
Abstract
Background:
This study aimed to assess efficacy of Ardh-Matsyendrasana and OM chanting on neck pain disability and pressure pain threshold (PPT) in mechanical neck pain, compared with conventional “active stretching technique” of neck muscles.
Materials and Methods:
This study was conducted at Amity Physiotherapy OPD, Amity University, Noida (Uttar Pradesh), India, after obtaining ethical clearance from the Institutional Ethical committee. A total of 40 subjects with bilateral mechanical neck pain of subacute duration, ages 18–30 years of both genders who met the inclusion criteria were included in the study. These 40 subjects were assigned to two groups: yoga (n = 20) and control (n = 20). For four weeks, the yoga group received Ardh-Matsyendrasana along with OM chanting for 15 minutes followed by 5 minutes of hot packs. The control group received 15 minutes of bilateral active stretching of the sternocleidomastoid muscle (SCM), followed by 5 minutes of the hot pack, for four weeks. Both the groups had preintervention data (baseline) and postintervention data on neck pain and disability parameter with Neck Disability Index (NDI) and PPT measurement bilaterally by digital algometer on SCM.
Results:
More prevalence of female cases (60%) as compared with males (40%) was found in both groups. Paired t-test showed significant improvement in pain-related disability (NDI) in both the yoga group (P < 0.05) and the control group (P < 0.05). Significant improvement for the PPT parameter was found in the yoga group (P < 0.05), as compared with the control group where the result was not significant.
Conclusion:
This randomized controlled study suggested that yoga with OM chanting and active stretching exercise may be used according to patient preference for improving neck-related pain and disability. Ardh-Matsyendrasana along with OM chanting was found to be an effective intervention for improving the tenderness of muscle as compared with the active stretching exercise of neck muscles. Overall, the yoga intervention proved to be more effective in patients with subacute mechanical neck pain. This study was registered with the Clinical Trial Registry of India (CTRI) with the registration number CTRI/2019/01/016985.
Introduction
Among nontraumatic musculoskeletal disorders, the neck is the most common site for pain. Neck pain leads to substantial suffering due to functional disability 1 and reduced quality of life. It has been estimated that up to 50% of the population can expect to experience neck pain at least once in their lifetime. 2 “Mechanical Neck pain” is also referred to as “nonspecific neck pain.” 3 It is not due to any organic lesion or any underlying systemic pathology and accounts for the diagnostic categories 1 and 2 by the Quebec Task Force on Spinal Disorders classification system. 4 Conditions of neck muscles, ligaments, and joints are included with these disorders. Most patients with neck pain present with nonspecific neck pain, where symptoms have either a postural or mechanical basis. About 30%–50% of the general population is estimated to be affected by mechanical neck pain. 5,6 Onset is generally insidious with mechanical neck pain cases and it is mostly multifactorial in etiology, including poor posture, neck strain, depression, anxiety, or occupational or sporting-related activities. 7,8
As the underlying pathology of mechanical neck pain remains unclear, treatment is basically aimed at relieving pain, improving posture, and reducing muscle stiffness. Conservative treatment includes nonsteroidal anti-inflammatory drugs, use of physical agents such as heat, cold, mobilization exercises, and therapeutic ultrasound. 9 In the United States, neck pain is the second most common condition for which complementary therapies have been used. 10 A study by Furlan et al. on cost-effectiveness, side effects, and efficacy of complementary therapies on cervical neck pain found that this type of therapy was significantly effective in reducing both short-term neck pain as well as immediate pain. 11 Yoga and meditation are common complementary therapies used for treating neck pain. As an add-on approach with conventional physiotherapy, several other complementary approaches are also utilized, including OM chanting and Mind Sound Resonance Technique (MSRT).
