
Abstract
Introduction:
Although the clinical use of electro-acupuncture is widespread, the neuromodulating influence of various applied frequencies is not well established.
Objectives:
Heart rate variability (HRV), stress and parasympathetic recovery are closely related to health, longevity and vitality in humans. This study was undertaken to determine the influence of different electro-therapy frequencies on various autonomic nervous system markers when applied to a Battlefield Acupuncture Protocol (BFA).
Design:
A detailed comparison of autonomic nervous system (ANS) response to low frequency (LF) 2.5 Hz electro-acupuncture and mid-frequency (MF) 15 Hz electro-acupuncture applied by point stimulation to acupuncture points was undertaken on 2 groups of 12 patients.
Interventions:
Both LFEA and MFEA were applied to Battlefield Acupuncture protocol, consisting of five (5) key acupuncture ear (auricular) points that isolate the autonomic nervous system (ANS) and central nervous system's role in the chronic/acute pain cycle. Evaluations entailed an advanced status of autonomic nervous system (ANS) function through Electro-Cardiogram (ECG) baseline markers reflecting: sympathetic stress (SI); parasympathetic vagal tone (high frequency [HF]) and heart rate variability (HRV = total power). All were repeated subsequent to electro-therapy using 2 separate electro-modalities of low-frequency (2.5 Hz) electro-acupuncture (LFEA) and Mid-Frequency (15 Hz) electro-acupuncture (MFEA). All 24 patients received one (1) elector-acupuncture session.
Results:
The autonomic nervous system response to LFEA (2.5 Hz) reflected a statistically significant pre-post improvement in three of the markers collected: heart rate variability (HRV) improved by 61% [p = 0.002]; sympathetic stress (SI) reduced 42% [p = 0.002]; and parasympathetic vagal tone (HF) increased 56% [p = 0.017]. In contrast, MFEA (15 Hz) showed positive but non-significant changes in outcomes in all nervous system markers.
Conclusions:
The autonomic nervous system response with LFEA showed a measurable reduction in sympathetic stress with subsequent improvement in vagal tone, and HRV. This positive sympathetic nervous system deactivation from LFEA application shown in this study could have a major impact on other pathologies related to human health and longevity. Further cohort studies are warranted to determine the validity of these outcomes.
Introduction
Imbalances of the parasympathetic (rest, heal, and calming) and sympathetic (flight/fight/freeze) branches of the autonomic nervous system (ANS) are associated with a wide variety of pain and diseases. Designed for short-term survival, “upregulation” or persistent tone in the sympathetic system, called stress, is directly related to a cascade of negative neurophysiologic responses that are connected to chronic disease and impaired exercise tolerance. 1 –12
Real-time analyses of sympathovagal responses may be now accurately measured using electrocardiograms (ECG). 7,13,14 Three key ECG markers directly relating to human health are as follows: stress index (SI-sympathetic), vagal tone (high frequency [HF] = parasympathetic vagal tone (high frequency [HF])), and heart rate variability (HRV-total power sympathetic/parasympathetic balance) (Table 1).
Description of Autonomic Nervous System-Electrocardiogram Markers: Stress Index, High Frequency, and Heart Rate Variability
ANS, autonomic nervous system; HF, high frequency; HRV, heart rate variability; SI, stress index; TP, total power.
