
Abstract
Abstract
Background:
Although acupuncture is a highly effective treatment for pain management, it suffers from lack of reproducibility of results. One of the many variables involved in achieving reproducible clinical results is the specificity of an anatomical structure being stimulated. Lack of target specificity obscures scientific understanding of how acupuncture works, leading to skepticism about the efficacy of acupuncture within the medical community and prejudice regarding the wisdom imparted through classical acupuncture texts.
Objectives:
The goals of this study were to test the hypothesis that classical acupoint locations described in the classics have a strong foundation in neuroanatomy and to promote a consensus among practitioners about neuroanatomy-based acupuncture.
Methods:
Acupoint locations for TE 1–TE 10 described in the Systematic Classic were transliterated, and each acupoint neuroanatomical target was determined by literature review, dissection, and/or electrical stimulation. An objective comparison was made between classical acupoint location and acupoint descriptions in a contemporary Chinese acupuncture textbook.
Results:
Classical acupoints TE 1–TE 10 had specific neuroanatomical targets. Neuroanatomical differences of the TE acupoints were found between classical and contemporary descriptions. Of the ten contemporary acupoints, 60% of targets were ambiguous (TE 1 and TE 5–TE 9) while 40% (TE 2–TE 4, and TE10) missed the corroborated neuroanatomical targets completely.
Conclusions:
This study demonstrates that each acupoint between TE1 and TE10 targets a distinct nerve and/or muscle enabling the achievement of feedback of highly distinct tissue stimulation, without any target redundancy. The transmission of erroneous and ambiguous anatomical targets found in contemporary texts highlights the urgency in advancing a science-based approach to study the neuroanatomical intents of other acupoints.
Introduction
I
As acupoint researchers and educators, the authors have observed disproportional emphasis on the functions and indications of acupoints at the expense of a neuroanatomy-based understanding, which is particularly relevant in assessment and treatment of pain and neurologic disorders. In order to demonstrate how clinically significant the understanding of acupoint neuroanatomical specificity is for effective pain management, the treatment of De Quervain's tenosynovitis (DQT) is also discussed, using just the TE acupoints on the forearm described in this study.
Methods
The Systematic Classic (Jia Yi Jing/JYJ) is the first complete manual of acupuncture and moxibustion, dating back to the third century. 4 The JYJ reported 349 acupoint locations, close to 50% more acupoints than in the other two classics of the Huang Di Nei Jing: Ling Shu and Su Wen. The value of this investigation relies on its Chinese-to-English transliteration of the Systematic Classic, as opposed to reliance on other available English translations. As in the recent study by the current author, transliteration was chosen in favor of translation in order to avoid possible misinterpretations of anatomical landmarks that are important for precise location. 3
Verification via Peer-Reviewed Articles
A thorough comparison between the transliterated version of the JYJ and the standardized Traditional Chinese Medicine (TCM) textbook, Chinese Acupuncture and Moxibustion (C&M), was made to determine descriptive discrepancies of each cutaneous acupoint location and its subcutaneous neuroanatomical target. 5 Whenever a discrepancy or neuroanatomical redundancy was identified in C&M, an alternate neuroanatomical target was proposed for that particular classical acupoint and verified with peer-reviewed anatomical research literature.
Verification via Cadaver Dissection
For certain acupoints, cadaver-based studies via peer-reviewed literature were limited or unavailable. Instead, inquiries on each specific neuroanatomical acupoint target were performed with a single cadaver dissection. The specimen was an 88-year-old female body acquired for anatomical education via the Human Body Donation Program at Queen's University, in Canada. The specimen was fixed with vascular perfusion, using a mixture of liquid phenol, 95% ethanol, glycerin, and water. The dissection occurred at the Anatomy Learning Centre in Queen's University as a part of the Complementary & Alternative Medicine—Human Dissection Experience program.*
Verification via Monopolar Electrostimulation of Acupoints
A Pointer Plus device (10 Hz monopolar electrostimulation device manufactured by Mayfair Medical Supplies Ltd., Hong Kong) was applied on live volunteers (authors) for the verification of electroacupuncture stimulation of neuroanatomical targets in all TE1–TE10 acupoints. When a distinct stimulation of an acupoint, either dermatomal paresthesia or myotomal recruitment, was observed or felt subjectively, the response was compared to the known actions of corresponding sensory nerves, muscles, or motor nerves. Each stimulation was subsequently attributed to a unique neuroanatomical target for that acupoint. The authors' knowledge of channel theory, functions and indications of acupoints, cadaver-based studies, and dissections contributed to establishing the proposed assignments.