MSRT is an advanced guided relaxation technique practiced in sitting or supine position to achieve deep relaxation of stiff neck muscles. It also improves mental concentration and can have positive impacts on health. OM chanting is included in MSRT. Yogitha and Ebnezar compared a yoga intervention with nonguided supine rest in common neck pain with 60 patients. The yoga group received MSRT after a conventional physiotherapy program and the control group received nonguided supine rest after physiotherapy treatment for 10 days. This study suggests that adding MSRT along with conventional physiotherapy provides enhanced efficacy by creating greater improvement in neck flexibility and reduction of pain. 12
According to the Upanishads, 13 the ancient Indian texts of life principles, OM (pronounced as AUM) is a combination of three letters—A, U, and M. The letter A (Akaar) is the state of waking, U (Ukaar) is dreaming, while M (Makaar) is the state of deep sleep. In the Yoga Sutra (ancient Yoga text), OM is stated as the controller of the life force. 14 Recitation of OM produces a specific modulated sound, which reduces blood pressure, heart rate, and skin resistance. 15 Some studies reported that OM chanting produces vibration in and around the ear that stimulates the auricular branch of the vagus nerve. 16 Stimulation of the vagus nerve helps to improve mood and well-being and manage depression. 17 Research has suggested deactivation of the limbic system through OM chanting 18 and that OM chanting significantly improves memory, 19,20 physiological alertness, and sensitivity to transmission of sensory impulses and increases synchronicity as well as sensitivity of biorhythms. 21
Ardh-Matsyendrasana, also known as “Half Spinal Twist Posture,” is among the most important of all postures in yoga. This posture is beneficial for various body systems, particularly the musculoskeletal system. Therapeutic indications of Ardh-Matsyendrasana include neck pain, cervical spondylitis, diabetes, and constipation. 22,23 It includes stretching of paraspinal muscles and soft tissues, which enhances spinal flexibility. This in turn provides core strength to the body. 24 –26 Inappropriate posture or weak neck muscles are the most important causes of mechanical neck pain, leading to poor curvature of the cervical and thoracic spine. Ardh-Matsyendrasana posture involves stretching of cervical and upper thoracic muscles, which in turn leads to improved flexibility and posture resulting in the beneficial effects seen in mechanical neck pain.
This study was designed to evaluate the effectiveness of Ardh-Matsyendrasana and OM chanting on neck pain disability and pressure pain threshold (PPT) in mechanical neck pain and its comparison with the conventional “active stretching technique” of neck muscles.
Materials and Methods
This randomized controlled trial was conducted in Amity Physiotherapy OPD, Amity University Uttar Pradesh, Noida, India. Ethical clearance was obtained from the Institutional Ethical Committee (IEC) of Amity University, Uttar Pradesh, Noida, India.
Inclusion criteria was patients with bilateral subacute mechanical neck pain without neurological involvement, in subjects aged 18–30, with dull aching pain increased by sustained postures, neck movement, and palpation of cervical musculature. Exclusion criteria was patients with diagnosed cases of spinal deformities, short neck, specific neck pain such as disk lesion, cervical spondylosis with radiculopathy, inflammatory disease, neoplasm, or history of osteoporosis, fracture, whiplash injury, cervical surgery, cervicogenic headache, and low back pain. The primary outcome measure was the Neck Disability Index (NDI) for assessing neck pain and disability. The secondary outcome measure was PPT with digital algometer. The treatment duration was four weeks.
Initially, a total of 48 patients were registered for the study and were randomized into two groups (yoga group and control group) after receiving their informed consent. A computer software research randomizer was used for randomization of the patients. Out of 48 patients, 3 were removed due to their nonwillingness to participate in the study and deviating from the inclusion criteria. During the study, two patients in the yoga group and three patients in the control group dropped out. Ultimately, 40 patients, 20 in each group, with subacute mechanical neck pain and satisfaction of the inclusion criteria, completed the study. After selection of the patients according to the inclusion criteria, a baseline assessment was done. Both groups received the intervention for four weeks, for five days per week, for 25 minutes per day. Baseline data and postintervention fourth-week data were collected and analyzed.
