
Abstract
Abstract
Background:
Oral anticoagulation is used extensively for prevention of thromboembolic events. Whether acupuncture is safe for patients taking anticoagulants is not clear.
Objective:
To describe a patient with a history of ischemic stroke and paroxysmal nonvalvular atrial fibrillation who was in stroke rehabilitation including acupuncture.
Design, Setting, and Patient
The patient developed sudden calf hematoma when optimal therapeutic intensity of international normalized ratio (INR) was achieved.
Results:
This patient was treated conservatively, without symptoms of compartment syndrome, and calf hematomas were resolved in 3 months.
Conclusions:
With increased acceptance of acupuncture worldwide and enforcement of clinical guidelines for prevention of thromboembolism, acupuncture-induced hematoma will be an emerging clinical entity. To minimize hemorrhagic complications, caution should be exercised when patients receiving oral anticoagulation request acupuncture treatment.
Introduction
Acupuncture has been incorporated into health care systems not only in East Asia for thousands of years, but also in Western countries in the past decades. It is estimated that in Taiwan, about 23% of the total population has used acupuncture. 5 Thus, there will be a substantial number of patients taking oral anticoagulation while undergoing acupuncture. Meanwhile, many patients may regard acupuncture as a complementary and alternative therapy for stroke rehabilitation. However, whether this ostensibly minimally invasive procedure could increase the risk for hemorrhagic complications in patients taking anticoagulation is uncertain.
To our knowledge, there is only 1 report that describes a case of acupuncture needle–induced hemorrhagic complication (calf compartment syndrome) during oral anticoagulation in the mid-1980s. 6 With gradually increased acceptance of acupuncture worldwide and enforcement of recent guidelines for prevention of thromboembolism, acupuncture needle–induced hemorrhagic complications is likely an emerging clinical issue. Herein, we report a patient with paroxysmal atrial fibrillation taking warfarin who developed sudden calf hematoma complicated by acupuncture. We also discuss differential diagnosis and management of unilateral calf swelling, potential benefits/risks of acupuncture during anticoagulation, and strategies to prevent hemorrhagic complications.
Case Report
A 60-year-old woman presented to the emergency department reporting a sudden attack of palpitations and shortness of breath for 1 hour. An electrocardiogram showed atrial fibrillation; heart rhythm spontaneously recovered to sinus rhythm 15 minutes later. Three years prior, the patient had an ischemic stroke. No obvious linguistic or movement dysfunctions developed. Since then, she reported a sense of numbness in her left lower extremity. Transthoracic echocardiography results and thyroid function were normal. Primary diagnosis was paroxysmal atrial fibrillation.
Considering the patient's age and risk factors, warfarin was prescribed. An optimal therapeutic intensity of international normalized ratio (INR) was maintained to 2.0–3.0. When the dose reached 3.75 mg/d 12 days after admission, the patient reported sudden sharp and continuous pain in her left gastrocnemius region while standing. Her calf was obviously swollen with tenderness, and positive for Homans sign (pain in the calf was aggravated by passive dorsiflexion of the ankle joint). No ecchymosis, erythema, or increased skin temperature was noted; pulse intensity of the dorsal pedal artery was normal. Vascular Doppler ultrasonography showed patency in deep veins and arteries of both lower extremities. The onsite test of INR was 2.2. B-mode ultrasound of the swollen region showed 2 intramuscular low-echo masses: lateral 5.8 × 2.4 × 2.3 cm, and medial 6.3 ×2.8 × 3.5 cm.
The patient had acupuncture treatment in her left leg in the outpatient department for 3 months prior, and she continued the treatment after admission. Therefore, traumatic intramuscular hematoma of the left calf was diagnosed. The patient was treated conservatively with mannitol. Before the patient was discharged home, the hematomas had regressed to 5.0 × 1.4 × 1.6 cm and 6.2 ×1.4 × 1.8 cm, respectively. We recommended the continued use of warfarin for stroke prevention, but the patient refused. Therefore, we prescribed aspirin instead. No obvious movement dysfunction of her lower extremity was detected. Three months later in follow-up, the hematomas were completely resolved.
Discussion
This case raised 2 interesting questions that may be encountered in clinical practice. The first one is the differential diagnosis of unilateral swelling of the lower extremity. In clinical practice, hematoma-induced unilateral swelling of the distal lower extremity is not rare. The most common cause of calf hematoma is partial rupture of the musculotendinous junction of the medial head of the gastrocnemius muscle during active plantar flexion of the foot and simultaneous extension of the knee (also called tennis leg). 7 Differential diagnosis of calf hematoma includes deep vein thrombosis (DVT), lymphedema, sarcoma, infection, and ruptured popliteal cyst. It is of great importance to make a quick discrimination between calf hematoma and DVT because delayed recognition and/or inappropriate heparinization may lead to compartment syndrome, a serious condition that frequently requires surgical decompression for limb salvage.
