
Abstract
Introduction:
This article examines the feedback of health care providers within the implementation of an integrative care project in a clinic for pediatric oncology in São Paulo, Brazil. Since 2017, the project has implemented external anthroposophic therapies in the activities of daily nursing. The objective is to evaluate how the project evolved and what impact it had on the daily operation of the hospital. A special focus emphasizes the perspective of study nurses.
Materials and Methods:
Twelve qualitative semistructured interviews were conducted. Audio files were transcribed, translated to German, and underwent a MAXQDA software-assisted analysis. Using a thematic approach, coherent cross-case topics were defined.
Results:
Three main topics emerged from analysis of the data. (1) The implementation and its effects on daily patient care demonstrated positive outcomes in patients and were well accepted with minimal changes in daily activities. (2) The perspective of study nurses showed a large motivation due to beneficial and stress-relieving effects of the application and a growing patient–health care provider relationship. (3) Problems and aspirations for improvement were the lack of time and the urge to make the project grow in the future.
Conclusion:
Not only patients but also health care providers seem to benefit from integrative methods. They have the potential to improve the working atmosphere and to strengthen relations between patients, caregivers, and family members. General feedback was positive and acceptance in the team arose over time when beneficial effects became visible.
Introduction
While the mortality of children with cancer in Brazil is declining due to the application of modern combination chemotherapy concepts, 1 patients are still confronted with acute side effects and long-term consequences of the therapy. 2 –4 For instance, chemotherapy can cause direct associated symptoms such as nausea, stomachache, fatigue, infections 5 or back pain from being bedridden. 6 Mood changes or sleeping disorders have also been described. 7 A U.S.-based study found that 86% of pediatric patients suffer discomfort or pain while being inpatient. 8 This distress is often treated with medications that play an important and undisputed role, 6 although some symptoms remain intractable. 9 Complementary and integrative medicine (CIM) may support conventional pharmacological and non-pharmacological treatment and reduce inpatient suffering and common side effects such as pain, anxiety, nausea, and fatigue. 10 –12 CIM combines traditional and complementary methods with conventional medicine for a patient-centered holistic approach. 13 An underlying concept is Anton Antonovsky's theory of salutogenesis 14 that defines health as an active process promoted by so-called salutary factors, not just the absence of disease. One of these salutary factors is the sense of coherence (SoC), a holistic approach that helps in overcoming challenging situations in life. Comprehensibility, manageability, and meaningfulness are key dimensions in the SoC and can be understood as adding an understanding, empowerment, and sense to the perception and handling of a disease. 14 In CIM this understanding of health applies not only to patients but also to health care providers. 15 It, therefore, makes use of different complementary therapies from whole medical systems such as Traditional Chinese Medicine, Ayurveda, and anthroposophic medicine, for example, phytotherapy, mindfulness, and music or art therapy.
At the same time, there is growing interest in CIM by patients and their families. 16,17 In Brazil, a cross-sectional study found a prevalence of CIM use of 4.1% in the general public 18 and 7.5% in patients with chronic diseases. In the pediatric area a study found that 41% of patients with type 1 diabetes in Brazil make use of CIM, often without the knowledge of their physicians. 19 In 2006, the Brazilian government integrated CIM practices into the public health care system, 20 while institutions started to offer CIM practices in daily clinical care. 21,22 Regardless of the increased use, a Brazilian literature review from 2019 on the implementation, access, and use of CIM practices in the Brazilian public health care system found that 52.94% of it occurs in a primary health care setting. 23 The authors explain the absence in secondary and tertiary care with a gap of knowledge and skepticism due to the lack of scientific evidence. This concludes that there may be a demand for further research. Especially in the pediatric area few descriptions of implementation processes exist. 24,25
The authors' group conducted a project based in the pediatric oncology intensive care unit (ICU) of a German University Hospital 26 –28 and developed an integrative care program (Charité Integrative Pediatrics program) that could be shared and implemented in other pediatric settings internationally. In this project, nursing therapies that derive from an anthroposophic background such as embrocations, warm compresses, poultices, and wraps with essential oils were introduced into the daily care of pediatric oncology patients. Through multisensory stimuli such as touch, warmth, and smell, these so-called external anthroposophic therapies (EAT) have the pursuit to contribute to patients' well-being and was found to be well accepted by families and staff. 29
At the Childhood Cancer Treatment Institute (Instituto de Tratamento do Câncer Infantil [ITACI]), which is a public hospital with a specialized pediatric oncology unit at the Children's Institute of the University of São Paulo Medical School in Brazil, a similar project has been introduced in collaboration with the Charité Integrative Pediatrics program as essential part in the emergence of a unit dedicated to integrative pediatrics. 21 In this study, the authors investigated this implementation of EAT in a university-based pediatric oncology clinic in Brazil.
