mechanism of acupuncture is still unclear, this treatment continues to show effectiveness in clinical studies on alleviating the symptoms of insomnia, and number of researches in acupuncture in treating insomnia is currently growing.
However, no confirmative benefit of acupuncture treating for insomnia could be drawn from our published systematic review in 2009 (46 trials, 3811 patients, searched until 2008) yet, mainly due to inadequate sample sizes and poor methodology. 17 Since more randomized controlled trials (RCTs) were published in the past 9 years, we conducted this systematic review to provide up-to-date evidence-based evaluation on the effectiveness and safety of acupuncture as a monotherapy or in combination with other therapy in treating primary insomnia.
Materials and Methods
Study registration
The protocol of this systematic review was registered at PROSPERO (CRD42016039642): YU Mei-Li, Cao Hui-Juan, Wang Li-Qiong, Fei Yu-Tong, Liu Jian-Ping, and Xu Hao. Acupuncture for primary insomnia: an updated systematic review of randomized controlled trials. The following was a brief introduction of methods.
Inclusion criteria
Primary insomnia is defined as chronic and persistent difficulty in either falling asleep, remaining asleep through the night, or waking up too early at least three nights a week for more than a month, and not suffered from any secondary diseases. 18,19 RCTs which compared acupuncture (any forms of needles invaded into the skin and retaining needle for at least 15 min) with no treatment, sham acupuncture, conventional therapy, or western medications for primary insomnia were included. Acupuncture combined with other treatments compared with the same treatments was also included. The primary outcome is the overall quality of sleep measured by internationally recognized sleep quality scales, including Pittsburgh Sleep Quality Index (PSQI), Athens Insomnia Scale (AIS) and SPIEGEL. PSQI consists of 19 items in 7 factors and the total scores range from 0 to 21. The total scores of AIS range from 0 to 24 and SPIEGEL is 0 to 30. A higher score indicates worse sleep quality. Secondary outcomes include sleep parameters, which include subjective sleep quality, sleep onset latency, sleep duration, sleep efficiency, sleep disturbance, and daytime dysfunction, measured by objective measurements or sleep scores about PSQI sub-items (each item scored 0 to 3 and a lower score is better), and quality of life measured by validated scales. Adverse events were reported as safety outcome. Included trials must report at least one of the primary outcomes or at least the first two secondary outcomes or adverse events.
Search strategy
An up-to-date comprehensive search was conducted in four Chinese databases and six English databases, including PubMed, EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), PsycINFO, The Allied and Complementary Medicine Database (AMED), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Chinese National Knowledge Infrastructure Databases (CNKI), Chinese Biomedical Literature Database (SinoMed), Chongqing VIP Chinese Science and Technology Periodical Database (VIP), and Wanfang Database. Search time was from January 2008 to October 2017. The searching strategy and results are listed in Appendix Table A1 for details.
Study selection and quality assessment
Two authors selected the eligible studies and extract data independently and assessed the methodological quality of included trials using the risk of bias tool. 20 The GRADE and the standards for reporting interventions in controlled trials of acupuncture (STRICTA) checklist were used to assess the quality of evidence and completeness and reporting quality of acupuncture intervention. 21
Trial sequential analysis (TSA) was also performed if there were more than eight included studies in the meta-analysis. We applied TSA version 0.9.5.5 (Copenhagen: The Copenhagen Trial Unit, Center for Clinical Intervention Research, 2016) to calculate the required sample size in a meta-analysis and to detect the robustness of the result. We used the diversity-adjusted required information size estimated from a control event proportion of the included trials and a priori intervention effect of 5%, and the diversity which was estimated in the included trials.
Data analyses
All statistical analyses were performed using RevMan 5.3 software. Data were summarized using risk ratio (RR) with its 95% confidence interval (CI) for binary outcomes or mean difference (MD) with 95% CI for continuous outcomes. Meta-analysis would be conducted with data from eligible included trials; subgroup analysis and sensitive analysis were also planned to be conducted when data were available. Details of the data analysis methods were also described in the registered protocol.
