
Abstract
Objective:
Auriculotherapy practitioners need a digital record-keeping method to track their cases that provides different ear maps and methodologies from different schools of auriculotherapy in one place.
Materials and Methods:
Main requirement were as followed: to be run whatever the platform; to manage different representations of the ear and to allow data analysis from multiple users.
Results:
Aurimatrix® is a software-as-a-service solution developed to help the practitioner enter all data pertaining to an auriculotherapy session. Although the software was originally designed for the two schools of French auriculotherapy, this software is highly configurable and can support the use of any ear chart in any language. Moreover, the ear charts are divided in several layers, allowing use of a representation of the ear of one school with the set of auricular points in use in another school. Because the list of medical conditions is limited and the modalities of variables used to evaluate the effectiveness of auriculotherapy are unchangeable, Aurimatrix enables comparison between different sessions, different patients, and different practitioners.
Introduction
Medical record keeping has become a legal requirement for practitioners. Because auriculotherapy remains an unsung therapy, no software dedicated to the management of this practice currently exists. Hence, practitioners have the choice to use one of the many kinds of available medical software, to use office software applications, or to record their cases on paper sheets.
All of these solutions are limited: for example, nonspecialized software does not allow quick entry of ear points. Paper-and-pen solutions are time-consuming and subject to errors in data-input procedure.
To provide practitioners with a digital solution, software-as-a-service (SAAS) solution was designed jointly with lecturers of the interuniversity diploma (in French DIU for Diplôme Inter Universitaire) for auriculotherapy and from a Lyon medical study group (in French GLEM for Groupe Lyonnais d'Etudes Médicales), that is the continuation group of Paul Nogier, MD's legacy.
The aim of developing this software was to give practitioners the opportunity to enter all data associated with auricular sessions and to use the data related to patients or medical conditions, and to provide researchers with a common framework to allow analysis with data from different practitioners.
Materials and Methods
Type of Software and Storage
SAAS was preferred to executable software because a SAAS can be run via a browser on any the operating system or platform—including a smartphone. Data should be encrypted and patients' identifiers should not be stored remotely.
Ear Mapping
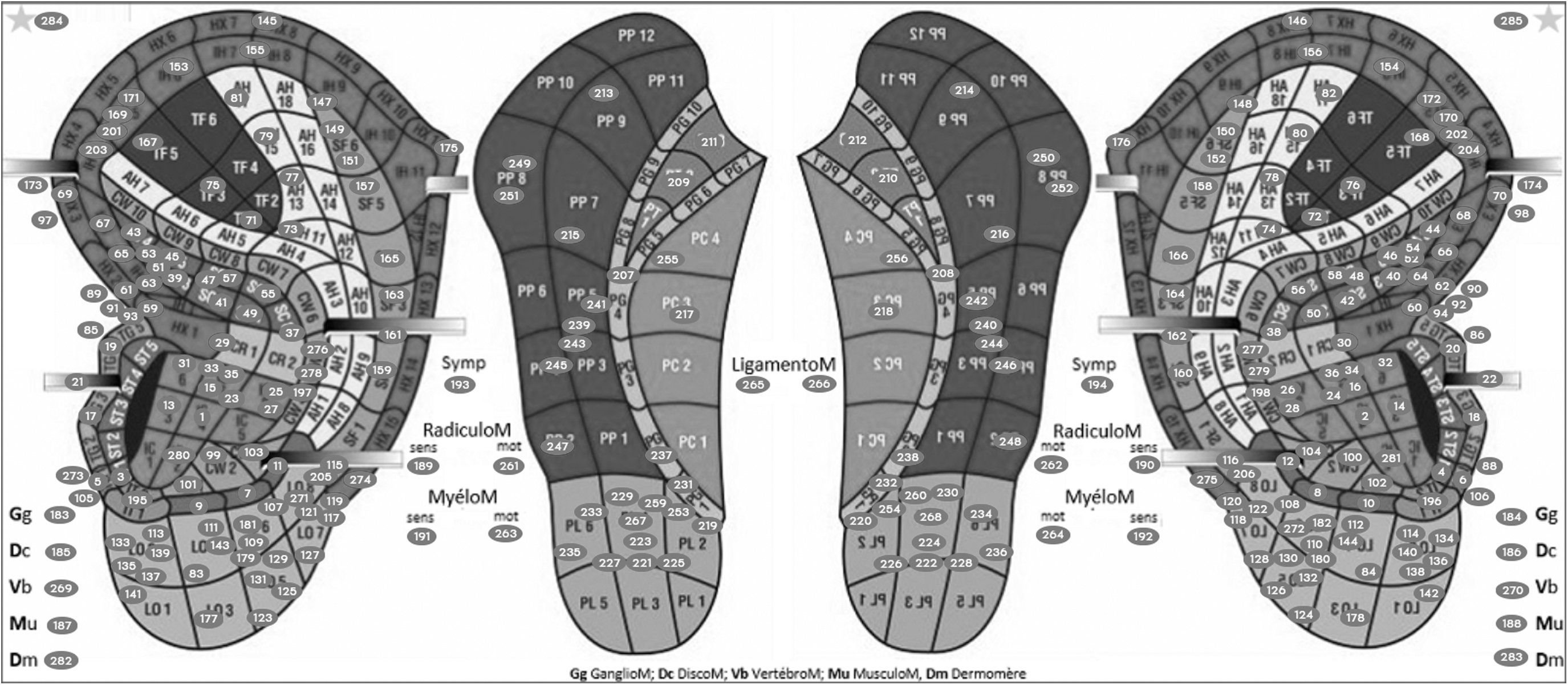
