
Abstract
Background:
Acupuncture enhances the endogenous analgesic system and reduces pain. However, its effect is not constant, and it has been reported that it varies depending on the endogenous analgesic system and spinal cord response. Therefore, we investigated whether there was a difference in the changes in pain thresholds in muscle and skin tissue due to differences in the spinal cord response when electroacupuncture was applied to healthy participants whose endogenous analgesic system works normally.
Methods:
We included 29 healthy volunteers who gave consent to participate. The participants underwent psychological evaluations, pain thresholds assessment for muscle and skin tissue, temporal summation of pain (TSP), and conditioned pain modulation (CPM). The participants subsequently received 30 min of acupuncture (scalp + three limbs) as an intervention, and the pain thresholds of muscle and skin tissue were measured before, 30 and 60 min after intervention. Note that participants were grouped by TSP based on high and low spinal cord response.
Results:
Analysis of participants grouped by spinal cord response showed no difference in CPM between high and low groups prior to the intervention, indicating that the endogenous analgesic systems were the same for the two groups. However, electroacupuncture intervention affected changes in muscle pain threshold (p = 0.03). A significant difference in pain threshold was noted in the high group, 60 min after intervention (p = 0.04).
Conclusion:
When electroacupuncture is applied to healthy participants, those with higher spinal cord response may have higher muscle pain threshold.
INTRODUCTION
Acupuncture has been shown to be effective in treating pain disorders, such as low back pain.1–4 Acupuncture is thought to be effective for pain disorders because acupuncture applied to the local area of pain improves peripheral analgesia through adenosine and peripheral opioids,5,6 along with increased blood flow. 7 In contrast, acupuncture applied to areas other than the local area of pain (remote areas) can enhance gate control 8 and the endogenous analgesic system.9,10 The effectiveness of acupuncture for chronic pain such as fibromyalgia has recently been demonstrated, 11 and it has been reported that the administration of electroacupuncture to the extremities (remote areas) enhances the endogenous analgesic mechanism and reduces pain. 12 Although there have been numerous reports on pain reduction by acupuncture in remote areas, the effect is not constant. 13 The reported factors include spinal cord hypersensitization and reduction of the descending pain inhibitory system due to aging and prolonged pain.14,15 Specifically, the involvement of N-methyl-d-aspartate (NMDA) receptors, which transmit excessive sensory information to the brain, has been implicated in causing spinal cord hypersensitivity. 16 Moreover, regarding the attenuation of the endogenous analgesic system, it has been reported that chronic stress, 17 hyperactivity of the amygdala involved in negative emotions, 18 and decreased function of the dorsolateral prefrontal cortex (DLPFC)19,20 are possible causes. In fact, changes in pain transmission mechanisms to the spinal cord and brain, and the endogenous analgesic system are characteristic of chronic pain patients 21 and have been suggested to attenuate the analgesic effects of acupuncture. 22 However, it remains unclear whether such changes are also observed in healthy participants.
In contrast, quantitative sensory testing (QST), including conditioned pain modulation (CPM) and temporal summation of pain (TSP), has recently made it possible to assess the function of the endogenous analgesic system and the extent of spinal cord responses related to ascending neural pathways.21,23,24 CPM refers to the phenomenon of diffuse noxious inhibitory control, in which nociceptive stimuli suppress pain in humans.24,25 TSP is a phenomenon in which repeated stimulation at 0.3 Hz causes windup in the spinal cord via C fibers in afferent nerves and progressive increase in pain perception and is considered to be one of the methods for expressing the state of the endogenous analgesia system and spinal cord responses. 26 Therefore, QST measurements are considered to provide information on the function of the endogenous analgesic system and spinal cord response.
We aimed to determine the relationship between the condition of the spinal cord associated with ascending neural pathways and efficacy of electroacupuncture. Therefore, we investigated whether the spinal cord responsiveness, as indicated by TSP, affects the changes in the pain thresholds of each tissue induced by electroacupuncture in healthy volunteers, in whom the endogenous analgesic system is presumed to be working normally.