Using qualitative interviews, this article outlines the overall effects and potential problems related to the implementation of an integrative care into normal medical pediatric practice based on the feedback of health care professionals. Furthermore, the authors present the perspective of study nurses who were part of the project.
Materials and Methods
Study design
Originally, eight nurses of ITACI and nineteen other nurses from other institutions in primary care and hospital care were trained in EAT in September 2017 by two experts of anthroposophic care from Havelhöhe Hospital in Berlin. Currently, six study nurses continue to apply EAT using an indication list, which is based on the Charité Integrative Pediatrics program (Fig. 1). This takes place unregularly throughout the ward, ICU, and the bone marrow transplantation unit in dependence of spare time during the shift of study nurses. Cases were selected where EAT were applied and subsequently discussed within the trained team.
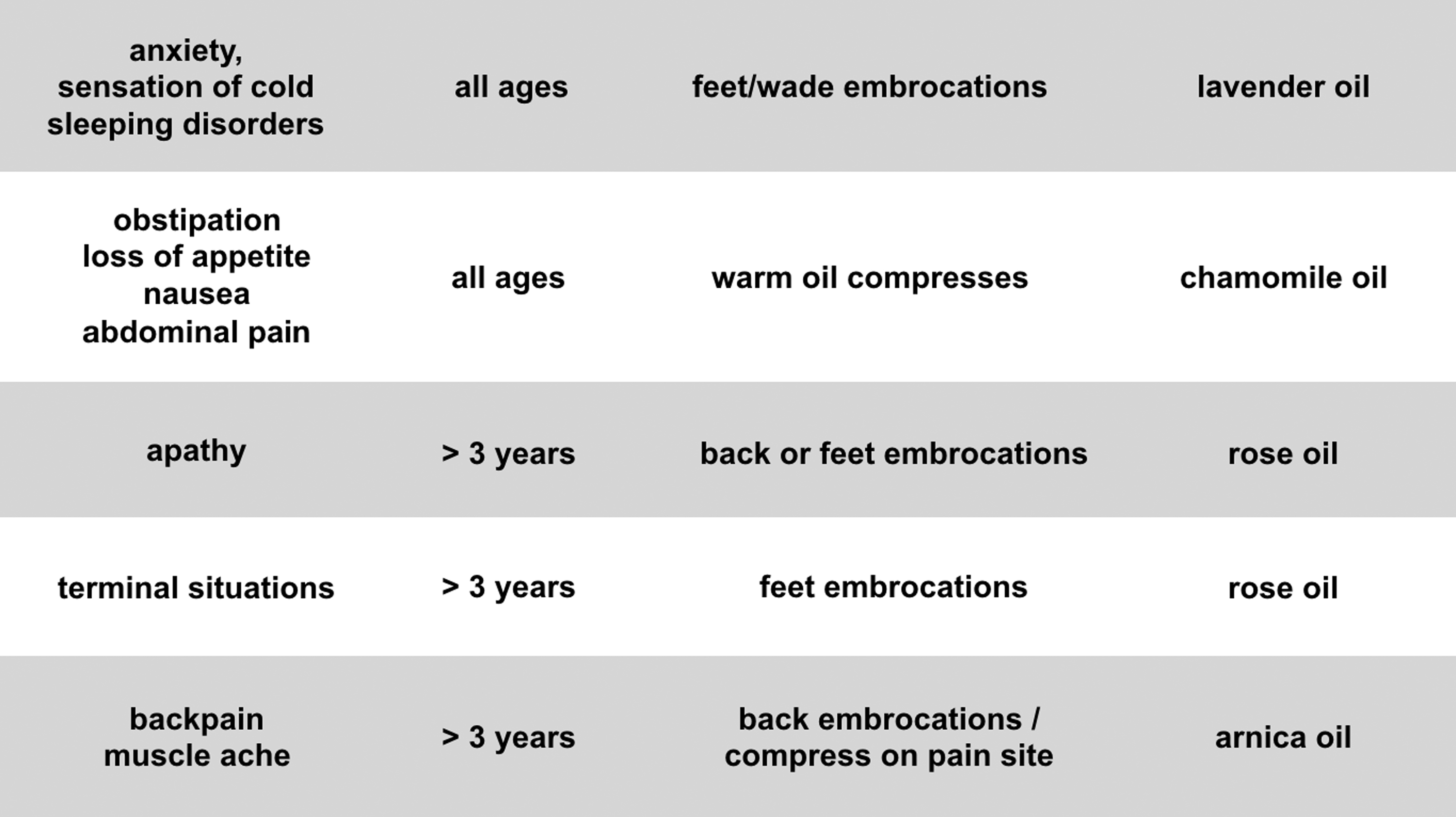
Extract of the list of indications. 21
To evaluate the perspective of health care professionals and family members who were connected with EAT, a qualitative study design based on a focused ethnographic approach, 30 including participant observation and semistructured interviews was chosen to provide deeper insights of the participants' experiences and opinions. Therefore, an external researcher (M.T.) visited the ITACI for 3 months. Participant observation, informal conversations, and semistructured qualitative interviews were carried out in between August and October of 2019. The ethical approval was granted from the Ethical Committee of the University of São Paulo (35592920.2.0000.0068).
Sampling
The authors conducted 12 interviews with staff to gather in-depth insights within the 3-month fieldwork time constraint. To facilitate the study and data collection (M.T.), a researcher and study nurse (K.P.) helped by intermediating between M.T. and potential participants. From August to October 2019, K.P. helped to recruit personnel and family members. Written consent was obtained for all participants. Anthroposophically trained and nontrained staff were recruited. While not directly part of the project, nontrained staff also had contact with the treated patients. Saturation of the data set was considered complete as it included all study nurses as well as an equal number of noninvolved counterparts. Participants represented all three units in which the project was undertaken.
Data collection
