
Abstract
We describe development and validation of a high-throughput screen (HTS) for identifying small molecules that restore the efficacy of carbapenems (adjunctives) and/or directly inhibit growth of carbapenem-resistant Enterobacteriaceae (CRE). Our HTS assay is based on a screen–counterscreen approach using a representative multidrug-resistant CRE strain, Klebsiella pneumoniae BIDMC12A. Specifically, we tested the ability of small molecules to inhibit bacterial growth in the presence (screen) or absence (counterscreen) of meropenem, a representative carbapenem antibiotic. Primary screening of 11,698 known bioactive compounds identified 14 with adjunctive activity and 79 with direct antimicrobial effect. Secondary screening identified triclosan as a strongly synergistic meropenem adjunctive (fractional inhibitory concentration = 0.48) and confirmed azidothymidine (AZT) (minimal inhibitory concentration [MIC] = 4 μg mL−1), NH125 (MIC = 4 μg mL−1), diphenyleneiodonium chloride (MIC = 8 μg mL−1), and spectinomycin (MIC = 32 μg mL−1) as potent direct antimicrobials. Spectrum of activity of AZT and spectinomycin was tested against a collection of 103 representative Enterobacteriaceae strains (≈50% CRE). AZT, a nucleoside analog used to treat human immunodeficiency virus, demonstrated an MIC50 of 2 μg mL−1. Spectinomycin, an antibiotic used to treat gonorrhea, had an MIC50 of 32 μg mL−1. Therefore, a significant percentage of CRE strains appeared relatively susceptible to these antimicrobials. These data identified AZT and spectinomycin as available agents warranting further study for potential treatment of multidrug-resistant CRE infection. Our results provide proof of principle and impetus for performing a large-scale HTS for discovery of novel, small-molecule adjunctives and antibacterial agents directly targeting CRE.
Introduction
Gram-negative Enterobacteriaceae are the most frequent cause of urinary tract infections and the second most frequent cause of surgical site and bloodstream infections. 1 Unfortunately, these bacterial pathogens commonly express resistance to a wide variety of antibiotics. Such resistance has increased dramatically in recent decades. 2 Previously, carbapenem antibiotics remained a broadly effective, relatively nontoxic treatment even for these multidrug-resistant bacteria. However, of great concern, carbapenem resistance has now emerged in Enterobacteriaceae (most notably among Klebsiella pneumoniae, Escherichia coli, and Enterobacter spp.), in the United States and around the world, undermining carbapenem efficacy. 3 Not surprisingly, carbapenem-resistant Enterobacteriaceae (CRE) infection is associated with a high mortality rate. 4,5 Often, either toxic or no therapeutic options remain. Accordingly, CRE are now classified in the highest threat level by the Centers for Disease Control and Prevention. 6 –9
Therefore, new effective treatments for CRE are desperately needed. These might include either new antimicrobials directly targeting CRE or adjunctive antimicrobials that restore susceptibility to existing antibiotics. Restoration of carbapenem activity may have particular merit based on the intrinsic broad-spectrum bactericidal activity and favorable safety profile of these β-lactam agents. 10 Current understanding of carbapenem pharmacokinetics–pharmacodynamics (PKs–PDs) indicates that therapeutic success depends on the minimal inhibitory concentration (MIC) of the organism being treated. 11,12 The MIC is defined as the lowest twofold dilution of antimicrobial that inhibits visible growth in vitro under standardized conditions. Specifically, Enterobacteriaceae with a meropenem (a carbapenem) MIC ≤1 μg mL−1 behave as clinically susceptible, 11,12 without regard to the potential underlying genotypic resistance mechanisms. Therefore, the current recommendations in the United States are to treat solely based on the MIC. 12
Carbapenem resistance in the United States is typically mediated by a β-lactamase called the K. pneumoniae carbapenemase (KPC). However, different strains possessing the same KPC gene show widely differing levels of inhibition by carbapenems, with MICs spanning the range of susceptibility to frank resistance. 13 Furthermore, transfer of carbapenemase-containing plasmids into E. coli K-12 is associated with a substantially lower MIC in the recipient. 14 These observations suggest that attributes of the host strain contribute substantially to the phenotypic expression of carbapenem resistance. We therefore hypothesized that CRE strains could be modulated using small molecules to lower the carbapenem MIC into the susceptible range and thereby restore carbapenem therapeutic efficacy.
