
Abstract
Objectives:
This study aimed to compare the efficacy of laser acupuncture (LA) treatment with that of placebo LA treatment in patients with idiopathic, mild-to-moderate carpal tunnel syndrome (CTS), as measured by subjective symptom assessments and objective changes in nerve conduction studies (NCSs).
Design:
A randomized, single-blinded, controlled study.
Settings:
A Teaching Hospital in the Taichung, Taiwan between March 2013 and November 2013.
Subjects:
84 consecutive treatment-naive patients with CTS.
Interventions:
Participants were randomly divided into two treatment arms: (1) LA, administered at traditional Chinese acu-points on the affected side, once a day, 5 times a week, for 4 weeks (N = 43); and (2) placebo LA, administered using the same device and protocol, with the LA device switched off (N = 41).
Outcome measures:
Patients completed the Global symptom score (GSS) at baseline and two and four weeks later. The primary outcome was changes in GSS. NCSs were performed at baseline and repeated at the end of the study as a secondary outcome.
Results:
There was a significantly greater reduction in GSS in the LA group than in the placebo group at week 2 (−9.30 ± 4.94 vs. −2.29 ± 4.27, respectively, P < 0.01) and at week 4 (−10.67 ± 5.98 vs. −2.90 ± 5.61, respectively, P < 0.01). However, NCSs did not show significant difference between the two groups.
Conclusions:
LA may be more effective than placebo LA in the treatment of mild-to-moderate idiopathic CTS in terms of subjective measurement. For patients who fear needle-based treatment, such as acupuncture or local injections, or those who do not opt for early surgical decompression, LA treatment can be considered as an effective and alternative form of acu-points stimulation therapy.
Introduction
Carpal tunnel syndrome (CTS) is an entrapment neuropathy of the median nerve in the wrist. The diagnosis is based on clinical symptoms and specific physical signs and is confirmed by electrophysiologic measurements. 1 –4 Patients complain of pain or paresthesia involving the fingers innervated by the median nerve and weakness of thumb abduction. The classical symptoms are usually worse at night, awaken the patients, and are often relieved by shaking the hands repeatedly. Although several treatment modalities are routinely used, there is no consensus for the best management for CTS. 5 –7
Surgical decompression, often considered the definitive solution, yields good results in only 75% of cases. 1,6,8,9 Of the nonsurgical treatments, a local injection of steroids has been shown to provide short-term symptomatic relief; however, a mechanical or chemical nerve injury can occur. 1,6,9,10 Wrist splints may be effective; nevertheless, the discomfort and restriction of hand activity hinders the patient's ability to work or perform daily activities. 1,3,6,8 Oral steroids are more effective than nonsteroidal anti-inflammatory drugs and diuretics; whereas, they have side effects. 11,12 Since the standard treatments for CTS are not fully satisfactory, other treatment modalities need to be further evaluated.
Laser acupuncture (LA) is defined as the stimulation of traditional acupuncture points by using low-level intensity (class IIIb laser: 5–500 mW, red beam or near infrared wavelength, 600–1000 nm), nonthermal, noninvasive, and painless laser irritation. 13,14 Both acupuncture and LA are the nonpharmacological and nonsurgical treatments for alleviating pain 15 –19 ; however, LA is one noninvasive treatment than acupuncture for those patients who feared it or had the potential risk for infection. Hence, LA may have the noninvasive advantage with wide acceptation.
Compared with needle-based acupuncture, low-level laser therapy (LLLT) can be used for almost all patients, regardless of platelet count and coagulation status; more importantly, it does not involve pain or fear of needles. Further, it is easier to achieve full blinding in LA clinical trials than in needle acupuncture studies, particularly when making comparisons. 6,14 Nevertheless, seldom studies reported the LA efficacy for CTS till this day.
Hence, we want to compare the efficacy of LA treatment with that of placebo LA treatment in patients with mild-to-moderate CTS by using subjective, self-reported symptomatic outcomes and objective electrophysiologic evaluations.
Materials and Methods
Study design and subjects
The CTS subjects were screened and enrolled from the neurological outpatient department of Kuang-Tien General Hospital. The recruited patients were randomly divided into two groups of “LA Group” and “Placebo LA Group” in this randomized, single-blinded, controlled study (Fig. 1).

CONSORT diagram of the study flow.
Ethics statement
The study was approved by the Institutional Review Board of Kuang Tien General Hospital (IRB9827). Written informed consent was obtained from each patient, and it was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12613001065785).