The semistructured qualitative interviews were held in Portuguese at the research site (ITACI) by M.T., a researcher fluent in Brazilian Portuguese and trained in qualitative interview techniques at Charité Universitätsmedizin Berlin. The questions consisted of a general knowledge and description of the project, perceptions and experiences of integrative care, and focused on the anthroposophic techniques used in this pilot project. Staff interviews addressed changes in work ambience, workload, changes in the relations with patients, as well as of mood and daily routine in the units of ITACI. The interview guideline was based on the reference study at Charité Universitätsmedizin Berlin and adapted throughout the interview process. Questions were designed to be answered from a broad range of experience and interviewees were encouraged to give extensive answers with little interruption.
Participant observation is a scientific method of data collection deriving from ethnographic research through which observations, informal conversations, and human interactions are documented. 31 Everyday clinical and care practices, patient and provider interactions, as well as informal conversations were documented in field notes by M.T. during the 3 months at the clinic. The observations were used to understand the context of the research site and to further adapt the interview guidelines throughout the data collection and hence increase validity. In addition, they were used to broaden the picture of each interview.
Data analysis
Interviews were audio-recorded, transcribed verbatim, and translated from Portuguese to German by M.T. Emphasis was on keeping semantics and content of the interviews as original as possible while adapting to the German language. Translation was needed to share the content with the research team. All personal data were pseudonymized. A thematic analysis approach 32 was used to define coherent cross-case topics. The German transcripts were entered into the qualitative analysis software MAXQDA and read intensively and summarized to get a deeper understanding of the gist. Then interview segments were coded line by line. A code system was constructed by combining deductive themes that originally derived from the interview question guideline and salient themes that emerged during inductive analysis. To increase research rigor, the approach and code system was refined throughout the process and was regularly discussed within the research team. Observation notes were used in the analysis process both at the beginning to understand salient themes about the program and also used during analysis of the transcripts to triangulate the information that was given in the interviews. Furthermore, the results were presented and discussed within the qualitative research group at the Qualitative Research Network at Charité Universitätsmedizin Berlin for further validation.
