
Abstract
Objective:
This pilot study explored interactions of domains of physical, psychologic, and social factors in the Patient-Reported Outcomes Measurement Information System®
Materials and Methods:
PROMIS-29 profile, version 2.1 was applied among participants with chronic musculoskeletal pain, who received acupuncture treatment for 5 weeks. Data from function-oriented and symptom-oriented domains as well as changes in pain intensity were evaluated at weeks 0, 3, and 5, in 9 patients who completed full sessions. Scores of the domains were analyzed by hierarchical cluster analysis at each timepoint to identify the patterns of interactions of PROMIS domains.
Results:
Hierarchical cluster analysis revealed the existence of 2 main clusters: one consisting of pain, fatigue, and emotional domains; the other comprising physical function and social domains. The general pattern was stable but interactions were found throughout the treatment. The score for sleep disturbance did not improve but was correlated with different domains at varying stages of treatment.
Conclusions:
Interaction between 2 clusters of pain with fatigue and emotional domains; and physical function with social domains showed that acupuncture produces holistic reductions in chronic musculoskeletal pain. However, the limitation of sample size and bias in this pilot study requires future research on the need to adopt an interdisciplinary and holistic approach to the recovery of patients with chronic musculoskeletal pain, who have dynamic needs.
INTRODUCTION
The Patient-Reported Outcomes Measurement Information System® (PROMIS®) is to be a trustworthy instrument for measuring the various domains of quality of life (QoL), encompassing the multiple dimensions of pain-related physical health, mental health, and social health; the system has revealed positive outcomes. 1 PROMIS provides 8 domains for evaluating pain and health-related QoL. 2 The PROMIS profile, version 2.1, covers function-oriented and symptom-oriented domains of pain interference, pain intensity, physical function, fatigue, depression, anxiety, sleep disturbance, and participation in social roles and activities. Assessment of domains promotes understanding of acupuncture and enables further development of this traditional therapy in modern and future medicine. 3
Chronic musculoskeletal pain is one of the most-successful indications for acupuncture. Mounting evidence in recent decades has demonstrated that acupuncture is a safe, cost-effective, and efficacious therapy with minimal risk.4,5 Acupuncture has good effectiveness for treating chronic musculoskeletal pain in different locations, including the head,6,7 neck,8,9 back,10,11 pelvis, 12 and knee, 13 as well as osteoarthritis in other joints.14,15
Acupuncture views the human body as an integrated system, considering the interplay among organs and viscera, the mind and the body, and the internal and external environment, to comprehend the balance and regulation of normal physiologic functions. 16 Studies demonstrate that acupuncture's advantages extend beyond alleviating pain, encompassing enhancing bodily functions, regulating emotions, and elevating QoL.17,18 While PROMIS can be used to assess these aspects, it is yet to be determined how physical, mental, and social factors interrelate and how these relationships emerge during treatment.
Inspired by research on the PROMIS system and the effect of acupuncture on chronic musculoskeletal pain, the current authors' team conducted a pilot study to explore the dynamic relationships among the domains in the PROMIS-29 system during acupuncture treatment and to try to explain the effect of acupuncture on the complex nature of musculoskeletal pain and its treatment.
MATERIALS AND METHODS
Study Design
Using a quasiexperimental methodology, this study was conducted to collect data on PROMIS-29 results at 3 distinct evaluation intervals. The study protocol was approved by the institutional review board (IRB) of the AOMA Graduate School of Integrative Medicine, in Austin, TX, USA. All participants provided written informed consent.
Participants
Individuals with chronic musculoskeletal pain were recruited through AOMA South Clinic flyers and were recruited without discrimination based on ethnicity. Eligible participants were at least 18 years' old, reported chronic musculoskeletal pain for more than 12 months, had not undergone acupuncture treatment in the preceding 3 months, and were willing to provide informed consent. Exclusion criteria during screening included acute pain, physical injury, pregnancy, psychosis, history of drug or alcohol abuse, use of analgesics, or prior pain treatment.
