
Abstract
Objective:
This study aimed to determine the efficacy of preoperative administration of Jidabokuippo (JDI), a Kampo medicine, in treating postoperative pain after tooth extraction with mandible bone removal.
Design:
This single-blind, randomized controlled study was conducted among two groups of adult patients who were scheduled to undergo tooth extraction with mandible bone removal under general anesthesia. Patients were randomly assigned to either the JDI or control group.
Intervention:
Before surgery, the JDI group received JDI (7.5 g), whereas the control group did not receive any treatment. Patients and the evaluator were blinded to the treatment status. At 0, 1, 3, and 24 h after anesthesia recovery, an investigator recorded the severity of postoperative pain and nausea using a numeric rating scale (0, no pain or nausea; 10, worst imaginable pain or nausea). The number of patients who requested nonsteroidal anti-inflammatory drug (NSAID) and that of additional NSAID administration within 24 h from anesthesia recovery, and the time to the first NSAID request from anesthesia recovery was also measured.
Results:
The severity of postoperative pain was significantly lower in the JDI group compared with the control group at 3 and 24 h after anesthesia recovery (p < 0.001 each). Both the number of patients requesting NSAID and additional NSAID administration after anesthesia recovery were significantly smaller in the JDI group than in the control group (p = 0.006, p < 0.001). The time to first NSAID request from anesthesia recovery was significantly longer in the JDI group compared with control group (p < 0.001). The severity of nausea did not differ significantly between the groups. No significant side effects related to JDI were noted during the trial.
Conclusions:
JDI administration before general anesthesia effectively decreased the severity of postoperative pain after anesthesia recovery in patients who underwent tooth extraction with mandible bone removal.
Introduction
P
Jidabokuippo (JDI, TJ-89) is a Japanese Kampo medicine that has been used to treat bruises and sprains. 6,7 Recent reports indicate that JDI alleviates rib fracture pain associated with swelling and inflammation. 6 Based on this evidence, we hypothesized that preoperative administration of JDI may alleviate postoperative pain associated after tooth extraction with mandible bone removal. To test this hypothesis, we decided to perform a prospective randomized clinical trial.
The primary objective of this study was to determine the efficacy of JDI in reducing postoperative wound pain after tooth extraction with bone removal. The secondary objective was to evaluate its efficacy for postoperative nausea alleviation.
Materials and Methods
This study was approved by the Institutional Review Board of Osaka Medical College (No. Clin179), and registered with the UMIN Clinical Trials Registry (Trial registration no.: UMIN000019038). Botanical property of JDI is shown in Table 1. JDI is composed of the herbs Cinnamomi Cassiae Cortex (Cinnamon Bark), Ligustici Chuanxiong Radix (Cnidium Rhizome), Nupharis Rhizoma (Nuphar Rhizome), Quercus Cortex (Quercus Bark), Glycyrrhizae Uralensis Radix (Glycyrrhiza Root), Caryophylli Flos (Clove Floral Bud), and Rhei Rhizoma (Rhubarb Rhizome). 6,7 Because previous studies have shown the safety of combination of anesthesia-related drugs and Kampo medicine 8,9 and this is an efficacy trial, we considered safety information have been secured.
Botanical Property of Jidabokuippo
7.5 g of this product contains 2.25 g of dried extract obtained from mixed raw herbs in the above ratio.
Glycyrrhizin (processed Glycyrrhiza Root) and ferulic acid (processed Cnidium Rhizome) are chosen as marker compounds for quality control.
Adult patients with an American Society of Anesthesiologists Physical Status of either 1 (normal, healthy patient) or 2 (patient with mild systemic disease), who were scheduled to undergo tooth extraction surgery under general anesthesia between February 2016 and March 2018, were eligible to participate. In our institute, we usually perform tooth extraction surgery under general anesthesia to patients who have dental phobia or to surgery, which contain invasive techniques such as maxillary or mandible bone removal.
Patients who were pregnant or those who used analgesics, anti-inflammatory drugs, or another Kampo formulation were excluded. 8,9 Patients who were scheduled to undergo only tooth extraction without bone removal under general anesthesia were excluded as well. A document explaining the purpose, procedure, and risks involved in the proposed study was provided to each patient and written consent was obtained.
Eligibility was assessed for a total of 156 patients. Randomization was performed by the envelope method. Patients in the JDI group were given three oral doses (2.5 g each) of JDI (TJ-89, Tsumura Co, Tokyo, Japan) just before falling asleep the night before surgery, and in the morning and around noon on the day of surgery (total 7.5 g). In our hospital, oral surgery under general anesthesia was performed in the afternoon. Patients in the control group did not take JDI. Premedication for general anesthesia was not provided.