Inclusion criteria
Treatment-naive patients with CTS, aged 20–65 years, were enrolled in this study. The inclusion criteria were based on a combination of clinical and electrodiagnostic findings of idiopathic mild-to-moderate CTS. The CTS diagnosis was based on the presence of at least one of the following symptoms: (1) pain, numbness, or paresthesia in the median nerve distribution; (2) precipitation of these sensory complaints by forceful or repetitive hand use, which could be relieved by resting, rubbing, and shaking of the hands; and (3) awakening from sleep due to such sensory symptoms. The diagnosis was often supported by a positive Tinel's or Phalen's test.
All patients with clinically diagnosed CTS demonstrated median neuropathy at the wrist, confirmed by the presence of one or more of the following standard electrophysiologic criteria: (1) prolonged distal motor latency (DML) to the abductor pollicis brevis (APB) (abnormal ≥4.7 ms; wrist to APB, 8 cm); (2) prolonged antidromic distal sensory latency (DSL) to the second digit (abnormal ≥3.1 ms; wrist to index finger, 14 cm); and (3) prolonged antidromic wrist-palm sensory nerve conduction velocity (W-P SNCV) at a distance of 8 cm (W-P SNCV, abnormal <45 m/s). 20
Mild CTS referred to a decreased conduction velocity at the palm-wrist segment and delayed DSL, with normal median sensory nerve action potential (SNAP) amplitude and compound muscle action potential (CMAP) amplitude of the APB. Moderate CTS referred to an abnormally delayed DML and DSL, with either decreased median SNAP amplitude or decreased CMAP amplitude of the APB muscle. Severe CTS patients referred to the presence of either fibrillation potentials or re-innervation on needle electromyography in the APB muscle. 11,12
Exclusion criteria
Patients were excluded if any of the following were present: (1) Symptoms occurring less than 3 months before the study (to exclude patients who might have spontaneous resolution of symptoms); (2) severe CTS that had progressed to visible muscle atrophy; (3) clinical or electrophysiologic evidence of accompanying conditions that could mimic CTS or interfere with its evaluation, such as cervical radiculopathy, proximal median neuropathy, or significant polyneuropathy; (4) evidence of obvious underlying etiologic factors of CTS such as diabetes mellitus, rheumatoid arthritis, hypothyroidism (acromegaly), pregnancy, alcohol abuse or drug usage (steroids or drugs acting through the central nervous system), and suspected malignancy or inflammation or autoimmune disease documented as underlying causes of CTS; or (5) cognitive impairment interfering with the subject's ability to follow instructions and describe symptoms.
Blinding and randomization
This was a single-blinded trial, in which patients could not tell the difference between the real LA (using invisible, near-infrared laser emission and red light) and placebo LA (using red light). There was little chance of communication between patients because most of them came for treatment at different times. The outcome measurements were evaluated by blinded assessors, and the statistical analyzers were not involved in the patients' clinical management; thus, they were unaware of the patient locations.
However, the LA practitioners were not blinded. Patients were randomly allocated to start with either real or sham LA treatment. The randomization list was compiled by an external physician and was not divulged to the study practitioners or patients. The same physician prepared a series of sealed, sequentially numbered envelopes containing the treatment assignments. When a patient was found to fulfil the inclusion criteria, the study physician would open the envelope to reveal the patient's group allocation. This procedure assured that randomization would not be influenced by the physicians, outcome assessors, or patients.
Electrophysiologic assessments
The electrophysiologic assessments were performed by using an electromyography (EMG)/nerve conduction study (NCS) system (Nicolet Viking IV, Madison, WI). Motor and sensory NCSs were performed across the carpal tunnel by using the standard techniques of supramaximal percutaneous stimulation and surface electrode recording. DML, DSL, motor nerve conduction velocity (MNCV), CMAP and SNAP amplitudes, and W-P SNCV were measured by using the methods described by Delisa et al. 21
The EMG recording was made with the filter band pass at 2–10 Hz, a sweep speed of 2 ms/cm, and an amplifier gain adjusted for full reviewing of the CMAP. For the measurement of SNAP, the instrument settings were as follows: filters, 20–10 kHz; sweep, 2 ms/cm; and gain, 10–20 mV/cm. We used the following electrophysiologic parameters as our secondary outcome: DML, CMAP, MNCV, DSL, SNAP, and W-P SNCV. The skin temperature of the forearm and wrist were maintained at >32°C throughout the measurements. The electrophysiologic assessments were conducted at baseline and were repeated again 4 weeks later.