Intervention
Surveys based on PROMIS-29 were conducted at 0, 3, and 5 weeks during participants' weekly acupuncture treatments for 5 continuous weeks. The Traditional Chinese Medicine style of acupuncture was used but the choice of acupoints was determined by the specific location of each participant's pain. The treatments were administered by 5 licensed acupuncturists who were Diplomates of the National Certification Commission for Acupuncture and Oriental Medicine and had a minimum of 5 years of clinical experience. Disposable acupuncture needles (DBC Spring Ten Acupuncture Needles with Guide Tubes, size 0.20 × 40 mm; Dong Bang Corporation, Seoul, Republic of Korea) were used, and no manipulation or electroacupuncture (EA) was applied to ensure the independent effect of needling. Every session lasted for 1 hour with 30 minutes for history taking, physical assessment, preparation, and needle insertions; and 30 minutes for retention of needles. Participants were treated in separate quarters to prevent communication, and adverse events were documented throughout the study.
Outcomes
In the 29-item PROMIS profile, version 2.1, higher scores in the function-oriented domains indicate improved functioning, while lower scores in symptom-oriented domains (pain intensity, anxiety, depression, fatigue, sleep disturbance, pain interference) and total scores represent better status. This PROMIS survey was administered at 0, 3, and 5 weeks, and research data were saved in REDCap® [Research Electronic Data Capture] data-collection software, 19 with access limited to researchers and IRB members. REDCap is a Health Insurance Portability and Accountability Act–compliant software designed to support clinical and translational research.
Data Analysis
Before the analysis, 2 investigators screened all data thoroughly and input results into SPSS. The PROMIS scoring system uses a standard T-score metric, wherein a mean score of 50 is derived from a relevant reference population and the standard deviation is 10. To enable accurate interpretation, the original patient scores are transformed into the T-score metric through the utilization of PROMIS adult profile instrument tables. 20
All statistical analyses were processed using SPSS, version 17. The normality of the data distribution was tested using a Shapiro–Wilk test, and either a simple t-test or a nonparametric Wilcoxon signed-rank test was applied in accordance with the distribution.
In hierarchical cluster analysis (HCA), grouping of data is based on the squared Euclidean distance between pairs of domains, represented by a proximity matrix. Euclidean distance is a measure of dissimilarity used to cluster observations into groups. 21 Average linkage was utilized to cluster the data, which involved calculating the distance between all points in 1 cluster to all other points in another cluster and averaging these distances to decide which clusters with small dissimilarities should merge. 21 Dendrograms were generated to illustrate the hierarchical relationships among the clusters. Each cluster was represented as a branch on the tree, with the length of the branches indicating the absolute value of the Euclidean distance between domains. Shorter branches were of greater similarity between domains in a cluster.
RESULTS
Between April 1, 2019, and August 15, 2019, 17 participants were screened for eligibility, of whom 12 were enrolled and 9 completed full surveys for all 3 timepoints (mean age: 55.3 ± 8.4). During the study, 1 participant lost contact at week 3 and 2 lost contact at week 5. No adverse events were reported. Demographics for the subjects are presented in Table 1.
Baseline Information of Participants
PROMIS Scores
After treatment for 5 weeks, there were improvements in physical function, and reductions of pain intensity and pain interference. In both weeks 3 and 5, the trends of anxiety and depression decreased (Fig.1A); social roles and activities had positively increased (Fig. 1B). In the pain-intensity domain, the chart showed that more patients reported lower scores along with the treatment (Fig. 1C). However, the sleep index did not show improvement during the 5 sessions of treatment. See Table 2.

a: Detected significance between week 0 and week 3; b: detected significance between week 3 and week 5; and c: detected significance between week 0 and week 5. *Significance detected (P < 0.05).
Wilcoxon Signed-Rank Test Detects Statistical Significance
P1 compares week 0 and week 3; P2 compares week 3 and week 5; and P3 is the comparison between week 0 and week 5.
Significance detected (P < 0.05).
PROMIS®, Patient-Reported Outcomes Measurement Information System®; SD, standard deviation.
Hierarchical Cluster Analysis
HCA was used to explore the structure of the clusters and identify dynamic patterns in the data. The relationships among the domains and the pain-intensity scale showed continuous changes during the 5-session treatment. As shown in Figure 2, domains merged at different distances based on the proximity matrices shown in Tables 3–5. The length of the lines connecting the domains indicated similarity: a shorter link meant higher similarity between domains, and a more-extended link meant less similarity.