Accordingly, we sought to develop and validate a high-throughput screen (HTS) to simultaneously detect antimicrobials that restore carbapenem susceptibility and/or directly target CRE. Identifying small molecules that successfully target Gram-negative organisms, especially those displaying a multidrug resistance phenotype, is notoriously difficult based on impermeability of the Gram-negative double membrane combined with extensive systems of efflux pumps. 15 Of note, K. pneumoniae is the most broadly resistant, clinically aggressive, and widespread CRE in the United States. We therefore adopted a live cell screen–counterscreen approach using a representative K. pneumoniae CRE strain so that hits identified in our HTS will have already passed the bar for efficacy against a clinically relevant, multidrug-resistant bacterium. In this study, we describe HTS data and secondary analysis for >10,000 bioactive compounds. In addition to obtaining proof of principle for our approach, we identified several available agents that may prove useful in treating CRE infection.
Materials and Methods
Bacterial Strains and Chemicals
BIDMC12A is a KPC-expressing K. pneumoniae clinical isolate. Its genome sequence (Carbapenem Resistance Initiative, Broad Institute,
Primary Screening
Primary screening was performed in duplicate at the ICCB-Longwood Screening Facility (Harvard Medical School, Boston, MA) using known bioactive libraries. Bioactive libraries include FDA-approved drugs, compounds with a history of use in clinical trials, and specialized libraries containing compounds with at least partially known biological effects, such as kinase inhibitors, ion channel inhibitors, G-protein-coupled receptor inhibitors, and active biolipids. See HTS Protocol (Table 1) for an overview of the HTS assay procedure.
HTS Protocol
1. Growth medium was dispensed using a Multidrop Combi Automated Liquid Handler (Thermo Fisher Scientific, Waltham, MA).
2. Positive controls were always located in column 24.
3. Compounds are introduced into experimental wells at a 1:200 dilution. Final concentrations varied between libraries. Final compound concentrations used were 25 μg/mL, 10 μg/mL, 50 μM, 16.7 μM, or 5.6 μM.
4. Negative controls were always located in column 23.
5. Final concentration of cells is ∼5 × 105 CFU/mL.
6. Plates are stacked no more than four plates high with ample space between stacks for even heat distribution.
7. OD600 was read using an EnVision Plate Reader (PerkinElmer, Waltham, MA).
8. Z-scores were calculated using the average and standard deviation of experimental wells. Hits were selected using the least significant z-score between replicates.
CLSI, Clinical and Laboratory Standards Institute; HTS, high-throughput screen.
Two days before use in the primary or secondary screening assays, bacteria were recovered from a frozen stock and passaged on trypticase soy agar containing 5% sheep blood (Remel, Lenexa, KS). Single isolated colonies were inoculated into cation-adjusted Mueller–Hinton broth (BD Diagnostics, Franklin Lakes, NJ) and grown overnight before each experiment (∼18 h at 37°C in a humidified 5% CO2 atmosphere).
Experiments were performed in clear 384-well plates (Greiner Bio-One, Monroe, NC). Less than 1 h before compound transfer, test and negative control wells were filled with 30 μL of cation-adjusted Mueller–Hinton broth with or without 20 μg mL−1 meropenem in the screen and counterscreen, respectively, using a Multidrop Combi Reagent Dispenser (Thermo Fisher Scientific, Waltham, MA). Positive control wells were filled with 30 μL of cation-adjusted Mueller–Hinton broth with 10 μg mL−1 colistin ±20 μg mL−1 meropenem.
Plates were then centrifuged at 150 g for 1 s. Three hundred nanoliters of each test compound was added to screening wells using a pin transfer robot. Bacterial inocula were prepared by dilution of an overnight culture of K. pneumoniae BIDMC12A to 1 × 106 CFU mL−1 in sterile, cation-adjusted Mueller–Hinton broth. Thirty microliters of this suspension was immediately added to all wells to achieve a final inoculum concentration of 5 × 105 CFU mL−1, consistent with the CLSI guidelines for antimicrobial susceptibility testing. 18 Note, the final meropenem and colistin concentrations cited in the previous paragraph were reduced twofold during addition of bacteria. Plates were incubated for 48 h at 37°C in ambient air with 100% humidity in stacks no greater than four plates high with ample space for air circulation.