Laser device and LA intervention
In our study, LA treatment indicates the use of LLL (class IIIb lasers, 400 mW, near-infrared, continuous wavelength, 810 nm, LaserPenR; RJ-LASER, Germany) at traditional Chinese acu-points as PC-7 (Daling) and PC-6 (Neiguan) on the affected side. LA consisted of treatments once per day for 5 consecutive days, followed by a 2-day break, with a total of 20 sessions in a 4-week period. Each laser stimulation treatment was performed in a continuous wave mode for 1 min. The energy transferred to the skin during a treatment of 1 min was up to ∼24 J/cm2.
For the placebo LA treatment, the same device with a red light was pasted on the acu-points in the same way, using the same protocol as for the active laser stimulation, but the laser apparatus was not switched on. It was impossible for the patients to differentiate between active and placebo laser because the same red light was visible with or without the invisible low-level laser in both groups.
Measurement of primary and secondary outcomes
Global Symptom Score (GSS) was used as a primary outcome in this trial. Clinical symptoms were rated from 0 (no symptoms) to 10 (very severe symptoms) in the following 5 symptom categories: pain, numbness, tingling, weakness/clumsiness, and nocturnal awakening. 11,12,22,23 Each patient was directly questioned, and each score was based on the patient's subjective answers. Therefore, the maximum score was 50 (most severe symptoms), and the minimum score was 0 (absence of symptoms). To ensure consistency, the evaluating physician who scored the main outcome measure, GSS, was the same person on each occasion for each patient and was blinded to the type of treatment. The patients completed the GSS standard questionnaires at baseline and 2 and 4 weeks later.
The following electrophysiologic parameters were used as secondary outcome: DML, CMAP, MNCV, DSL, SNAP, and W-P SNCV. Additional secondary outcome measures were the following treatment efficacy grades: good improvement, defined as a >50% reduction in GSS; moderate improvement, defined as a 30%–50% reduction in GSS; lost to follow-up, defined as <30% reduction; and treatment failure, defined by the presence of APB muscle wasting or receiving surgery or other conservative treatment.
Adverse events (AEs) and serious AEs (SAEs) with side effects were collected at each treatment session.
Statistical analysis
The last observation carried forward method was used to impute missing data, and the intent-to-treat analysis principle was adopted. If patients reported symptoms in both hands, we included the more affected hand with a higher GSS for data analysis.
The means and standard deviations were calculated for all subjects in each group, for each parameter. The independent two-sample t test was performed to compare the changes in the objective EMG/NCV findings and subjective symptoms assessment between the two groups for the baseline, 2-week, and 4-week evaluations. The paired t test was performed to compare the week-2 and week-4 data for the objective EMG/NCV findings and subjective symptoms assessment with the baseline data within each treatment group. For the five main symptom scores of the GSS and six measures of the NCS, Bonferroni adjustment was made to control for type I errors. Repeated-measures analysis of variance (ANOVA) was used to compare the values of the subjective symptom's assessment over time between the groups.
All hypothesis tests were two tailed, and a level of significance was set at 0.05. With a two-sided test, significance level of 0.05, power of 80%, standard deviation of 4.5, and 20% drop-out rate, at least 45 subjects per treatment were required to detect a difference of 3.0 in mean reduction of GSS from baseline between the two groups. All statistical analyses were performed by using the SPSS software for Windows, Version 15.0 (SPSS, Inc., Chicago, IL).
Results
Patients' demographics
There were no significant differences in age, sex, duration of symptoms, GSS, and subjective symptom assessments such as numbness, pain, paresthesia, weakness, and nocturnal awakening at baseline between the two treatment groups (Table 1).
Demographic Characteristics and Subjective Symptom Assessments at Baseline for Both Groups
p-Value by two independent-sample t tests or Fisher's exact test when appropriate.
NS, no significance; SD, standard deviation; Sig., significance.
Changes from baseline clinical outcomes at weeks 2 and 4
Both groups showed a significant improvement in the GSS, numbness, and weakness (p < 0.05), and only the real LA group showed a significant improvement in pain, paresthesia, and nocturnal awakening assessment (p < 0.01) at weeks 2 and 4 when compared with baseline. The real LA group also showed a significantly greater improvement in the GSS, numbness, pain, and nocturnal awakening than the placebo LA group (p < 0.01) at weeks 2 and 4, and in paresthesia at week 2 (p < 0.01). No significant difference was observed between the two groups in changes in the degree of weakness from baseline during the study period. The repeated-measurement ANOVA results indicated a significant difference (p = 0.009) in the GSS between the groups over time (Table 2 and Fig. 2).