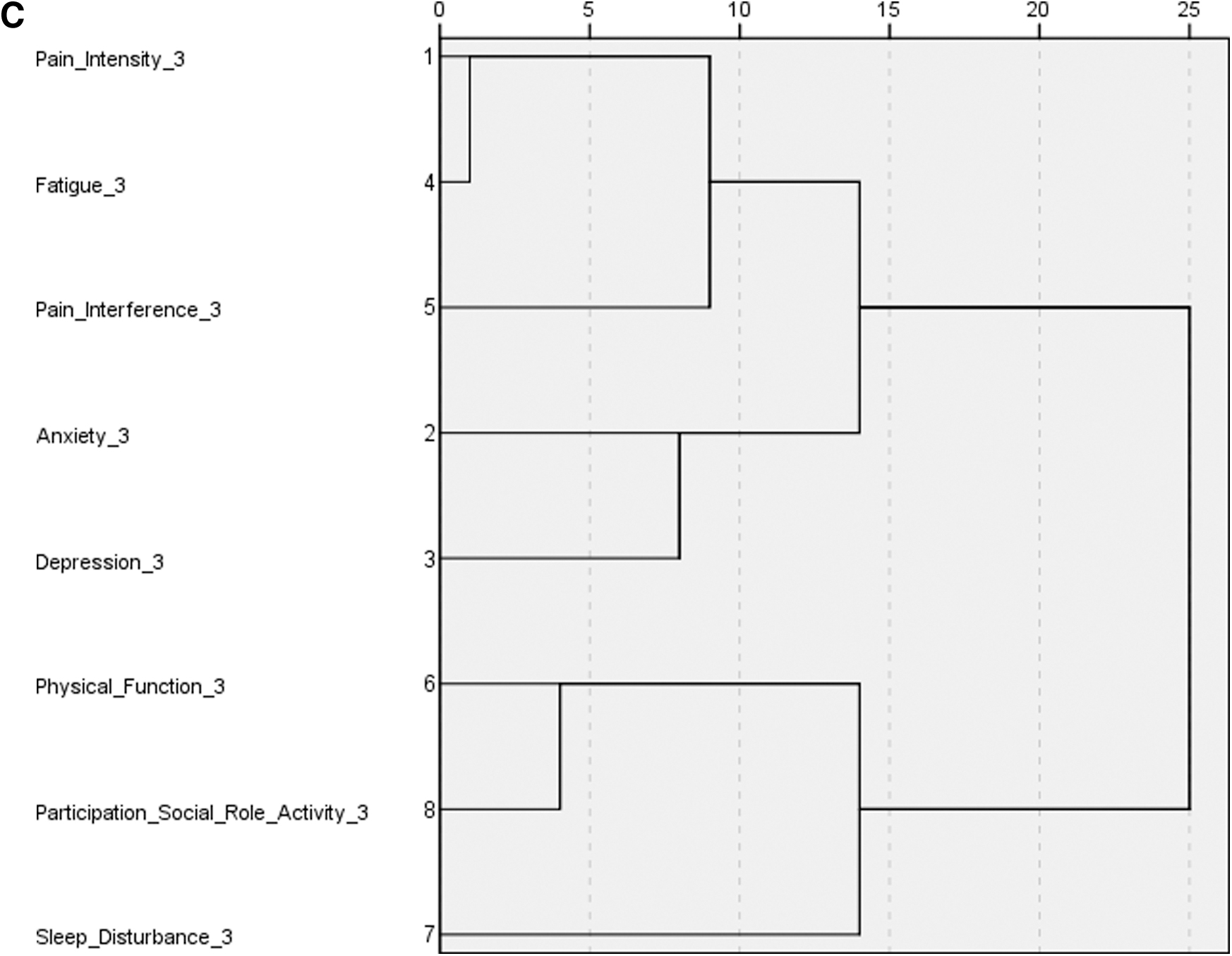
The dendrograms of three timepoints showed that the domains merged into different clusters.
Proximity Matrix of Data at Week 0 a
Results of the squared Euclidean distance between every domain pair, calculated by the average linkage method.
Proximity Matrix of Data at Week 3 a
Results of the squared Euclidean distance between every domain pair, calculated by the average linkage method.