The ear mapping includes three different layers. The first layer is the representation of the ear. It can be either a drawing or a picture of an ear. The second layer is the reference system used to locate the ear points. Two different systems are used: (1) the “grid” system or (2) the “anatomical” system. The grid system was the first mapping of the ear, proposed by Kovacs and is still in use as square grids in a German group. 1 Next to square grids, radial grids were proposed by other researchers: (1) Romoli devised a system dividing the auricle in 40 equal parts originating from the concha ridge 2 ; (2) Alimi proposed a 20 × 20 grid radiating ahead of the tragus 3 ; and (3) an anatomical system was proposed by the World Federation of Acupuncture-Moxibustion Societies 4 and by Oleson. 5 The third layer is the set of points. Although the original points originated from Dr. Paul Nogier's work, each group developed its own version. From one version to another version, some points are not accepted by all groups, and some shared points do not share the same locations on the auricle.
The specifications of the software were the ability to manage different representations of the ear and different sets of points, and to be modifiable.
Reporting of Medical Conditions
It was beyond the scope of this software to be able to encode all possible medical conditions, whereas the eleventh International Classification of Diseases had ∼15,000 entities. 6 The list of medical conditions had to comply with 2 opposite objectives: (1) to be broad enough to encode as many encountered diseases that could be addressed beneficially by auriculotherapy and (2) to be as short as possible to enable multiple comparisons. A distinction was made between a symptom and an etiology. Both symptom and etiology lists had to be extendable on request.
Enter a Session of Auriculotherapy
The specifications were as follows: (1) The software had to let a practitioner select an ear point by clicking on it. (2) For each selected point, the name of the point had to be associated with key features, such as the path of stimulation or various comments. If the ear had to be transfixed with needles, the pathways in and out had to be available, whatever the nature of the pathway out (i.e. another point or a metameric level) might be.
Evaluating the Effectiveness of Auriculotherapy
The effectiveness of auriculotherapy had to be quoted with 2 variables: (1) the intensity of the response and (2) its duration. Coding the intensity had to include a worsening of the medical condition. Side-effects of the session had to be quoted too.
Results
Type of Software and Storage
Patients identifiers are encrypted locally like passwords before being saved on remote servers. All data stored on servers are encrypted. These servers are in France. Aurimatrix,® the software that was developed, is available in French.
