
Abstract
Objective:
Moxibustion (MOX) is used to treat a wide variety of disorders, including those with gastric symptoms. However, the exact mechanisms underlying the beneficial effects of MOX are unknown. The purpose of this study was to investigate if application of indirect MOX (iMOX) to ST 36 reduces restraint stress (RS)–induced alteration in gastric responses of conscious rats, and if a somatoautonomic reflex mediates gastric emptying (GE).
Materials and Methods:
One group of rats was fed solid food after 24 hours of fasting. Immediately after food ingestion. These rats were subjected to RS. Ninety minutes after feeding, the rats were euthanized, and their gastric contents were removed to calculate GE. iMOX had been performed at ST 36 bilaterally throughout the stress loading. To investigate if vagal-nerve activity was involved in mediating the stress-induced alterations of GE by iMOX, atropine was intraperitoneally administered to other rats just before initiating RS; bilateral truncal vagotomy had been performed on day 14 before GE measurement.
Results:
RS delayed GE significantly (42.9 ± 5.8%)in stressed rats, compared to nonstressed rats (68.7 ± 1.8%). iMOX at ST 36 reduced stress-induced inhibition of GE significantly (67.1 ± 2.4%). MOX-mediated reduction of GE disappeared upon atropine injection and vagotomy.
Conclusions:
RS-induced delayed GE may be ameliorated by iMOX at ST 36. Somatoautonomic, reflex-induced vagal-nerve activity helps mediate the stimulatory effects of iMOX on RS-induced delayed GE. As a complementary and alternative medicine, iMOX may also be advantageous for patients with gastric disorders, such as functional dyspepsia.
Introduction
Moxibustion (MOX) is a treatment that gives thermal stimulation to the acupoints, and is one of the most important traditional Japanese medicines. As a technique used in medical treatment, Japanese-style acupuncture often involves the use of MOX to achieve optimal results. MOX is also used as a self-care treatment. Moreover, MOX is used to treat a wide variety of disorders in areas such as gastroenterology, cardiology, and urology, to name a few. 1 In gastroenterology, several studies have examined the effectiveness of MOX in irritable-bowel syndrome, ulcerative colitis, Crohn's disease, and gastric ulcers. Although the efficacy of MOX for treating several symptoms and/or diseases has been demonstrated clinically, little is known about its underlying mechanisms.
Previous studies have reported on the effect of MOX on gastric motility and presented contradicting results. Tobosa et al. 2 showed that suspending MOX over the abdomen, but not the hind limbs (ST 36 and SP 6), increased gastric emptying (GE) of plastic beads significantly. Sugai et al. 3 demonstrated further that suspending MOX over the abdomen (REN 10, REN 12, and ST 25) increased GE via the 5-hydroxytryptamine pathway. In contrast, studies that used a heat generator as a MOX-like stimulus, showed an increase in heat stimulation at ST 36 and a decrease at CV 12, as measured by the intrapyloric balloon method.4,5 While there are differences in measurement methods and in MOX devices used, it is evident that opinions are divided in these reports.
This current study investigated the effect of indirect MOX (iMOX) at ST 36 in relation to restraint stress (RS)–induced gastric emptying (GE) and the mechanisms of action. Specifically, the study explored if the effect of iMOX on RS-induced GE was mediated via the vagal efferent nerve and the central endogenous opioid pathway.
Materials and Methods
Seventy-two male Sprague–Dawley rats (body weight: 250–300 g) were used in this study. The rats were obtained from a commercial supplier (CLEA Japan, Inc., Tokyo, Japan). The animals were housed in standard cages, maintained on a 12-hour day–night cycle (08:00–20:00), with free access to food and water. All animals were kept in individual cages in a controlled environment at a constant temperature (23°C). The rats were adapted to the conditions for 1 week.
All animal experiments were carried out as approved by the Animal Care and Use Committee of the Meiji University of Integrative Medicine, Kyoto, Japan (approval numbers: 22-20 for the study of moxibustion and atropine; 23-5 for the study of naloxone; and 24-2 for the study of vagotomy), and in accordance with the regulations provided by the U.S. National Institutes of Health Guide for the Care and Use of Laboratory Animals. 6 All efforts were made to minimize animal suffering and to reduce the number of animals used in experiments.