Results
Description of the included trials
A total of 73 RCTs were included in the review. The flow chart of study searching and screening is shown in Figure 1.

Flow chart of study search and selection. Preferred reporting items for systematic review and meta-analysis (PRISMA). RCTs, randomized controlled trials.
The random methods of 24 trials were confirmed by original authors (contacted by telephone or e-mails) and the authors for the other 49 trials were failed to contact to verify the randomization procedure. All of the included trials were published in Chinese and conducted in China with a total of 5533 participants (2785 in the intervention group and 2748 in the control group). The sample sizes of all included trials varied from 22 to 196 participants (10–98 participants in each group). There was a wide variation in the age of subjects (18–60 years) and disease duration (30 days to 18 years). The treatment duration ranged from 7 to 60 days.
Acupuncture was used alone or combined with medications in the included trials. Needle types included manual acupuncture (51 trials), 22 –72 electroacupuncture (14 trials), 73 –86 scalp acupuncture (6 trials), 87 –92 wrist–ankle acupuncture (1 trial), 93 and eye acupuncture (1 trial). 53 The controls included medication (70 trials), sham acupuncture (needles were located at the same acupoints with accessory device, but were not inserted into the skin) (1 trial), 94 or no treatment (2 trials). 31,88
Most of the included trials used semistructured prescription of the points. The number of the selected acupoints ranged from 2 to 20, and the top 10 commonly used acupoints were Baihui (GV20), Sishencong (EX-HN1), Shenmen (HT7), Sanyinjiao (SP6), Anmian (EX-HN22), Neiguan (PC6), Taichong (LR3), Shenting (GV24), Zhaohai (KI6), and Yintang (GV29). The top three meridians with the most selected points were Dumeridian, HandShaoyin meridian, and HandJueyin meridian.
Sixty-nine trials used the PSQI scores as the outcome measure. SPIEGEL 25,39,70,74,83 and AIS 25,70,74 were also reported. Twenty-six trials reported sleep parameters and daytime functioning, which are sub-items of PSQI score. Sleep onset latency was reported in three trials 57,84,88 and one trial 88 reported quality of life measured by the Medical Outcomes Study item short form health survey (SF-36). Seventeen of the included trials 25,26,28,31,32,38,42,48,50,66,67,81,83,85,88,89,94 mentioned the safety issue. Twelve trials reported data of adverse events and the remaining five trials 32,48,66,67,88 mentioned no adverse events. Five trials 26,30,88,90,94 mentioned the follow-up duration of post-treatment, which varied from 7 to 90 days. Characteristics of the 73 included trials are listed in Appendix Table A2.
Methodology quality assessment
Risk of bias of included trials
Ten 24,26,28,30,73,74,87,88,89,94 of the included trials were judged as high quality (at least 4 of 7 items were assessed as low risk of bias, which were strictly designed with randomization, must be included). Twenty-four of included trials used proper methods to generate randomization sequence and this was confirmed by the original authors through telephone/emails. Sixteen trials failed to contact but are described in the articles that random sequence was generated by random number table. Fourteen trials 24,26,28 –30,32,34,73 –75,87–89,94 described methods of allocation concealment. Only one trial 94 used sham acupuncture as control and was assessed as low risk of bias on blinding to participants. Six trials 25,26,71,73,88,94 used the third party to evaluate the outcome indicators and were assessed as low risk of bias on blinding of outcome assessors. Thirty-two trials 26,29,34,38,39 –43,45,46,49 –51,57,58,60,62 –66,68,70,78 –80,82,84,85,91,93 were assessed as unclear of bias on the item of incomplete outcome data, since there were dropouts (less than 5% of the total) excluded from analyses. Baseline characteristics were comparable between the two groups, but the reason of the dropout was not provided and not performed by the intention-to-treat analysis. Other 41 trials 22 –25,27,28,30 –33,35–37,44,48,52 –56,59,61,67,69,71 –77,81,83,86 –90,92,94,95 reported no dropouts and assessed as low risk of bias. Protocol of all included trials could not be accessible, but we assessed them as having low risk of reporting bias, since they all reported the important outcome measurements for insomnia. Twenty-four trials 26,39,41,44,46,48,49,52,54,55,58,59,61,62,64,67,77,80,81,83,88,90,93,94 were assessed as low risk of other bias by the good baseline comparability, detailed descriptions on inclusion/exclusion criteria, and adequate follow-up. However, none of the included trials reported sample size calculations, essential for ensuring adequate statistical power, or described the funding issue. We evaluated the remaining trials as having an unclear risk of other bias. Risk of bias graph of 73 included trials is shown in Figure 2.