Anesthesia was performed by anesthesiologists who were blinded to patient status for JDI administration. Routine monitoring, which included percutaneous oxygen saturation, noninvasive blood pressure, heart rate, electrocardiography, and end-tidal carbon dioxide measurements, was performed. Anesthesia was induced with propofol 1–2 mg/kg and remifentanil 0.3–0.5 μg/kg/min. Rocuronium 0.8–1.0 mg/kg was administered as a muscle relaxant. Nasotracheal intubation was performed. Anesthesia was maintained with sevoflurane 1.5%–2% and remifentanil 0.1–0.3 μg/kg/min. 10 At the phase of sample out, 100 μg of fentanyl was administered as postoperative analgesia. We did not add any other analgesics such as NSAIDs or acetaminophen during surgery. Dental surgeons performed topical anesthesia using 2% lidocaine. We removed the mandible bone surrounding the tooth with a dental drill with round bar of engine (EL COMED100®, W&H Dentalwerk Burmoos, Austria). At the end of surgery, remifentanil and sevoflurane were attenuated. To reverse the neuromuscular blockade, sugammadex (2–3 mg/kg) was administered. Patients were extubated after confirming recovery of awareness.
For postoperative analgesia, patients were able to order 25 mg of diclofenac suppository or 60 mg of oral loxoprofen. Patients were monitored for postoperative wound pain for the first 24 h after surgery. The severity of postoperative wound pain (the primary outcome) and severity of nausea were recorded immediately, and 1, 3, and 24 h after anesthesia recovery by blinded investigators (anesthesiologists) using a numeric rating scale (NRS) (0, no pain or nausea; 10, worst imaginable pain or nausea). 11 The number of patients who requested NSAIDs and that of additional NSAIDs within 24 h from anesthesia recovery was measured. The time to first NSAID request from anesthesia recovery was also recorded. We also monitored the side effect of JDI administration with anesthesia drugs by vital sign, blood test, and physical examination such as auscultation.
Statistical analysis was performed with JMP® 11 (SAS Institute, Inc., Cary, NC). Statistical tests included Mann–Whitney U-test and chi-square test. Data were expressed as mean ± SD. The level of significance for both tests was set at p < 0.05. In a preliminary study, the incidence of wound pain (NRS more than 4) on first 24 h after surgery was 80% in the control group, but only 30% in the JDI group. To detect significant differences (p < 0.05) at a power of 80%, a sample size of 54 (27 in each group) was deemed necessary. Therefore, we planned to recruit 30 patients for each group to account for the possibility of missing data.
Results
Patient demographics