MATERIALS AND METHODS
Participants
Twenty-nine students (18 males and 11 females; mean age, 22.1 ± 2.8 years) were selected from the Meiji University of International Medicine after the purpose of this study and observance of privacy protection were fully explained orally and in writing. Their written consent to participate was obtained. The exclusion criteria are as follows: (1) Japanese version of the Pain Catastrophizing Scale (PCS), which is thought to influence the endogenous analgesic system, with a score ≥30 points or higher and strong catastrophic thinking; (2) Japanese version of the Hospital Anxiety and Depression Scale (HADS) with a score ≥11 points or higher in each item and strong depression and anxiety; (3) presence of acute pain, use of analgesic drugs within 24 h, or use of over-the-counter cold medications; (4) history of psychiatric or neurological disorders; and (5) body mass index 18.5≤ or >25 kg/m2. This study was approved by the Ethics Committee of the Meiji University of International Medical Science (approval number: 2022-007).
Psychological Assessment
For psychological evaluation of research subjects, catastrophic thinking was evaluated using the Japanese version (PCS), 27 and anxiety and depression were evaluated using the Japanese version (HADS). 28
Catastrophic thinking was assessed using the PCS. 27 The PCS comprises 13 questions on rumination, magnification, and helplessness and is rated on a scale of 0–4. Of note, a score of ≥30/52 was considered as a strong catastrophic thought.
Anxiety and depression were assessed using the HADS. 28 There were seven questions on anxiety and seven questions on depression, with a score of ≥11/21 for each item indicating high levels of depression and anxiety.
TSP
As a preliminary step in TSP measurement, the thermal pain threshold was measured using a thermal pain meter (UDH-104, Unique Medical, Japan) at the center of the thenar eminence of the participant’s nondominant hand. Thereafter, based on the temperature of the thermal pain threshold, the temperature at which the pain intensity of each subject was 20–40 mm on the Visual Analog Scale (VAS) was identified, and this temperature was used for TSP measurement. For TSP, the probe of the thermometer with the aforementioned temperature setting was contacted 10 times at 0.3 Hz interval to the center of the thenar eminence of the nondominant hand, and stimulation sensation was confirmed by VAS. The TSP value was subsequently calculated by subtracting the initial stimulation sensation from the 10th stimulation sensation. Moreover, after the experiment was completed, the participants were grouped into a high group, comprising those with a TSP value of 32.1 mm or higher, and a low group, comprising those with a TSP value of 32.0 mm or lower, to previous studies, 29 to compare the analgesic effect of electroacupuncture application.
CPM
As a preliminary step in CPM, a thermal pain threshold equivalent to 50 mm was measured using a thermal pain meter (UDH-104, Unique Medical, Japan) on the participant’s nondominant upper arm as a test stimulus. The CPM was measured using VAS for stimulus sensation after 10 s when the test stimulus was simultaneously applied, while the participant’s dominant hand was immersed in cold water at 10°C as the conditioned stimulus. The CPM effect was defined as follows: CPM = [(VAS during conditioned stimuli)/(VAS of test stimuli only) − 1] × 100, expressed as an arbitrary value (AU).
Intervention
Intervention comprised simultaneous stimulation of the extremities and head, which has been shown to be effective in patients with treatment-resistant chronic pain. 24 Specifically, electroacupuncture was applied to the participant’s dominant forearm (LI10), between the base of the thumb and index finger (LI4), to both lower extremities (ST36, GB34), and to the head (ST8) for 30 min, using an Ohm Pulser LFP-4000A (made by Zen-Ren, Japan). The depth of penetration was 10–20 mm, and stimulation frequency was 4 Hz for the upper and lower extremities and 100 Hz for the head. Leads were connected between LI10 and LI4, ST36 and GB34, and ST8 on both left and right sides. Stimulus intensity was set to a level at which the participants felt the stimulus firmly and comfortably. The needles were 0.18 × 40 mm in dimensions for the upper and lower extremities and stainless steel and 0.20 × 50 mm in dimensions (Seirin, Japan) for the head.
Measurement of Pain Threshold
Pain thresholds were measured using a pulse algometer (UPA-201, UNIQUE MEDICAL, Japan) to measure skin and muscle thresholds. For the measurement, a 0.18 × 40 mm insulated needle (Mitsuba, Japan) was inserted under the skin and into the muscle of the nondominant forearm (5 cm from the lateral epicondyle of the humerus and on the brachioradialis muscle) using an ultrasound system (Nippon Sigmax, Japan). Power was gradually increased, the switch was stopped when the patient experienced pain, and the pain threshold was measured. Measurements were performed twice, and the average value was taken as the representative value. Measurements were taken before and at 30 and 60 min after intervention. Given the potential influence of unconscious bias from research collaborators on pain threshold measurements, we conducted the study with comprehensive verification from both objective and subjective perspectives.