Proximity Matrix of Data at Week 5 a
Results of the squared Euclidean distance between every domain pair, calculated by the average linkage method.
The dendrogram showed that there were 2 main clusters in week 0 (Fig, 2A): depression, fatigue, anxiety, pain intensity, pain interference, and sleep disturbance; another cluster was physical function and participation in social roles and activities. In week 3 (Fig. 2B), the main pattern was similar, but changes occurred. Depression, fatigue, and anxiety were still in the same subcluster, but pain intensity was merged; pain interference was separated from sleep disturbance and joined the cluster of fatigue and emotions; physical function and participation in social roles and activity remained in the same place, but distance was shorter. At week 5 (Figure 2C), domains merged into 2 clusters at a distance of 15: anxiety, depression, fatigue, and pain interference were in 1 cluster; sleep disturbance merged into another cluster of physical function and participation in social roles and activities.
The prevalent pattern was consistent throughout the treatment. Nevertheless, the position of sleep disturbance changed and was correlated with different domains of pain, emotions, and physical and social function at varying stages of treatment.
DISCUSSION
Pain results from complex and dynamic biologic, psychologic, and social interactions. 1 According to the biopsychosocial model, the aim of treatment not only focuses on reducing pain but also on improving QoL, which aligns with the more-realistic expectations of patients. This pilot study used the PROMIS-29 system and data-mining tool to evaluate the multidimensional benefits of acupuncture treatment of musculoskeletal pain.
In recent years, data-mining technology has been applied widely in the analysis of acupuncture research. Rules and patterns behind complex systems can be unveiled innovatively, including meridians and acupoint selections.22–24 Cluster analysis is one of the popular tools for exploring the underlying structure of a dataset. By allowing the algorithm to act without guidance, the data-reduction process classifies mixed domains into more-homogenous clusters based on available features. 25 Without prior training, it would group unsorted information based on similarities, patterns, and differences. 26 HCA was used to exhibit the correlations among domains and to present results visually through dendrograms.27–29 In this study, HCA helped explore the dynamic pain-induced experience and how it was affected by acupuncture.
Over 5 weeks of treatment there were reductions in pain, fatigue, anxiety, and depression, as well as improvements in physical function and participation in social roles and activities. No adverse events were reported. However, there was no progress with respect to sleep disturbance. Furthermore, the HCA results indicated dynamic changes in patterns among the PROMIS domains as the treatment progressed.
Temporal Variations in Interactions of PROMIS Domains During Acupuncture Treatment
During the course of treatment, 2 predominant clusters were identified. The first cluster comprised the domains of pain, fatigue, and emotional well-being.
Fatigue is correlated with the emotional domains of anxiety and depression, suggesting that fatigue could stem from emotional exhaustion. The stress of chronic pain has a detrimental impact on the mind–body connection. A patient with chronic musculoskeletal pain in the body may also suffer from emotional turmoil, having difficulty concentrating, feeling depressed or anxious, and that patient's judgment can also be affected. 30
Pain and fatigue are commonly observed in patients with chronic pain, 31 but the cluster analysis in this study demonstrated a dynamic relationship between them. Fatigue is associated with emotions before treatment but is linked to pain interference later. When patients seek help for acupuncture, they may suffer from both fatigue and emotional exhaustion.
Another study involving functional magnetic resonance imaging demonstrated that the brain has a specific activity reserved for pain-related cognitive or emotional factors, even at rest, emphasizing the close associations among pain and emotions and cognition. 32 In Chinese Medicine, the importance of treating Shen, or Spirit, should be considered throughout the treatment. EA on GV-20 and GB-34 is effective for treating chronic pain–induced psychiatric deficits, according to previous studies on acupuncture. 33
The second cluster encompasses physical function and participation in social roles and activities.
Within the PROMIS assessment, physical function falls under the category of physical health, while participation in social roles and activities is part of social health. The relationship between physical and social domains implies that pain-induced physical limitation will weaken one's ability to obtain satisfying family, work, and social relationships. 34 Studies have also shown that social attachment and support can help improve physical activities and pain sensation.35,36 Our study, as reflected by PROMIS scores and cluster analysis, demonstrates that patients with chronic musculoskeletal pain exhibit improved physical function and greater participation in social roles and activities after undergoing acupuncture therapy.
