
Abstract
Background:
Trigger finger (TF; a type of stenosing tenosynovitis) is common, affecting the flexor tendons of the hand, often causing significant pain and functional impairment. Treatment can include splinting, corticosteroid injection, or surgical release. There is little published research on the role of electroacupuncture (EA) for treating TF.
Case:
After more than 1 year of pain and triggering, a 58 year-old male had locking of his left, fourth ring finger requiring painful manual reduction. EA was performed with 4–6 needles in a rectangular pattern along the radial and ulnar aspects of the A1 pulley of the fourth digit, with 10 Hz delivered in a daisy-chain formation for 45 minutes. Nodule size, frequency of triggering and locking, and severity of pain were assessed before and after 4 treatments over ∼1.5 months.
Results:
This patient's frequency of locking and severity of pain decreased significantly by 50% after his first treatment. Additional clinically significant reductions of locking, pain, and nodule-size were evident after each treatment along with substantial functional gains between visits. After his fourth treatment, he reported 100% resolution of his symptoms with no further pain or triggering. Throughout this time, he continued his usual activities.
Conclusions:
EA alone directed at the A1 pulley may be an effective treatment modality for patients with TF. The authors hypothesize that EA may reduce pain enabling a return to normal function and compression of the nodule, thus eliminating triggering. Further research evaluating the efficacy of EA for TF may help substantiate these results.
INTRODUCTION
Trigger finger (TF), or stenosing tenosynovitis, is a common cause of hand pain with a lifetime occurrence rate of 2.6% in healthy adults, 1 most commonly middle-age women, 2 and 10% in people with diabetes. 1 Most cases of TF are idiopathic. Associated medical conditions include diabetes, thyroid disease, amyloidosis, connective-tissue disorders, rheumatoid arthritis, gout, glycogen-storage diseases, acromegaly, and renal disease.2,3 TF can coexist with de Quervain's tenosynovitis and carpal tunnel syndrome. 2
The ring finger is affected most often, followed by the middle finger and thumb. 4 The main risk factor for TF is thought to be chronic mechanical overuse resulting in microtrauma from repetitive gripping activities pinching the tendon and first annular (A1) pulley (Fig. 1) between a firm surface and the corresponding metacarpophalangeal (MCP) joint leading to a thickened stenotic A1 pulley with or without thickening of the flexor tendon. 5 Some researchers question this hypothesis, finding no association with repetitive finger activities or correlations with patients' workplaces. 4 Irrespective of the mechanism, the result of the pathogenesis is that the tendon is no longer able to glide smoothly. Stage I is a painful nodule without mechanical catching. As the condition advances, the tendon can catch momentarily causing triggering (stage II) or locking (stage III, requiring passive extension to correct). Stage IV is “fixed” flexion, not passively correctible without surgery. Triggering can be preceded by pain and joint stiffness, 6 but, initially, snapping, catching, triggering, or locking can be painless.
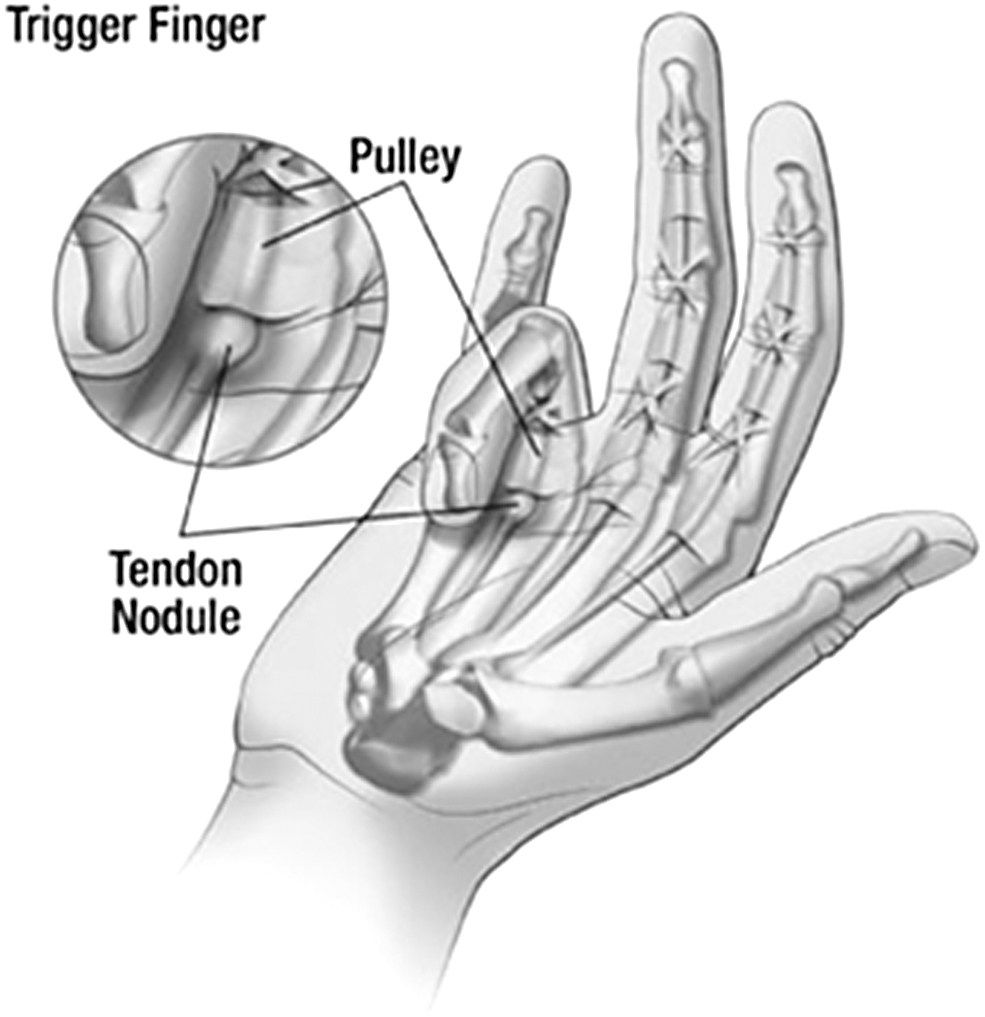
Trigger finger and A1 pulley.