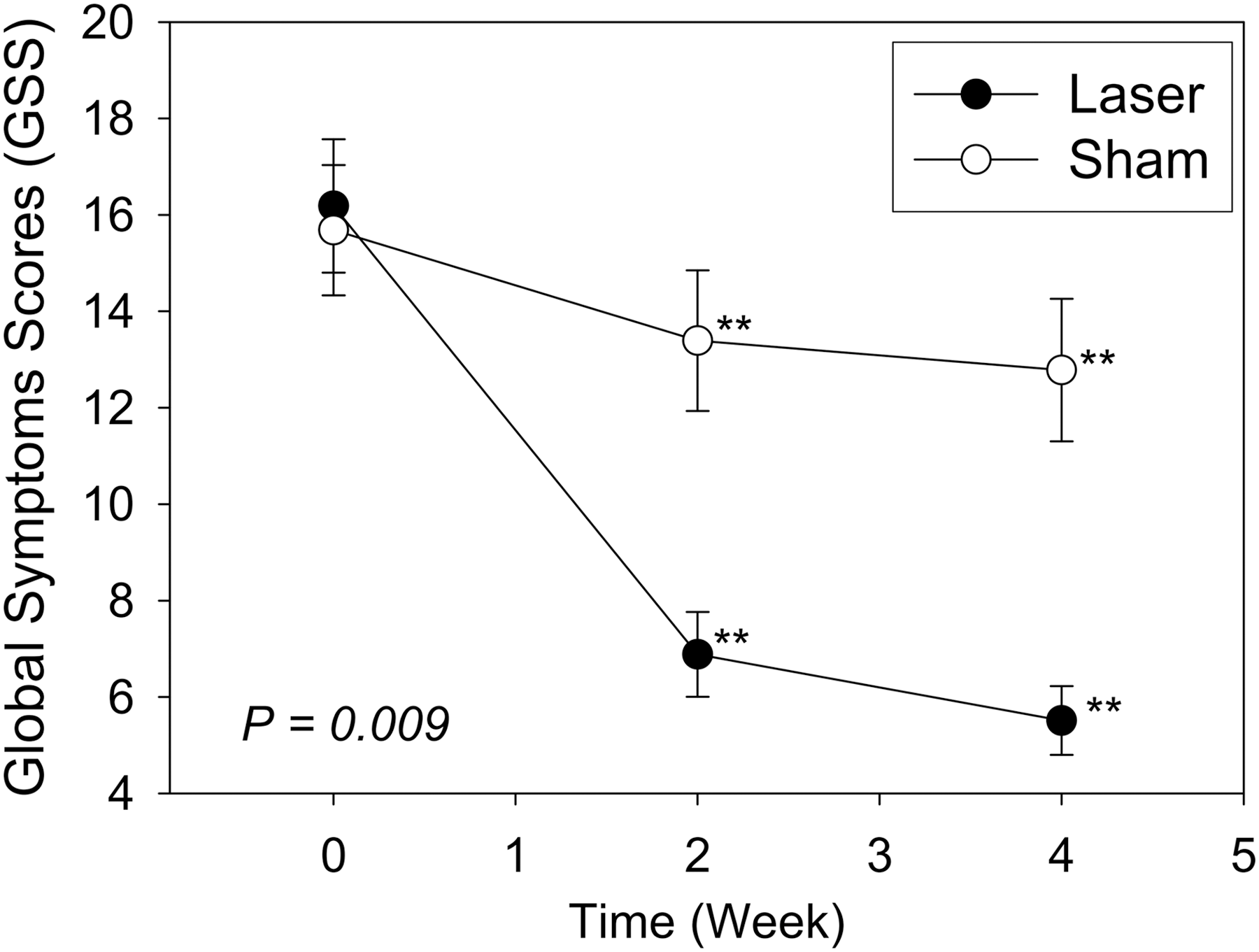
Means with standard error of the total Global Symptom Score with LOCF for the real and sham laser acupuncture groups over time. A significant difference (p = 0.009) was observed between the two groups by repeated-measures ANOVA. **p < 0.01 by the paired t test with Bonferroni adjustment for p-value when compared with the baseline level within each group. ANOVA, analysis of variance; LOCF, last observation carried forward.