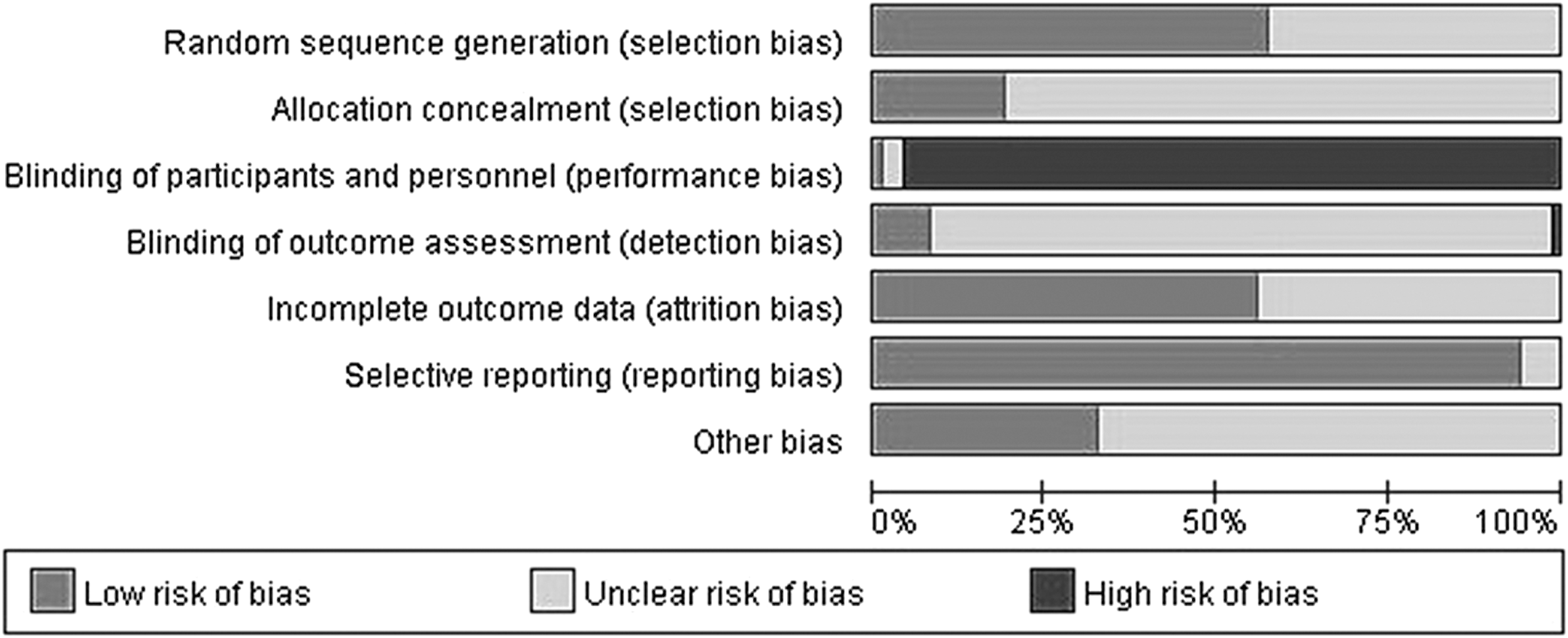
Risk of bias graph of 73 included studies.