Sympathetic stress represents the percentage (%) of the body's immediate cardiac muscle oxygen demand in relation to heart work (amount of stress the body is experiencing at the present time), 15 and measured as the SI. SI is correlated to C-reactive protein and is a marker of sympathetic failure. C-reactive protein is produced by the liver and increases with inflammation. 16 It is well-established that high stress values (sympathetic overactivity) are implicated in cardiac pathology, morbidity, reduced quality of life, and precipitous mortality. 17,18
The parasympathetic nervous system (vagal tone as a marker of HF) is involved with restoration and repair, nourishment digestion and detoxification, immunologic balance, and provides an innate sense of vitality and well-being. This control of the sympathovagal response is mediated through the 10th cranial nerve (vagus nerve) 19,20 and results in slowing of the heart rate, controlling sweating, regulating blood pressure, stimulating peristalsis, and controlling vascular tone. Low HF values are cited with poor sports recovery and reduced muscle strength 21 and suboptimal health. 22 –24
HRV measures the beat-to-beat variations in heart rate to determine sympathetic or parasympathetic dominance of the ANS. HRV is an important electrophysiologic marker for the assessment of functional vitality, health, and well-being in science. 1 –8 Health, zest for life, longevity, and well-being are directly connected to the regulatory control of this balance. 25 –30 Optimal HRV values are associated with improved exercise tolerance, 9 –12,31 –33 cardiovascular health, 34 –37 improved ANS control, 38 –43 improved vagal tone, 44 better emotional regulation, 45 –49 and enhanced neurocognitive processing. 50 –52
Electroacupuncture (EA) is a form of noninvasive acupuncture where concentrated electric currents are applied to acupuncture points via point stimulation. 53 There are two common types of electrical acupuncture frequencies applied in the marketplace. These are low-frequency (2.5 Hz) electroacupuncture (LFEA) and midfrequency (15 Hz) electroacupuncture (MFEA). The use of MFEA in acupuncture therapy is widespread for pain management. 53 –55
There is a dramatic difference in the two therapies. MFEA is applied using alternating current (AC) in the milliamperage range (10–3 amperes), at frequencies (>10 Hz), and is referred to in the marketplace as EA. 53,56 –58 Many studies support the use of EA current for functional outcomes and pain relief. 56 –61 LFEA is applied in the microamp or millionth of amp (10–6 amperes) range at lower frequencies (1–4 Hz) using direct current (DC) and is called microcurrent point stimulation (MPS) or microcurrent EA. 61 –63 It is theorized that LFEA and MFEA have different modulating effects on the ANS. 64 –66
This study investigates the influence of low-frequency (2.5 Hz) EA and midfrequency (15 Hz) EA on ANS functioning and stress levels in two cohorts of 12 patients. As there is little consensus in the literature regarding the neuromodulating efficacy of the different EA frequencies, this study was undertaken to validate scientifically and to identify the best practice measures for electrostimulation for optimal nervous system regulation.
Patients, Materials, and Methodology
Patient selection
This study entailed the use of EA in 24 healthy patients (13 females, 11 males), who presented to us for therapy. The diagnoses of pain, location, severity, sex, previous interventions, or surgeries were not considered exclusion criteria. There were no other exclusion criteria. All patients provided informed written consent to partake in treatment and the study assessments. Patients were randomly divided into two groups (Table 2).
Descriptives by Gender and Age for n = 12 Electroacupuncture Groups
AC, alternating current; DC, direct current; SD, standard deviation.
Methodology
Two electromodalities in total were used (Table 2); AC EA (MFEA) and DC EA (LFEA) both applied to a Battlefield Acupuncture (BFA) protocol (Fig. 1). LFEA was applied using the Dolphin Neurostim (Center for Pain & Stress Research Ltd, Ontario, Canada) (Fig. 2). This is an FDA-approved device that applies a low-frequency (2.5 Hz), monophasic DC microcurrent through a point stimulator (contact surface area = 0.0104 cm2, Table 3) for the relief of chronic pain and stress. 67 MFEA was applied with Pointer Plus Excel (Electro-Therapeutic Devices, Ontario, Canada) (Fig. 3). This is an FDA-approved device that applies a midfrequency (15 Hz), biphasic AC electrocurrent through a point stimulator (contact surface area = 0.0656 cm2, Table 3) for the relief of chronic pain. 68 Both EA devices have built-in point locators that can detect low-resistance acupuncture points. EA treatments lasted 5 min, and all treatments and data were collected over a 2-day period.