Restraint Stress
As has been previously described,7,8 each rat was placed on a wooden plate with the animal's trunk wrapped in a confining harness consisting of a bandage created from packaging tape for 90 minutes. The rats were able to move their limbs and heads but not their trunks.
iMOX Procedure
The MOX used in this experiment was iMOX (iMOX, Kamayamini-Kyo, Kamaya, Japan). The structure and temperature curve of iMOX are shown in Figure 1. The peak temperature and time of iMOX were 65.7 ± 1.3°C and 190 ± 6 seconds, respectively. iMOX was performed above ST 36 bilaterally. ST 36 is located at 5 mm lateral to and below the anterior tubercle of the tibia in rats.9,10 Hair located around the acupoint bilaterally was cut off to expose the local skin before iMOX application. Given that the heat sensation caused by iMOX occurs during stress, 6 iMOX applications were performed at 5, 20, 35, 50, 65, 80 minutes, alternating left and right, and after food feeding, with the rats fully conscious.
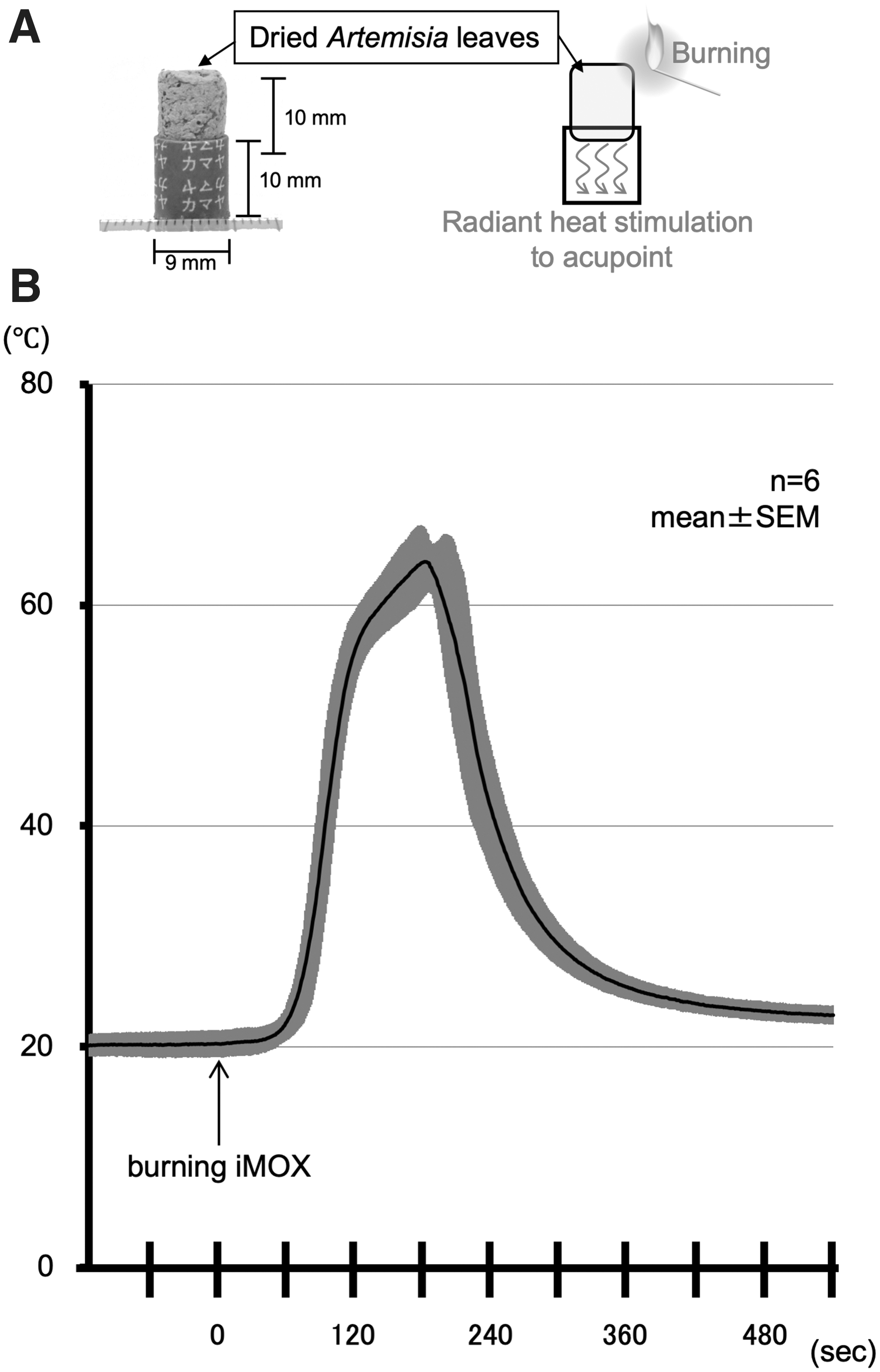
Indirect moxibustion (iMOX) used in the current study.
