
Abstract
Objective:
This systematic review evaluated equine-assisted activities and therapies (EAATs), formerly referred to as equine-assisted services (EAS), in children and youth (ages 6–18 years) with attention-deficit/hyperactivity disorder (ADHD), according to the International Classification of Functioning, Disability, and Health.
Methods:
Electronic database searches were conducted of studies from inception through December 2020.
Results:
A total of 12 articles were included: 8 noncontrolled prospective studies and 4 randomized-controlled trials (RCTs). Furthermore, seven of moderate methodological quality studies and five of moderate high methodological quality studies were included. Evidence was found for the effectiveness of various forms of EAS, including equine-assisted physical therapy (EAPT) and therapeutic riding (TR). Improvements in body functions and structures (n = 10) were found in the domains of mental and neuromusculoskeletal functions, as well as functions of the cardiovascular system using EAPT (n = 6). Limited evidence was found regarding the positive effect on activity and participation (n = 4) following TR interventions. Quality of life (QoL) was improved in both TR and EAPT (n = 4).
Conclusion:
There seems to be preliminary evidence that EAS may be beneficial in promoting the physiological functions of body systems for children with ADHD. The influence on participation and QoL still requires further evidence. More generally, further controlled studies, including bigger sample sizes, are needed to understand the specific effects of different EAS on the core symptoms and consequence of ADHD.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by the presence of symptoms including inattention, hyperactivity, and impulsivity. 1 ADHD is currently one of the most common pediatric diagnoses. Approximately 6.4 million children ages 4–17 years across the United States were diagnosed with ADHD in 2014, with boys experiencing a 2- to 9-fold greater prevalence than girls. 2
ADHD is characterized by a developmental and chronic impairment of executive functions (EFs), which are high-level cognitive self-management processes often associated with the frontal lobes of the brain. Via dorsal frontostriatal circuits, EFs allow individuals to regulate their behavior, thoughts, and emotions, and thereby enable self-control, goal-directed behavior, response inhibition, interference control, working memory, and set shifting. 3 As these skills are critical for cognitive, social, behavioral, and psychological development, 4,5
ADHD is often further associated with impairment of psychosocial functioning and a wide variety of daily tasks beyond the core symptoms. 6,7 These can lead to significant difficulties in academic achievements, and in social and personal relationships, 5 which result in low self-esteem and reduced quality of life (QoL). 7 To enable a child with ADHD to participate in daily activities, treatment must address factors that hinder performance. The current recommendation for the most effective intervention is a combination of administration-approved pharmacologic drug medication and/or evidence-based psychological and behavioral therapy interventions. 1
The most common pharmacologic treatment for ADHD is stimulant medication (methylphenidate and amphetamine), which has been shown to reduce symptoms. 1 Other nonpharmacologic interventions focus on cognitive training of single or multiple domains of EF, such as working memory, inhibition, or cognitive flexibility. These approaches are led by neuroplasticity principles and are based on intensive repetitive training and immediate feedback. 8,9 While these approaches address core symptoms such as hyperactivity and inhibition, they do not address everyday performance; they therefore cannot be applied to functional tasks. 10
Behavioral interventions that have been applied successfully to children with ADHD are subject centered and occupation based. They focus on personal functional goals and include strategy acquisition. 11 –13 Although these approaches show substantial evidence for improving EFs and functional/academic skills, they do not address the psychological difficulties that children with ADHD usually experience. The psychological interventions include, for example, behavioral programs, psychoeducation for parents, and expressive therapies. 14 The existing interventions improve core symptoms, EFs, everyday functions, or emotional symptoms. Despite multiple existing interventions, it seems that each of them addresses only one specific aspect of ADHD.
