
Abstract
Introduction:
Integrating traditional Chinese medicine with Western medicine has been extensively studied in managing respiratory disease. Therefore, in this study, we aimed to examine interferon point alteration (IPA) and its association with disease severity in patients with COVID-19.
Methods:
This cross-sectional study was conducted on patients hospitalized due to COVID-19 with lung involvement. The control group consisted of patients hospitalized with a diagnosis other than COVID-19. The prevalence of IPA was compared between patients with and without COVID-19. Clinical and laboratory findings were compared in patients with and without IPA.
Results:
A total of 126 participants, with a mean (SD) age of 57.2 (16.4) years, were included in this study. 54.8% of participants were men. There was a significant difference between patients with and without COVID-19 regarding the frequency of IPA (p = 0.045). No significant differences were observed between variables in patients with and without IPA (p ≥ 0.05). The only variable that could significantly predict the IPA in COVID-19 patients was the severity score of lung involvement in HRCT (OR: 5.32, 95% CI: 1.08–26.05, p = 0.039). IPA showed a sensitivity and specificity of 80.9% and 34.9% in identifying COVID-19 patients, respectively.
Conclusion:
Our study found a significant association between IPAs and the severity of lung involvement in hospitalized COVID-19 patients and a significant association of COVID-19 with IPAs.
INTRODUCTION
COVID-19 is an infectious respiratory disease caused by severe acute respiratory syndrome coronavirus 2.1–3 COVID-19 infection can impact multiple organs throughout the body, leading to varying severity and clinical symptoms.4,5
Despite global vaccination efforts and the development of herd immunity, severe cases and resulting mortality from COVID-19 continue to occur, particularly among high-risk populations.6,7 In addition, mild cases of the disease can still present bothersome symptoms and contribute to virus transmission.5,8 Numerous pharmacological and nonpharmacological treatment approaches have been evaluated for managing COVID-19 patients.9–11 The treatment of COVID-19 remains an active area of research, with alternative medicine-based approaches. 12
The integration of traditional Chinese medicine (TCM) with Western medicine has demonstrated favorable therapeutic outcomes and has been extensively studied in treating and managing respiratory disease complications. 13 The World Health Organization highly appreciates China’s high cure rate and low mortality with COVID-19, attributed to the application of TCM.14,15
Some studies have indicated that TCM and Acupuncture can effectively treat COVID-19.16–19
Auricular causative diagnosis (ACD) is a pillar of TCM that provides objective visualization of organ status and aids in functional diagnosis. In a study by Volf et al. on 34 severe COVID-19 patients, similar auricular visual markers were found in specific areas of their external ear, which were absent in healthy individuals. 20 This specific point is referred to as the interferon point (Fig. 1), an area in the corner of the supratragic notch.
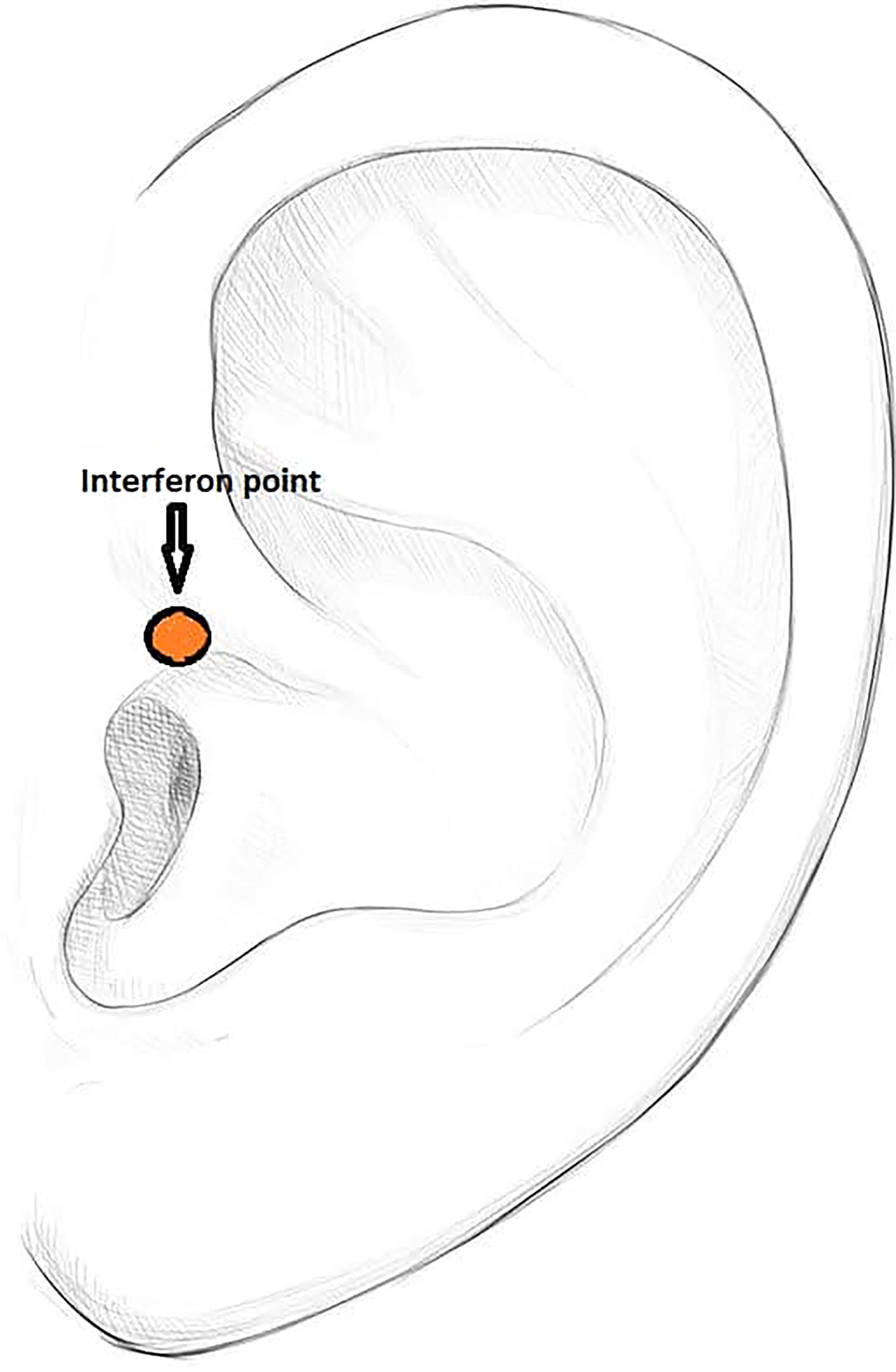