Data Collection and Analysis
Cell growth was quantified by optical density at 600 nm (OD600) using an EnVision Plate Reader (PerkinElmer, Waltham, MA). Z′-scores were calculated for the screen and counterscreen on a plate-by-plate basis using data from 16 positive and 16 negative control wells using the following formula:
Z-scores were calculated for each well using the formula
Hit Confirmation
Hits were cherry-picked from library plates using an EVO75 Liquid Handling Platform (Tecan, Medford, MA) and analyzed in an abbreviated two-dimensional synergy/direct inhibition test to verify their activity. Specifically, fourfold serial dilutions of cherry-picked compounds (dissolved in DMSO) were dispensed into 384-well plates alone or in combination with 10 or 2.5 μg mL−1 meropenem using a D300 Digital Dispensing System (Hewlett-Packard, Palo Alto, CA). Total DMSO concentration in the wells was kept below 1%, as recommended by the CLSI guidelines for testing antibiotics dissolved in this solvent. 12 Wells were inoculated with K. pneumoniae BIDMC12A at a density of ∼5 × 105 CFU mL−1 in cation-adjusted Mueller–Hinton broth in a 60 μL assay volume. Plates were incubated at 37°C in ambient air at 100% humidity for 48 h. Growth was quantified by reading OD600. Percent growth inhibition was calculated compared with controls.
Two-Dimensional Synergy Testing
Two-dimensional synergy testing was conducted for select antimicrobials using the method of Chiaraviglio and Kirby with modifications. Briefly,
Dose–Response Curves
Inhibitory effects of AZT, diphenyleneiodonium chloride (DPI), NH125, and spectinomycin were tested using the CLSI guidelines for broth microdilution. 18 Experiments were performed in triplicate with at least two replicates per experiment. Dose–response curves were generated by plotting log10 concentration of compound versus percent growth normalized to an antibiotic-free control. As per convention in the antimicrobial resistance field, concentrations were plotted in micrograms per milliliter. IC50 and IC90 values were calculated using regression analysis. The MIC values in the same experiments were determined according to the CLSI guidelines for microbroth dilution, that is, the lowest concentration of compound resulting in complete visible inhibition of growth. 18
Activity Spectrum Testing
A total of 103 clinical isolates (50 carbapenem resistant and 53 carbapenem susceptible) were used to investigate AZT and spectinomycin activity spectrum. Strains were stored at −80°C arrayed in 96-well plates (Corning, Corning, NY) in 50% glycerol. One day before experiments, 96-well plates containing 100 μL sterile, cation-adjusted Mueller–Hinton broth were inoculated using a 96-pin replicator (Boekel, Feasterville, PA) and grown to stationary phase. On the day of the experiment, stationary phase cultures were diluted 1:400 into fresh media. A replicator tool was used to inoculate diluted bacteria into 96-well plates, each containing a separate twofold dilution of the appropriate drug. Plates were incubated overnight at 37°C in a humidified 5% CO2 atmosphere. Cell growth was then quantified by measurement of OD600 using an Epoch Microplate Reader (BioTek). MICs were defined as the concentration at which 95% of bacterial growth was inhibited compared to a control containing media alone. Experiments were performed in triplicate on separate days with independent inocula, and median MIC values were reported.
Results
Primary Screening
Our HTS for adjunctives and direct antimicrobials was designed as a parallel screen–counterscreen assay, in which each test compound was simultaneously evaluated for its ability to potentiate a subinhibitory concentration of a widely used carbapenem, meropenem (screen), and for its direct antibacterial effect (counterscreen). Simply, a representative K. pneumoniae CRE strain, BIDMC12A, was inoculated into a 384-well plate in the presence (screen) or absence (counterscreen) of 10 μg mL−1 meropenem. Inoculum concentrations and growth media corresponded to standards used for in vitro susceptibility testing. 18 Output was optical density measurement of bacterial growth after 48 h. Compounds that inhibited growth solely in the screen were considered potential adjunctives, while those that inhibited growth in both the screen and counterscreen were considered direct antimicrobials. Selection of the 48-h incubation period was based on initial experiments showing superior Z′-scores in the screening assay at 48 (average Z′ = 0.77) versus 24 h (average Z′ = 0.43).