STRICTA assessment of 73 included trials
Almost all of the included trials (98.63%) had detailed descriptions on acupuncture rationale and treatment regimen. More than 69.49% trials provided a comprehensive description on the needling details. At least 68 trials (93.15%) have reported a precise description of the control interventions. However, for practitioner background, only four of the trials (5.48%) described, but insufficiently (only mentioned performed by professional acupuncturist, but their professional affiliation, years in acupuncture practice, or other relevant experience were not described in detail). According to predefined inclusion criteria, only acupuncture therapy was included and all of include trials do not need to be reported on the item of other interventions. The detailed assessment results are summarized in Table 1.
Checklist of 73 Included Trials for Items in STRICTA 2010
STRICTA, Standards for Reporting Interventions in Controlled Trials of Acupuncture.
Estimate Effects of Acupuncture for Primary Insomnia
Comparison 1: acupuncture versus no treatment
Overall quality of sleep
The pooled results of two trials 27,34 compared with no treatment showed significant difference in decreasing the PSQI total scores (MD −5.58, 95% CI −6.85 to −4.31, I 2 = 0%, p < 0.00001, 105 participants, very low-quality) (Appendix Table A3).
Quality of life
One trial 27 reported that acupuncture had an improvement in the physical component scores compared to no treatment on the SF-36 (MD 197.57, 95% CI 148.40 to 246.74, p < 0.00001, 1 trial, 65 participants).
Sleep onset latency
One trial 27 reported sleep onset latency detected by monitoring devices, and the results showed acupuncture had at least 40 min shorter sleep onset latency than no treatment (MD −40.42 min, 95% CI −50.84 min to −30 min, p < 0.001, 1 trial, 65 participants).
Comparison 2: acupuncture versus sham acupuncture
Overall quality of sleep
One trial 94 showed that real acupuncture reduced more PSQI total scores than sham acupuncture (MD −8.46, 95% CI −9.59 to −7.33, p < 0.00001, 1 trial, 65 participants).
Sleep parameters
The trial 94 reported that real acupuncture was more likely to have improvement in PSQI sub-items, including the subjective sleep quality, sleep onset latency, sleep duration, sleep efficiency, sleep disturbance, and daytime dysfunction (MD −0.43 to −1.78, p < 0.0001).
Comparison 3: acupuncture plus estazolam versus estazolam alone
Overall quality of sleep
The pooled results of four trials 29,30,54,62 found a better effect of the intervention group on PSQI total scores compared with the control group (MD −3.17, 95% CI −4.74 to −1.61, I 2 = 72%, p < 0.0001, four trials, random-effects model (REM), 253 participants, low quality) (Appendix Table A3).
One trial 30 showed similar result measured by AIS (MD −1.06, 95% CI −1.75 to −0.37, p = 0.003, 1 trial, 70 participants) and Epworth Sleepiness Scale (MD −2.73, 95% CI −4.56 to −0.90, p = 0.004, 1 trial, 70 participants).
Comparison 4: acupuncture versus western drugs
Overall quality of sleep
According to the different types of sedatives and hypnotics, we conducted two subgroup analyses to compare acupuncture with benzodiazepines and nonbenzodiazepines, respectively.
Subgroup 1: Acupuncture versus benzodiazepines
The pooled results of 32 trials showed that acupuncture had a better effect on decreasing the PSQI total scores than estazolam (1 mg once daily) (MD −1.73, 95% CI −2.11 to −1.35, I 2 = 69%, REM, p < 0.00001, 32 trials, 2452 participants, very low quality). With increasing dose of estazolam, the differences of curative effect between acupuncture and estazolam was getting smaller. When 2–4 mg of estazolam was used, the results of two trials were smaller compared with the difference between acupuncture and 1 mg estazolam (MD −1.54, 95% CI −1.87 to −1.20, p < 0.00001, 2 trials, 142 participants) (Supplementary Fig. S1).