Figure 1 shows the CONSORT flowchart for patient recruitment. A total of 156 patients who planned to undergo tooth extraction under general anesthesia were deemed eligible. No patient refused to participate in the study, and 96 were excluded because their surgery did not include mandible bone removal. Ultimately, 60 patients were enrolled in the study (JDI group, 30 patients; control group, 30 patients). No patient was lost to follow-up throughout the entire evaluation period, and all patients completed the study. Table 2 summarizes the demographics of patients in the JDI and control groups. All demographic data did not significantly differ between the groups (Table 2).
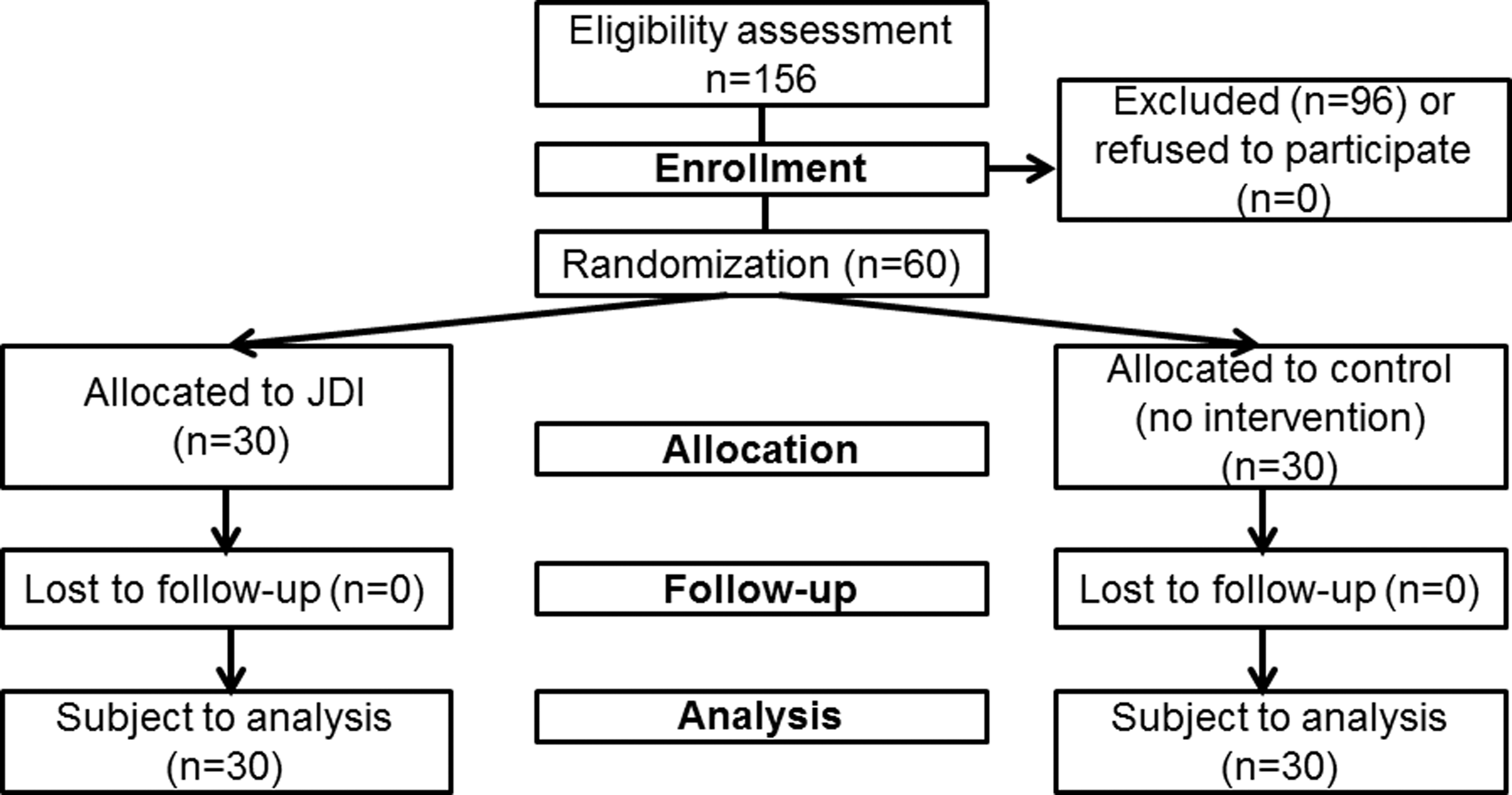
CONSORT flowchart for patient recruitment. JDI, Jidabokuippo.
Patient Background (Jidabokuippo Group vs. Control Group)
Data are presented as mean ± SD or number of patients.
Data were analyzed utilizing Mann–Whitney U-test or chi-square test.
BMI, body mass index; JDI, Jidabokuippo.
Comparison of postoperative wound pain between JDI and control groups
Table 3 shows the severity of postoperative pain. Upon recovery and 1 h from anesthesia, NRS scores on wound pain did not significantly differ between the two groups (p = 0.750, p = 0.130). After 3 and 24 h from anesthesia recovery, however, the NRS score on wound pain was significantly lower in the JDI group than in the control group (3 h p < 0.001, 24 h p < 0.001). The number of patients who requested NSAIDs within 24 h from anesthesia recovery was significantly smaller in the JDI group compared with the control group (JDI group 21 patients, control group 29 patients, p = 0.006). The number of additional NSAIDs administered within 24 h after anesthesia recovery was significantly higher in the control group than in the JDI group (JDI group 1.0 ± 0.8 times, control group 2.7 ± 0.8 times, p < 0.001). Moreover, the time to first NSAID request from anesthesia recovery was significantly longer in the JDI group compared with the control group (JDI group 6.5 ± 3.4 [95% confidence interval 8.3–5.1] hour, control group 3.4 ± 2.2 [95% confidence interval 4.4–2.6] hour, p < 0.001).
Comparison of Postoperative Wound Pain Between Jidabokuippo and Control Groups
Data are presented as mean ± SD [95% confidence interval] or number of patients.
Data were analyzed utilizing Mann–Whitney U-test and chi-square test, * p < 0.05.
JDI, Jidabokuippo; NRS, numeric rating scale; NSAID, nonsteroidal anti-inflammatory drug.
Comparison of nausea between JDI and control groups
Table 4 shows the severity of postoperative nausea in the JDI and control groups. During the follow-up period, the severity of nausea did not differ significantly between the two groups.
Comparison of Nausea Between Jidabokuippo and Control Groups
Data are presented as mean ± SD or number of patients.
Data were analyzed utilizing Mann–Whitney U-test.
JDI, Jidabokuippo; NRS, numeric rating scale.
Side effects
No significant side effects related to JDI, such as edema, hepatic impairment, interstitial pneumonia, hypovolemia, or hypokalemia, were noted during the clinical trial.