Gastric Emptying Study
Before the experiments began, the rats were fasted for 24 hours but allowed water ad libitum. The rats were given a solid food pellet (1.5 ± 0.1 g) for 10 minutes, as has been previously described.7,8,11 Rats that did not eat all 1.5 g of the food within 10 minutes were eliminated from the experiment. Immediately after feeding, the rats were subjected to RS for 90 minutes as described above. Ninety minutes after stress loading, the rats were euthanized by cervical dislocation and exsanguination after confirmation that the heartbeat and breathing had stopped by an overdose of isoflurane inhalation. Each rat's stomach was surgically removed after euthanizing, and the gastric contents were recovered, dried, and weighed. Solid GE was calculated using the following equation, as has been previously described:7,8,11
Gastric emptying(%)= [1-(dried weight of food recovered from stomach/weight of food intake)]*100
Pharmacologic and Surgical Approaches
To investigate if endogenous opioid and muscarinic neurons are involved in the mechanism of action of iMOX in GE, naloxone hydrochloride (a nonselective opioid receptor antagonist; Sigma Chemical Co., 1.0 mg/kg) or atropine methyl bromide (a muscarinic receptor antagonist; Sigma Chemical Co., 50 μg/kg) were administered intraperitoneally immediately before applying RS. These antagonists were dissolved in saline at 1 mL/kg. These doses and administrations were based on previous reports.12,13
To determine if the parasympathetic pathway mediated the GE improvement caused by iMOX, a truncal vagotomy was performed under anesthesia (2% isoflurane). This surgical procedure had been performed 2 weeks before the GE recording. A previous report had indicated that this was the optimum amount of time required to remove any effects that the surgical operation might have had on gastric function. 10 Truncal vagotomy was performed by cutting the vagal trunks around the abdominal esophagus, as has been previously described. 10 Saline-injected rats served as controls to each pharmacologic agent.
Statistical Analysis
All results were expressed as mean ± standard error (SE). Initial statistical comparison for multiple groups was made using a one-way analysis of variance (ANOVA). If a difference was detected, post hoc analysis (Tukey–Kramer test) was then performed. Statistical comparison between the 2 groups was performed using a nonpaired t-test. P < 0.05 was considered significant.
Results
RS significantly delayed GE (42.9 ± 5.8%; n = 8; one-way ANOVA P = 0.0001; post hoc P = 0.0003) unlike in non-RS rats (68.7 ± 1.8%; n = 8). iMOX at ST 36 significantly improved RS-induced inhibition of GE (67.1 ± 2.4%; n = 8; post hoc P = 0.0005; Fig. 2).

Effect of indirect moxibustion (iMOX) at ST 36 on gastric emptying (GE) in the different groups. Analysis via one-way-analysis of variance (ANOVA), followed by a Tukey–Kramer test. *P < 0.05. SE, standard error; NS, nonsignificant (statistically).
GE in rats treated with atropine and RS was 29.0 ± 3.8% (n = 8). iMOX at ST 36 had no stimulatory effect on delayed GE induced by RS in the presence of atropine (28.9% ± 2.2%; n = 8; nonpaired t-test P = 0.9914; Fig. 3).