Change from Baseline in Clinical Assessments for Both Groups at Weeks 2 and 4
Values are mean and standard deviation of change from baseline (data at week 2 or 4–baseline). Sig.: p-value by two independent-sample t tests using Bonferroni adjustment to compare the two groups.
p < 0.01; ** p < 0.05 values of week 2 or 4 were significantly different from baseline by using the paired t test within each group with Bonferroni adjustment.
GSS, Global Symptom Score; LOCF, last observation carried forward; NS, no significance; SD, standard deviation.
A sensitivity analysis for missing data with the worst case scenario was performed for week 4. The condition of the early discontinued LA patient was assumed to be worse than that at baseline, and the three placebo subjects had improved outcomes at week 4 when compared with baseline. All the conclusions remained the same as the last observation carried forward approach (Table 2 and Fig. 3).
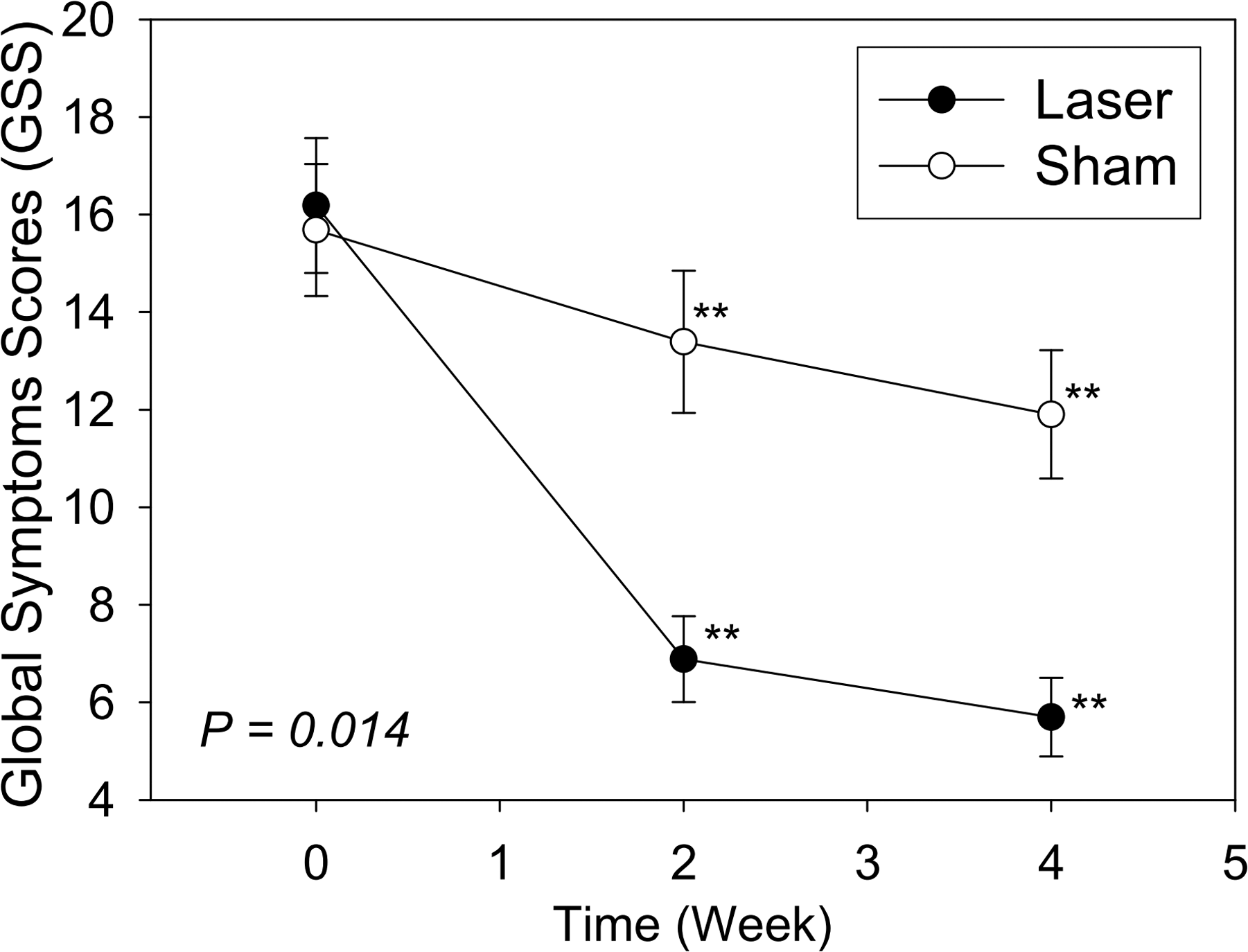
Means with standard error of the total Global Symptom Score with sensitivity analysis for the real and sham laser acupuncture groups over time. A significant difference (p = 0.014) was observed between the two groups by repeated-measures ANOVA. **p < 0.01 by the paired t test with Bonferroni adjustment for p-value when compared with the baseline level within each group. ANOVA, analysis of variance.