Importantly, our screening strain is a representative of K. pneumoniae ST258 (Carbapenem Resistance Initiative, Broad Institute,
The subinhibitory concentration of meropenem (10 μg mL−1) used in the screening assay was fivefold below the highly reproducible MIC (50 μg mL−1) of the screening strain determined by the CLSI broth microdilution reference method (data not shown). Therefore, in primary screening, we were asking for compounds that could lower the meropenem MIC significantly (≥5-fold) but not necessarily into the susceptible range (MIC ≤1). Therefore, the meropenem screening concentration was chosen as a balance between sensitivity and stringency, with the knowledge that a subset of CRE might be shifted into the clinically susceptible range with a fivefold carbapenem MIC reduction, and the activity of potential hits might be improved upon during follow-up structure–activity relationship studies.
Initially, the assay was optimized for incubation time and well volume (data not shown) resulting in Z′ that routinely exceeded 0.6 in the screen and counterscreen. Using the optimized assay, we screened 11,698 compounds from the known bioactive collection at the ICCB-Longwood Screening Facility (Harvard Medical School, Boston, MA). Both screen and counterscreen were performed in duplicate to reduce the false-positive rate with use of the least significant z-score from each pair for categorizing hits. 21 The assay demonstrated good correlation between replicate wells (screen, R 2 = 0.76, and counterscreen, R 2 = 0.74; Fig. 1). Z′ for all plates in the HTS effort averaged 0.69 in the screen and 0.62 in the counterscreen.
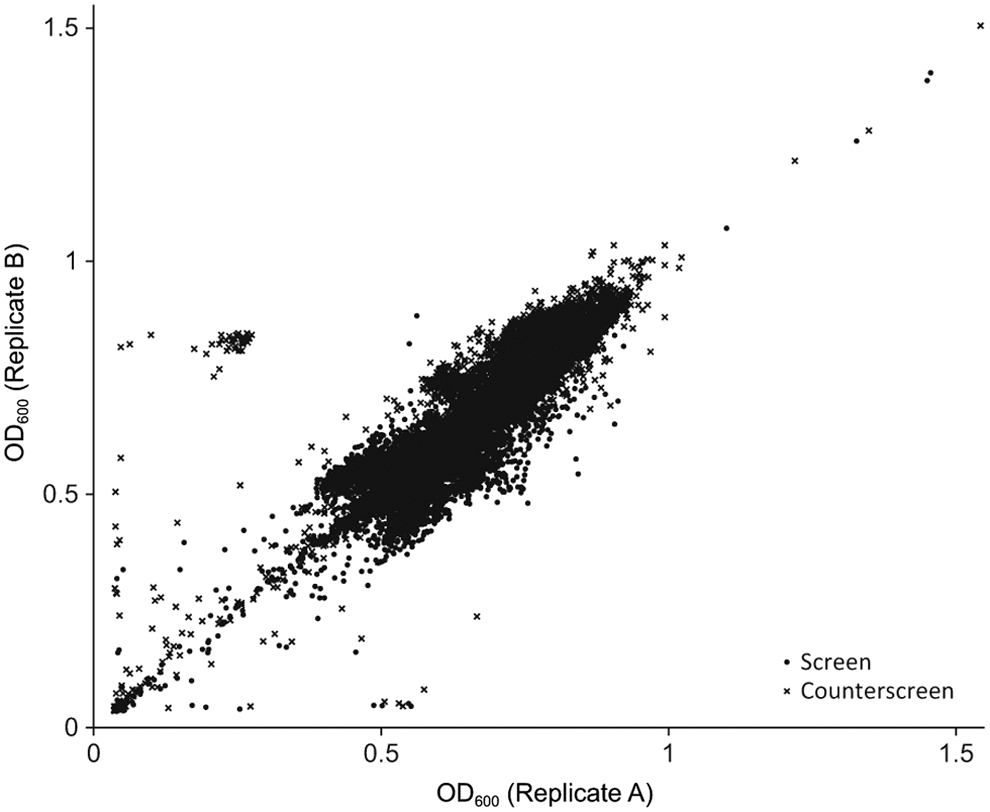
Correlation between replicates. Our screen was performed as a screen–counterscreen experiment, each with two replicates (A and B). OD600 values are plotted for each replicate of the screen (×) and counterscreen (•), respectively. Screen, R 2 = 0.74, and counterscreen, R 2 = 0.76.
Screening hits are summarized in Supplementary Tables S1 and S2 (Supplementary Data are available online at
Notably, z-scores correlated well with relative growth (R 2 = 0.86) and proved sensitive enough to identify hits with even modest inhibition (see Fig. 2 for representative data from a single screening plate). Due to this sensitivity, 25.7% of hits had less than 50% growth reduction. To limit our secondary analysis to compounds likely to be highly active, we excluded those that consistently displayed less than 50% growth reduction in primary screening.