Experimental Procedure
All study participants provided informed consent for participation, and the same pain thresholds, TSP, and CPM measurements in the main experiment were also taken during the training session, with the former being conducted on a different day. After psychological evaluation (PCS and HADS), the pain thresholds of each tissue, TSP, and CPM were measured. Measurements were performed by a single researcher. Intervention comprised electroacupuncture in the supine position for 30 min, and pain thresholds were measured 30 and 60 min after intervention. The electroacupuncture interventions were performed by acupuncturists with at least five years of national certification. After experiment, those with a high TSP were divided into two groups—the high and low groups—and the pain thresholds of each tissue were compared (Fig. 1).
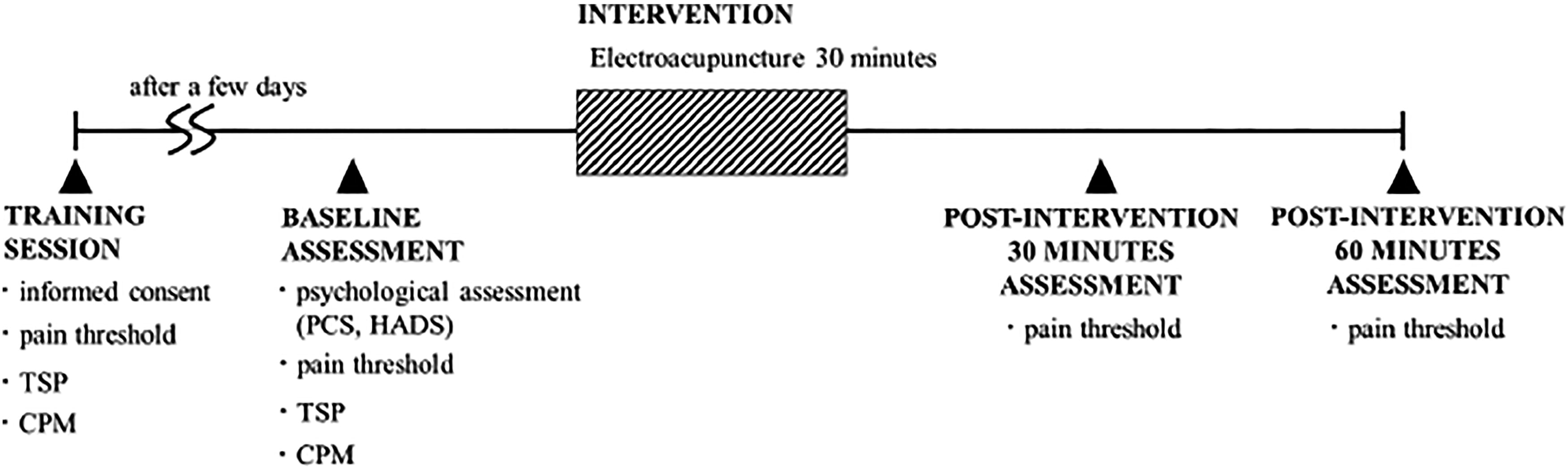
Trial procedure. Figure shows the study protocol. A training session was conducted a few days before the start of the study to obtain informed consent, pain thresholds, TSP, CPM, and other training periods. On the day of the study, following psychological evaluation (PCS and HADS) and measurement of the pain threshold of each tissue and TS and CPM of the study subjects, acupuncture was applied (4 Hz to three limbs [LI4, LI10, ST36, and GB24] and 100 Hz to ST8) for 30 min. The pain thresholds of each tissue were measured again 30 and 60 min after the end of acupuncture application. CPM, conditioned pain modulation; HADS, Hospital Anxiety and Depression Scale; PCS, Pain Catastrophizing Scale; TSP, temporal summation.
Statistical Analysis
Values are expressed as mean (±standard deviation [SD]), and the amount of change in pain threshold before and after intervention was analyzed. IBM SPSS Statistics version 25 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. A two-way analysis of variance was used for group comparisons of pain thresholds, and the post hoc Bonferroni test was used when a statistically significant interaction was indicated. An independent t-test was used for group comparisons of basic information. A p-value <0.05 was deemed statistically significant.
RESULTS
Participants Characteristics
Of these 29 participants, 24 did not meet the exclusion criteria and completed the study. Of the five excluded participants, one was excluded because of PCS scores, three because of medication use, and one because of failure to complete the study. The mean age of the 24 participants was 22.17 (±2.97) years, mean HADS score was 6.96 (±4.40) points, mean PCS score was 10.71 (±10.27) points, mean TSP was 29.77 (±16.76) mm, mean CPM was 69.68 (±33.22) AU, mean baseline skin pain threshold was 1.07 (±0.57) mA, and the mean muscle pain threshold was 2.96 (±1.35) mA. The high and low groups comprised 10 and 14 participants, respectively. There were no significant differences in age, psychological factors (HADS and PCS), endogenous analgesic mechanisms (CPM), or baseline skin and muscle pain thresholds between groups (Table 1).