The second question concerns the safety issue of acupuncture in patients taking oral anticoagulation. The prevalence of atrial fibrillation is 0.4% to 1.0% in the general population and increases with age. 8 The rate of ischemic stroke among patients with nonvalvular atrial fibrillation is about 5% each year. In the United States, about 795,000 people experience a new or recurrent stroke each year. 9 About 15% of strokes are attributable to atrial fibrillation. 10 Warfarin has been used extensively as a standard prophylaxis of stroke in patients with nonvalvular atrial fibrillation. 11 In patients with atrial fibrillation without antithrombotic treatment, stroke risk is increased 5-fold.
Cerebrovascular accident rehabilitation now accounts for 12% of the total cases of outpatient acupuncture clinic treatment in China. 16 There is a growing number of clinical trials in Asia and the West evaluating the efficacy of acupuncture for stroke survivors. Due to the insufficient quality of the available trials, evidence supporting the beneficial effects of acupuncture on subacute or chronic stroke is not available.12–15 However, because of its less severe side effects and lower cost, acupuncture warrants further large and methodologically sound trials. Therefore, there is a considerable number of patients having acupuncture while taking oral anticoagulants.
In addition, patients receiving mechanical prosthetic heart valve replacements are at potential risk for hematoma during acupuncture. Each year, 300,000 prosthetic heart replacement surgeries are done worldwide 17 and 106,000 in the United States. 18 The total number of replacements undergone is steadily increasing due to a high incidence of rheumatic heart disease in developing countries and to a growing burden of degenerative valve disease in aging populations in developed countries. Among these, at least 50% were mechanical valve replacements, an undisputed indication for oral anticoagulation. Compared with individuals undergoing therapeutic stroke prevention, these patients need a more prolonged INR (usually 2.5–3.5) to achieve therapeutic efficacy, which portends increased risk for hemorrhagic complications. Smith and colleagues reported compartment syndrome produced by hemorrhage into the anterior compartment of the leg, caused by acupuncture treatment in a 68-year-old man taking anticoagulant therapy after mechanical prosthetic valve replacement. 6 Because lifelong oral anticoagulation is indispensable after cardiac valve replacement, the potential benefits of acupuncture should be weighed against its risk for hemorrhage.
Finally, patients taking warfarin for primary and secondary prevention of venous thromboembolism are also at risk for hemorrhagic complication during acupuncture. However, due to the limited duration of drug treatment, it is unlikely that patients would be treated with acupuncture during anticoagulation.
Warfarin-induced hematomas are not rare hemorrhagic complications. We searched PubMed for articles on “warfarin (anticoagulation) and hematoma” from 1966 to present and retrieved 186 case reports (261 cases). We categorized these cases into 3 groups according to their anatomical locations (summarized in Figure 1). The most frequently involved region is the retroperitoneum, which accounted for 16.5% of the total cases (43/261, Figure 1C). Most of the organs and tissues listed in Figure 1A are less likely involved in acupuncture-induced injury, due to their relatively deeper location in the body. However, data in Figure 1 panel B are important because a majority of acupoints are located in the extremities and abdominal wall, and these regions are prone to develop hematoma even without any forms of injury during oral anticoagulation. Moreover, these regions are predilection sites for compartment syndrome (1 case of rectus muscle hematoma induced fatal abdominal compartment syndrome, 19 1 case in the forearm, 20 2 cases in the upper arms,21,22 and 1 case in the thigh 23 ). Therefore, we strongly suggest that when performing acupuncture in these regions in patients receiving anticoagulation, caution should be exercised and additional procedures to minimize hemorrhage are warranted.