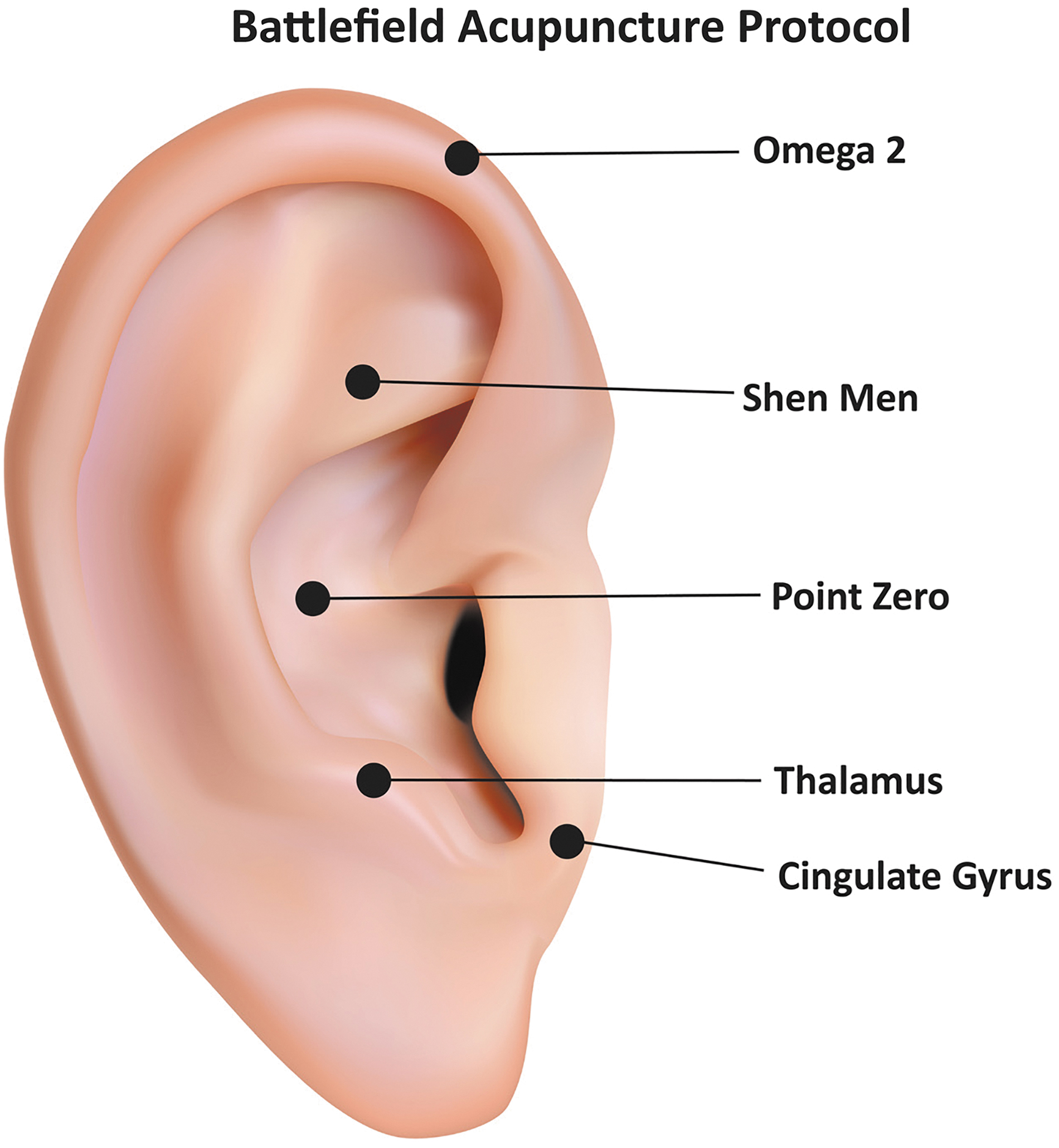
Battlefield Acupuncture protocol.