Animal therapy is defined as treatment in which various animals are used to promote therapeutic goals in the physiological, cognitive, psychological, and sociological areas. 15 Specifically, equine-assisted services (EAS), until recently called equine-assisted activities and therapies (EAATs), are a variety of multimodal and complex activities and therapies, designed for achieving therapeutic and other goals through interaction of subjects with equines. These interventions differ from one another by the therapeutic goals and the therapy provider. As complex interventions, EAS involve a number of behaviors required by those receiving and delivering the intervention, which requires a degree of flexibility and tailoring the intervention to a specific individual. 16
EAS interventions are classified into three broad areas of professional work: therapy, learning, or horsemanship. The Therapy division relates to the broad area of therapy as licensed therapy professionals may incorporate horses in five distinct therapies: counseling, occupational therapy, physical therapy, psychotherapy, and speech-language pathology. These licensed therapy professionals work within the scope of practice of their particular discipline. 17 It incorporates equine activities and/or the equine environment. 18 Therapeutic goals aim to promote functional outcomes, which may include enhancing participation, promoting QoL, and encouraging social interaction. 19
Rehabilitative goals are related to the patient's needs and the medical professional's standards of practice. Equine-assisted physical therapy (EAPT), formerly named hippotherapy, 20 uses equine movement and purposeful manipulation as a specific therapeutic tool used by occupational therapy, physical therapy, or speech-language therapy professionals to engage sensory, neuromotor, and cognitive systems and achieve functional goals within the providers' scope of practice as part of their overall treatment plans. 17 While riding, the rider is in a state of constant physical interaction with the horse, responding to the horse's movement. Equine-assisted psychotherapy is defined as an interactive process in which a licensed mental health professional working with or as an appropriately credentialed equine professional partners with suitable equine(s) to address psychotherapy goals set forth by the mental health professional and the client. 21
Learning division includes equine-assisted learning (EAL) in education, organizations, and personal development. It is related to the broad area of learning, and specially trained or certified professionals may incorporate base activities (e.g., grooming, handling, leading, and observing). These activities may help participants attain individualized horsemanship skills. 17
Horsemanship division is related to the broad area of horsemanship, and equine professionals may offer four distinct nontherapy services that are adapted from traditional equine disciplines of horseback riding, driving, and vaulting. These include adaptive equestrian sport, adaptive riding or therapeutic riding (TR), driving, and interactive vaulting. 1 7 These aim to enhance the cognitive, physical, emotional, and social well-being of individuals with special needs, while learning riding skills and caring for a horse. TR treatment is performed during the horseback riding, through creation and development of a connection between the rider and the horse, and between the rider and the instructor. 19 Since none of the studies in the current systematic review includes horsemanship interventions, except for TR, they are not fully elaborated.
Several characteristics of EAS are believed to address the core symptoms, EFs, emotional aspects, QoL, and daily function among children with ADHD. Data show that TR and unmounted activities address EFs and core symptoms of attention in children with autism spectrum disorder (ASD) 22 as well as transferring of goals to the home and community environment. EAS were also shown to improve EFs among children with ASD. 23 As many of these features are also common to ADHD, the authors hypothesized that different EAS could prove therapeutic to this population as well. Horses increase motivation, while requiring full attention and engagement in the learning situation. It was found that the animal–human emotional relationship promotes changes in the children's functioning, including activities of daily living (ADL), and psychological and motor functions. 24
The animal–human relationship also evokes attachment behavior, 25 along with the reinforcement of positive actions. 23,26 The connection with an animal provides a sense of confidence, helps decrease anxiety, and is perceived as a social connection and relationship with the participant. 19 In addition, one can hypothesize that riding the horse and caring for it may provide an ideal learning environment for acquiring cognitive strategies. It is hypothesized that the sensory stimulation of both the ground-level and mounted activities can help to modulate physiological arousal levels, also improving attention and engagement in the activity. The immediate feedback that the rider receives from the horse enables physical and mental self-regulation. 27 Finally, an intervention that includes both horses and riders in various forms can be tailored to address many difficulties present among children with ADHD.
To date, few studies have systematically examined the effects of the different EAS on children and youth with ADHD. Pérez-Gómez et al. have conducted a systematic review aimed to examine the EAS effect in ADHD-diagnosed children, comparing studies of methodological quality and therapeutic protocols. 28 This updated systematic review aims to summarize the current evidence supporting the various EAS to improve the core symptoms of children with ADHD in light of the International Classification of Functioning, Disability, and Health (ICF).
The specific research questions are as follows: (1) Which body functions and structures, as well as participation limitation and QoL, are successfully addressed by the various EAS among children with ADHD and (2) which EAS have been found successful at ameliorating core symptoms of children with ADHD? The results of the current review will help form the scientific basis for developing suitable interventions to address various difficulties presented by children with ADHD, as well as to determine which EAS are best suited to treat the individual manifestation of ADHD presented by individual subjects. It will also indicate future research needed regarding this population.