Results
The results of this study are shown in the tables, figures, and Supplementary Videos S1–S3 (Supplementary Data are available online at www.liebertonline.com/acu) as described in the sections below. Because of the complexity of these results, they are also intertwined with parts of the Discussion section, where they are presented in more detail and elucidated.
Transliterations of Triple Energizer Acupoint Locations and Historical Location Drifts
Transliterations of TE 1–TE 10 acupoint locations from the JYJ are presented in Table 1. Comparisons of contemporary (C&M, modern TCM) and Classical TE 1–TE 10 acupoint locations with their associated anatomical targets are presented in Table 2. Classical and contemporary anatomical locations of TE 10 are presented in Table 3.
C&M, Chinese Acupuncture and Moxibustion, rev. ed. (ref. 5); TCM, Traditional Chinese Medicine; m., muscle.
P.R.O.C., People's Republic of China.
Neuroanatomical Visual Descriptions of Triple Energizer Acupoints
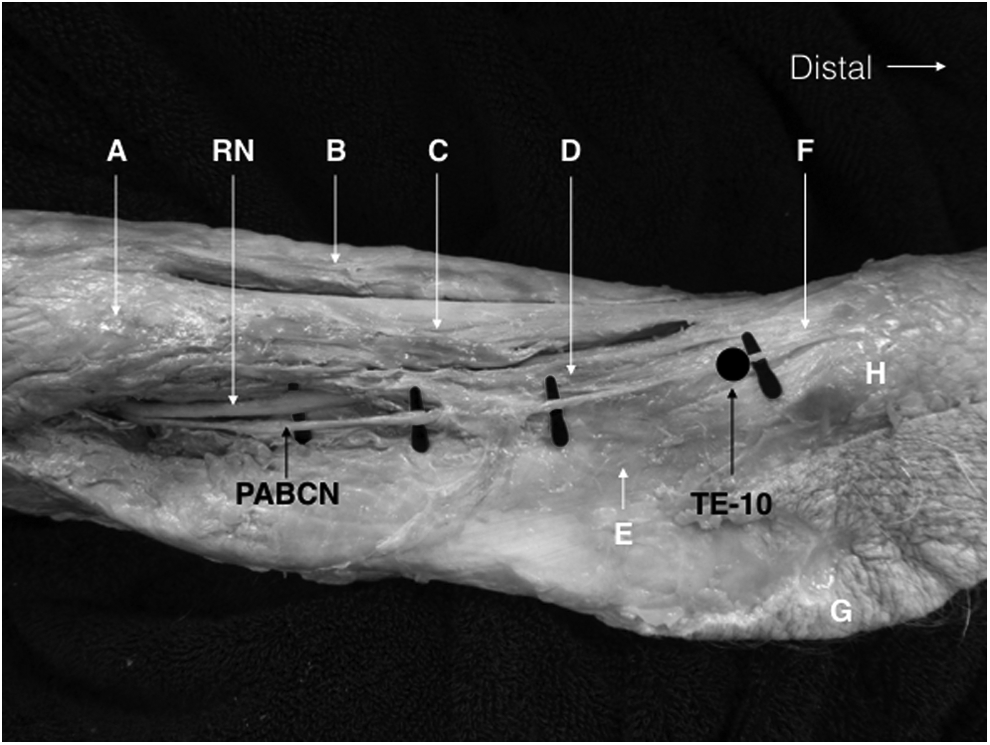
Neuroanatomical targets of acupoints TE 1–TE 3 by the dorsal branch of the ulnar nerve on the dorsal hand are shown in Figures 1 and 2. Detailed innervation of acupoint TE 4 by the posterior interosseous nerve and adjacent structures are shown in Figure 3. Unique musculoskeletal targets of acupoints TE 5–TE 9 in the dorsal forearm are shown in Figure 4. The neuroanatomical target of acupoint TE 10 by the posterior antebrachial cutaneous nerve and adjacent structures are shown in Figure 5.