Multidisciplinary consensus guidelines for managing TF suggest that splinting, corticosteroid injection, and surgery are all indicated based on timing, symptom severity, and previous therapy. 7 Spontaneous resolution is more common than previously believed; up to 52% of untreated adult TF cases resolve by 8 months after initial clinic presentation. 8 Therefore, TF may not always require medical attention.
TF is diagnosed by the patient's history and confirmed with examination demonstrating catching, triggering, or locking, with or without a palpable palmar nodule. A conservative initial approach may include observation, activity modification, splinting, oral nonsteroidal anti-inflammatory drugs (NSAIDs), or some combination.2,8,9 Corticosteroid injections are usually recommended when conservative treatment fails,10,11 although an injection at the initial clinic presentation is common. Surgical release is reserved for stubborn cases. To the current authors' knowledge, this is the first case reported in the U.S. literature that involved using electroacupuncture (EA) alone in the treatment of TF.
CASE
Mr. J is 58 years old. He tends a small herd of goats and walks 2 large dogs on a leash. Other activities in his yard necessitate repeated gripping of various tools. More than 1 year prior to presentation, he began having some pain and triggering of his left ring finger. His job requires typing, and his triggering became problematic. He identified a tender nodule and commonly had to manually release the finger (stage III), more for resumption of a full active range of motion than for pain. He did not use NSAIDs. A physical examination revealed a 0.75-cm nodule at the distal palmar skin crease of the ring finger. Locking was demonstrated; it required manual release.
Mr. J presented with a classic history and examination for TF. Conservative options were declined, as was a steroid injection. Despite the physician's lack of experience with using acupuncture for TF, this patient insisted on having acupuncture to treat his TF.
Treatment #1, Day 0
The patient had a slightly tender, well-defined palmar nodule in line with his left ring finger. A local approach was chosen. Four sterile acupuncture needles (SEIRIN® 0.2 × 30 mm) were inserted into the radial and ulnar sides of the flexor tendon ∼8-mm deep, just distal and proximal to the A1 pulley. Ten Hz was delivered in a daisy-chain formation with the anode attached to the proximal needle and the cathode attached to the distal needle on the radial side and respectively on the ulnar side of the tendon and for 45 minutes (Fig. 2). Intensity of the current was to tolerance and was increased for accommodation. After needle removal, Mr. J had no pain or triggering, which he showed by opening and closing his hand.

Electroacupuncture needle arrangement.
Treatment #2, Day 7
One week later, Mr. J reported having complete resolution of pain and triggering following the first treatment until a couple days later when he performed “a lot” of farming activities. Despite the regression, overall he estimated his pain was 50% reduced and his locking was 25% less than prior to initial treatment. He also noticed his palmar nodule was not as large nor as tender as it had been before treatment began. This was confirmed on examination. The initial treatment was repeated for 40 minutes. Afterward, he could open and close his hand quickly and frequently and said that he “would not have been able to do this before today's treatment.” While demonstrating these movements, he had no pain or triggering.