Results
A total number of 12 interviews were conducted: 6 with anthroposophically trained study nurses, 3 with nontrained clinic nurses, and 3 with physicians. On average the interviews were 30 min in length. The following main topics emerged in the analysis (Table 1).
Participants
The implementation and its effects on daily patient care
The interviews demonstrated how new techniques were welcomed and general acceptance by staff was positive (Table 2). Some staff articulated how they were skeptical about the necessity and the benefit at the beginning of the project, yet most stated that their support grew after the project evolved and demonstrated the first positive effects. Furthermore, interviewed staff argued that the fact that EAT caused no harm contributed to the overall acceptance.
The Implementation and Its Effects on Daily Patient Care
EAT, external anthroposophic therapies.
I'll admit, I don't think everybody thinks it's gonna work. But they believe that it'll help and doesn't hurt their wellbeing and so it's welcome. (Physician)
At the same time, other clinic health professions such as physicians or physiotherapists began to engage more in informal discussions about the cases as they became more aware of the EAT project. The participants stated that communication had improved through such exchanges and that they enjoyed these interdisciplinary consultations.
And we find that this makes a big difference. And it was all done together. Physical therapy gave their opinion, so did the medical team. (Study nurse)
Changes in daily procedures in ITACI were minimal, as the project was in the initial stages and run in parallel with other daily tasks that are not affected. Participants reported they noticed a change in the clinic atmosphere. Some interviewees described the EAT as establishing a more “humanistic” environment. Employees involved in the project reported that their view of the patient had changed over time and become more holistic. They described this as beginning to view the EAT not only as a separate treatment but an integrated part of patient care therapy collaboration.
But we saw and learned that the patient isn't just made up of a body, but also has a soul with wishes and needs to consider. (Physician)
Nearly all of the interviewees said that they perceived effects in the patients during or after the EAT treatments.
Patients appeared calmer, less anxious, and had fewer sleeping problems. Sometimes the treatment helped to alleviate pain.
Patients who are not doing well, who are under palliative treatment, they feel much better after the massage. They are calmer. It seems to calm them, and their body is able to relax. (Clinic nurse).
Even when EAT had not diminished symptoms per se, interviewed staff reported that the children were more satisfied and in a better mood. Two of the physicians justified that the change in mood made patients easier to approach and, therefore, more accessible. For staff, the change eased the inpatient handling and enhanced compliance during subsequent treatments.
And after they have had a massage, for example, they are able to have a conversation or are more responsive because they feel better. It makes the work we do easier. (Physician)
The physicians viewed the integrated treatment as complementary to and maintaining the status quo of conventional therapy. In some cases, they stated that the alleviation of pain, anxiety, or nausea was so effective that a reduction of analgesics, antiemetics, or sedatives was possible. Some patients did not like a specific smell of the oil or declined treatment, but most interviewees said that patients asked for repeated treatment after receiving it once.
Most people keep asking for it. They don't want it to stop. They always want more and sometimes we even can't keep up. (Study nurse)
The interviewed study nurses reported that in general the feedback of families was very positive because they did not see EAT as just another drug or a treatment associated with discomfort. Hence, nurses experienced that parents were more motivated for their children to accept EAT. In general, interviewed staff underscored that family members were also very interested in the treatment techniques. Study nurses mentioned that some were given background knowledge of the methods and a little bottle of oil to enable them to practice massages on their own.
The families expressed to the interviewed staff an appreciation of how the EAT led to physical and mental improvements in their children. This sentiment was supported by informal conversations the authors had with relatives during the participant observation on the ward. Mothers of inpatient children told the authors they experienced their child as being calmer and relaxed after the treatment.
The use of EAT had impacted the relationship between practitioners and patients. In interviews study nurses explained that they felt a stronger connection and how they had the impression that this extended to the parents, increasing trust in the nursing staff.