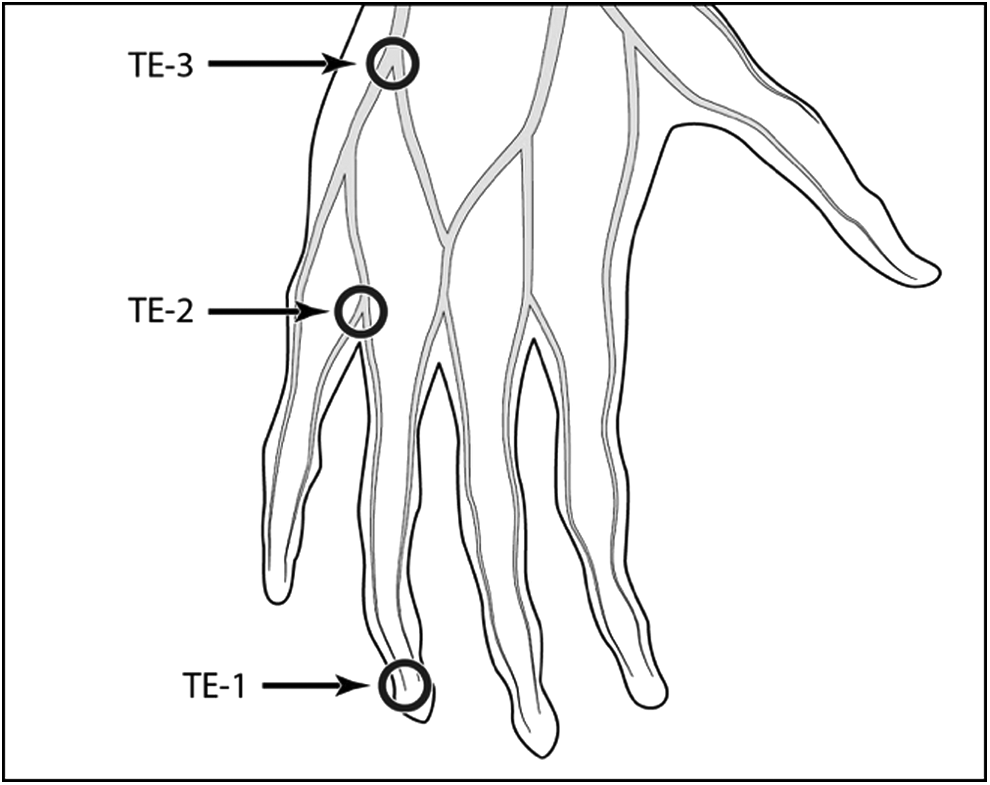
Neuroanatomical targets of acupoints TE 1, TE 2, and TE 3 by the dorsal branch of the ulnar nerve on the dorsal hand. (Original illustration is adapted from Gray's Anatomy, 1918 Public Domain Image 813). 14
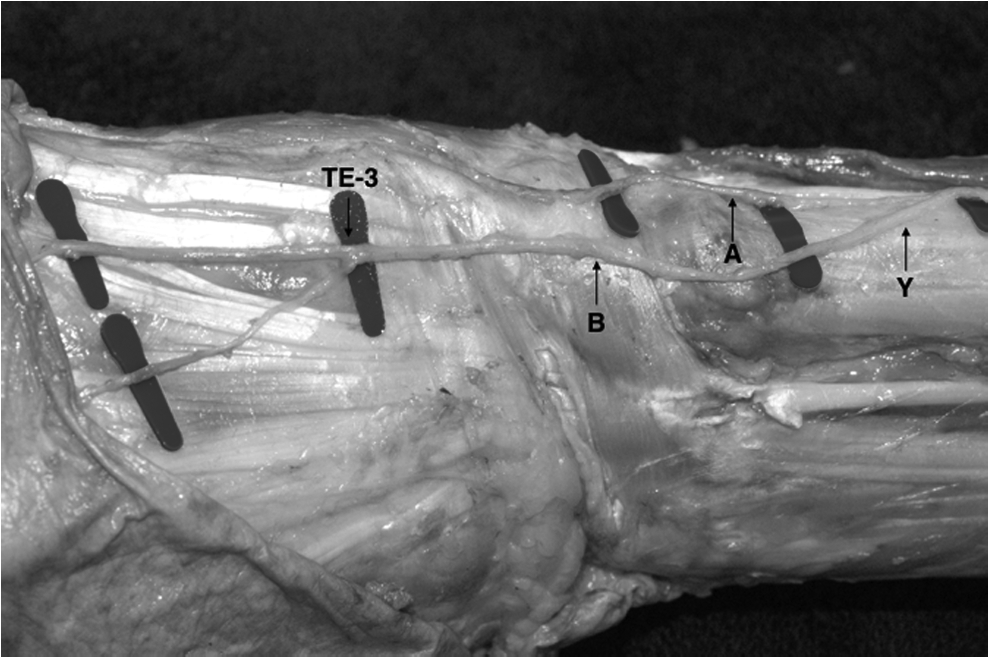
From right to left: Bifurcation point
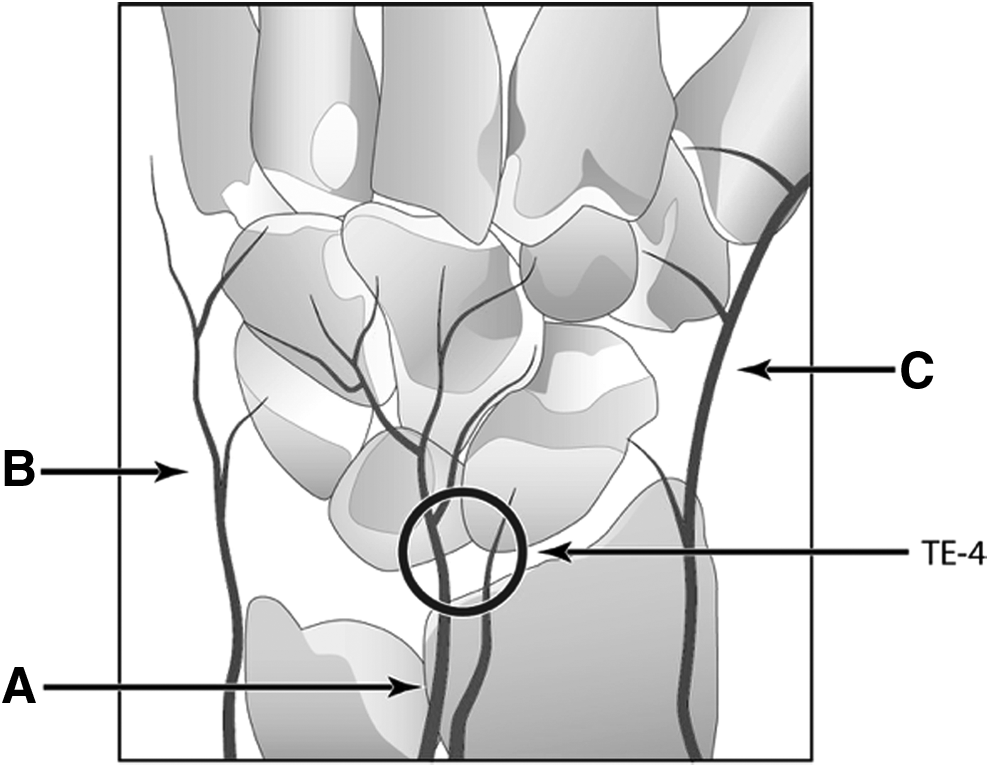
Innervation of dorsal wrist by
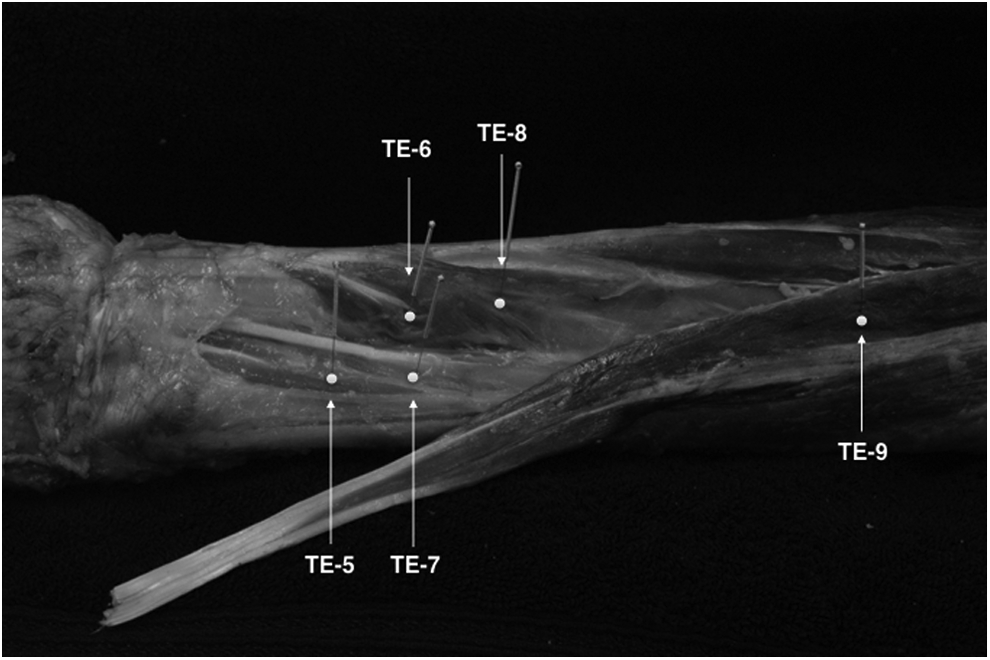
Unique musculoskeletal targets of acupoints in close proximity on the dorsal forearm: extensor indicis
Right upper arm depicting
Electrostimulation of Triple Energizer Acupoints with Unique Motor Responses of Dorsal Forearm Muscles
Electrostimulation of acupoint TE 5 with motor responses of the extensor indicis muscle is shown in Supplementary Video S1. Electrostimulation of acupoints TE 6, TE 7, and TE 8 with each corresponding motor response of the abductor pollicis longus, extensor pollicis longus, and extensor pollicis brevis is shown in Supplementary Video S2. Electrostimulation of acupoint TE 9 with the motor response of the extensor digitorum communis is shown in Supplementary Video S3.
Discussion
Triple Energizer 1