Ear Mapping
This version of Aurimatrix includes 2 representations of the ear and two sets of points. The representations of the ear are associated with a noneditable reference system. Two representations are in use: (1) a radial grid system based on Alimi's work and (2) an anatomical system introduced by Oleson.3,5 Two sets of points are proposed: (1) the one in use by the Lyon medical study group and (2) the one by the French interuniversity diploma group. Furthermore, a blank ear map is available, enabling recording of ear zones rather than ear points. Figure 1 summarizes what is currently available to users.
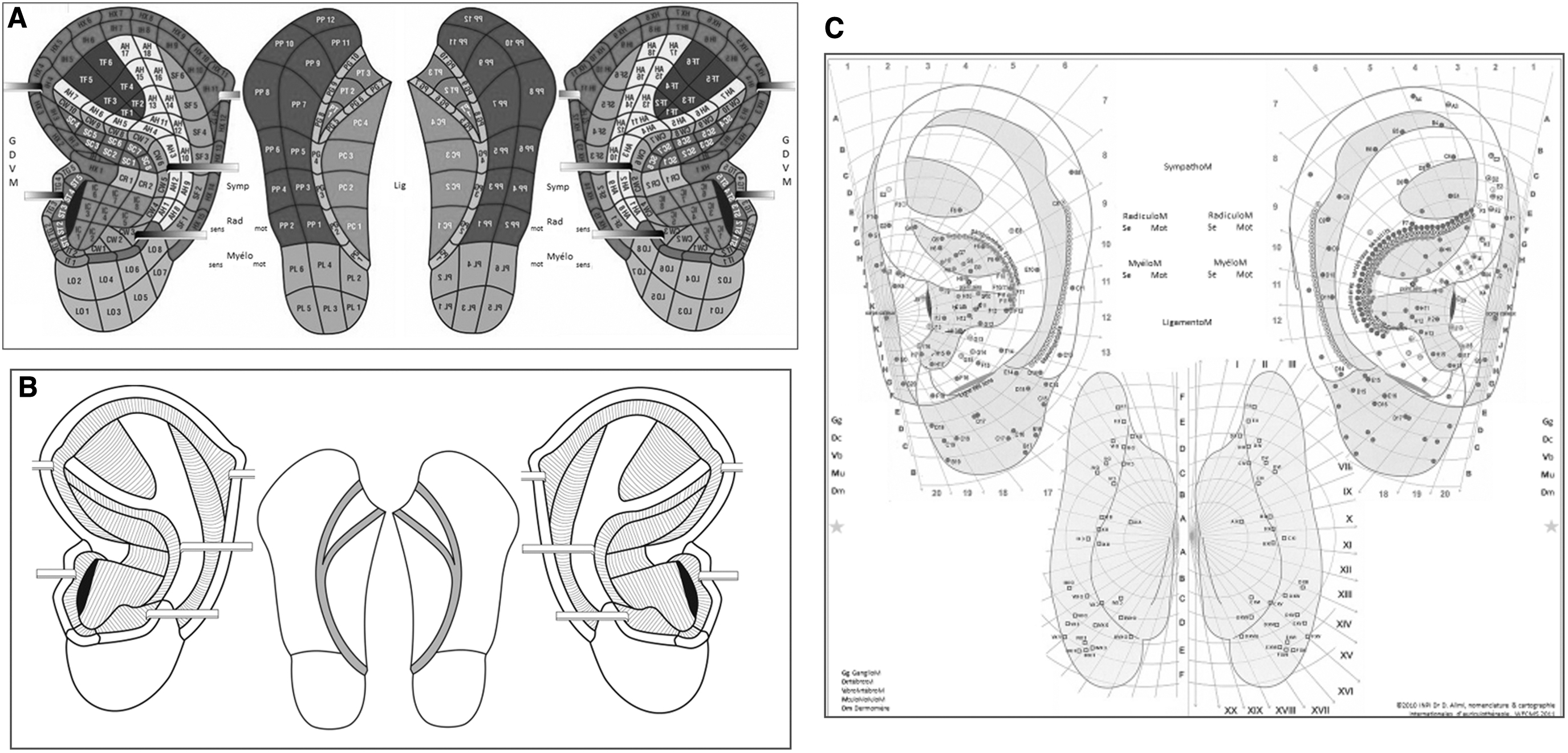
Ear charts in use in Aurimatrix.®
Reporting of Medical Conditions
A short list of fewer than 100 symptoms and 130 etiologies were selected. Medical conditions are grouped by medical and surgical specialties.