Perspective of study nurses
Among the study nurses, some were interested in the treatments from the start while others were chosen because of their administrative roles (Table 3). All emphasized how they witnessed an evolution of their knowledge and attitude toward EAT. One study nurse explained that she liked it because of the different and more humanistic approach.
Perspective of Study Nurses
It was where I was able to show a more human side […] So for me it is a switch from everyday routine and a focus on the benefits I can provide for myself and what I can offer the children and families. For me this is a very good thing. (Study nurse)
One motivation highlighted by the study nurses derived from the ability to switch roles from treating pain or illness, to contributing to comfort and well-being of patients. In return they underscored that this was affirmed by the positive feedback and the trust they received.
Study nurses stated how they enjoyed this relationship progression with their patients and how intimate moments afforded a refuge from daily stress and failure.
From the very beginning you get a sense of the interaction with the family, the interaction with the patients, which is contained in this touch. That is something special for us. I don't see that kind of interaction anywhere else. Not in other therapies, not in other tools of care. (Study nurse)
They often described this as having a cyclical effect: the patients felt better and less anxious leading to satisfaction of the nurses. In addition, they explained the stress-relieving effect of applying EAT in these tranquil moments.
Besides the professional attainment of having new care skills, the study nurses asserted in the interviews that their personal life was impacted and they started using EAT at home with their families. Furthermore, they expressed their enjoyment at being a part of a treatment care innovation and that ITACI advanced. They emphasized they were eager to publish about the positive effects of EAT that they experienced.
Some of the study nurses highlighted how they really enjoyed this new and holistic approach to their patients. Especially for terminal and palliative patients, the application of EAT created a sacred space that eased the situation for everyone.
She picked the music, she relaxed there in bed and we massaged her feet. The father cried and gave thanks for making such a big difference. The child died that very same day. For days she hadn't been able to relax. (Study nurse)
Appreciative of the positive patient response, this study nurse tied this to their motivation to learn more about the methods and anthroposophic theory.
Problems and aspirations for improvement
The broad high level of satisfaction reported about the project was not without mentioned need of improvements (Table 4).
Problems and Wishes for Improvement
Structural problems with lack of time and personnel were the most frequently listed problems in the interviews.
Interviewees stated that as a public hospital with limited funding, constraints on the ITACI through third-party funds were made clear during the project. Understaffing or a high fluctuation within staff were also noted challenges of the working conditions in the public hospital system. Specific to the project, material resources and specific oils often became scarce and needed to be handled sparingly.
The study nurses entrusted with administrative tasks were observed to have a greater workload in oncologic nursing, and time for the application of EAT was limited. Some clinic nurses described this double role as an overload of work. One study nurse expressed particular frustration at not being able to meet the demand.
So if you try to fit it in and then your shift ends and you failed to manage to do it, I find that burdensome. It's frustrating. (Study nurse)
The schedule of other treatments often thwarted EAT planning as did mood changes or limited availability of practitioners.
In addition, the ability to provide EAT was mentioned to be sometimes hindered by clinical limitations to treat patient-related problems. Especially patients in the ICU, who often suffered from skin rashes or immune deficiency, were unable to be treated with EAT. Aromatherapy was mentioned as a possible alternative to treat these children.
The participants voiced various recommendations for improvement of EAT to solidify treatments in the clinic, and then recognized how some of this was implemented to integrate therapies into the day-to-day of ITACI, yet also must be fostered.
And I believe, how do you say, we sowed the seeds and now we need to water the plant so that it will grow. (Study nurse)
Other voiced propositions were the expansion of the trained team, as well as shifts dedicated to EAT applications, which could help satisfy the demand for EAT by medical patients. Some participants imagined an expansion of the project to the day clinic to be useful. However, this would be limited by both time and space. This implementation would need an isolated room to provide the tranquility needed.
The physicians expressed that they would like the therapies to be integrated into their daily work and also wished for an expansion of competence of the care team to take a lead role in implementing EAT. Still, some parts of ITACI were observed to continue to lack information about EAT. One physician of the ward indicated that he did not foresee it as becoming part of the routine, but supported the project.
The clinic nurses interviewed clearly supported participating in and potentially being trained.