C&M describes the innervation for TE 1 as the palmar digital proprial nerve derived from the ulnar nerve. This description is in agreement with dissection studies that show frequent innervation of the dorsal skin of the second, third, and fourth digits by the palmar digital nerves.6,7 However, in another dissection study, performed by Mok et al., of 30 cadavers, 29 specimens showed innervation contributions at the dorsal ulnar side of the fourth digit by the dorsal branch of the ulnar nerve (DBUN). 8 Of these 29 specimens, only 1 had dual innervation contributions from the DBUN and the superficial branch of the radial nerve. For completeness, the current authors proposed to reinterpret the neuroanatomy of TE 1 as the anastomosis of the palmar digital and dorsal digital nerves of the ulnar nerve (Table 2). This supports the meridian theory description in which Yin and Yang polarity changes at the extremity of each meridian. This can be explained by considering Yang as dorsal digital nerves, Yin as palmar digital nerves, and their connection as the transforming point between Yin and Yang. 3
Triple Energizer 2 and 3
C&M describes the innervation for TE 2 and TE 3 as both being supplied by the DBUN. This redundant description for the neuroanatomical basis of both points provides an opportunity to investigate their precise anatomical differences. Mok et al. 13 described the innervation territory of the DBUN in detail, where, in 80% of subjects (24 of 30), the DBUN branched out and extended to innervate from the ulnar side of the fifth digit to the ulnar side of the third digit (Fig. 1). 14 The common branching pattern was described first as a bifurcation of the DBUN into the first and second branches proximal to the styloid process of the ulna. The first branch innervates the ulnar side of the fifth digit. The second branch extends and bifurcates, where a third branch separates from it. The second branch subsequently bifurcates at the web space to innervate the radial side of the fifth digit and ulnar side of the fourth digit. The third branch also bifurcates at the web space to supply the radial side of the fourth digit and the ulnar side of the third digit. TE 3 occupies the bifurcation point into the second and third branches (Fig. 2). TE 2 occupies the bifurcation point of the second branch into the web space between the fourth and fifth fingers.