The yoga group received Ardh-Matsyendrasana along with OM chanting. OM chanting was conducted using a prerecorded tape with headphones and the patients were advised to rhyme OM chanting along with performing Ardh-Matsyendrasana on both sides, for 15 minutes including 3 minutes of a rest period in between. While performing the Ardh-Matsyendrasana, patients were advised to inhale deeply and after that while exhaling, produce OM chanting rhythmically to the prerecorded tape that was played. In the Asana posture, there is a twist and rotation of the neck and upper torso along with the abdomen. The left arm is pressed against the right knee and the right arm is wrapped behind the back, which leads to increases in the body twist. The spine is erect and the chest opens. The left leg and knee stay on the floor. The right knee should be near the left armpit. 27,28 The process of the yoga session was detailed to the patient on the first day of the session through personal instructions by the therapist. The process of the asana posture along with OM chanting was repeated bilaterally as a 10-second hold with a 10-second relaxation. Such movements were asked to be performed 9 times/side/set. Three minutes of rest was also advised in between two sets. 29 The two sets were then followed by five minutes of a hot pack and ergonomic advice. The patients in the control group were taught active stretching of the sternocleidomastoid muscle (SCM). Stretching was repeated bilaterally for 15 minutes per day followed by 5 minutes of a hot pack and ergonomic advice.
There were two time points for data collection. One was at baseline and the other at postintervention, which was collected at the end of the fourth week. Outcome measures were assessed two times: once at precollection of data (baseline assessment) and the second after completion of fourth week. The primary outcome measure was the NDI. 1 Each subject was asked to mark the best suitable option for each of 10 listed questions or items on a 6-point scale ranging from 0 to 5. Lower and higher values depict lower and higher disability, respectively. The secondary outcome measure was neck muscle tenderness or PPT, which was assessed by using a digital algometer (Orchid Digital Algometer with software ALGO-DS) applied to the superior sternocleidomastoid, bilaterally. The unit verified a valid calibration as it provides a built-in calibration routine and a digital readout for pressure.
The assessment of superior SCM tenderness of both sides was performed with the patients in sitting posture. Trigger points were highlighted by the marker for further assessment. The pressure was perpendicularly applied by a digital algometer (1.0 cm2 tip) at each palpated marked point. The patient was asked to inform the point of time when pressure applied to a tender point of muscle converts to a painful sensation, and that reading (pressure level) was obtained. 30 Using calibrated pressure algometry for measuring the PPT provides a valid, accurate, and reproducible method for assessing tender spots. 30 –32
Data were depicted as mean ± standard deviation. Data analysis was performed using the IBM Statistical Package for Social Sciences, SPSS version 26.0. The test used was a paired t-test. P-value <0.05 was considered significant.
Results
Forty-five patients meeting the inclusion criteria were included in the study. Baseline characteristics are shown in Tables 3 and 4 (age group and gender of patients, respectively). There were five dropouts (three in the control group and two in the yoga group); the reasons are depicted in the trial profile (Fig. 1). Owing to this dropout, 20 patients in the yoga group and 20 in the control group completed the study (Fig. 1). Of these patients, 24 were females and 16 males.