Methods
Search strategy
This review was conducted according to the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 29 (PRISMA checklist in Supplementary Appendix SA1). Relevant literature was first identified through electronic searches. A comprehensive and systematic search of relevant databases (PubMed, Cochrane Database, Web of Science, and Google Scholar) was conducted to identify original studies published in peer-reviewed journals in English from inception to December 2020, which explored the use and benefits of EAS for children and youth with ADHD.
A literature search was conducted using medical subject heading (MeSH) terms and a combination of several keywords (e.g., “attention” [MeSH] OR “attention deficit disorder with hyperactivity” [MeSH] OR attention deficit AND “therapeutic riding” OR “equine-assisted therapy” OR “hippotherapy” OR “equine-assisted activities and therapies” OR “horseback riding” OR “equine-assisted learning” AND “child” [MeSH] OR child* OR “adolescent” [MeSH]). Since the optimal terminology for services that incorporate horse 17 was published after completing the search, the authors used previous common relevant terms. Further relevant articles were identified by manually searching the references of retrieved articles. The complete search strategy of PubMed can be found in Supplementary Appendix SB2.
Study selection
Two independent investigators (Y.G. and A.H.) assessed study eligibility. The two reviewers extracted the following parameters from each study: first author, year of publication, study population characteristics, study design, and nature of the EAS (e.g., which EAS it was, duration, frequency, goals, and outcome measures). A third reviewer was considered to adjudicate on differences of opinion, but this was not required because a consensus was reached. The studies were also examined to identify and isolate clusters reporting the same data, so as to avoid the risk of bias. 30
The PICOS (participant, intervention, comparison, outcomes, and study design) framework was used to develop inclusion and exclusion criteria for the review. Inclusion criteria were as follows: participants (a) all participants in the sample were children or adolescents (up to 18 years) diagnosed with ADHD; interventions: (b) EAS protocol was described in the research article; comparison (c) control groups for interventions were not restricted and studies were considered for inclusion if they used preintervention measures; outcomes (d) studies included outcome measures that can be categorized according to the ICF; and study design (e) any study design was considered for inclusion dependent on whether EAS intervention was carried out.
The following types of studies were excluded: (a) studies with a mixed sample of adults and children; (b) reviews or theoretical articles; (c) case studies; and (d) studies' full text was not published in English.
Linking to the ICF
The ICF provides a scientific basis for understanding and studying health and health-related states of people, by establishing a common language to facilitate communication and information transfer across health professions. The authors followed a three-step procedure for data processing and linking all studies (n = 12) to the ICF as follows: [1] extracting study general information—age of participants, gender, study design, and intervention characteristics; [2] identified the outcome measures; and [3] linking the outcome measures to the appropriate ICF domains. 31
Two investigators (Y.G. and A.H.) independently linked each measure to the domains of the ICF and a consensus reached by discussion. The ICF domains include the following: (1) functioning and disability related to the ability or inability to perform critical ADL, including body functions (a), body structures (b), activities and participation (c); and (2) contextual factors, including environmental and personal factors (d). 31
Body functions are described by the ICF as physiological and psychological functions of the body systems. Body structures are anatomic parts in the human body and their components. 31 These include neuromusculoskeletal and movement-related functions that relate to movement, and mobility involving joints, bones, reflexes, and muscle function. 31 Activity is defined as execution of a task or action by an individual, while participation is defined as involvement in a life situation. 31 Contextual factors include the individual's background features that are not part of a health condition or health state. They include age, gender, socioeconomic state, lifestyle, habits, education, past and current experience, and other characteristics that may play a role in disability at any level. Environmental factors make up the physical, social, and attitudinal environment in which people live and conduct their lives. 31
The World Health Organization has conceptualized QoL as an individual's perception of his or her health and health-related domains of well-being. 31 It can also be defined as the subjective perception of happiness or satisfaction with life in domains of importance to an individual. In this respect, many researchers equate QoL with functioning, or base their assessments very heavily on participation. 32 Despite the link between QoL and participation, QoL was not captured in the current ICF. However, because QoL is considered to be an important issue in the field of child health 33,34 and is a long-term goal in therapeutic interventions, the authors described QoL findings in the context of EAS for children with ADHD.