Triple Energizer 4
C&M describes the innervation for TE 4 as the terminal branch of the posterior antebrachial cutaneous nerve (PABCN) and the DBUN. An innervation and surgical study of the wrist by Van de Pol et al. showed that the main innervation of the dorsal wrist joint is attributed to the posterior interosseous nerve (PIN). 15 Van de Pol and colleagues also found that the PABCN had no articular branch entering the dorsal wrist capsule and the contribution from the DBUN to the wrist joint was very small. Therefore, the current authors propose assigning the articular branches of the PIN to TE 4 (Fig. 3).
Triple Energizer 5, 6, 7, and 8
TE 5–TE 8 are located in close proximity, but their anatomical specificities can be demonstrated. Although C&M describes the neuroanatomy of these points as the PABCN and PIN for this group of points, as well as the medial antebrachial cutaneous nerve for TE 7 and TE 8, this anatomical description falls short of considering four distinct posterior forearm muscles in this region: the extensor indicis (TE 5); the extensor pollicis brevis (EPB; TE 6); the extensor pollicis longus (TE 7); and the abductor pollicis longus muscles (APL; TE 8) See Fig. 4. These distinct muscles are accessible with acupuncture needles and each of their expected motor actions can be confirmed with electrical stimulation (Supplementary Videos S1 and S2). Based on the current authors' cadaver dissections, there is not sufficient evidence to suggest that these points are neuromuscular junctions; however further research with a larger sample size is recommended to confirm if TE 5–TE 8 correspond to motor points.
TE 5 is considered the Luo-Connecting point of the TE meridian, which was first recorded in Chapter 10 of the Spiritual Pivot. The Spiritual Pivot describes the Luo-Connecting point separating into its interior–exterior related meridians for eleven of twelve meridians, with the exception of the TE. Unlike the rest of the meridians, the TE meridian makes a direct connection to the Pericardium (PC) organ rather than indirectly through its interior–exterior related meridian.
It is tempting to speculate whether needling TE 5 deeply could approach the median nerve or anterior interosseous nerve (median nerve branch) on the flexor side of the forearm, thus satisfying a TE-to-PC meridian connection. To attain this anatomically, the interosseous membrane between the radius and ulna would have to be punctured. The current authors were unable to break the interosseous membrane with an average acupuncture needle. However, with electrical stimulation from the Pointer Plus device, it is often possible to activate the pronator quadratus muscle, which is innervated by the anterior interosseous nerve (median) from this location. This could satisfy the requirement of a Luo connection from TE 5 to the PC meridian, even though such a connection is a modern adaptation not described in Chapter 10 of the Spiritual Pivot.
Triple Energizer 9
TE 9 is known as Si Du, which translates into Four Rivers. The current authors propose that Four Rivers is an accurate anatomical description of the four tendons of the extensor digitorum communis. In a study on the distribution of nerve entry points on forearm muscles, Safwat et al. showed that, in 23 specimens, the extensor digitorum communis muscle had a mean value of 3.4 ± 1.3 of motor points located along the proximal third (65.2%) and middle thirds (34.8%) of the muscle. 16 This area encapsulates TE 9, which, from a neurofunctional perspective, would be a rich motor entry zone for the extensor digitorum communis muscle (Fig. 4). The motor response of this muscle can be stimulated easily via electrical stimulation (Supplementary Video S3).
Triple Energizer 10
In a study, MacAvoy et al. observed that the PABCN became subcutaneous at an average distance of 6.6 cm proximal to the lateral epicondyle and passed an average 2.1 cm anterior to the lateral epicondyle in 29 of 30 specimens. 17 Distal to the lateral epicondyle, the PABCN branched out over the central cutaneous region on the posterior forearm, terminating at the distal third of the forearm. This cutaneous innervation precisely mirrors the TE channel distribution.