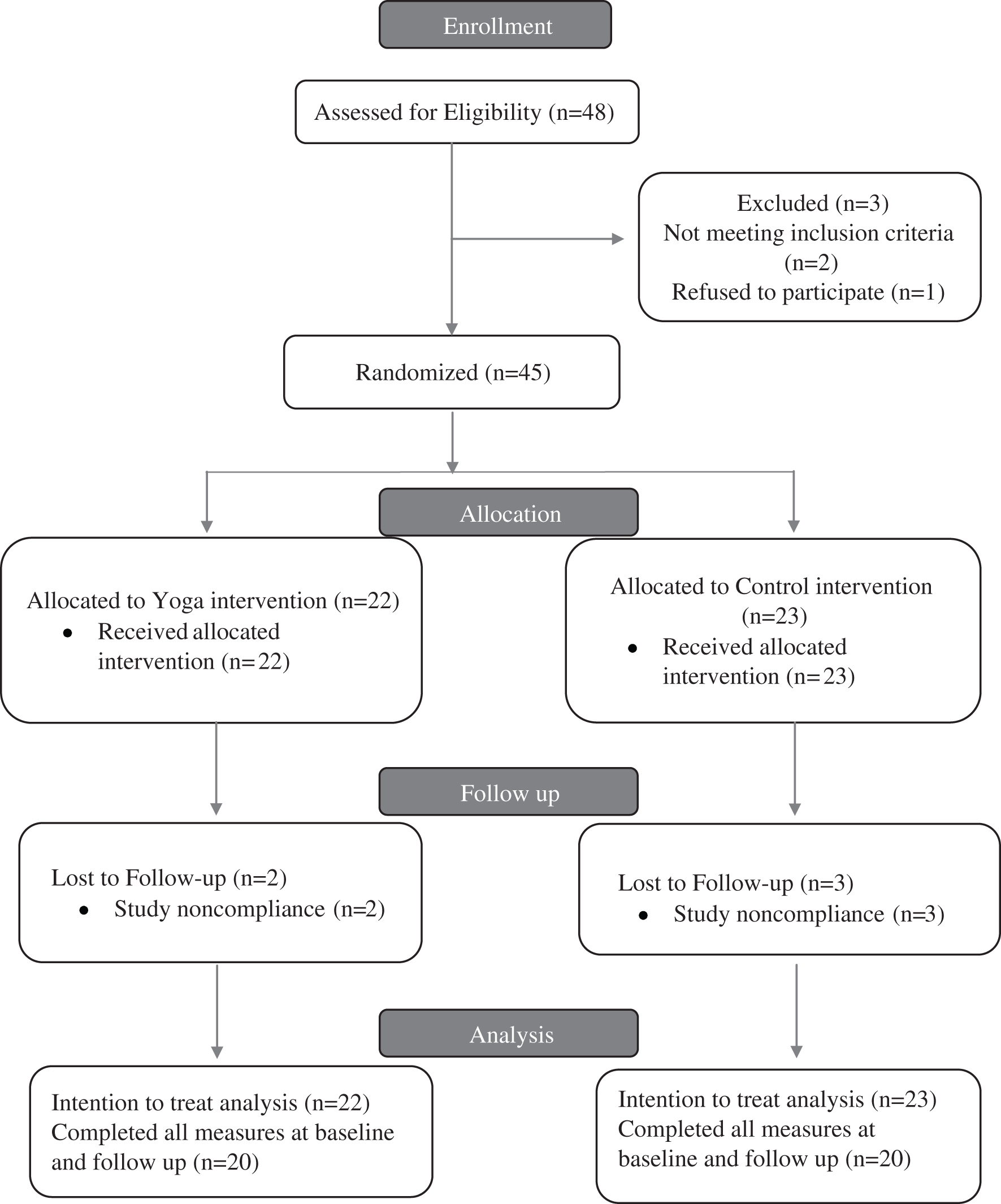
CONSORT trial flowchart.
Baseline data
The ages of the patients ranged from 18 to 30 years. Females were in the majority in the control group and the yoga group (60%). Table 1 presents baseline characteristics (age, gender, and causes of neck pain). The mean and standard deviation of age in the yoga group (experimental group) was 23.45 ± 3.31 years, while it was 23.0 ± 3.16 years in the control group. There was heterogeneity in the samples in terms of pain causative factors. Postural neck pain was a dominant causative factor in both the yoga group and the control group as compared with nonspecific causes of neck pain. Postural neck pain was recorded in 55% of patients in the yoga group, whereas it was 65% in the control group. As anticipated, the yoga group had higher treatment outcome expectation (P < 0.001), Table 2 represents the results of pre- and postintervention.
Demographic Data
M, mean; SD, standard deviation.
Intervention
P < 0.05 for paired t-test (within groups).
NDI, Neck Disability Index; PPT, pressure pain threshold; SCM, sternocleidomastoid muscle.
Outcome measures
Primary outcome
At the end of the fourth week, the paired t-test showed significant improvement in both the yoga group and the control group in neck pain and disability parameters (P < 0.05) as shown in Tables 3 and 4.