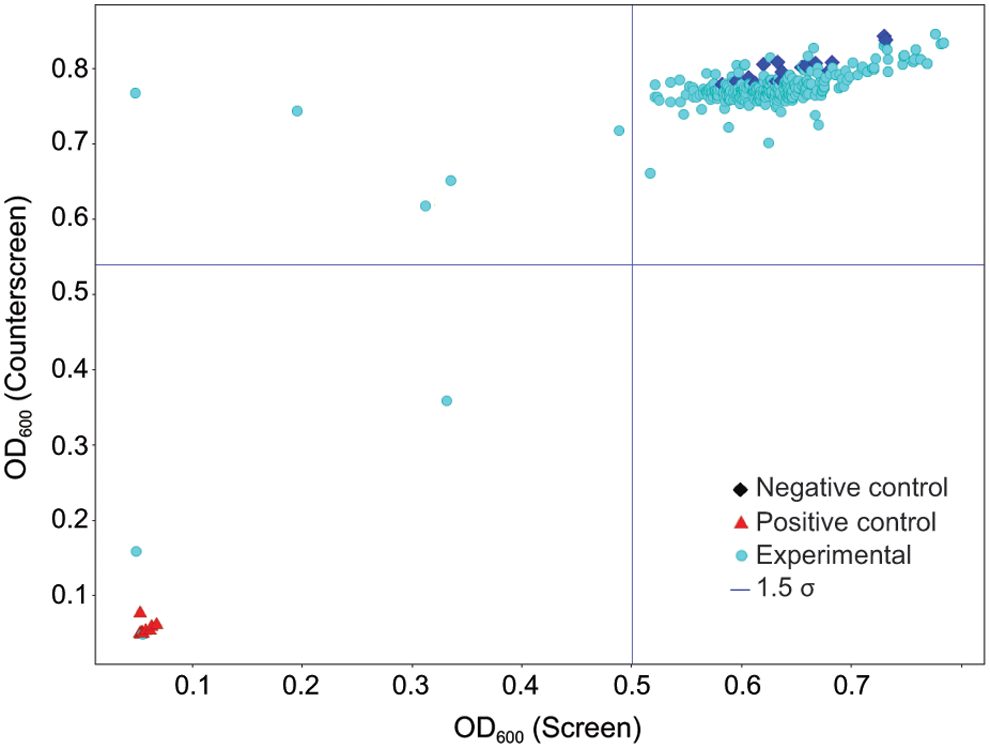
Representative screening data. OD600 values from a representative 384-well plate (screened in duplicate) were averaged between the screen and counterscreen and plotted on the x and y axes, respectively. Experimental compounds (◯) that result in low growth in the screen but high growth in the counterscreen (upper left-hand corner of the graph) were considered putative adjunctives. Those that show inhibition in both the screen and counterscreen were considered direct antimicrobials. Positive (▲) and negative (♦) controls are located in the lower left and upper right, respectively. Color images available online at
Secondary Analyses and Two-Dimensional Synergy Testing
Based on this criterion, secondary analysis was selectively performed on 56 potential direct antimicrobials and 13 potential adjunctives (see Supplementary Table S2 for a list of included and excluded compounds and Supplementary Table S3 for results of secondary analysis) using small volume cherry picks from screening libraries. Fourteen (25%) suspected direct antimicrobials showed at least 50% growth inhibition in secondary analysis and were considered confirmed. Seven (12.5%) compounds initially classified as direct antibacterials demonstrated growth inhibition ranging from 25% to 49% and were classified as weakly active. In contrast, adjunctive activity detected in the primary screen was not confirmed during low-resolution checkerboard analysis using a fourfold dilution series. However, 14 (25%) compounds initially identified as direct antimicrobials displayed lower MIC or IC50 values in the presence of meropenem and were therefore reclassified as adjunctive. Compounds for which an MIC or IC50 could not be observed and showing less than 25% inhibition at concentrations equal to those tested in the HTS (50.7% of all compounds tested) were classified as negative.