Electrophysiologic outcomes at baseline and week 4
No significant difference in the baseline electrophysiologic assessments was observed between the two groups (Table 3). After a 4-week treatment, the changes from baseline of all electrophysiologic assessments were not significantly different between the two groups, and none of the after-treatment assessments were significantly different from those at baseline within each group (p > 0.05) (Table 3).
Electrophysiologic Assessments at Baseline and After Treatment for Both Groups
None of the after-treatment assessments were significantly different from those at baseline within each group using the paired t test. Sig.: The change from baseline (after treatment—baseline) was compared between groups by using the independent two-sample t test.
CMAP, compound muscle action potential; DML, distal motor latency; DSL, distal sensory latency; MNCV, motor nerve conduction velocity; NS, no significance; SD, standard deviation; Sig., significance; SNAP, sensory nerve action potential; W-P SNCV, wrist-palm sensory nerve conduction velocity.
Patients' improvement rates
Compared with the baseline levels, the percentages of patients with treatment failure, moderate improvement, and good improvement were significantly different between the two groups at week 2 (4.7%, 18.6%, and 76.7% for the real LA group, and 65.9%, 14.6%, and 19.5% for the placebo LA group, respectively [p < 0.001]) and at week 4 (2.3%, 9.3%, and 88.4% vs. 51.2%, 17.1%, and 31.7%, respectively [p < 0.001]) (Table 4).
Improvement Rates from Baseline to Weeks 2 and 4 for Both Groups
A reduction in the Global Symptom Score of more than 50% was defined as good improvement, 30%–50% as moderate improvement, and less than 30% as treatment failure. p-Value by Fisher's exact test.
LOCF, last observation carried forward.
In addition, AEs and SAEs were not reported from the participants in either group for all of the sessions in this study.
Discussion
In this study, the patients with CTS who underwent the real LA treatment had a significantly greater, clinically relevant improvement in terms of the primary outcome measure, GSS, at weeks 2 and 4, than that of the patients who underwent the placebo LA treatment. This result was also supported by the higher percentage of >50% improvement in the actual treatment group than in the placebo group at weeks 2 and 4 for the subjective measurement of GSS; however, the before-after treatment difference in the assessment with objective measurement of NCSs between the two groups was not significant. The strength of this study is that both clinical and electrophysiologic assessments based on valid and standard measures were used. The application of LLLT on the traditional Chinese acu-points was clearly described in the treatment protocols, making our study reproducible.
The clinical evidence of the efficacy of LLLT for the treatment of idiopathic CTS is controversial and consists of studies presenting ambiguous conclusions. 21,24 –30 Naeser et al. investigated the effects of real or sham LLLT plus microampers transcutaneous electric nerve stimulation (TENS) in patients with CTS. 24 The investigators used a helium neon laser (632.8 nm, continuous wave, 15 mW) on acupuncture points on the affected hands, and infrared gallium arsenide (GaAs) (904 nm, pulsed, 9.4 W) on acupuncture points located at the elbow, shoulder, upper back, and cervical paraspinal areas. Significant improvement was observed in the pain level, sensory latency, and Phalen's and Tinel's test results after the real LLLT, but not after the sham treatment.
However, no significant differences were observed in any objective evaluation. Irvine et al. compared the effects of LLLT therapy with those of a sham laser therapy by using a Ga-Al-As diode laser with a wavelength of 860 nm. 25 A total dose of 6 J/cm2 given over 15 min to the area surrounding the carpal tunnel was delivered three times a week, for 5 weeks. The investigators did not find any significant difference in the CTS symptoms, hand function, or the NCS findings between the control and treated groups. Evcik et al. compared the efficacies of LLLT and sham laser therapy by using a Ga-Al-As diode laser with a wavelength of 830 nm. 26 Their patients underwent laser therapy over the carpal tunnel area at the wrist with a power output of 7 J/point for 2 points, once a day, for 10 treatment sessions.