Enter a Session of Auriculotherapy
To illustrate the specifications, a fictive session was reported. Figure 2 represented the support used—representation of the ear from Oleson with the set of points from Alimi. Clicking on a point such the ones pictured in Figure 2 generated a line on a table as shown in Figure 3. In this example, 5 points were entered. The first point was a skewering of radicular points with a needle from metameric S-1 to L-3 levels. The second point was a transfixion of a radicular point at the L-5 metameric level with a needle. The third point was the puncture of the reticular point with a semipermanent needle (Aiguille Semi-Permanente® [ASP®], Sedatelec,® Irigny, France). The fourth point was the puncture of the thalamus point with a cryogenic needle (Matauris,® Maisons Alfort, France). The fifth point was the electrical stimulation of the sensory Master point. For each point, various comments could be entered into the system, such as comments related to the skin, methods, or detection features. Comment columns could be shown or hidden. In the example, only the comment column related to skin features was not hidden.
Oleson's ear map with Alimi's set of points.

Entering points during an auriculotherapy session.
Evaluating the Effectiveness of Auriculotherapy
The variables selected to assess the effectiveness of an auriculotherapy session were the intensity of the effect; the duration of the effect; and ancillary data such as side-effects, delayed effectiveness, and other comments.
The intensity of the effectiveness is quoted on a 7-modality scale, ranging from none to complete improvement. The coding includes the possibility to quote “worsening” or “not evaluable.” The duration of improvement ranges from 48 hours to more than 6 months on a 9-modality scale. The coding includes the “not evaluable” and “no effect” items.
Discussion
To date, Aurimatrix is the only software to provide the caregiver with the opportunity to enter sessions of auriculotherapy irrespective of the school of auriculotherapy. Key points are the ability to manage patients' databases, to compare different protocols, and to be used regardless of the school of auriculotherapy. For 1 school, Aurimatrix allows the dissociation between the representation of the ear and the set of ear points.
Aurimatrix cannot be compared with Auriculo 360® (Miridia Technology Inc., Meridian, ID, USA), the only software dedicated to auriculotherapy to date. Unlike Aurimatrix, the latter is a research tool, Auriculo 360 is an educational tool providing the user with points and protocols on a 3-dimensional view of the ear. This software offers the possibility to add points and protocols, but not to amend existing ones. It does not support the management of a consultation of auriculotherapy or a patient's database.
Limitations of Aurimatrix are the 2-dimensional (2-D) representation of the ear and the language of the software. A 2-D ear does not prevent a practitioner from representing points because 2 solutions are used: either (1) an unfolded ear, like the one proposed by Oleson, or (2) different attributes associated to a point like the system proposed by Alimi.3,5 Languages packs are being implemented.
Conclusions
Aurimatrix is an SAAS designed to manage auriculotherapy sessions and store a database on patients receiving this treatment. The software's main strength is the ability to manage different ear charts and sets of points from different auricular schools as well as the possibility to merge observations of different practitioners.
Footnotes
Acknowledgments
The current authors are grateful to Terry Oleson, PhD, and David Alimi. MD, for having provided their ear maps and allowing use of them for the Aurimatrix. Thanks are also extended to all the teachers and students with interuniversity diploma of auriculotherapy for their helpful comments.
AUTHORS' CONTRIBUTIONS
Dr. Sagui conceived of the software and drafted the article. Dr. Maugendre helped substantially with conceiving of the software, added new functionalities, and revised the article. Dr. Costadura improved the software and revised the article.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
Conception and maintenance of the software were financed by public funding (the University of Paris–Saclay, France), a nonprofit organization, (the Complementary and Alternative Medicine Institute [Institut des Médecines Alternatives et Complémentaires] by B. Paquier, MD, of Lyon, France), and by the authors.
Use of the software is free of charge for clinicians. Data belong to the clinicians and no commercial use will ever be made of any collected or stored data.