The anatomical location of the interferon point.
METHODS
Study Design and Patients
This cross-sectional study was conducted between 2021 and 2023 on patients admitted to Al-Zahra Hospital in Isfahan, Iran. The inclusion criteria for the case group patients included age over 18, hospitalization due to COVID-19 diagnosed with positive reverse transcriptase polymerase chain reaction (RT-PCR) or confirmed lung involvement in high-resolution computed tomography (HRCT) (ground-glass opacity) as determined by a radiologist, and clinical symptoms of COVID-19. The control group consisted of patients admitted to different wards, excluding the COVID-19 or respiratory ward. These patients tested negative for PCR, showed no clinical or imaging evidence of COVID-19, and consented to participate. Exclusion criteria included abnormal ear shape and ear infections.
Data Collection
After selecting the patients and obtaining written informed consent from the patient or their legal guardian (in the case of patients under mechanical ventilation), photographs of both ears, including the interferon point area, were taken. The patient’s information, including demographic characteristics, including age and gender, as well as laboratory and clinical findings, including C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and saturation of peripheral oxygen (SPO2), were recorded. Afterward, the photos lacking subject names or identifiable characteristics were reviewed by a third physician to evaluate the shape of the interferon point. According to the study of Volf et al. 20 , unusual auricular conditions include edema in the tragus, supratragus notch, and ascending branch of the helix was considered interferon point alteration (IPA). Figure 2 shows the IPA in different ages and sex.

Altered interferon against unaltered interference point. 1, 2, 3: Normal interferon point. 4, 5, 6: Interferon point alteration.
A scoring system was implemented to assess COVID-19 severity using HRCT. The scoring criteria were as follows: a score of 1 was assigned for lung involvement of <20%, a score of 2 for involvement between 20% and 50%, and a score of 3 for involvement >50%.
Data Analysis
Data analysis was done using IBM SPSS 28. After using the Kolmogorov–Smirnov test, the median [IQR] and mean (SD) were used to describe continuous variables, and the number (%) was used to describe categorical variables. To compare the studied variables between patients with and without COVID-19, as well as patients with and without IPA, independent samples t-test, chi-square, and Kruskal–Wallis tests were employed. To investigate the predictive factors for the occurrence of IPA in COVID-19 patients, we conducted the following analyses: First, we utilized receiver operating characteristic curve analysis to determine the optimal cutoff values for the quantitative variables associated with IPA by comparing COVID-19 patients with and without IPA. Subsequently, we performed a multivariate binary logistic regression analysis to calculate the relationship between these variables and the occurrence of IPA in COVID-19 patients, using the identified cutoff values. A p < 0.05 was considered statistically significant (two-sided).