The current authors propose that the historically correct location for TE 10 is 1 cun proximal to the lateral epicondyle rather than 1 cun proximal to the olecranon, as it is popularly taught. In the Systematic Classic location for TE 10, the big bone on the outside (lateral) of the elbow would logically be the lateral epicondyle, not the olecranon. It would be illogical to interpret “the big bone” as the olecranon (elbow) because it cannot simultaneously be outside (lateral) of the elbow and be the elbow itself. Furthermore, in the Systematic Classic description for SI 8, a structure called the “big bone” appears again. This time the acupoint (SI 8) is located outside (lateral) to the big bone inside the elbow ( ). Therefore, for both the big bone and the elbow terminologies to remain consistent within the Systematic Classic, the big bone (
). Therefore, for both the big bone and the elbow terminologies to remain consistent within the Systematic Classic, the big bone ( ) would logically be the epicondyle while the elbow would be the olecranon.
) would logically be the epicondyle while the elbow would be the olecranon.
The location of TE 10 proximal to the lateral epicondyle described in both the Spiritual Pivot and Systematic Classic remains conserved into the Qing Dynasty, drifting behind the olecranon only within the twentieth century (Table 3). The Bronze Man Classic from the Song Dynasty did not describe a large bone outside the elbow. This absent description may be a possible source where “the big bone” lateral to the elbow (lateral epicondyle) became lost to future generations. The depression between the two sinews referred to in the Systematic Classic location of TE 10 are interpreted as the lateral head of the triceps brachii and the extensor carpi radialis longus (Fig. 5).
Clinical Application: De Quervain's Tenosynovitis
DQT is a painful tendinopathic disorder of the first dorsal compartment caused by the impaired gliding of the APL and EPB tendon sheaths. 18 The gliding impairment of these tendons is thought to be a result of the thickening of the extensor retinaculum with subsequent narrowing at the fibro-osseous canal.19,20
Treatment of DQT consists of conservative care (e.g., steroid injections, splinting, heat, and/or manual therapy) and, in severe cases, surgical intervention. Corticosteroidal injections have been the “gold standard” among conservative care treatments, although their efficacy remains unclear. 18 Moreover, clinical studies have shown potentially harmful side-effects of extra-articular corticosteroid injections. A systematic review of the risks and benefits of steroid injections for tendinopathies showed that local steroidal injections have significant negative effects, including decreased cell viability, cell proliferation, and collagen synthesis, resulting in tendon ruptures, as well as increased collagen disorganization and necrosis. 21 When steroid injections fail to succeed, patients are referred to surgical treatment, which is more invasive and is accompanied by a higher cost and the possibility of complications.
Most conservative treatments for DQT focus on pain management and reduction of inflammation at the first compartment of the wrist and ignore APL and EPB myopathies. Chronic repetitive stress of muscles leads to severe spasms, muscle shortening, knotting, and possible development of trigger points. 22 Consequently, all of these will cause impaired gliding of the APL and EPB tendons and abnormal friction of their respective compartment sheaths when subject to the tensile motion of antagonist muscles. Regardless of whether DQT is due to primary or secondary disorder of the APL and EPB tendons, tendinopathy will logically involve its corresponding affected muscle. 23
Acupuncture can be an effective treatment option for DQT, especially when there is a comprehensive understanding of the relevant neuro–tendino–muscular anatomy. For example, acupuncture has been effective for many tendinopathic disorders, such as Achilles tendinopathy, rotator cuff tendonitis, and tennis elbow.24–26 However, the acupuncture literature for the treatment of DQT is limited and results are usually poor. One trial study by Hadianfard et al. compared the efficacy of acupuncture versus corticoid steroid injection and failed to show that acupuncture was more effective. 27 In the Hadianfard et al. study, the selection of acupuncture points was poor and failed to target the APL and EPB muscles specifically. In another case study by Howell, the treatment design once again failed to target the APL and EPB muscles. 28
A treatment proposal study by da Silva et al. emphasized the importance of needling, among other acupuncture points, the APL and EPB muscles in the treatment of DQT in order to reduce muscle shortening and spasms that can result in chronic overload of the tendons due to repetitive stress. 23 This approach seems to be the most comprehensive of all the studies because it included the neuroanatomical structure of the tissues directly involved in the pathology. However, da Silva et al. relied only on palpation to needle the APL and EPB. There was no confirmation of precise and effective needling of the muscles via electrical stimulation. Nonetheless, da Silva et al. recommend verification of correct needling with a unipolar stimulator in order to contract the APL and EPB muscles.