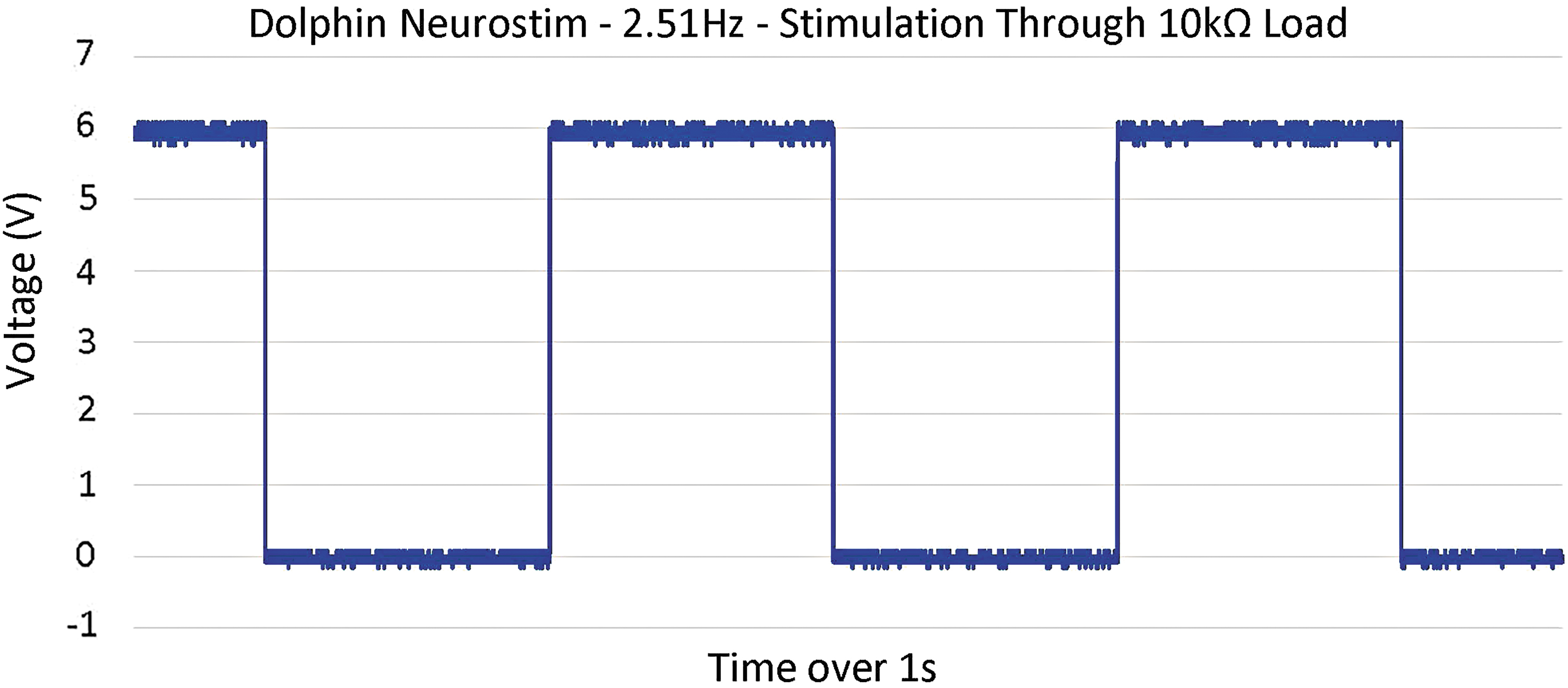
Low-frequency electroacupuncture—MPS 2.5 Hz. MPS, microcurrent point stimulation.

Midfrequency electroacupuncture—PPlus 15 Hz.
Electrical Parameters of Electroacupuncture Devices
AC, alternating current; DC, direct current.
Protocol
Both LFEA and MFEA were applied using BFA protocol, developed by Col. Dr. R. Niemtzow of Andrews AFB, as a standardized protocol to provide a simple, nonpharmaceutical solution for the military's pain management needs in the clinical and battlefield settings. 69 –71
The protocol involves the application of a stimulus to five key acupuncture ear (auricular) points that isolate the ANS and central nervous system's role in the chronic/acute pain cycle (Fig. 1). When these points are collectively treated, it has been reported that a wide variety of neuromyofascial pain syndromes can be effectively relieved in a timely basis. 72
Patient information
Patients were referred by health care professionals and provided informed written consent to partake in treatment and the study assessments. Patients were asked not to eat or smoke 2 h before treatment and ECG testing. During the data collection, patients were instructed to sit comfortably and breathe normally during ECG testing and EA treatments. Starting with the left ear, all five BFA points were stimulated for 30 sec per point in a series using the following order: Point Zero, Shen Men, Omega 2, Thalamus, and then Cingulate Gyrus. Both ears were treated for a total EA application time of 5 min, and an ECG testing time of 10 min for each pre/post collection. All patients were seated during ECG testing and EA treatments. ECG scores were recorded immediately before EA treatments and recorded after 10 min of rest time post-EA applications.