Demographic Characteristics of Each Group
p < 0.01 in the comparison between high group and low group.
High group shows a high TSP, low group shows a low TSP. Data are presented as numbers or mean (standard deviation).
AU, arbitrary value; CPM, conditioned pain modulation; HADS, Hospital Anxiety and Depression Scale; PCS, Pain Catastrophizing Scale; TSP, temporal summation.
Moreover, the intensity of electroacupuncture was determined by the participants’ sensations, and no participant exhibited an extremely different stimulation intensity in this study.
Analgesic Effect of Acupuncture
Because there was a large variation in the pain thresholds of each tissue before intervention, the pain threshold was shown as the amount of change before and after intervention.
Effects on Skin Pain Threshold
The skin pain threshold of the high group was 0.38 (±1.07) mA 30 min after the intervention and 0.80 (± 1.23) mA 60 min after the intervention, whereas that of the low group was 0.04 (± 0.48) mA 30 min after the intervention and 0.14 (±0.32) mA 60 min after the intervention (Fig. 2). No interaction effects in skin pain thresholds over time were observed between the high and low groups (p = 0.12, η2 = 0.09). The needle insertion depth was approximately 2 mm for all participants, as measured using an ultrasound device.

Skin pain thresholds at over times for each group. The figure shows the change over time of the skin pain thresholds of the high TSP group (■) and low-TSP group (▲). The vertical axis represents the skin threshold, and the horizontal axis represents the time course. Analysis revealed no interaction effects in skin pain threshold over time between the high and low-TSP groups (p = 0.12; η2 = 0.09; two-way analysis of variance). Data are presented as mean (standard deviation). The high group shows a high TSP; the low group shows a low TSP.
Effects on Muscle Pain Threshold
The muscle pain threshold of the high group was 1.05 (±1.43) mA 30 min after the intervention and 1.14 (±1.19) mA 60 min after the intervention, while the muscle pain threshold of the low group was 0.24 (±0.71) mA 30 min after the intervention and −0.03 (±1.00) mA 60 min after the intervention (Fig. 3). Interaction effects in muscle pain thresholds over time in the high and low groups were identified between both groups (p = 0.01, η2 = 0.14). Comparing the main effects of the within-group pain thresholds, a significant difference was found in the high group before and 60 min after the intervention (p = 0.04), while no significant difference was found in the low group (p = 1.00). The needles were approximately 4–5 mm deep in all participants, as measured using an ultrasound device.
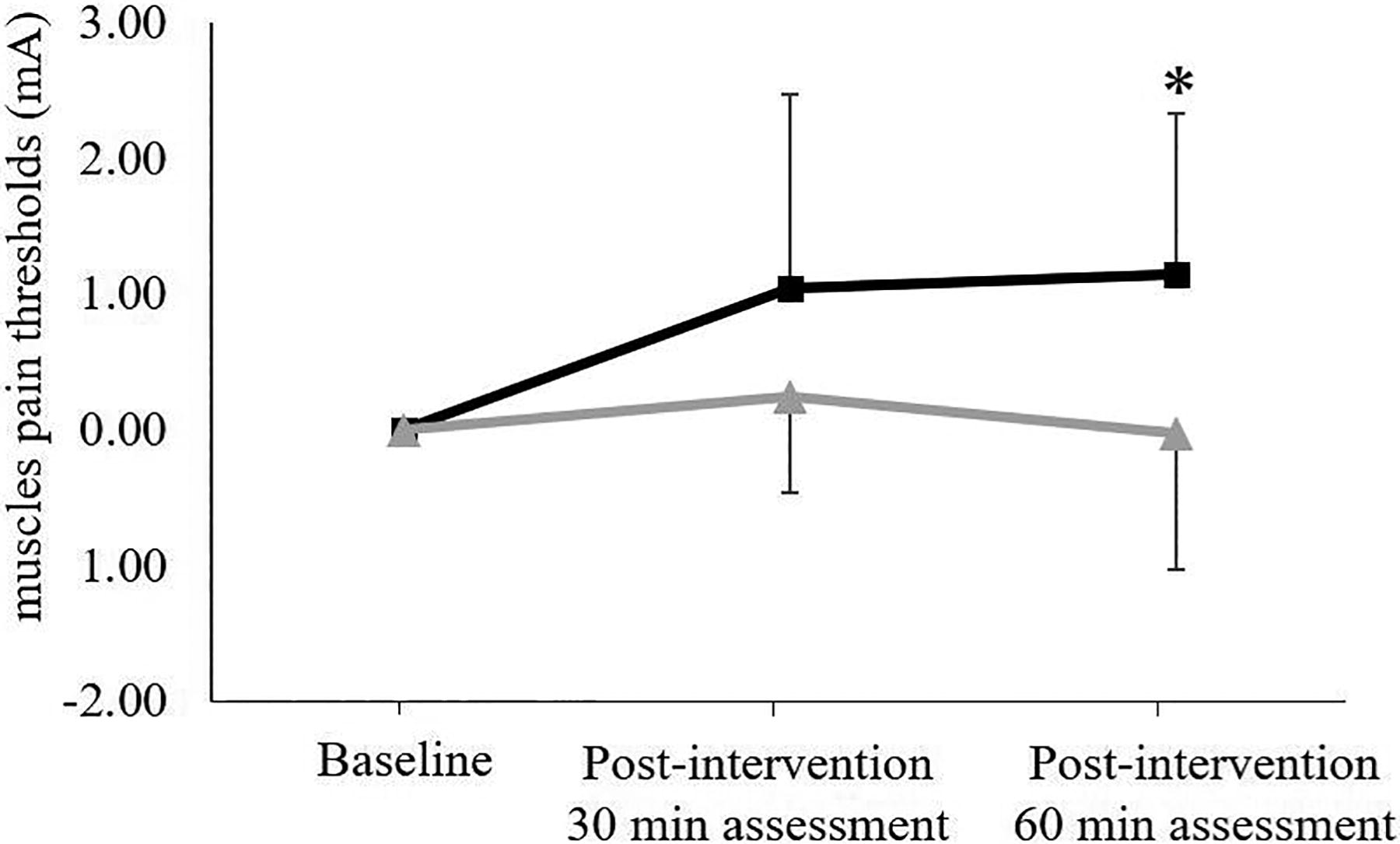
Muscle pain thresholds over time for each group. *p < 0.05 in the baseline and other measurements. The figure shows the change over time of the muscle pain thresholds of the high TSP group (■) and low-TSP group (▲). The vertical axis represents the skin threshold, and the horizontal axis represents the time course. There were interaction effects in the muscle pain thresholds over time between the high- and low-TSP groups (p = 0.03, η2 = 0.14, two-way analysis of variance). There was also main effect between baseline and 60 minutes after the intervention in the within-group comparison of the high group (p = 0.04, Bonferroni test). Data are presented as mean (standard deviation). The high group shows a high TSP, and the low group shows a low TSP.