Evaluating the study quality and risk of bias
Due to the need for quality control of evidence, the authors assessed the risk for bias by using the physiotherapy evidence database (PEDro) scale 35 and the Newcastle–Ottawa Scale (NOS), 36 as well as the Oxford Centre for Evidence-based Medicine (OCEBM). 37 Two independent reviewers (authors Y.G. and A.H.) completed the checklists based on these scales, to prevent the risk of assessor bias. Discrepant scores were resolved by discussion and consensus. Since this review reported the results of only 10 studies, all levels of evidence were included. Assigning lower levels of evidence to some studies does not cast doubt, per se, on the validity of the results for the population studied in those particular investigations, but rather raises concern for the degree to which bias might affect the generalizability of the findings. 38
The PEDro scale rates controlled trials based on random and concealed allocation of participants; similarities of the participants at baseline; blinding of subjects; therapists and assessors; dropout rates; the use of intention-to-treat analysis and reporting point measure; measures of variability; and between-group statistical comparisons. A total score out of 10 was derived for each study, based on the number of criteria satisfied. Studies with PEDro scores ≥5 were considered at low risk for bias and moderate to high methodological quality 39 and were included in the analysis. Higher scores indicated better quality of evidence. 40
The NOS 36 was used for assessing the quality and the potential for bias of nonrandomized studies in three areas: participant selection; comparability; and outcome. 36 This is one of two tools recommended by the Cochrane Collaboration to evaluate the methodological quality of nonrandomized studies 30 and provides good performance with greater ease of use and more specific criteria relating to observational studies. 41 Using the NOS tool, each study is judged on eight items, categorized into three groups: selection of the study groups; comparability of the groups; and ascertainment of either the exposure or outcome of interest for case–control or cohort studies, respectively. The highest quality studies are awarded up to nine stars. The authors considered studies with zero to three, four to six, and seven to nine stars to represent low, moderate, and high quality, respectively.
All studies were also classified according to their level of evidence by using the classification proposed by OCEBM: a hierarchy of the likely best evidence, designed so that it can be used to find the likely best evidence. The OCEBM Levels of Evidence was designed so that in addition to traditional critical appraisal, it can be used as a heuristic by clinicians and patients to answer clinical questions quickly and without resorting to preappraised sources. It allows to appraise evidence for prevalence, accuracy of diagnostic tests, prognosis, therapeutic effects, rare harms, common harms, and usefulness of (early) screening. It is divided into five levels of evidence, level 1 the highest and level 5 the lowest. 37
Results
Figure 1 shows that the literature search provided a total of 739 articles in the electronic databases: PubMed (n = 13), Cochrane Library (n = 4), Google Scholar (n = 719), and Web of Science (n = 3). After discarding duplicate articles, 5 were excluded because they were written in a language other than English, and 680 were omitted because they clearly did not meet the inclusion criteria. Following this first extraction, 30 articles were obtained and reviewed. Conference proceedings were excluded as well (2). Thus, a final total of 12 articles that met the eligibility criteria were included in this systematic review. The interventions in the included studies are named according to the EAS terminology as used by the authors, most of which use the former terminology of EAAT.

The preferred reporting items for systematic reviews and meta-analyses flow diagram.
Table 1 summarizes all the evidence from included articles relating to EAS according to the ICF model and presents the risk for bias and the quality of the evidence according to the PEDro or NOS and OCEBM rating scales.
Summary of the Characteristics, Quality Assessment of the Methodology, and Outcomes of the Included Studies (n = 12)
Significant statistical improvement.
Mean age includes standard deviations.
ADHD, attention-deficit/hyperactivity disorder; Age, range in years; ASD, autism spectrum disorder; BDNF, blood-derived neurotrophic factor; DCD, developmental coordination disorder; EAAT, equine-assisted activities and therapies; EAPT, equine-assisted physical therapy; EAS, equine-assisted services; EF, executive functions; NOS, Newcastle–Ottawa scale; OCBME, Oxford Centre for Evidence-based Medicine; PEDro, physiotherapy evidence database; QoL, quality of life; RCT, randomized-controlled trial; TR, therapeutic riding; X, nonsignificant effect.
Quality of included studies
Of the 12 included studies, all were quantitative. Only 6 out of 12 studies had control groups, and thus, the remaining 6 scored with high risk of bias. The authors found great heterogeneity among the included studies, in terms of sample sizes, intervention protocol, and study designs, which might result in high bias from other sources.
Five of the trials were controlled, and therefore rated according to the PEDro scale; those scores ranged between 5 and 7 points out of 10 (mean 6.4 ± 1.67), which reflects moderate-high methodological quality. 39 The remaining seven trials were not controlled, and therefore rated according to the NOS. The mean quality score for the NOS was 5.28 ± 1.6, indicating moderate quality on average. Regarding the OCEBM, nine studies were rated at level 3/5, while the other three studies were rated at level 2/5.