I think that there should be more courses to involve the team in the therapies so that the whole nursing team can be trained. So everyone can start contributing to the project. (Clinic nurse)
Looking into the future, most interviewees stated that every pediatric patient in oncology could benefit from EAT. All participants of the team wanted to continue the project and make it grow. They highlighted how they could imagine that one day it would be accepted as a normal discipline and part of a multidisciplinary patient care just like physiotherapy.
Discussion
The aim of this study was to show the impact that the implementation of EAT had on the day-to-day work in a pediatric oncology hospital through direct feedback of health care providers and by highlighting the perspective of study nurses. The interviews demonstrated that the reported effects were predominantly positive. Through the positive feedback of patients and family members, general acceptance can be increasingly achieved. Participants reported they felt able to improve inpatient well-being while diminishing some adverse side effects of cancer treatment. Furthermore, the use of EAT seemed to benefit practitioners as well. Caring for the well-being of their patients, nurses were appreciative of the positive feedback they received and their relationship with the children deepened. Being in an early stage of implementation, the project is confronted with organizational and structural problems while being dependent on lacking public health care resources. Still, involved personnel was found to have a high motivation for a continued evolution of EAT.
Notable were the reported stress-relieving effects on both patients and study nurses that convinced other personnel to want to get involved. The increased compliance and improved general well-being and sleep patterns of patients have been found to go in hand with positive effects described for massage therapies. 33
In the oncology setting, massages have been found to be beneficial in reducing nausea and vomiting in children with cancer. 34 A meta-analysis of nine included randomized controlled trials demonstrated a positive effect on cancer pain within adults. 35 At the same time, they are able to increase vagus tone while simultaneously decreasing cortisol levels. 36,37
This might be explained partially by oxytocin-mediated effects. Best known for its bond-strengthening role in the mother and child relationship, it can also be released through massage strokes and is associated with sedative and stress-relieving effects. 38 Through positive touch, secreted oxytocin has an important role in the parent–child bond or attachment to other caregivers and could also explain the reported deepening in the relationship. Even if there are no data available, it is conceivable that positive touch applied by EAT might induce this effect, and that this plays an important positive role also in older children and especially in extreme situations such as during oncologic treatment. Such stress-relieving and positive effects may be helpful in regard to longer time periods as chronic stress has been linked to dysregulated immune systems 39 and can be associated with various negative effects and diseases. 40 Furthermore, there is some clinical and experimental evidence that draws a correlation between chronic stress and the emergence and progression of cancer. 40 –42
Interestingly, the results show that EAT appeared to have an affect not only patients but also nurses' perception of stress. Chronic stress is a prevalent problem 43 within nursing, which is associated with decreased job satisfaction 44,45 and a higher prevalence of burnout 46 and post-traumatic stress disorder (PTSD). 47 Still, huge differences exist in the degree to which these problems are manifested within health care provision. 48 A possible explanation for this variance could be found in the concept of salutogenesis and the SoC. 14 As indicated, SoC describes a general orientation, which helps to cope with challenging circumstances in life. In a cross-sectional study SoC has been found to be a correlate in general mental health problems and PTSD within anesthesiology and ICU staff of a major German University Clinic. 49 Nurses working in pediatric oncology are especially confronted with burdensome situations and, therefore, would need efficient coping systems. 50 Some of the study nurses reported that moments of solitude with the children helped to relieve their own stress. Performing procedures such as EAT may promote regenerative resources and relieve the perception of side effects that in turn may generate the positive feedback by patients and their parents. This could possibly have a long-term motivating effect on nurses and acts as a possible coping factor here.
At the same time, it may be possible that the enhanced competency of performing the treatments further helped increase the manageability of complex treatment situations as conceptualized in the three dimensions of SoC. 14 The study nurses explained how they experienced their new skills and autonomy as very rewarding and meaningful, which may have increased their manageability. Furthermore, interviewed physicians supported the nurses taking on this role and then added this new treatment dimension to multidisciplinary case discussions. Also, other staff members started to ask for the advice and the competence of study nurses. Similar to the concept of SoC and the authors' findings, a so-called psychological empowerment through meaning, competence, and self-determination 51 was found to be associated with increased job satisfaction and reduced burnout in two systematic reviews on workplace empowerment with nurses. 44,45 This is not only of individual importance, but could be beneficial for the health care sector in general.