The pooled results of five trials 24,50,56,75,82 showed that manual acupuncture had a better effect on decreasing PSQI total scores than estazolam with 2 mg (MD −1.30, 95% CI −2.31 to −0.30, I 2 = 67%, p < 0.01, 5 trials, REM, 328 participants) (Supplementary Fig. S1). The results of electroacupuncture and scalp acupuncture were not pooled due to high heterogeneity (I 2 > 75%), and the result showed a better effect compared with estazolam. Other five trials 48,65,66,79,87,88 with other benzodiazepines (alprazolam, chlordiazepoxide, diazepam, clonazepam) reported the similar result. The results of individual trials are shown in Appendix Table A3.
The pooled results of three trials 25,70,74 showed that acupuncture had a better improvement on the overall quality of sleep than estazolam measured by AIS (MD −1.64, 95% CI −2.40 to −0.89, p < 0.0001, 180 participants, low quality) and SPIEGEL (MD −2.86, 95% CI −3.54 to −2.18, p < 0.00001, 326 participants, low quality) (Appendix Table A3).
Subgroup 2: Acupuncture versus nonbenzodiazepines
Nine trials compared acupuncture with nonbenzodiazepines, including trazodone, zolpidem, oryzanol, zopiclone, and melatonin. The results of meta-analysis found a minor effect of acupuncture in decreasing the PSQI total scores than nonbenzodiazepines (MD −0.94, 95% CI −1.55 to −0.33, I 2 = 46%, p = 0.003, 9 trials, REM, 643 participants, very low quality) (Appendix Table A3).
Sleep parameters
The pooled results of 21 trials
26,27,33
–35,43,50,51,59,66
–68,69,73,76,77,79,81,83,84,89
on sleep parameters measured with PSQI sub-items reported that acupuncture had some improvement than benzodiazepines in terms of subjective sleep quality (MD −0.32, 95% CI −0.41 to −0.23, I
2
= 68%, p < 0.00001, REM, 1812 participants), sleep efficiency (MD −0.25, 95% CI −0.36 to −0.15, p < 0.00001, I
2 = 63%, 19 trials,
26,27,33
–35,43,50,51,59,66
–69,76,77,81,83,84,89
REM, 1618 participants), and sleep duration (MD −0.18, 95% CI −0.29 to −0.08, p < 0.0004, I
2 = 64%, 18 trials,
26,27,33,35,43,50,51,59,66
–69,76,77,81,83,84,89
REM, 1586 participants) (Supplementary Fig. S2). However, pooling analysis on sleep disturbance and daytime functioning were not used due to the significant statistical heterogeneity (I
2 >
Sleep onset latency
The results of sleep onset latency measured by PSQI sub-item were not pooled due to high heterogeneity (I 2 > 75%). The subgroup analysis results of 14 trials 26,27,33 –35,43,50,51,59,66 –69,81 showed that manual acupuncture had an improvement in the sleep onset latency than benzodiazepines (MD −0.35, 95% CI −0.47 to −0.23, I 2 = 65%, p < 0.001, REM, 1213 participants) (Appendix Table A6).
However, the pooled results of two trials 43,84 measured by monitoring devices showed no difference between acupuncture and benzodiazepines on this outcome (MD −0.86 min, 95% CI −3.70 to 5.42, p = 0.71, 110 participants).
Safety
Seventeen trials 25,26,28,31,32,38,42,48,50,66,67,81,83,85,88,89,94 reported outcome of adverse events. One trial 94 found no difference between real and sham acupuncture on frequency of adverse events (RR 1.43, 95% CI 0.29–6.92, 67 participants). Other five trials 32,48,66,67,88 comparing acupuncture with western medication reported no occurrence of adverse events. The remaining 16 trials compared acupuncture with western medication, 11 of which showed lower incidence of adverse events in acupuncture group than the western medication group (RR 0.23, 95% CI 0.11–0.48, I 2 = 56%, p < 0.0001, REM, 914 participants). The adverse events of acupuncture group were fainting, bleeding, dizziness, skin flushing, and so on. The adverse events in acupuncture group were fade fasting, which was recovery after removing the needles. The details of adverse events are listed in Appendix Table A7.