Outcome measures
The outcomes assessed in the 12 studies together covered all three of the ICF domains: impairments of body structure and function, activity, and participation (Table 2). Of the 34 multiple-item measures linked to the ICF, the ADHD rating scale for core symptoms assessment 42 was the most frequent measure used (four studies, 11.7%), followed by the Clinical Global Impression scale (three studies, 8.8%); and functional magnetic resonance imaging (fMRI) and electroencephalogram (EEG) for assessing symptom severity (three studies, 8.8%).
Total Number of Studies Assessing Outcomes Within the Domains and Categories of the International Classification of Functioning, Disability, and Health
Most ICF outcome measures were used to assess body function and structures (52.9%), while fewer (20.5%) were used for activity and participation, including social behavior and maladaptive behavior, and QoL. Only a few of the measures covered most of the ICF components, including body functions, activity and participation, environmental and personal factors. The content of measures differed significantly in their representation of the ICF chapters in all components. As some researchers included comorbidity, some outcome measures referred to other diagnoses such as ASD. Where instruments contained subscales and several items, these were individually assigned to the relevant category (Table 2). Contextual factors were not assessed separately.
Using the ICF as a framework, the codes and categories within health and health-related domains relevant to ADHD were first identified. Second, the outcomes assessed in the 10 retrieved studies were mapped to the relevant domains and categories of the ICF (Fig. 2).
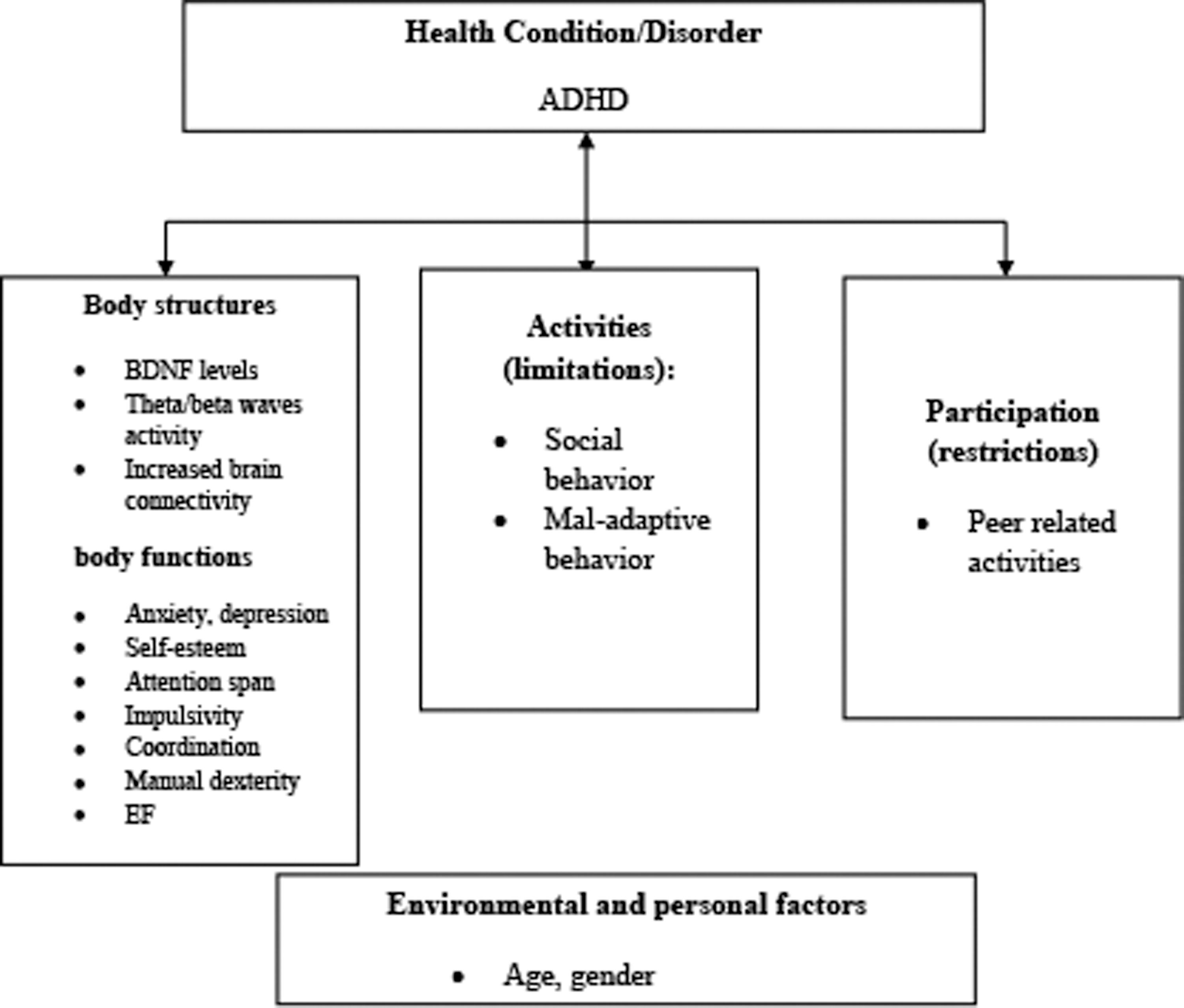
ICF health-related domains relevant for ADHD identified during the study. ADHD, attention-deficit/hyperactivity disorder; BDNF, blood–brain-derived neurotrophic factor; EF, executive function; ICF, International Classification of Functioning, Disability, and Health.