Three putative adjunctives (azithromycin, calmidazolium, and triclosan) based on low-resolution testing were selected for follow-up high-resolution (
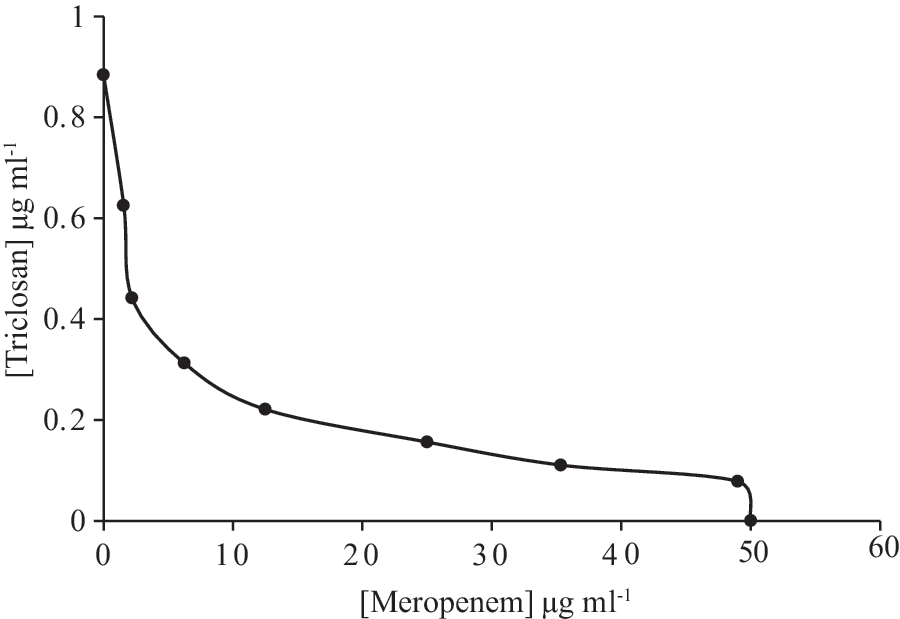
Isobologram suggested synergy between triclosan and meropenem. The isobologram was generated using
Generation of Dose–Response Curves
Several compounds not typically considered antibacterial agents were found to have a strong antimicrobial activity in primary and secondary analyses. Among these compounds, DPI, NH125, and AZT were selected for further examination by dose–response curve analysis (Fig. 4). Although the MICs of these compounds were similar (Table 2), the dose–response curves differed (Fig. 4). NH125 showed a sharp decline in growth inhibition at dilutions below its MIC. In contrast, DPI exhibited a more gradual inhibition. AZT, a nucleoside analog used to treat human immunodeficiency virus infection, 27 showed a sigmoidal inhibition curve, with appreciable inhibition at concentrations well below its MIC (4 μg mL−1), manifesting in an IC80 (see Discussion) of 0.53 μg mL−1 and an IC50 20-fold below the MIC. Spectinomycin, an aminoglycoside antibiotic used to treat Neisseria gonorrhoeae infections, 28 was also selected for further analysis (Fig. 4) based on growth inhibition in primary screening at concentrations significantly below those achievable in human serum 29 (Supplementary Table S1). In dose–response testing, spectinomycin inhibited growth at concentrations as low as 8 μg mL−1, with an MIC of 32 μg mL−1 (Table 2).
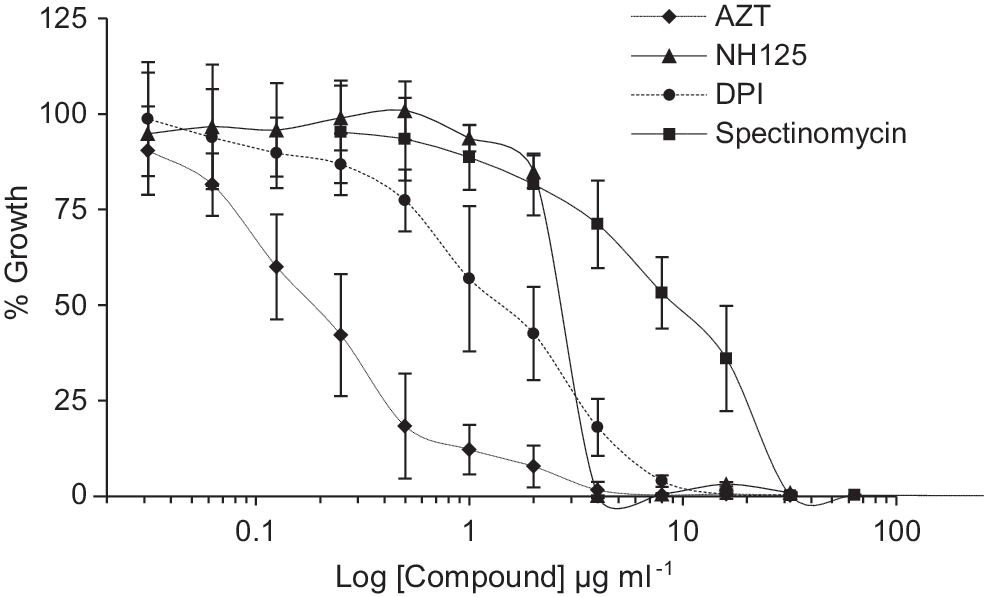
Dose–response curves for selected compounds. Data points represent mean ± one standard deviation (error bars) of at least three experiments; AZT (♦), NH125 (▲), DPI (•), and spectinomycin (■). AZT, azidothymidine; DPI, diphenyleneiodonium chloride.