Assessment for Publication Bias
The funnel plots of 58 trials comparing acupuncture with western drugs for the outcome of PSQI total score was asymmetrical, suggesting publication bias (Supplementary Fig. S3).
An asymmetrical funnel plot of 21 trials comparing acupuncture with benzodiazepines in PSQI sub-items score is shown (Supplementary Fig. S4).
GRADE: Summary of Findings on Acupuncture for Insomnia
We summarized the main outcomes by using a GRADE system, and the results from low or very low-quality evidence showed acupuncture appeared more beneficial than western medications on PSQI reduction and moderate quality evidence showed acupuncture was superior to no treatment on this outcome as well. This was mainly due to the poor methodological quality and high heterogeneity among relevant trials. The details of GRADE summary of finding are shown in Table 2.
GRADE Summary of Finding
The basis for the assumed risk (e.g., the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
Blinding of participants and personnel (performance bias) was high risk of bias.
Allocation concealment (selection bias) and blinding of outcome assessment (detection bias) were unclear.
High heterogeneity.
The medicine of control was different.
There is a certain publication bias.
AIS, Athens Insomnia Scale; CI, confidence interval; GRADE, Grading of Recommendations Assessment, Development and Evaluation; PSQI, Pittsburgh Sleep Quality Index; RR, risk ratio.
Trial Sequential Analysis
We conducted TSA with the data from 2 meta-analyses, in which more than eight trials were included. One was conducted with data from 25 trials, which compared manual acupuncture with 1 mg estazolam on PSQI total scores' reduction. TSA illustrated the cumulative Z-curve across the traditional boundary of 5% significance (horizontal line) and the monitoring boundaries (inward sloping curves) (in Fig. 3a). After Liu YY 2014, the significance testing had been performed each time a new trial was added to the meta-analysis, which means the sample size achieved the required 244 participants and we had enough power to confirm the evidence (that the acupuncture may decrease 1.7 more PSQI total scores than estazolam 1 mg daily) controlling for the risk of random error.
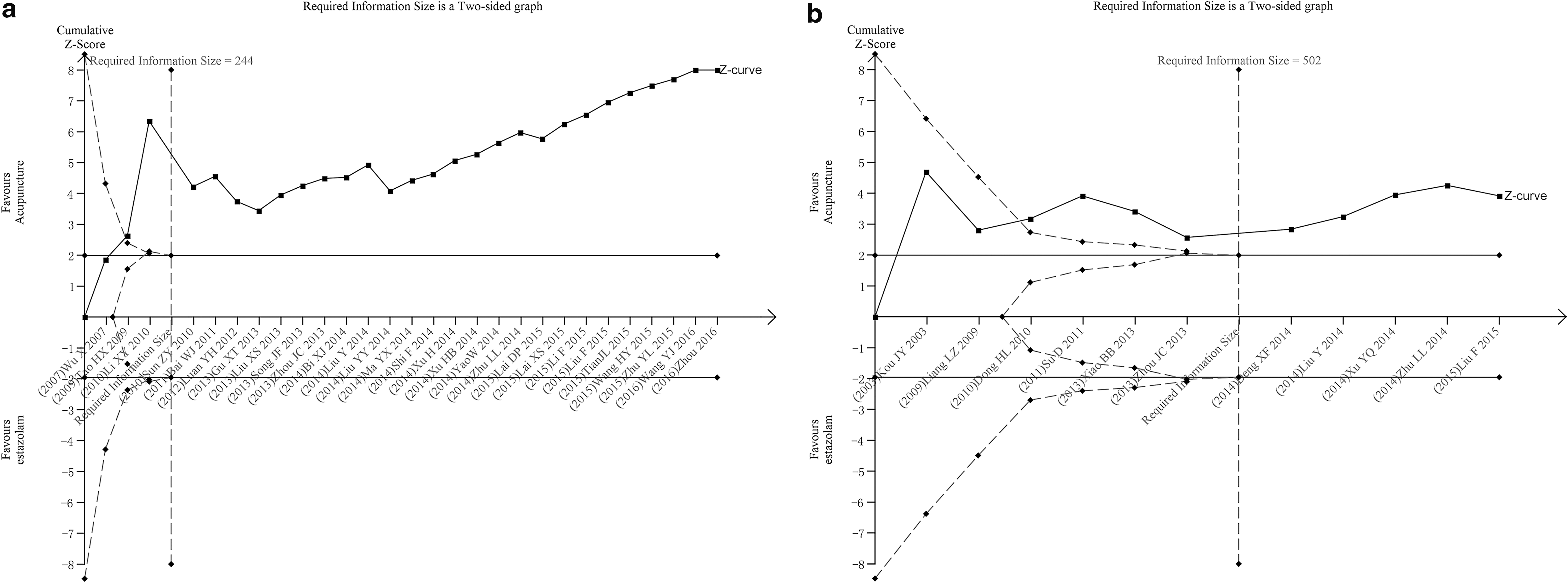
TSA of two meta-analyses compared manual acupuncture with estazolam 1 mg.
A similar result was shown in another TSA with data from 11 trials, which also compared acupuncture with estazolam on incidence rate of adverse events. TSA also illustrated the cumulative Z-curve across the horizontal line and the inward sloping curves (in Fig. 3b), which means the sample size achieved the required 502 participants and we had enough power to confirm the evidence (that the acupuncture may have 75% fewer adverse events than estazolam).