To achieve reproducible therapeutic results, the current authors propose confirmation of EPB and APL via electrostimulation at their corresponding acupoints, TE 6 and TE 8, to influence the two muscles that are relevant to DQT.
Summary
Each of the current authors' proposed classical locations of acupoints TE 1–TE 10 has unique and distinctive anatomical targets. TE 6 and TE 8 correspond to the EPB and APL muscles, respectively. It is interesting and clinically significant to note the relative classical location of TE 8 to TE 6: “1 cun behind.” Anatomically, the APL muscle is found directly proximal to the EPB muscle. This description has neuroanatomical and functional significance and can be corroborated by applying unipolar electrostimulation to each needled acupoint. Distinctive muscular contraction of the EPB (TE 6) and APL (TE 8) muscles can be observed resulting in extension and abduction of the thumb, respectively (Supplementary Video S2).
It is the current authors' opinion that contemporary textbooks emphasize functions and indications of acupoints, which is important primarily for the internal medicine application of acupuncture. However, when treating musculoskeletal dysfunction and managing pain, emphasis should be given to the acupoint's neuroanatomical specificity. Together, the accurate neuroanatomical stimulation of a set group of acupoints can correct primary and secondary musculoskeletal dysfunctions and lead to outstanding clinical results.
Comparatively, several studies have shown that manual and electrical stimulation of verum acupoints modulate a wider extension of brain areas and elicit greater intense responses, compared to control points or nonacupoints in healthy volunteers.29–32 Future studies should determine if stimulation of specific neuroanatomy-based acupoints leads to greater intensity, or perhaps has greater specificity, in neuromodulation of brain areas compared to nonacupoints and/or contemporary non-neuroanatomy–based acupoints.
Conclusions
Classical acupoints are highly precise landmarks in the body that facilitate access and stimulation of distinct neuroanatomical target tissues. The current study demonstrated that acupuncture is not anatomically redundant; instead, each acupoint has a unique neuroanatomical target—even when acupoints are relatively close to each other. Classical acupoints show that the authors of ancient acupuncture classics had a clear understanding of where to stimulate the body, based on detailed knowledge of neuroanatomy. This wisdom was transmitted through Classical scripts and detailed carvings of acupuncture sculptures to preserve for future generations the most optimal neuroanatomical target sites.
The current study demonstrated the differences in the anatomical interpretations between the Systematic Classic and C&M, with the latter shown to have inaccuracies in its neuroanatomical descriptions of acupoints. For the 10 forearm acupoints of the TE meridian, four acupoints (TE 2, TE 3, TE 4, and TE 10) missed the corroborated neuroanatomical targets and the rest lacked anatomical specificity (TE 1) or were found to have redundant neuroanatomical targets (TE 5, TE 6, TE 7, TE 8, and TE 9). To illustrate the importance of transliteration and adherence to the knowledge transmitted in the earliest classics—the Spiritual Pivot and Systematic Classic—the current authors highlighted the various anatomical locations of TE 10 from different historical periods and identified a possible source for its location drifting from Classical times as early as the Song Dynasty.
Clear knowledge of neuroanatomical targets within each acupoint is clinically important. An acupuncturist can be certain of effective needling by knowing beforehand the correct cutaneous paresthesia or motor response of each neuroanatomical target or, in Chinese Medicine terms, reproducible De Qi sensation.
In summary, this research article provided evidence that Classical acupoints are grounded in neuroanatomy. The authenticity of acupoints was verified using peer-reviewed anatomical research and objective methods, such as acupoint dissection and electrostimulation. Clarity of the specific neuroanatomical targets of acupoints is the first step toward standardizing reproducible acupoint stimulation required for objective clinical research into specific physiologic functions and effects of acupoints.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.