ANS testing
ANS assessments were taken before and after electrotherapies with the ANS1 (Biosensor Equipment LLC, Houston, TX), an FDA-approved device that measures sudomotor, adrenergic, and cardiovagal functions. The ANS1 utilizes a multimodal approach to assessing both the sympathetic and parasympathetic nervous systems, galvanic skin response functions through an autonomic nerve assessment, an arterial assessment, and an assessment of cardiometabolic markers, 7,13,14,73 using a photoplethysmography sensor and a blood pressure device to comprehensively assess cardiac autonomic neuropathy and endothelial dysfunctioning. ANS1 device measured physiologic health markers HRV, HF, and SI, placing each patient measurement categorically into abnormal, borderline, and optimal goal columns (Table 1). ANS1 measurements were collected and recorded digitally and measured in milliseconds/square second (ms2). Two ECG company technicians were present to collect data and ensure accuracy. Two additional therapists applied LFEA and MFEA to patients using BFA protocol (Fig. 1).
Statistical analyses
The data are expressed as mean ± standard error of the mean. Normality assumption was checked using a Shapiro–Wilk normality test, and if the data held true, a paired t-test was performed to show statistical evidence before and after EA treatments. If the Shapiro–Wilk test revealed a non-normal distribution, a paired Wilcoxon signed rank test was implemented, which compares the median differences in two sets (Table 4). Averages, medians, and standard deviations of all parameters were calculated to describe pre- and postmeasurements as well as their difference. All tests were interpreted with 95% confidence intervals. All statistical analyses were independently performed using RStudio, which is an integrated development environment for R (version 3.6.1) programming language.
Pre/Post Treatment Descriptives
ANS, autonomic nervous system; HF, high frequency; HRV, heart rate variability; N/A, not applicable; SI, stress index
Results
The application of MFEA to BFA protocol produced positive but nonsignificant outcomes in all nervous system markers (Table 4). The ANS response to LFEA applied to the BFA protocol reflected a statistically significant pre/post improvement in all three of the markers collected: sympathetic stress (SI) reduced by 42% (88.417 points, 95% CI [38.575 to 138.259]; p = 0.002); parasympathetic vagal tone (HF) increased by 56% (113.833 points, 95% CI [−203.222 to −24.445]; p = 0.017), and HRV improved by 61% (705.333 points, 95% CI [−1086.466 to −324.201]; p = 0.002).
Discussion
Technology such as advanced ECG autonomic testing can now provide scientific evidence as to the inner workings of nervous systems in ill-health and disease, 58,59 permitting the real-time collection of quantifiable data for the purpose of science and education. 74 –76 Therefore, ECGs are the ideal testing modality to determine the therapeutic influences of EA frequencies on nervous system regulation.
The results from this study clearly show that the application of MFEA (15 Hz) did not produce statistically significant modulations within the ANS. In comparison, the application of LFEA significantly restored a more normal physiologic state throughout the various nervous systems (both parasympathetic and sympathetic) when applied to acupuncture points. There were marked improvements in stress reduction, HRV, and HF parasympathetic-vagal tone postlow-frequency EA application.
It is reported in the literature that various electrofrequencies have different modulating influences on the sympathovagal response. 65,66,77 LFEA is reported to increase the parasympathetic-vagal activity, 65,78,79 while higher frequencies (>10 Hz) are reported to increase sympathetic activity. 65,80 –82 The authors have previously reported this relationship in literature. 65 This study showed that LFEA (2.5 Hz) provided superior stress reduction and vagal activation in comparison with MFEA (15 Hz), supporting the previous reported evidence that higher frequencies (Hz) may negatively influence the sympathovagal balance. These data clearly showed that MFEA (15 Hz) produced nonsignificant outcomes; in comparison, HRV, an important indicator of human longevity and directly linked to mortality, 26 –30,83 –89 was only enhanced after LFEA application.