Discussion
Summary of findings
A total of 73 RCTs were included, and 10 of them were assessed as high quality according to risk of bias. For comparison of acupuncture with no treatment, sham acupuncture, or acupuncture plus estazolam compared with estazolam alone, the results showed acupuncture appeared to be more effective on decreasing PSQI total scores (range of MD from −3.17 to −8.46, low quality). Acupuncture showed better effect on decreasing the PSQI total scores than estazolam (very low quality), and the degree of decline is inversely proportional to the dose of estazolam. The pooled results also showed that acupuncture could improve patients' overall quality of sleep than benzodiazepines on AIS scale (low quality) and SPIEGEL scale (low-quality evidence).
For the secondary outcomes, the results of 21 trials showed positive effect of acupuncture on subjective sleep quality, sleep efficiency, and sleep duration than benzodiazepines. However, the scores of PSQI sub-items average decreased less than 0.5 score (MD −0.25 to −0.32) and might not be clinically relevant.
The results showed that the incidence of adverse events in acupuncture group was about a quarter of the western drugs group (low-quality evidence).
Limitation and strength
We had contacted the original authors to confirm the randomization procedure as far as possible. However, there were still 47 authors who failed to contact due to their personal reasons. Therefore, random sequence generation was not confirmed and blinding of acupuncturists and patients was hardly applied. Therefore, the quality of included trials was low.
Compared with the previous reviews, our study conducted an update comprehensive search and included 73 trials, which is the best-rounded systematic review of acupuncture treatment for primary insomnia yet. According to the STRICTA assessment, we conducted an assessment of acupuncture report quality of included trials. Although we draw a consistent conclusion with previous trials in terms of PSQI total score for comparisons between acupuncture and no treatment/sham acupuncture, we found a better effect of acupuncture for primary insomnia compared with estazolam (1 mg once daily). The incidence of adverse events was only a quarter than estazolam, which suggests acupuncture may reduce the dose of estazolam to avoid the side effect. This was supported by TSA results.