Inhibitory Activity (μg mL− 1) of Selected Compounds
aTrailing endpoint MIC for AZT (listed in parentheses) was calculated using guidelines for thymidine salvage pathway inhibitors, trimethoprim and sulfamethoxazole.
bIC50 and IC90 values were calculated by regression analysis, except for NH125, due to the abrupt change near the MIC.
DPI, diphenyleneiodonium chloride; MIC, minimal inhibitory concentration.
Spectrum of Activity
Based on the relatively low MICs, AZT and spectinomycin were tested for activity spectrum against 103 carbapenem-resistant and carbapenem-susceptible clinical isolates collected at our institution over the past 7 years. Assays were performed in triplicate on consecutive days. The median MIC calculated from all three experiments is shown in Tables 3 and 4. For all strains tested, the MIC50 for AZT was 2 μg mL−1. Importantly, the MIC value was ≤4 μg mL−1 for 56% of CRE strains. The MIC50 for spectinomycin was 32 μg mL−1. Forty-one percentage of the CRE strains were susceptible to spectinomycin (MIC ≤32 μg mL−1) based on interpretive criteria for N. gonorrhoeae. 12
AZT Susceptibility Data for Clinical Enterobacteriaceae Strains
aMeropenem resistance defined as an MIC of ≥2 μg/mL−1.
bIncludes four strains of Serratia marcescens and one strain of Citrobacter freundii.
ND, too few strains represented to make an accurate determination.
Spectinomycin Susceptibility Data for Clinical Enterobacteriaceae Strains
aMeropenem resistance defined as an MIC of ≥2 μg/mL−1.
bIncludes four strains of S. marcescens and one strain of C. freundii.
ND, too few strains represented to make an accurate determination.
Discussion
In this work, we describe an HTS–counterscreen assay to simultaneously detect compounds that act either directly or indirectly, through potentiation of carbapenem activity, to inhibit growth of CRE. The whole-cell bioassay demonstrated robust statistical performance and allowed us to identify potentially clinically useful hits from a large known bioactive collection.
Options for treatment of CRE are extremely limited. Therefore, there is a critical need for new antimicrobials that overcome the plethora of resistance mechanisms associated with CRE. This motivated us to design an HTS assay capable of identifying two types of agents that inhibit multidrug-resistant, carbapenemase-producing K. pneumoniae. The nature and rationale for the first—direct antimicrobial compounds—are obvious. However, the rationale for the second—compounds adjunctive with a carbapenem—deserves further comment. Carbapenems are broadly acting, bactericidal, β-lactam agents with a very favorable safety profile. Carbapenemase enzymes aside, carbapenems are effectively immune to hydrolysis by the multiplicity of additional β-lactamase enzymes carried by CRE strains (noted in a homology search of genomes available through the Carbapenem Resistance Initiative, Broad Institute,
Importantly, variable phenotypic expression of the same KPC gene in different bacterial host backgrounds suggests that certain attributes of the host strain could be modulated to restore carbapenem susceptibility. Indeed, there is some precedent for use of adjunctives to restore carbapenem efficacy. The conceptually simplest are small-molecule adjunctives that directly inhibit carbapenemase activity. Two examples are avibactam, 31 recently FDA approved, and RPX7009, currently in stage III clinical trials. 32 Modulation of carbapenem susceptibility in CRE strains through use of double carbapenem therapy or tigecycline–carbapenem combination has also been suggested in human case reports, 33,34 animal models, and/or in vitro studies. 35 However, it could be imagined that there are many other classes of compounds that might restore carbapenem efficacy through effects on antimicrobial transport, cell wall dynamics, or currently unknown mechanisms.