RESULTS
A total of 126 participants, with a mean (SD) age of 57.2 (16.4) years, were included in this study. Sixty-nine (54.8%) of participants were men. In the positive COVID-19 group, there were 63 individuals with mean (SD) age of 57.6 (15.0) years, and 35 (55.6%) of them were men. The negative COVID-19 group consisted of 63 individuals, with a mean (SD) age of 56.9 (17.7) years, of which 34 (54%) were mean (Table 1).
Comparison Between Patients with and Without COVID-19
Chi-square.
Independent t-test.
According to Table 1, no significant differences were found between the two groups regarding age and gender, indicating that the two groups were homogeneous regarding age and gender. However, there was a significant difference between the two groups regarding the frequency distribution of IPA (p = 0.045), suggesting an association between IPA and COVID-19 infection. Demographic, clinical, and laboratory findings were compared based on the presence of IPA in patients with COVID-19 (Table 2). Although no significant differences were observed but patients with IPA demonstrated higher mean (SD) age, severity score of HRCT, and ESR compared to those without IPA.
Comparison of Studied Variables Between COVID-19 Patients with and Without IPA
Chi-square.
Independent t-test.
Kruskal–Wallis.
CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HRCT, high-resolution computed tomography; IPA, interferon point alteration; IQR, interquartile range; SD, standard deviation; SPO2, saturation of peripheral oxygen.
Conversely, patients without IPA had a higher mean (SD) CRP level. In addition, the median (IQR) duration from disease onset and SPO2 level (with oxygen therapy) were higher in patients with IPA.
In contrast, the median (IQR) SPO2 level (without oxygen therapy) was higher in the patients without IPA. Table 3 presents the cutoff values obtained for predicting the incidence of IPA in patients with COVID-19 using the studied variables. However, none of the obtained cutoffs were statistically significant (p ≥ 0.05), suggesting that their discriminatory power may be limited. The cutoff for CRP was 54 mg/L (AUC = 0.618, p = 0.208), ESR was 22 mg/L (AUC = 0.613, p = 0.096), and the time elapsed since the onset of the disease was 3.5 days (AUC = 0.596, p = 0.094).
Cutoff Values for Variables Predicting IPA in Patients with COVID-19
AUC, area under the curve; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; IPA, interferon point alteration; HRCT, high-resolution computed tomography; SPO2, saturation of peripheral oxygen.
Table 4 presents the results of a multivariate analysis aimed at identifying variables that predict the occurrence of IPA in patients with COVID-19, using the cutoff values established in Table 3. Multivariate analysis indicated the only variable that can significantly predict the IPA in patients with COVID-19 to be the severity score of lung involvement in HRCT (OR: 5.32, 95% CI: 1.08–26.05, p = 0.039).
Multivariate Analysis of Predictive Variables for IPA in COVID-19 Patients
CI, confidence interval; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HRCT, high-resolution computed tomography; IPA, interferon point alteration; OR, odds ratio; SPO2, saturation of peripheral oxygen.
IPA showed a sensitivity, specificity, and accuracy of 80.95 (95% CI: 69.09–89.75), 34.9 (95% CI: 23.34–47.97), and 57.94% (95% CI: 48.82–66.67) in identifying COVID-19 patients, respectively.
DISCUSSION
Numerous studies have demonstrated that TCM is effective in improving clinical symptoms and the quality of life. 21 In emergent situations like the COVID-19 pandemic, where we face limited resources and a lack of knowledge about the disease, exploring and investigating alternative medicine such as TCM becomes crucial. TCM offers a variety of diagnostic techniques, such as tongue diagnosis and pulse diagnosis, to help diagnose the diseases or involved organs.22,23 There are various techniques, such as inspection, pressure pain test, and electrical skin resistance test, for detecting auricular points (APs). Among these techniques, the inspection usually efficiently identifies APs.24,25 According to the study conducted by Volf et al., based on the inspection method, patients with severe COVID-19 may exhibit a specific auricular visual marker known as interferon point. 20 Interferon point, previously identified (Fig. 1) by Frank Bahr, can possess properties that strengthen the immune system against viral infections, particularly in children, by alleviating symptoms such as fever and diarrhea.26,27 Stimulating interferon point may hasten the recovery process in COVID-19 patients, diminishing the necessity for mechanical ventilation and enabling quicker extubation, thus promoting a return to normal breathing.