Implications for clinical practice
In this review, we included primary insomnia with disease courses more than a month. The baseline total scores of PSQI ranged from 12 to 19 (total scores >5 associated with poor sleep quality). 96 It can be seen from the results that acupuncture showed better improvement than no treatment or sham acupuncture on PSQI total score (by reducing 5–8 scores). Some research also suggests that increased risk of adverse effects of benzodiazepines would occur with high-dose drug. 97 So, for the insomniacs with no effect or inefficiency treated by the single drug therapy, the treatment of acupuncture-combined drug therapy may be a better choice. The top five acupoints used frequently were GV20, EX-HN1, HT7, EX-HN22, and GV24. The combinations of GV20 and EX-HN1, BL62 and KI6 were mostly used. According to the acupoints distribution, meridians, including Du meridian, Hand Shaoyin, and Hand Jueyin were selected more. Furthermore, this study suggests that acupuncture may get a better effect when the treatment course is more than 14 days. However, due to the inadequate follow-up, the conclusion needed further researches to be confirmed.
Implications for future research
According to the STRICTA assessment, less description was mentioned about the qualifications of researchers in the involved trials. Generally, acupuncturist who could participate in a clinical study in china should have a formal practicing certificate already. It is necessary to pay attention to the important role of researchers in the clinical curative effect of acupuncture. Meanwhile, researchers are encouraged to register their study protocols before trial implementation to ensure a high standard of research is maintained so that valid conclusions may be generated.
Future researches are urged to use more rigorous methodology, including appropriate sample sizes and adequate follow-up with long-term duration. In the outcome assessment, the objective outcome may be better than personal satisfaction of improvement, such as recognized sleep scale (PSQI, AIS, etc.) or other monitoring facility, to confirm the conclusion less affected by subjective factors. Acupoint selection (the number or different position) might have an influence on the curative effect of acupuncture treatment for insomnia. The relationship between the dose of western medicine and the effect of acupuncture needs further investigation.
Conclusion
With the results of fifty more included trials and the TSA analysis, we would like to suggest that the clinicians may consider to use acupuncture alone or plus western drugs for patients with primary insomnia according to the actual situation of the patients. Of course, further large sample-size and rigorously designed RCTs are still needed (see PRISMA 2009 Checklist in Appendix Table A8).
Footnotes
Acknowledgments
The authors thank Dr. Xia Yun (affiliated to the Oriental Hospital, Beijing University of Chinese Medicine) for her guidance on the TSA methods used in this review. This work was partially supported by the National Natural Science Foundation of China (81673828) and Beijing Municipal Organization Department (2017000020124G292) to Hui-Juan Cao.
Author Disclosure Statement
No competing financial interests exist.
PRISMA 2009 Checklist
| Section/topic | # | Checklist item | Reported on page # |
|---|---|---|---|
|
|
|||
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | 1 |
|
|
|||
| Structured summary | 2 | Provide a structured summary, including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; and systematic review registration number. | 1–2 |
|
|
|||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | 2 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | 2 |
|
|
|||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information, including registration number. | 2 |
| Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. | 2 |
| Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | 3 |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | 3, Appendix 2 |
| Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). | 3 |
| Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. | 3 |
| Data items | 11 | List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. | 3 |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. | 3 |
| Summary measures | 13 | State the principal summary measures (e.g., risk ratio, difference in means). | 3–4 |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | 3–4 |
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). | 3 |
| Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were prespecified. | 3–4 |
|
|
|||
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. | 4, Figure1 |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | 4, Table 1 |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). | 4–5, Table 2, Figure2 |
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. | 5–6, table 3–7 |
| Synthesis of results | 21 | Present results of each meta-analysis done, including confidence intervals and measures of consistency. | 5–7, table 3–7 |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | 4 |
| Additional analysis | 23 | Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). | 5–7 |
|
|
|||
| Summary of evidence | 24 | Summarize the main findings, including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers). | 7–8 |
| Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias). | 8 |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence, and implications for future research. | 9 |
|
|
|||
| Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. | 9 |
From: Moher D, Liberati A, Tetzlaff J, Altman DG; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med 2009;6:e1000097.
For more information, visit:
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.