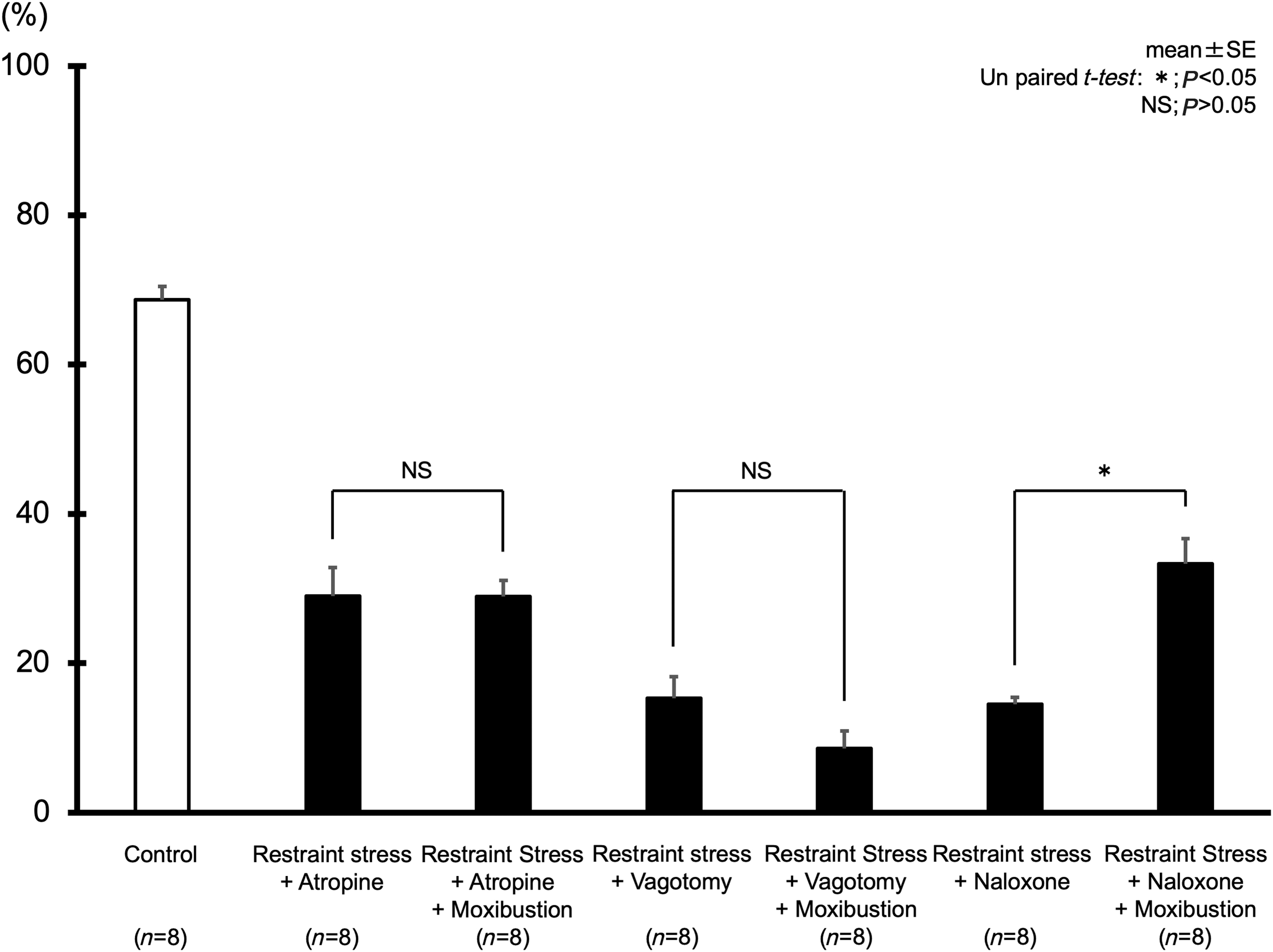
Involvement of the muscarinic receptor, vagal nerve, and endogenous opioid in indirect moxibustion (iMOX)–mediated improvement of restraint-stress(RS)–induced gastric emptying (GE). Analyses were via nonpaired t-tests. *P < 0.05. SE, standard error; NS, nonsignificant (statistically).