However, controlled clinical trials and additional research are essential to validate these findings and confirm the effectiveness of this auricular point. 17 While observations in Volf et al.’s study are preliminary, the findings are intriguing and may hold clinical significance. They raise questions about the potential of the interferon point serving as a visible anatomical marker easily identifiable in hospitalized COVID-19 patients. 20 Based on our findings, we employed the inspection method in our study to identify changes in the interferon point among hospitalized COVID-19 patients. In our study, 81% of COVID-19 patients and 65.1% of non-COVID-19 patients exhibited alteration in the interferon point. Although not statistically significant, the frequency of IPA was higher in COVID-19 patients compared to other patients. It is important to note that our study differed from that conducted by Volf et al., which focused on patients with severe forms of COVID-19 admitted to the intensive care unit (ICU). On the contrary, our study included patients hospitalized in both the ward and ICU with varying degrees of severity. This distinction serves as both a limitation and a strength of our study.
This aspect is a notable strength of our study as it encompasses a broad spectrum of disease severities, not just limited to severe patients. We also aimed to explore the association between the disease severity (based on imaging and laboratory findings) and the presence of auricular visual marker. 20 Our results revealed a significant association between the presence of the IPA and the severity of lung involvement in HRCT scans.
It is worth mentioning that while IPA were commonly detected in COVID-19 patients, a substantial number of individuals in the control group also displayed these findings. This could be linked to the severity of their illness or the presence of acute or chronic inflammation. In other words, IPA were sensitive findings in COVID-19 patients but showed poor specificity. Therefore, future studies examining interferon point changes in patients with different severities of disease, inflammation, and infection other than those with COVID-19 would be preferable.
Although our study had certain limitations, some previously mentioned, it is worth noting additional restrictions such as the small sample size, which may have impacted the statistical significance of several ratios investigated. Moreover, the severity of the disease, particularly among non-COVID-19 patients, was not recorded, potentially acting as a confounding variable. It is plausible that the positive cases observed in the non-COVID-19 group are associated with disease severity, and the proportion of critical patients in the non-COVID-19 group may differ from the other group, thereby influencing the study results. Considering that IPA were seen in a significant percentage of patients in the control group, the availability of ESR and CRP test results for these patients could help identify the possible etiologies of this finding. However, this limitation still needed to be solved due to budget constraints and the need for interventions such as taking blood samples to check these markers in some control group patients. Another limitation of our study arose from the heterogeneity of diseases within the control group. Nevertheless, due to restrictions in previous studies and uncertainty about the exact causes of IPA, we endeavored to attain a more comprehensive understanding of this clinical observation by refraining from confining the control group to a particular disease category.
Another unanswered question is whether the change in electrical charge in the ear area causes swelling and whether it is possible to find a change in electrical resistance or electrical charge before IPA?
Maybe some COVID patients who don’t have interferon edema show a change in electrical resistance.
The next studies with more samples and with different methods, for example, comparing two groups of COVID-19 and completely healthy patients, as well as using other diagnostic methods, such as pressure sensitivity or electrical resistance of the interferon point, will produce more accurate results.
Despite these limitations, our study also possessed strengths. Including a control group among the patients investigated enhances the reliability of our findings. In addition, we examined patients with varying degrees of disease severity, extending beyond severe cases.
CONCLUSION
Our study found a significant association between IPA and the severity of lung involvement in hospitalized COVID-19 patients and a significant association of COVID-19 with IPA. However, the study had limitations, including a small sample size and the absence of recorded disease severity among non-Covid-19 patients. Given the observation of IPA in a high percentage of hospitalized patients for diagnosis other than COVID-19, we recommend investigating IPA in non-COVID-19 patients with various severities of disease, inflammation levels, and infections in future studies. Due to the low specificity of IPA in COVID-19 patients, future studies should better investigate these alterations in non-COVID-19 patients with varying diseases and inflammation levels.
Footnotes
AUTHOR’S CONTRIBUTIONS
All authors contributed to the initial draft and final approval of the work for publication. All authors attest to the validity and integrity of data, and the whole process of the research
M.R.H.: Conceptualization, project administration, supervision, and writing—original draft preparation. M.S.: Data analysis, methodology, validation, and supervision. A.G.: Data collection and curation. M.H.S.: Writing—review and editing. S.F.: Data collection, curation, and software. S.M.H.: Conceptualization and data analysis.
ETHICAL CONSIDERATIONS
The present study was approved by the Research Ethics Committee of Isfahan University Medical Sciences (Ethical Code: IR.MUI.MED.REC.1400.232). Written informed consent was obtained from all participants to participate in the study, and adherence to the Helsinki Ethics Statement and its latest amendments was followed at all stages of the study.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.