The investigators found positive effects on the hand and pinch grip strength that were superior to the placebo treatment; however, there was no difference in the pain relief and functional capacity. Chang et al. placed an 830-nm laser (10 Hz, 50% duty cycle, 60 mW, 9.7 J/cm2) directly above the transverse carpal ligament, which is between the pisiform and navicular bones of the wrist. 27 After 2 weeks of treatment, no significant differences were found in the grip strength or in the symptoms and functional assessments. However, there were statistically significant differences in these variables at the 2-week follow-up.
For the NCS findings, there was no statistically significant difference between the groups after treatment and at the 2-week follow-up. Shooshtari et al. used a low-power laser (400 nm, pulse wave, 9–11 J/cm2) at the carpal tunnel area for 15 sessions, and they found no difference in the symptoms or grip strength; however, they did note a slight improvement in the electrophysiologic findings with LLLT. 28
The controversial results in different clinical studies may be related to various factors such as the study designs, study populations, outcome evaluations, and treatment parameters. Regarding the treatment device and application procedures, different types of lasers may have different effectiveness in wide variations of therapeutic parameters, such as the wavelength, energy density, duration of treatment, number of treatments, and mode of delivery. 13,14,31,32 The laser mode used in our study differed from the designs mentioned earlier. In addition, the energy density (J/cm2) reported in our study (24 J/cm2) was stronger than in any of the previous studies.
Further, the positive effect of LLLT when used to stimulate the acupuncture points as defined in the Channels theory of Traditional Chinese Medicine, an effect that was observed in our study as well as in the trial of Naeser et al., 24 may explain the importance of the stimulating sites. Traditional acupuncture points have been reported to have a lower electrical impedance and higher capacitance compared with adjacent controls. 33 The dosage and treatment time with the 810 nm laser in the stimulation of the acu-points may be sufficient to provide an effective energy for resolution of the clinical symptoms.
LA might provide a new treatment modality and bring into perspective an integrated Western and Traditional Chinese Medicine. In the future, further comparisons should be made with different types of laser settings and stimulating locations to provide practitioners better therapeutic programs for patients with CTS.
The efficacy of LLLT has been demonstrated in a variety of medical conditions; some proposed mechanisms have been documented and include the suppression of inflammation, tissue repairing and regeneration, and facilitating nerve recovery by stimulating regeneration. 34,35 Previous studies have also shown that laser energy would increase the ATP production, improve cellular respiration, and increase the levels of serotonin and endogenous opioids. 36,37 In our study, there was significant improvement in the subjective GSS; however, there was no statistically significant before-after difference in the NCS findings between or within the two groups.
The discrepancy between the clinical improvement and objective change in the NCS findings has two possible explanations. First, previous studies have shown that LLLT can induce a reversible blockade of neurotransmission in the A-delta and C fibers. 38 If the small fibers were predominantly affected by the LLLT, this would allow a decrease in the pain transmission, leading to symptoms relief without accompanying objective changes in the NCSs, because the standard NCS techniques provide information only on the largest and fastest-conducting myelinated nerve fibers. Second, the post-treatment NCS may have been obtained too early to detect an obvious change in the findings.
This is similar to the postoperative findings for CTS; there was a rapid subjective improvement postsurgery, with a delayed improvement in the NCS parameters. 39 –42 A long-term follow-up using NCSs might be helpful to detect the delayed effects of LLLT on the affected nerves in CTS.
No patients in either group reported any adverse effects with regards to the LA. This is in line with reports on the safety of LLLT. 13 In our previous study, we demonstrated that needle acupuncture was as effective as short-term low-dose prednisolone at 1 month, and it had better outcomes at 12 months in patients with mild-to-moderate CTS. 22,23 However, during the recruitment phase, some of the subjects expressed fear of needle acupuncture procedures and were unwilling to take part in the study. In addition, since the acupuncture intervention is more invasive (skin penetration with a needle) than the control group intervention (pills), placebo effects may have contributed to the between-group difference observed in that study.