The clusters have shown a dynamic relationship between pain and quality of life factors in acupuncture treatment during 5-week sessions. On the one hand, they indicate that chronic musculoskeletal pain involves biologic, psychologic, and social aspects of life. On the other hand, they highlight the importance of multiple domains in the treatment. acupuncture has shown holistic improvement, but a patient-centered, and interdisciplinary approach is also necessary to optimize the effectiveness of pain treatment, taking into account the dynamic needs of patients in different stages of treatment.
Relationships Between Sleep and Other Domains
During the treatment, the sleep domain showed some interesting interactions with others. The score of sleep domain score remained high but its location shifted after treatment and became associated with different domains at different timepoints.
Sleep disturbance and musculoskeletal pain have a bidirectional relationship. 37 Before treatment, the sleep disturbance is clustered with both pain intensity and pain interference. According to the questionnaire of PROMIS-29, this means pain sensation affected patients' subjective evaluation of sleep quality, refreshment after getting up, and difficulty falling asleep. This is not uncommon in clinic. The sleep studies show that 67%–88% of patients with chronic pain have sleep complaints, 38 and 60.3% of patients with chronic musculoskeletal pain reported a non-recovering effect of sleep. 39 For patients suffering from chronic pain, it disturbs sleep continuity and quality while poor sleep further exacerbates pain, leading to the negative loop. Research has indicated that acupuncture can break this loop by reducing pain and improving sleep in patients with different conditions,40–43 but this was not found in the current study.
In the third week, the distance of sleep with pain and emotional domains expanded, and finally merged with physical function and social role and activities in the fifth week. A possible interpretation is that, as subjective pain sensation is relieved by acupuncture treatment, poor sleep quality exerts a more-negative impact on objective life function and social activity. Poor sleep has been proven to impact the capacity for physical and social performance negatively during the day. 44 The ability to perform tasks may be impaired when a patient with chronic pain is also suffering from poor-quality sleep. The remaining disorder of sleep may also prevent other factors from improving further.
These findings are a reminder to practitioners that a pain-targeted treatment plan may not be sufficient to improve sleep. Addressing sleep should be an integral part of pain management. Utilizing acupoints and other techniques to target sleep disturbances is necessary. To optimize patient outcomes, encouraging patients to adopt regular sleep habits, and have consultations for behavioral therapy may be valuable for inducing better sleep in pain recovery. 45
The findings in this study revealed the holistic effect of acupuncture in multiple domains and emphasized the necessity of treating sleep disturbance. However, 2 major limitations challenged the study's validity. First, the results of the small sample size were not representative due to the potential for selection bias and also reduced the power of the study while increasing the risk of type II errors. As such, a larger sample size with a longer treatment duration will provide more informative clues about the pattern changes in chronic musculoskeletal pain. Second, the assessment tool used in the study, the PROMIS-29, while reflective of patients' subjective and realistic needs, required additional objective processes to assess joint range of motion, joint function, strength, and pain sensations. Introducing more subjective and objective assessment tools is needed to gain a full understanding of the comprehensive and precise patterns and models of domains contributing to reducing chronic musculoskeletal pain.
CONCLUSIONS
The data collected from PROMIS-29 measurements showed a positive effect of acupuncture on domains of pain intensity, interference, fatigue, and physical function. The HCA revealed the evolving interactions between 2 clusters of pain with fatigue and emotional domains, and physical function with social domains, while both have interaction with sleep. The limitation of sample size and bias of this pilot study requires future research on the importance to adopt an interdisciplinary and holistic approach to the reduction of chronic musculoskeletal pain with dynamic needs.
Footnotes
AUTHORs' CONTRIBUTIONS
Drs. Fan and Jin were responsible for conceptualization and supervising the project, curating the data, conducting the formal analysis, and reviewing and editing the article's draft. Dr. Wang was responsible for visualization, investigation, writing the article's original draft, and reviewing and editing the final version. Drs. Wang and Jin worked together and contributed equally to the study. Dr. Sun was responsible for reviewing and editing the article's draft. Drs. Fu, Zhang, and Li were responsible for the study's methodology and validation.
AUTHOR DISCLOSURE STATEMENT
No financial conflicts of interest exist.
FUNDING INFORMATION
No funding was received for this work.