Neck Disability Index Yoga (Pre–Post)
The result is significant at P < 0.05.
Neck Disability Index Control (Pre–Post)
The result is significant at P < 0.05.
Secondary outcome
Tables 5 –8 represent the pre- and postintervention results for the right and left SCM on the PPT parameter in both the groups. The paired t-test showed a significant improvement in the yoga group (P < 0.05) in terms of PPT for the right and left SCM, whereas no significant improvement was seen in the control group in both the right and left SCM for the PPT parameter (P-value >0.05).
PPT Yoga Right Sternocleidomastoid Muscle (Pre–Post)
The result is significant at P < 0.05.
PPT Yoga Left Sternocleidomastoid Muscle (Pre–Post)
The result is significant at P < 0.05.
PPT Control Right Sternocleidomastoid Muscle (Pre–Post)
The result is not significant at P < 0.05.
PPT Control Left Sternocleidomastoid Muscle (Pre–Post)
The result is not significant at P < 0.05.
Discussion
Neck pain involves a high socioeconomical and medical impact. This randomized controlled trial was conducted to assess the efficacy of Ardh-Matsyendrasana with OM chanting, compared with conventional active stretching exercise to understand which is more effective in patients with subacute mechanical neck pain.
The prevalence of neck pain is higher in females as compared with males as shown in a study by Hoy et al. 33 Our study was in accordance with previous studies, showing a greater ratio of female (60%) to males (40%) in both the groups. Outcome analysis of this study indicated a significant difference in both the groups on neck pain and disability parameters. Similarly, a significant difference in PPT was found in the yoga group, whereas no significant difference in the control group was observed.
In this randomized controlled trial, the yoga group showed significant improvements in pain-related disability (P < 0.05), which supports the findings of previous studies. 34 The psychological and physical improvement from yoga was described in the case of hatha yoga, consisting of physical movements involving isometric strengthening of muscles, flexibility, and stretching components along with mental mindfulness of bodily movements involving breathing patterns. 35 OM chanting relaxes the body and also produces a calming and soothing effect on the mind. 36 There are currently no studies that have used OM chanting for subacute mechanical neck pain.
Stretching exercises showed significant improvement in strength and neck-related disability (NDI) in a previous study by Lee and Yoo. 37 The results of this study are also in accordance with this previous study. Based on these findings, both yoga and stretching exercises may be effectively used for reducing neck-related pain and disability.
In this study, the results showed a significant improvement in the yoga group (P < 0.05) for the PPT parameter as compared with the control group. However, the intervention was not significant in reducing tenderness. Results of this study are consistent with the previous studies for improvement of PPT in the yoga group. 38 This indicates that the tenderness or PPT of the muscle improves more with the yoga posture than with active stretching exercises of the same muscle.
Strengths of this study include the effectiveness of the single asana Ardh-Matsyendrasana and OM chanting per the yoga protocol over a conventional stretching intervention for mechanical neck pain. This is the only published study known to demonstrate the effectiveness of this yoga protocol in managing mechanical neck pain. Both groups received interventions with the help of active attention by the therapist, whereas most of the previous studies on the effect of yoga on neck pain included no active participation of therapists in the control group or the home-based exercise group.
Limitations
This study is limited by the small sample, which could overestimate the effect size. 39 In addition, the intervention period was only four weeks; therefore, the effects of a longer duration intervention remain unknown. Future studies are needed including with a larger sample size with long-term duration. A follow-up of this study is needed to assess the long-term impact of the treatment effects.
Conclusion
This randomized controlled study suggests that both yoga with OM chanting and active stretching exercise may be used according to patient preference for improving neck-related pain and disability. Ardh-Matsyendrasana along with OM chanting was an effective intervention for improving the tenderness of neck muscles as compared with the active stretching exercise of neck muscles. Overall, the yoga intervention proved to be a more effective intervention in patients with subacute mechanical neck pain.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.▪