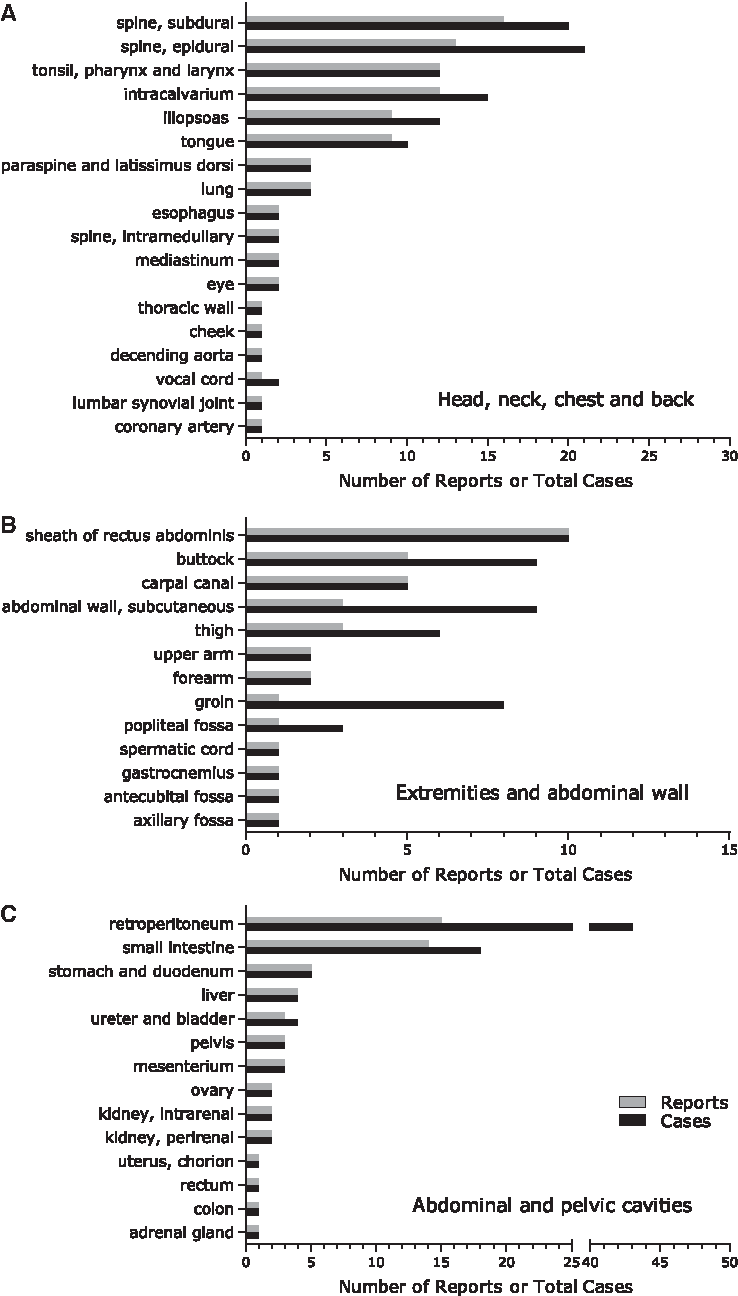
Summary of 186 case reports, 261 cases retrieved from PubMed for warfarin-induced hematomas. All the cases have been categorized into 3 major portions of the body, as shown in panels A to C.
Our patient at admission reported that she was receiving acupuncture therapy, but we failed to realize that such kind of microinjury has the potential to increase the risk for hemorrhagic complication during anticoagulation therapy. Approaches that may alleviate unwanted complications during oral anticoagulation (combined with a thorough knowledge of anatomy 24 ) include the following: careful manipulation, direct pressure on the site of acupoints after needle removal, having the patient sit quietly for 15–30 minutes to allow clotting for potentially injured vessels, and use of needles with larger diameters (acupuncture needles usually with diameter of 0.2–0.4 mm). It has been confirmed that core needle biopsy of the breast using 14-gauge (2.1 mm in outer diameter) or 11-gauge probe (about 3 mm in outer diameter) in patients receiving warfarin therapy is relatively safe and no significant hemorrhagic complication was observed compared with a control group.25,26 For a similar invasive procedure in patients receiving anticoagulant therapy, needle electromyography, there was no significant increase in the risk of intramuscular hemorrhage when direct pressure was applied after removal of the needle. 27
Conclusions
Warfarin is currently prescribed in 30%-50% of appropriate patients in the United States and Europe, 28 and in 10% of nonvalvular atrial fibrillation patients in China. Considering the huge number of total patients and the worldwide widespread use of acupuncture as an alternative therapy, acupuncture-induced hematoma during oral anticoagulation is an emerging clinical issue. Prior or current use of acupuncture and locations of acupoints should be requested from patients receiving oral anticoagulation, particularly when the patients are in stroke rehabilitation or after heart valve replacements. In addition, the patient should be informed of potential risks for hematoma if taking anticoagulation medications along with acupuncture treatment. If acupuncture is necessary for patients undergoing anticoagulant or antiplatelet therapy, caution should be exercised and efforts aiming to accelerate the closure and clotting of acupoints after needle removal should be applied to minimize potential hemorrhagic complications.
Footnotes
Disclosure Statement
No competing financial interests exist.