In this study, these visible effects on patients and study nurses seemed to have affected other personnel, spreading as acceptance increased throughout the project when positive feedback was given. This might be crucial for a successful implementation of CIM practices in the routine hospital care. Elsewhere the integration of CIM has been described as similar to the merging of two companies, where positive synergy may be achieved by the development of a new corporate culture. 52 The building of an integration team at ITACI seemed to create the development of a new work culture within the clinic. Having visible staff members from both the conventional and complementary side work to carry out the integration, have a good overview of project implementation, and exemplify good teamwork provides exemplary champions for EAT integration. In this study, the study nurses can be considered such visible champions. Education in conventional medicine and ability to adopt and implement the newly developed integrative skills of the pilot have demonstrated their ability to shoulder the responsibility and lead by example. In addition, as staff with the greatest amount of patient contact, they are most likely to directly monitor the effects on patients.
These observations are congruent with other studies. An Israeli study 53 combined the training of nurses in CIM modalities with questionnaires in which the nurses perceived themselves as mediators between patients and other staff members. Through close contact, they could likewise build relationships with the patient and better understand feelings and needs.
A comparable study to implement a pediatric integrative care program in a U.S.-American bone marrow transplant unit found a similar increased acceptance and demand from parents and patients. 25 The authors' group showed that parents are a valuable resource because of their vast interest and willingness to engage in the application of EAT. 27 Also similar to the authors' findings, study nurses felt more confident in the measures over time. In the description of the successful implementation of CIM in a German hospital, the good communication during the project and a team of motivated pioneers was highlighted.24
The biggest hurdle to the ITACI project was the lack of time. With a high level of motivation within the team, a better organization and the training of more employees, the situation could be foreseeably improved. Training parents in EAT methods to assist with their children's treatment could also potentially help counteract the lack of time during shifts.
Limitations
The qualitative interviews allowed an in-depth sample of voices and opinions on the project implementation to be voiced. However, the authors recognize that the participants, as part of this project, may already be positively disposed toward this study. Because of this, a limitation is that a wider or comparative sampling with similar or different clinics may have allowed a greater differentiation in viewpoints to emerge. These findings can only highlight a direction in which the project could evolve and the experiences made so far. Given time constraints and difficulties in approaching patients and their relatives for time-consuming qualitative interviews led to a focus on health care providers. Using a study nurse to engage participants was necessary due to the fact that M.T. was not integrated into this health system, but this approach might have influenced the selection of interview partners. Despite critical reflection of the researcher role undertaken throughout the interview phase, intercultural differences and M.T. as an external person could have created bias. The translation process might have had a small impact on statements.
Conclusion
Integrative care could be a chance to improve the inpatient well-being of children in pediatric oncology. At the same time, it could improve the work atmosphere and employee satisfaction. Especially in the often burdensome area of oncology, CIM treatments may ease stress, illness, and treatment symptoms. In addition, they may forge trust and stronger bonds between health care providers, patients, and family members. Acceptance within a team can be achieved by visible positive results and through their close contact to patients; nurses are key in this process. They, too, could benefit from integrative care through an expansion of their competencies and improved manageability of daily stress and failure. At the same time, systematic problems of care may persist, such as understaffing and the lack of time. Scaling up of such projects would afford opportunities to evaluate and research the effectiveness of such programs more broadly.
Footnotes
Authors' Contributions
Conceptualization, formal analysis, investigation, writing—original draft, and visualization by M.T. (first author). Conceptualization, methodology, validation, writing—review and editing, supervision, and project administration by W.S. Validation, resources, writing—review and editing, and funding acquisition by V.O. Resources, writing—review and editing by K.P. Validation, resources, writing—review and editing, project administration, and funding acquisition by R.G. Conceptualization, verification, resources, writing—review and editing, supervision, project administration, and funding acquisition by G.S. All authors contributed to the article in significant ways, reviewed the article, and have agreed upon the submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was kindly supported by the MAHLE-Foundation, Brazil. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; or decision to submit the article for publication. The grant number is PE 17045 S.