DISCUSSION
In this study, we investigated how spinal cord responses in healthy participants affect the change in pain threshold induced by electroacupuncture using TSP. These results suggested that pain threshold alteration caused by electroacupuncture may differ depending on the spinal cord response to TSP.
TSP and Pain Threshold
TSP is a reaction in the spinal cord windup phenomenon in which glutamate and substance P are released from C fibers and is thought to reflect the windup phenomenon, in which the enhancement of NK1 receptors causes a gradual and progressive increase in pain as glutamate binds to NMDA receptors.26,30 In recent years, TSP has been extensively used in studies on pain, and it has been reported that TSP may be a predictor of chronic postoperative pain after total knee arthroplasty in patients with knee osteoarthritis. This is also associated with the occurrence of acute postoperative pain in thoracotomy patients, suggesting that higher TSP results in higher postoperative pain scores and that the spinal cord enhancement response indicated by TSP may play a significant role in the development of chronic pain.31,32 Other findings included the fact that oral administration of the opioid drug oxycodone decreases TSP in healthy participants, while CPM remains unaffected. 33 In a study examining the effects of acupuncture analgesia in healthy participants, TSP was lower in the electroacupuncture group than in the sham group after 24 h, suggesting the presence of endogenous opioid. 34 Thus, TSP has been used in various pain studies. The spinal cord response exhibited by TSP is thought to influence the chronicity of pain, and its reactivity is more influenced by opioids than by serotonin or noradrenaline, which are endogenous analgesic systems. In contrast, TSP has been reported to be more enhanced in patients with chronic pain than in healthy participants, but it is known that TSP also occurs in healthy participants, albeit to a lesser degree.21,26 Considering that the participants in this study had no chronic pain, PCS and HADS were within the normal range, and CPM, an indicator of endogenous analgesia, was within the normal range, it is highly likely that the spinal condition indicated by TSP was involved in the change in pain threshold in the present study. In a previous study, it has been reported that, in healthy participants, the periaqueductal gray matter and rostroventromedial medulla, which are involved in the endogenous analgesic system, are enhanced when TSP levels are high, and various stimuli that induce TSP are applied. 29 In this study, we did not examine the active brain sites. However, since previous reports have shown enhanced endogenous analgesic system, 12 it is highly likely that similar sites were enhanced in the present study, resulting in an increase in the pain threshold of the muscles. However, the cutoff TSP value requires further consideration in future research.