RS delayed GE to 15.3 ± 2.9% (n = 8) in rats who underwent vagotomy. GE of vagotomized rats almost completely abolished iMOX-induced improvement of GE (8.6% ± 2.3%; n = 8; nonpaired t-test P = 0.0928; Fig. 3).
GE in rats treated with naloxone and RS was 14.5 ± 0.9% (n = 8). iMOX at ST 36 had a stimulatory effect on delayed GE induced by RS in the presence of naloxone (33.3% ± 3.4%; n = 8; nonpaired t-test P = 0.0007; Fig. 3).
Discussion
In the present study, iMOX at ST 36 reduced stress-induced delayed GE. The accelerating effects of iMOX were mediated by the vagal pathway via the muscarinic receptor, but not through endogenous opioids.
A study by Chiba et al. indicated that the maximum temperature reached by iMOX was ∼65°C on the skin and 45°C in the subcutaneous layer. 14 Given that the maximum temperature reached by the iMOX was 65.7 ± 1.3°C on the thermocouple, it was assumed that the skin temperature at ST 36 reached the same level. Although maximum temperature is dependent on the basal skin temperature, 15 iMOX in this study increased above 45°C in the subcutaneous layer.
MOX evokes multisensory sensations, including touch, pressure, warmth, pain, and chemical senses. 16 The temperature of heat stimulation (46°C) predominantly targeted unmyelinated C afferent fibers. 17 Transient receptor potential cation channel subfamily V member 1 (TRPV1) can be activated by capsaicin, low pH, low voltage, and high heat stimulation (> 42°C). TRPV1 transcript and protein were also found to be most highly expressed in sensory neurons, especially in small-diameter neurons within the dorsal root ganglia (RG) and trigeminal sensory ganglia. This is likely due to cell bodies consisting of unmyelinated C-fibers.18,19 This is consistent with the knowledge that polymodal C–fibers are involved in nociception. The upregulation of TRPV1 expression in DRG was considerably greater in the 46°C MOX group than in the 38°C MOX group. 20 Local MOX-like stimuli at 43°C modulated gastric motility via TRPV1 heat nociceptors. 4 Thus, the results of this study suggest that the effect of iMOX was determined by the activation of TRPV1, which is associated with the stimulation of C-fibers.
GE is delayed by psychologic and physical stress.7,11,21–26 Intracisternal or intracerebroventricular injection of corticotropin-releasing factor (CRF), which is produced in the hypothalamic paraventricular nucleus (PVN), reduces delayed GE.7,27,28 RS increases CRF mRNA in the PVN and amygdala. 29 Thus, endogenous CRF plays an important role in mediating stress-induced inhibition of GE. 11 However, the major downstream targets of PVN neurons are the sympathoexcitatory neurons of the rostral ventrolateral medulla (RVLM).30–33 RVLM CRF–receptor activation acutely activates lumbar sympathetic nerve activity, 34 indicating that sympathoexcitation is likely to mediate the pressor response to RVLM CRF. 35 Moreover, RS inhibits GE via a central CRF type 2 receptor and the peripheral sympathetic neural pathway via the ß-adrenoceptor.7,26 Therefore, this study suggests that RS might induce CRF in PVN, which, in turn, stimulates the sympathetic nerve via the CRF receptor of the RVLM.
A previous report showed that acupuncturelike stimulation at the hind paw elicited excitatory gastric motility, which was accompanied by increased activity of the gastric vagal efferent nerve as a somatoautonomic reflex. 36 Electroacupuncture (EA) can also accelerate gastric motility and GE via excited vagal nerve activity.10,11,37 Moreover, acupuncture or EA at ST 36 significantly increased the number of c-Fos immunopositive cells at the mediocaudal and caudal nucleus tractus solitarius (NTS), and the dorsal motor nucleus of vagus (DMV). 38 Thus, exciting somatic neurons at ST 36 stimulates the vagal efferent nerve via the NTS and DMV, which enhances gastric motility. In this study, iMOX at ST 36 accelerated GE, which completely abolished the effect of atropine administration and truncal vagotomy. These results suggest that iMOX can stimulate the vagal efferent nerve via NTS and DMV via the somatoautonomic reflex.