Discussion
Pain management after tooth extraction by oral surgeons typically consists of local anesthetics or pain medication. 12 While pain after tooth extraction is controlled immediately with local anesthetics, the pain is greatest during the first 24 h after the procedure. 13 Tooth extraction with bone removal may result in bleeding and pain that can last for up to 3 days. 14 This pain may be accompanied by bleeding and swelling of the gums, as well as soreness and tenderness in the tooth socket. Various analgesics, such as NSAIDs and tramadol, are available to treat pain following tooth extraction. 15
JDI is herbal mixture created in Japan for contusion-induced swelling and pain. Nuphar Rhizome has the effect of absorbing internal hemorrhage and repairing tissue; Quercus Bark has analgesic, detoxifying, anti-inflammatory, and hemostatic effects; Cnidium Rhizome has anti-inflammatory and analgesic effects; and Clove Flower Bud and Rhubarb Rhizome improve microcirculation. 6,7 Therefore, JDI can be used to treat swelling and pain associated with trauma that was considered to be also effective for alleviating postoperative tooth extraction pain.
From a molecular view, most herbs composing botanical components of JDI exert antioxidant effects, 6 which are crucial for suppressing inflammation-related pain. 16 The polyphenol content, which show strong antioxidant effect is highest in Rhubarb Rhizome, followed by Quercus Bark, Nuphar Rhizome, Glycyrrhiza Root, Clove Flower Bud, and Cinnamon Bark. 6 Diphenylpicrylhydrazyl containing radical-scavenging potential is highest in Rhubarb Rhizome, which is followed by Quercus Bark, Nuphar Rhizome, Clove Flower Bud, and Cinnamon Bark. 16
In the present study, the severity did not significantly differ between the groups immediately and 1 h after anesthesia recovery. The result which the severity of pain did not differ between groups immediately after anesthesia recovery may be related to the effects of local lidocaine administration during surgery. There is also possibility that the analgesic effect of fentanyl was augmented by drug–herb interactions. In contrast, the severity of pain was significantly smaller in the JDI group compared with the control group at 3 and 24 h after anesthesia recovery, whereas the number of NSAID administration was smaller in the JDI group than in the control group. These results suggest that postoperative pain after tooth extraction with bone removal is severe regardless of frequent NSAID administration, and JDI is clinically effective against wound pain after tooth extraction with mandible bone removal. The difference in pain severity at 3 and 24 h after anesthesia recovery may be attributed to JDI's ability to suppress swelling of the gums and inflammation.
JDI did not alleviate postoperative nausea. Since JDI regulates inflammation, we anticipated an antiemetic effect, but this was not the case. One probable explanation for this is that postoperative nausea is induced by the central nervous system, in which the utility of antipsychotic drugs, such as droperidol has been validated. In this regard, we previously reported the utility of Go-Rei-San in preventing PONV. Future comparisons of the components and pharmacological activities of JDI and Go-Rei-San may be informative. 17
This study has some limitations worth noting. First, we used a relatively low dose of JDI (total preoperative dose of 7.5 g), and thus a higher amount of JDI may enhance the observed effects. Second, there is a possibility of drug–herb interactions. There are reports that some herbal contents can affect the metabolism of perioperative analgesics, such as lidocaine and fentanyl. 18,19 Evaluation of drug–herb interaction between JDI and perioperative anesthetics and analgesics is warranted. Third, the study was single blinded. A double-blind model using placebo may further clarify the role of JDI on postoperative pain. Fourth, we included both sex for evaluation. As woman is a risk factor of postoperative nausea, 20 it may be clearer if we evaluated the severity of nausea in the same sex.
For future direction, evaluation of JDI effect on postoperative pain after 24 h of operation is warranted. Randomized control study comparing the perioperative efficacy and side effect between JDI and conventional analgesics, such as NSAIDs or tramadol, is also needed. Furthermore, as this study was performed at a single institute, a multicenter large-scale clinical study may be needed to verify our results.
Conclusions
Our results demonstrate that prophylactic administration of JDI before general anesthesia can effectively reduce the severity of postoperative wound pain in patients undergoing tooth extraction with bone removal.
Footnotes
Acknowledgments
Financial support for the study was provided by our institution and department and Young Researcher Funding from the Uehara Memorial Foundation. UMIN Clinical Trials Registry No.: UMIN000019038.
Authors' Contributions
N.K. contributed to the study design and implementation, statistical analysis, and article preparation; K.Y., Y.I, and M.O. contributed to data collection, article preparation, and data interpretation; and T.U. and T.M. contributed to the study implementation and article preparation. All authors discussed the methods and results, and approved the final article.
Author Disclosure Statement
No competing financial interests exist.