Treatment #3, Day 35
Four weeks later, despite a hiatus in treatment due to his schedule and the active use of his hands, this patient's pain and triggering remained reduced. He felt that the nodule had shrunk further, but he was now having new discomfort closer to the level of the proximal palmar crease. The nodule was smaller and not tender. The needle number and arrangement was modified to accommodate the increase in the symptomatic area: Three sets of acupuncture needles were inserted on either side of the tendon with each middle needle being level with the A1 pulley; on the radial side, the proximal and middle needle handles were crossed and clipped with the anode and the cathode was attached to a single distal needle; on the ulnar side the reverse was organized to maintain a daisy chain formation. A current of 10 Hz was delivered for 40 minutes. After the needles were removed, he was able to open and close his hand without pain or triggering.
Treatment #4, Day 49
Two weeks later, Mr. J was pain-free. The nodule was difficult to identify; there was no tenderness in the area or triggering. Treatment #3 was repeated, after which, he was asymptomatic.
Long Term Follow-Up
Twenty-three months after initial therapy with EA, there was only 1 day on which the patient had “a little bit of pain,” which resolved on the following day. As of this writing, he remains pain- and trigger-free.
DISCUSSION
Mr. J's response to EA remarkable, especially the immediate elimination of pain and triggering and how rapidly the nodule shrunk. Inoue, et al., suggests a number of effects of manual or EA that could be in play, including improved blood flow to the affected finger and decreased inflammation through modulation of humoral factors. 12 However, histopathology of TF shows fibrocartilaginous metaplasia resulting from repeated friction and compression between the flexor tendon and the corresponding inner layer of the A1 pulley without evidence of an inflammatory process. Thus, tenosynovitis is a misnomer. Indeed, chondroid metaplasia is seen in the deepest tissues adjacent to the tendons in the fiber-osseous canal of the flexor sheath, resulting in an increased volume of tissue deposition.
These noninflammatory findings are not surprising, considering that the conditions associated with TF largely involve accumulation of ground substance and extracellular matrix (e.g., diabetes, thyroid disease, and amyloidosis, among others). The favorable response to steroid injection can be explained by atrophy of the tenosynovial volume and thereby reduction in mechanical triggering in the sheath. It is possible that any approach that provides analgesia allows the patient to use the affected finger and thereby mechanically “flatten” the nodule so it does not trigger anymore. This may be the case for Mr. J, as he only received an intermediate frequency (with an initial plan to increase each subsequent visit to higher frequencies to induce the anti-inflammatory effect, not appreciating the pathophysiology at the time). Initiation was at the lowest end of the Hz range to gauge patient tolerance and, given the results, never needed to be increased.
EA for TF compares favorably to conventional conservative therapy. The mainstays of conventional therapy include rest, activity modification, splinting, and short-term NSAIDs. Oral NSAIDs are used to reduce pain during rest and splinting but do not appear to have a direct local affect. Topical NSAIDs are not effective and locally injected NSAIDs results are mixed. 11 Splinting has a high success rate if started before 6 months of symptoms and less so after 6 months of symptoms. 2 Splinting holds the finger in extension so that the nodule is maintained in the fibro-osseous canal causing it to become “squeezed” and constricted into a smaller mass resolving the triggering. A study of a custom thermoplastic metacarpal–phalangeal blocking splint showed decreased triggering symptoms in a single isolated trigger finger in 92.9% of subjects over 6–10 weeks. 2 In contrast, the current patient was symptomatic for more than 1 year, exceeding the threshold of 6 months for splinting to be effective; his symptoms responded immediately to EA, and he has remained trigger-free 23 months later, despite returning to his previous activities.
When conservative therapy fails, local corticosteroid injections are used. Steroid injections rarely lead to complications but carry the risk of fat necrosis, skin depigmentation, and spontaneous tendon rupture. Both splinting and injections have been shown to improve grip strength and reduce pain and frequency of triggering, but in 1 study, while patients were more satisfied with the corticosteroid treatments, there was a greater rate of symptom recurrence after 6 months. 3 In the current case, the patient has not had any recurrence, and EA carries only minor risks of local bruising.
There are only a handful of reports in the United States on treating TF with acupuncture, but none used EA alone, and patients received multiple modalities, such as osteopathic manipulation. 13 Outside of the United States, use of EA has been reported but also involved cotreatment with other modalities.14,15
CONCLUSIONS
EA may be a more-convenient therapy for TF as opposed to wearing a splint for months and EA may also be safer alternative to corticosteroid injections. Further study is warranted.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No financial conflicts of interest exist.
FUNDING INFORMATION
No funding was provided for work on this case report.