Effects of various EAS on body function and structures
EAS were found to be beneficial among children with ADHD with respect to the following body functions and structures:
Mental function
TR (n = 4) and EAPT (n = 6) studies have shown that riding offers an opportunity for success that raises global mental functions such as self-confidence, self-esteem, and motivation. 27,43 –45 In addition, EAPT studies (n = 3) showed an improvement in specific mental function. For example, a significant increase was found in memory functions of the left bilateral middle frontal cortex, right bilateral middle frontal cortex, and left precentral cortex. 44 Improvements were found in specific core symptoms, including hyperactivity, impulsivity, and inattention using the ADAD rating scale, 46,47 however, one study showed no improvement in the attentional test.
Studies used equine-assisted Occupational Therapy (OT) and TR, found improvement in EFs, especially in monitoring, working memory, and initiation. 45,48 These two studies used the Behavior Rating Inventory of Executive Function 49 a valid questionnaire for EF assessment among children with ADHD. 50 However, another TR study, which included unmounted activities and riding, found null results in core symptoms' improvement. 51
Neuromusculoskeletal and movement-related functions
A study with five children ages 10–11 years participating in 16 sessions found an improvement in motor performance. 43
Metabolic functions
One study assessed the effect of 32 TR sessions and found a decrease in body fat in insular areas. 44
Nervous system functions
The influence of EAS on the nervous system was demonstrated in five studies using three different objective outcome measures (e.g., fMRI, EEG, and blood testing). 27,44,46,52,53 Blood–brain derived neurotrophic factor (BDNF) plays a key role in nerve-cell dopamine receptors, which is thought to affect core symptoms in ADHD. In a study including 16 children that lasted 16 sessions of combined EAPT and neurofeedback training, a significant increase was found in the BDNF level in the research group, which may indicate brain function improvement. 54 Another study showed similar results after 32 sessions without neurofeedback using a control group. 44 fMRI was used in three studies and demonstrated decreased activity in the right precentral cortex, where more neurotransmitter activation is found, 50,52 in addition, cerebellum activation was increased after EAPT. 44
Effects of EAS on activity and participation
EAS (n = 4) have been found to enable participation in activities in the following domains:
Interpersonal interactions and relationships
There is evidence of social behavior and participation improvement following EAPT among children with ADHD. Social behavior traits targeted for improvement included immature behavior, clinginess, not getting along with peers, clumsiness, and preferring to play with younger children. 46 A study that included TR and unmounted activities reported significant changes in maladaptive behavior, which decreased after six sessions of 3 h each. Significant improvement in empathy was also found. In addition, another study, which also incorporated unmounted activities and TR sessions, found moderate improvement in interpersonal relationships. 51 However, another study found no improvement in socialization and communication skills after a 5-week TR and unmounted activities. 55
Regarding social role behavior, an improvement was found in emotional symptoms and conduct problems relative to before the TR. 43 It is important to mention that some results have been reported by teachers and some by parents and thus have the risk of bias as they do not hold both reports.
