
Abstract

C
According to existing literature, overactive pelvic-floor muscles may often lead to coccydynia, causing myofascial pain in the pelvic-floor area. 2 Myofascial pain syndrome (MPS) is a persistent ailment that emanates from myofascial trigger points (MTrPs) present in skeletal muscles, inducing stiffness, weakness, and localized or referred pain. Despite being a common phenomenon in clinical practice, MPS is frequently misdiagnosed or underdiagnosed. 3 An important consideration is that coccyx pain may not solely originate from an overactive pelvic floor. MTrPs located in other muscles in the surrounding area, such as the gluteus maximus muscle (GM), have the potential to cause pain that radiates toward the coccyx and may play a crucial role in the etiology of coccydynia (Fig. 1). 4
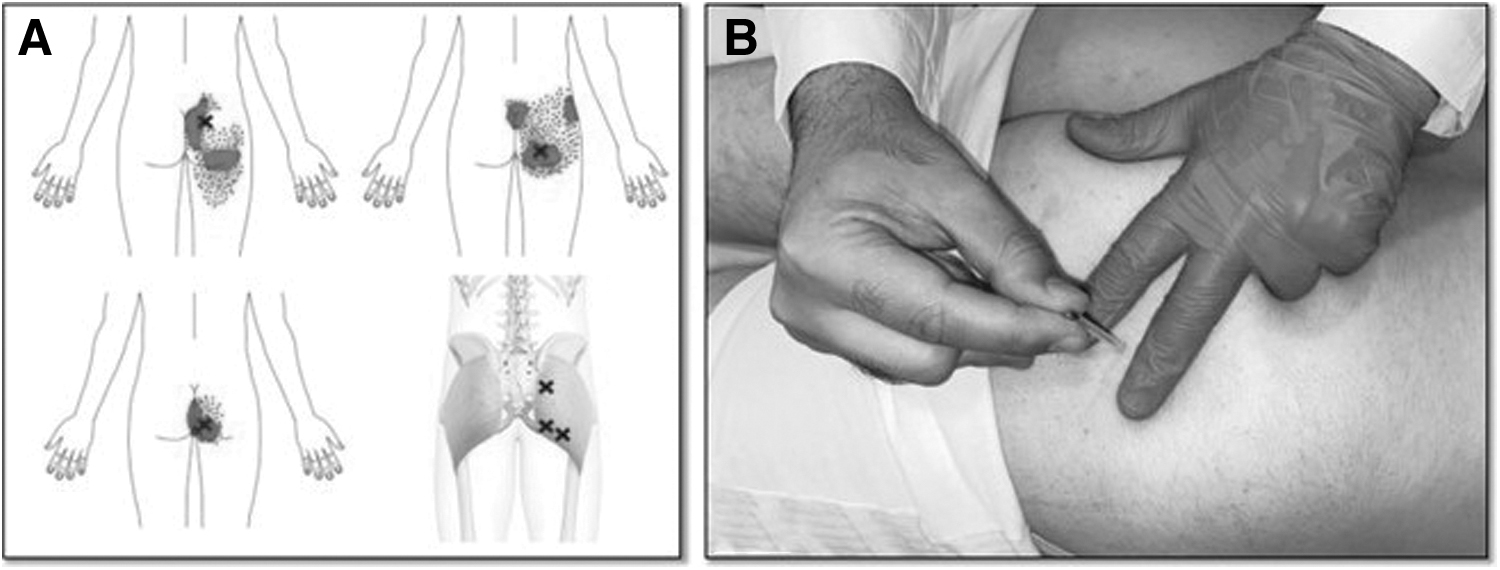
The GM covers the posterior pelvis and has a complex biomechanical role in the hip, knee, and lumbopelvic region. The GM stabilizes the pelvis on the femur and propels the body forward during ambulation. MTrPs in this muscle can be activated by certain activities, leading to pain in the buttock region that may be misdiagnosed as other conditions such as sacroiliac-joint dysfunction, trochanteric bursitis, or high hamstring-strain symptoms. Additionally, MTrPs of this muscle can refer pain to the coccyx area and cause coccydynia (Fig. 1A). 4
Dry needling (DN) is a minimally invasive and cost-effective approach for relieving muscle tension and pain by targeting MTrPs. This technique can be used alone or in combination with other therapies to treat various musculoskeletal conditions effectively. DN can be applied using blind or ultrasound-guided techniques and can also be applied to the MTrPs in the GM, making DN a promising treatment option for patients with coccydynia. 5
DN should be performed on the patient in a prone position with the knee slightly flexed. The technique involves using flat palpation to insert a needle into the skin at a 45° angle in a lateral-to-medial direction (Fig. 1B). A 0.30 m × 50 m needle should be used. Precautions should be taken to avoid the proximity of the sciatic nerve, inferior gluteal nerve, and trochanteric bursa. 5
We suggest that MTrPs of the GM should be taken into account during evaluation of patients with coccydynia. It is hypothesized that inclusion of the MTrPs of this muscle in treatment protocols may have a positive effect on patient outcomes.
Work for this letter was performed at the Üsküdar State Hospital, Üsküdar, İstanbul, Turkey. Dr. Temel was responsible for conceptualization, methodology, software used, data curation, and writing the original draft. Dr. Bagcier visualized and supervised the project; worked with the software; investigated and validated the technique; and reviewed and edited the final letter.