There is no consensus in literature to explain this phenomenon. It is reported in literature that low-frequency microcurrent therapies applied below 500 mca (≥0.5ma) activate ATP, protein synthesis, and increased metabolism, 64 while higher frequency/amplitude currents inhibited these vital processes that are necessary for normalizing the milieu. 64 This suggests that low-amplitude DC microcurrent is more beneficial to cellular regeneration than high-amplitude AC stimulation. This improved cellular activity postmicrocurrent is widely supported in literature with wound management, 90 –94 ; however, increased cellular healing may not be sufficient to explain the significant neuromodulating differences between the frequencies applied in this study.
In the 1970s, Pomeranz, considered the father of neuroendocrinology, developed and supported his endorphin theories utilizing low-frequency DC. 95 –100 Pomeranz discovered in experiments with rats that electrofrequencies influence HPA-endocrine activity. By applying various electrofrequencies and using naloxone as a control, he determined that beta-endorphins were only released within a narrow electrofrequency range of 2–4 Hz. 95,96 It is widely known that the regulation of the HPA-axis and the ANS is physiologically closely related. 101 It is therefore plausible that the LFEA (2.5 Hz) applied in the study may have activated the release of beta-endorphins, resulting in nervous system modulation. However, further HPA-axis and ECG studies would be required to confirm this relationship.
The concept of electrically stimulating the auricular branch of the vagus nerve (ABVN), which provides somatosensory innervation to several aspects of the external ear, is now gaining recognition in literature. 102 –104 Vagus nerve stimulation (VNS) has been reported to improve HRV 105,106 through activation of the parasympathetic system, 107,108 and noninvasive stimulation of the ABVN in the ear using transcutaneous VNS has also reported in both vagal tone and HRV activation. 109 –111
Reviewing the anatomical location of BFA points reveals that the majority fall within the concha regions of the ear, which are innervated by the ABVN. Electrical analysis discovered that LFEA stimulation produces 5.78 times the current density (0.0578/0.0010 A/cm2 = 5.78, Table 3) and coulomb charge (301.9E-6/52.1E-6 Coulomb/s = 5.78, Table 3) that MFEA stimulation produces. It is reasonable to surmise that the higher current density and coulomb charge values that LFEA applied to this region of the ear may have been responsible for activating a stronger neuromodulating response than MFEA in this study, but further research with much larger sample sizes is required to quantify this hypothesis.
It is also prudent to examine the heart, an electrically sensitive muscle that beats at an electrical frequency range of 1.0–1.6 Hz (60–90 beats per minute). 112 –115 It is widely reported that low frequencies enhance the sympathovagal balance. It is likely that mid (10–20 Hz) to high (>50 Hz) electrofrequencies may disturb the heart's delicate relationship with the ANS, physically altering heart beat frequency and activating sympathetic stress, but this is another area where further research is needed.
The widespread use of wearable ECG technology providing accurate HRV measurements is now currently available to the public, with improved future technology guaranteeing increased accuracy and availability. Patients in the future will be able to monitor in real time the HRV and sympathovagal influence of all electromodalities applied clinically, ushering in a new medical paradigm. Therefore, it may be prudent for clinicians to monitor the electrotherapeutic parameters of devices being clinically applied if neuromodulation is a desired outcome in their future patient populations.
In conclusion, this study validates the impact of various electrofrequencies on ANS functioning and stress levels. The results are, however, markedly different with frequency (Hz) applied—LFEA provides superior nervous regulation with upregulation of parasympathetic and downregulation of sympathetic nervous system. These significant differences in outcomes in this study suggest that the therapists' choice of electrocurrent and frequency (Hz) may have a stronger influence on ANS regulation and human health than has hitherto been acknowledged; MFEA is in common practice today and its application may need to be reviewed based on the outcome of this study. However, further investigation is warranted with a much larger focus group to confirm these results and to assess their impact.
Footnotes
Acknowledgment
Independent electrical analyses on EA devices were performed by RMF Design and Manufacturing, Inc., a full-service electronic research, design, and manufacturing firm with more than 35 years of experience.
Author Disclosure Statement
K.A. was the lead author and key contributor to the article. Both K.A. and W.T. were responsible for performing EA treatments. R.G. is a research consultant with a passion for science who overviewed and edited this article. All authors received financial compensation as educational or research consultants from the sponsoring company that may create the appearance of a conflict of interest in connection with the submitted article.
Funding Information
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. This study was funded by The Center for Pain & Stress Research.