In the ADHD population, there was improvement in self-regulating behavior after TR sessions 44 and in the behavioral inhibition system, 53 as well as improvement in occupational performance and occupation-based goals after equine-assisted OT. The functional goals were related to education (e.g., doing homework independently), self-care (e.g., performing morning routine on time), and leisure and socializing (e.g., engaging in a soccer game with friends in the afternoon). 48 In another study, statistically significant improvement was found in anxiety and depression measures, as well as learning disorder improvement following TR sessions. 27
Contextual factors
The EAS take place in the physical surroundings of the stable: a nonconventional treatment environment that might encourage therapeutic engagement. By involving animals and instructors, who are not perceived as a part of the medical or clinical world, the stigma of treatment is removed. 56 In this review, however, no research was found examining the specific effect of various EAS on other personal factors.
An important and unique issue relevant for EAS is the safeness of the intervention in the stable surroundings. Six studies reported safety considerations taken in advance to prevent adverse events. They specified safety equipment supplies for riders such as helmets and harnesses and safety education, as well as the use of proper trained horse adequate for the EAS intervention. 27,44,47,52,54,55 No safety events have been reported in all included studies.
Quality of life
The authors found that despite the importance of QoL as an outcome measure, the impact of EAS on QoL was tested in only four studies using different outcome measures, which might increase bias. 43,45,47,51 The intervention included TR and EAPT, demonstrating that all three can enhance QoL aspects. An improved QoL was reported both by children and parents in two studies. 43,45
Discussion
This systematic review summarizes the literature, namely, 12 peer-reviewed studies that met the inclusion criteria, which investigated the effectiveness of using EAS, defined broadly as various interventions incorporating horses for children diagnosed with ADHD, using the ICF concepts and terms. Using the ICF, it is possible to describe important and meaningful aspects of function and intervention outcomes among children with ADHD. It is easy to understand why these domains and factors play such important roles in the potential outcome of any health intervention.
Most of the studies that the authors examined investigated the effects of various EAS on body structures and functions, with an emphasis on the motor, sensory, and psychological areas. These studies are based on bottom-up rehabilitation approaches, which act on the distal physical level and aim at influencing the central nervous system. 57 These are believed to be prerequisites to successful occupational performance or functioning. 58 Some of the studies addressed activity and participation, and QoL.
Altogether, the reviewed studies showed moderate methodological quality, while five studies demonstrated moderate-high methodological quality. Studies showed mostly positive outcomes, which support the use of different EAS for promoting body functions and participation among children with ADHD. The current results shows that EAPT studies had greater influence in terms of body functions and structures, especially improvement in specific mental functions, 44,46,47,53 even in distant environments outside the stable. 48
It is hypothesized that the effect of the interventions on body function and structures derives from two main sources. First, the riding itself provides unique sensory input and encourages motor response during the movement. 59 The horse's pelvic movement during its walking pace has a rhythmic three-dimensional step that mimics the movement of the human pelvis, and therefore, it provides the same form of motor, sensory, and proprioceptive input that is received during the human walking gait. 44,60 –63 The rider must learn how to adjust his or her body and align it with the horse's body.
Second, riding requires the rider to calm his/her senses and pay attention, to succeed in giving the correct body signals for asking to walk, run, or halt; otherwise, the horse will not perform the task the rider requires. It is also assumed that when riding is performed on different terrains and in varying rhythms (walking, running, and cantering), it requires focus on matching the range of attention to the different activities; it therefore helps to improve the attention span. 64 In terms of body function, however, studies regarding the effects of EAS on cognition, intellectual processes, temperament, and other nonphysical functions are still needed.
EAS are also assumed to promote participation through various psychological benefits. 65 These improvements have been found in most TR interventions, incorporating unmounted activities (currently classified as EAL) with the horses, rather than solely riding them. 27,43 TR has been shown to improve social interactions, maladaptive behaviors, and interpersonal relationships. 51,55
There are several hypotheses regarding the mechanisms of EAS in promoting participation. First is the interaction that occurs in the stable, both with the horse-riding instructor and with other riders. The relationship established between the rider and the horse is an important aspect in the riding process. It is assumed that bonding with the horse makes allowances for the rider's difficulties in a nonjudgmental context. 25 The second is the set of tools and skills that the rider acquires during the intervention that can be transferred to other contexts and interactions outside the stable. Some evidence has shown generalization of treatment outcomes following EAS to the home and community environments, as well as to the classroom.