In this study, the clinical effect of LA for CTS was likely due to the combination of the actual biological effect of LLLP on the acu-points, and the nonspecific effects, such as nearly daily contact with the physicians, or patient expectations of the treatment effects. 43,44 Blinding patients to the placebo-laser setting in this study was used to rule out a possible placebo effect or biases caused by expectations and subjective assessments. Indeed, some of the patients treated with sham laser experienced remarkable clinical improvement, which is in line with previous studies. 25,28
Based on these results, we believe that placebo LA can serve as a valid control procedure for evaluating specific LA effects. The results in our study demonstrated that the patients with real LA treatment had significant improvement in the subjective symptom assessment compared with the patients with placebo LA treatment.
The missing data on week 4 for the 4 early discontinued subjects were originally replaced with the data obtained on week 2 for analysis. Since significant differences were observed between the two groups for most of the clinical assessments at week 4 with the last observation carried forward, a sensitivity analysis with the worst case was performed as suggested by the reviewers to verify the robustness of such methods. The condition of the LA patient who failed to return at week 4 was assumed to be worse than that at baseline; all assessments were replaced with the values of baseline plus 2, that is, GSS plus 10. On the contrary, the condition of the three early discontinued placebo subjects was assumed to be better than that at baseline, with all data replaced with the baseline values minus 2, that is, GSS minus 10.
The results are presented in Tables 2, 4, and Figures 2, 3 given next and all the conclusions remained the same as the last observation carried forward approach. The results from repeated-measurement ANOVA also indicated a significant difference (p = 0.014) in the GSS score between the groups over time. Although the number of early withdrawals was greater in placebo than in LA group, 3 versus 1, all the 3 placebo subjects actually had a worse condition at week 2 than that at baseline. Now we assumed that their conditions at week 4 improved even better than those at baseline instead of being the same as week 2, and the difference between the two groups remained significant. This result implies that the treatment effect, indeed, existed and the impact of missing data would not alter the conclusion significantly in this study.
This study has several limitations that are worth noting, each of which points toward improvements that can be considered in a future study. First, only the short-term effectiveness of LLLT was evaluated, and evaluations of long-term beneficial effects are necessary. Second, although patients were unaware of their treatment group, the physicians were not blinded to the patients' treatment assignment. Thus, we are not sure whether the degree of the observed change was due to nonspecific effects in this regard.
Third, the natural history of CTS is not necessarily progressive; patients may even spontaneously recover if they change their lifestyle or risk factor-related behavior after they recognize their disease characteristics. 28,45 However, the superiority of the real over the placebo LA in our study could not be explained by spontaneous improvement, because when using randomization, spontaneous improvement would occur evenly in both groups. Fourth, the treatment protocol required more study visits. Each subject had to visit the physician 5 times per week for 4 weeks. This limited the number of subjects who were willing to participate. Fifth, the GSS was recorded as the only affected side with higher severity in this study, and we did not include the bilateral hand to analyze. It may be one limitation for efficacy evaluation, so we add this deficiency in the limitation. We may include the bilateral CTS with both hands analysis in future.
Conclusion
Despite these limitations, this randomized, single-blinded controlled study indicated that LA is more effective than placebo LA in the treatment of mild-to-moderate idiopathic CTS in terms of subjective measurement. Therefore, we recommend that LA treatment be considered as an alternative therapy for those who fear needle-based treatment, such as acupuncture or local injections, or those who do not opt for early surgical decompression. Future studies should consider comparisons between LA and acupuncture or other conservative treatments, and they explore the underlying mechanisms and biophysical effects of LA on the nerve tissue regeneration in CTS. Treatment frequency could hamper translation to clinical practice and may be one limitation for LA efficacy.
Authors' Contributions
C.W.J., T.H.L., C.M.C., and C.P.Y. were responsible for the study concept and design, modification of the study design, and review and interpretation of the data. C.W.J., T.H.L., C.M.C., and C.P.Y. were responsible for drafting the article. M.H.C., C.L.H., T.C.L., and K.L.W. made modifications to the study design and revised the article. C.W.J., T.H.L., and T.C.L. contributed to the collection and analysis. M.H.C., C.L.H., C.M.C., and C.P.Y. contributed to the interpretation of data and revised the article. All authors read and approved the final article.
Ethics Approval
The study was approved by the Institutional Review Board of Kuang Tien General Hospital, Taichung, Taiwan (IRB9827). Written informed consent was obtained from each patient.
Footnotes
Author Disclosure Statement
All authors listed in the article have contributed sufficiently to it, have approved the article, and declare that they have no conflicts of interest to declare.
Funding Information
This study was supported by a grant from Kuang Tien General Hospital, Taichung, Taiwan, and NSC-99-2628-B-075A-008-MY2.