Differential Pain Threshold in Tissue
In the present study, when the groups were divided by TSP, there was no difference in CPM, which reflects the status of endogenous analgesic mechanism,21,24 between groups prior to the intervention. However, there was a significant difference between both groups only in the muscle pain threshold after electroacupuncture intervention, and a significant difference in muscle pain threshold in the high group at 60 min after intervention was confirmed within the groups. In general, it has been reported that the analgesic effect of electroacupuncture involves endogenous opioids, including β-endorphin in addition to the descending pain inhibitory system. 9 In the present study, low-frequency stimulation was applied for 30 min, and muscle pain thresholds increased 60 min after the intervention in the high group. It has been reported that low-frequency electroacupuncture takes some time to produce analgesic acupuncture effects, and the effects are suppressed by naloxone. 35 Moreover, β-endorphin and enkephalins are involved in the analgesic effect of low-frequency acupuncture.9,35 Accordingly, it is highly likely that endogenous opioids are involved in the increase in pain threshold 60 min after the intervention with low-frequency electroacupuncture. Nevertheless, the fact that only muscle showed a significant increase in pain threshold in the present study is based on reports that the opioid drug remifentanil increased the muscle pain threshold more than the skin pain threshold. 36 Moreover, opioid antagonist naloxone affected muscle pain thresholds, but not skin pain thresholds, suggesting that skin pain thresholds are serotonergic and that muscle pain thresholds are opioidergic and strongly involved. 37 Accordingly, it is likely that opioids had the main influence on the increase in pain threshold in the present study and that only the muscle pain threshold increased.
Limitations
The study participants were healthy without chronic pain and had PCS and HADS scores within the normal range, which were thought to affect the endogenous analgesic system, as well as low levels of catastrophic thinking and anxiety. However, it has been suggested that, in patients with chronic pain, strong catastrophic thinking causes functional impairment of DLPFC, 19 and strong anxiety increases the activity of the limbic system and suppresses the function of the descending inhibitory pain pathways. 38 Furthermore, the endogenous analgesic system affects spinal cord hypersensitization, 39 which is known to have a significant impact on analgesic efficacy. Therefore, it is unclear whether the results would be similar to those of the present study if patients with chronic pain were included. Moreover, although the present study was conducted in younger participants, reduced endogenous analgesic system 14 and spinal cord hyperalgesia have been reported in older adults, 40 and estrogen may affect pain sensitivity in women. 41 Additionally, the psychological effects of electroacupuncture should be considered; thus incorporating both a sham group and a control group is necessary. Therefore, it is necessary to examine the present results with various participants to ensure generalizability and validity.
CONCLUSIONS
In this study, we examined how the spinal cord response in healthy participants affects the change in the pain threshold induced by electroacupuncture, using TSP which reflects the spinal cord response. In healthy participants in whom the endogenous analgesic mechanism was confirmed to work normally, a difference in the effect of electroacupuncture depending on the spinal cord response indicated by TSP was observed; the muscle pain threshold increased only in the group with high TSP.
Footnotes
ACKNOWLEDGMENTS
AUTHORS’ CONTRIBUTIONS
The draft study protocol was prepared by M.O. and adopted, with some modifications, under the guidance of S.S. and K.I. Data were collected mainly by M.O. and partly with the cooperation of S.H. Data and statistical analyses were performed by M.O. under the guidance of K.I. The article was drafted by M.O., who prepared the final manuscript with reference to all coauthors’ comments. Moreover, the article was edited for language by Editage. All coauthors have approved the final manuscript for publication.
AUTHOR DISCLOSURE STATEMENT
There are no conflicts of interest to disclose regarding this article.
FUNDING INFORMATION
No research funding was received for this article.