It has also been shown that EA at ST 36 leads to the induction of the central opioid system. 39 Previous studies have shown that endogenous opioids were involved in EA-induced analgesia in somatic pain and visceral hyperalgesia.40–43 The antiemetic effect of EA is also mediated via the central opioid pathway. 44 Moreover, the stimulatory effect of manual acupuncture is determined in part by the opioid pathway. 10 Opioid receptors in the RVLM mediate the inhibitory effects of EA.45–48 Thus, it seems that the underlying mechanism of action for manual and EA is associated with the release of endogenous opioids in analgesia and the regulation of visceral function.
In contrast, endogenous opioids were not involved in the somatoautonomic reflex on arterial pressure by manual acupuncture. 9 Opioid-receptor blockade was ineffective for disrupting the reflex pathway of acupuncturelike stimulation–induced bradycardia. 49 Naloxone did not affect the stimulatory effects of EA on stress-induced delayed GE. 11 Naloxone did not block the effect of auricular EA on gastric sensitivity to gastric distention. 50 Thus, previous studies have shown opioid involvement in the mechanism of acupuncture depending on various conditions. The stimulatory effects of acupuncture at ST 36 were mediated, in part, via opioid pathways in the interdigestive state. 10 In contrast, enhancement of GE by EA was not mediated via opioid pathways during the fasting state. 43 This result suggests that iMOX might influence GE in the interdigestive state but not during the fasting state.
Functional dyspepsia (FD) is defined as persistent or recurrent pain/discomfort centered in the upper abdomen, without organic disease. FD is a common functional gastrointestinal disorder. Prevalence of dyspepsia in the general population ranges from 5.3% to 20.4%. 51 FD causes a variety of symptoms, including epigastric pain and/or discomfort, early satiety, postprandial fullness, bloating, and nausea.52,53 FD-induced chronic symptoms markedly reduce a patient's quality of life.54,55 Multiple factors are associated with the development of FD of which psychologic stress plays a major role.56,57 Psychologic and physiologic stresses, such as RS, have been shown to feed inhibition and gastric hypersensitivity, and inhibit antral motility and GE in studies with rats.7,8,58,59 Transportation of food residue to the duodenum via GE is one of the most important postprandial functions of the stomach. 60 An estimated 30%–50% of patients with FD have motor disorders, such as delayed GE and impaired gastric accommodation after a meal. 61 Although GE is delayed by gastric ulcers and diabetic mellitus,62,63 it is important to ameliorate abnormal stress-induced GE in patients with FD.
Given that iMOX can reduce stress-induced delayed GE and can be used as a self-care treatment, iMOX might also be advantageous for patients with FD as a complementary and alternative medicine.
The effect of iMOX alone could not be established, as the results suggested that iMOX and ST 36 act together. Therefore, it is necessary to compare this result with those of other acupoints. Moreover, the mechanisms of action relating to iMOX involve the combination of heat (burning pain and heat stress), tar (extract), aroma (fume), and psychologic stress. 16 Hence, the effect of iMOX should be considered in multiple stimulations. Although thermal stimulation is central to MOX, it is necessary to consider the possible influence of other stimuli.
Conclusions
The results of the current study provided strong evidence that improvement of GE by iMOX at ST 36, on RS-loading rats, was a somatoautonomic reflex, similar to that induced by acupuncture. The afferent pathway might be associated with unmyelinated C-fibers via the TRPV1 receptor, while the efferent pathway is related to vagal-nerve activity via the muscarinic receptor. iMOX at ST 36 on humans should be evaluated appropriately.
Footnotes
Acknowledgments
The authors are deeply grateful to Professor Toku Takahashi, MD, PhD, of the Medical College of Wisconsin for his assistance in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by JSPS KAKENHI (Grant Number JP15K21508 to H.T.).