It is worth noting that these effects were found in interventions applied by licensed therapeutic professionals. 48,66 Third, EAS are perceived as a sport and not as a therapy process. 67 Riding enables the rider to perform a normative leisure activity, where the individual can express him/herself freely. It serves as a motivational stimulus to “forego” treatment. This held true among participants with psychopathologies, as well as children and adults with ASD, where social motivation, social interaction, and communication skills were enhanced following the intervention. 22,56,64
Regarding QoL, it is assumed that improving body functions and structures will improve participation in meaningful life areas, which will positively influence the individual's QoL. 58 Only three studies have shown improvement in QoL and well-being following EAS among children with ADHD. 43,47,51 Interestingly, these studies included EAPT and TR combining riding and unmounted activities. Those results are nevertheless in line with others that assessed the impact of EAS on QoL among children with cerebral palsy and intellectual disability. 68,69
All interventions included under the definition of EAS safely incorporate both provider and horse and sometimes involve significant others (e.g., parents, teachers). Complex interventions such as these require multiple interacting components that must be addressed in a single intervention session. As can be seen in this review, the unique intervention components (e.g., horse, environment, unmounted activities) have been shown to have some benefits in various areas, especially when performed by certified professionals and while combining unmounted activities.
Each intervention showed specific improvement in different components according to the ICF. For example, EAPT was found to be effective in improving body function (e.g., specific mental functions) and TR in activity and participation (e.g., social behavior). It should be mentioned that some studies have shown no improvement in attention, 46 self-esteem, and socialization. 27,55 These results might be explained by the fact that the TR and EAL were not performed by a licensed therapist. In addition, the authors hypothesized that these results might also relate to the combining of unmounted activities and less riding time on the horse.
Further research is needed to address the mechanisms of change involved in the various intervention characteristics. This knowledge will be helpful in developing specific modality of goal-directed interventions that can be tailored to each child. Studies that will evaluate the long-term effects and influence of EAS on QoL and participation in daily life of children with ADHD through various contexts are needed as well. In addition, combining objective with subjective commonly used outcome measures can enhance the validity of intervention and enable replication.
Limitations
While the existing evidence is from research studies, potential biases in evidence might have influenced the results. The PEDro Scale and NOS assessments have been shown to have acceptable levels of psychometric properties. 70,71 The NOS has the potential for more limited ability to detect bias in the examined studies, particularly in the areas of selection of appropriate study design, statistical analysis, reporting, and generalizability of results. 72 It is important to note that assigning lower levels of evidence to some studies does not cast doubt, per se, on the validity of the results for the populations studied in those particular investigations but rather raises concern about the degree to which bias might affect the generalizability of the findings.
Moreover, the authors excluded conference proceedings and abstracts, potentially resulting in publication bias since the proportion of studies with null findings is likely greater in those presented at conferences but not published, compared with those published in peer-reviewed journals. 30 Another potential for bias was the selection of articles written in English only, while research in other languages were excluded, as most studies have been done outside the United States or non-English-speaking countries such as Korea, 27,44,46,47,52,53 Spain, 51,55 and Iran. 73
Furthermore, the definition of each EAS intervention and attribution to each methodology (therapy, horsemanship) seemed to be unclear at times. In addition, most studies had no unified protocol within their treatment modality (e.g., TR, EAPT), and therefore, no precise way to replicate those measures and outcomes. Most studies did not specify the exact course of treatment (i.e., the number of sessions needed, group versus individual intervention, the type of horse in terms of conformation and character), but only gave general outlines of performance. These limitations might restrict the generalizability of the findings.
Conclusion
Over the past 20 years, only 12 studies were found evaluating EAS among children and adolescents with ADHD. Most research has shown the positive effect of EAS in terms of body structures and functions, activity and participation, as well as QoL. Specifically, it has been found to improve the core symptoms of ADHD, such as hyperactivity, impulsivity, and inattention, especially during EAPT sessions and interventions. 46,48,53,74 Positive changes were also seen in participation, especially in social integration during TR session and unmounted activities with the horses. 46,55 However, despite the research and evidence gathered on the effectiveness of various EAS among children with ADHD, there is yet a long way to go until solid verification is established.
Future studies that will examine different EAS can be valuable to promote the understanding of unique mechanisms of change within each treatment modality. This will allow us to establish a better-suited and tailored intervention for each individual. Understanding the meaning of a multimechanism and complex intervention is also crucial for setting treatment goals and outcomes. Within the existing studies, most of the samples were small and the criteria for the various impairments were inconsistent. Hence, larger RCTs are required to confirm the current evidence and provide more data on EAS outcomes for children with ADHD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The work submission is the authors'. This review did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SB2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.