Our screen–counterscreen is capable of identifying three broad groups of adjunctives: (1) pure adjunctives that have no direct antimicrobial action in the absence of meropenem; (2) mixed adjunctives that display enhanced antimicrobial activity in the presence of meropenem, however, without reaching the formal definition of synergy in high-resolution checkerboard testing; specifically, their ΣFIC values were between 0.5 and 1; and (3) synergistic adjunctives that display enhanced antimicrobial activity in the presence of meropenem, with an ΣFIC value of <0.5. Hits from known antimicrobials often showed mixed adjunctive activity.
Interestingly, in replicate testing either in different primary screening libraries and/or in secondary screening, some compounds tested alternatively either as direct antimicrobials or pure, mixed, or synergistic adjunctives (Supplementary Tables S1–S3). These results are not surprising. Concentrations of the same compound in different libraries may differ either by design or through differential degradation during storage or freeze–thaw cycles. Our primary screening test for adjunctive activity was also necessarily limited to one concentration of meropenem, which may not have been optimal or discriminatory for detecting adjunctive activity.
In secondary analysis, digital dispensing technology allowed us to maximally use volume-limited cherry picks to test for basic adjunctive activity with two subinhibitory dilutions of meropenem and several fourfold dilutions of test compound. In this study, adjuvancy was defined as increased antimicrobial activity in the presence of meropenem as this analysis was not powered to detect or refute synergism by commonly used standards (i.e., FIC <0.5). For select compounds, we therefore tested formally for synergism by checkerboard titrations. Triclosan is an example of an antimicrobial compound that was not picked up as adjunctive in primary screening likely because concentrations tested (10 and 14.5 μg mL−1) were 10-fold greater than its MIC (0.88 μg mL−1). However, in secondary cherry-pick screening, we were able to test concentrations as low as 0.04 μg mL−1, more than 20-fold below the MIC. This allowed us to detect previously unidentified adjunctive activity. Triclosan was therefore selected for checkerboard testing, where it was found to be synergistic with meropenem. Interestingly, there are previous reports of synergy between triclosan and amoxicillin, another β-lactam antibiotic, reminiscent of our findings. 36
Notably, in checkerboard synergy testing, the synergistic demarcation of FIC <0.5 is a conservative cutoff based on the inherent error in twofold dilution checkerboard testing. It is possible to have true but less dramatic adjuvancy/synergism with a higher FIC index. However, reliable detection requires more robust methods, for example, through use of more discriminatory
Most direct antimicrobials identified in primary screening were neither adjunctive nor synergistic with meropenem. The most potent of these direct antimicrobials were NH125, DPI, spectinomycin, and AZT. Only the last two are approved for human therapy. NH125 is reported to have bactericidal and/or growth inhibitory activity against Gram-negative 38 and Gram-positive 38,39 organisms. Our calculated MIC of 4 μg mL−1 (Fig. 4) is similar to that found for E. coli K-12 (3.1 μg mL−1). 38 DPI is a nonspecific flavoenzyme inhibitor 40,41 with, to our knowledge, no previously reported antimicrobial activity. However, in a previous screen conducted by our laboratory, both compounds showed toxicity to the J774A.1 eukaryotic cell line at concentrations relevant to bacterial killing, 19 suggesting unacceptable selectivity. As such, they were not examined further.
Interestingly, several nucleoside analogs showed direct activity in primary and secondary screening assays. These results highlight nucleoside analogs as a promising class for future exploration to combat CRE as they appear to have some ability to avoid entrenched resistance mechanisms in these strains. AZT stood out as particularly potent.
AZT is best known as an inhibitor of HIV reverse transcriptase. 42,43 However, AZT is also a substrate for bacterial thymidine kinase (TK). 44 TK, a critical part of the thymidine salvage pathway, catalyzes the first of three phosphorylation events that make thymidine or AZT competent for incorporation into DNA. 44 Incorporation of AZT into DNA results in chain termination and ultimately cell death. 44 Therefore, AZT also acts as an antibacterial agent, and previous studies have reported activity against Escherichia, Enterobacter, Klebsiella, Salmonella, and Shigella. 44 –47 Our findings are therefore consistent with prior studies performed with a small number of carbapenem-susceptible Enterobacteriaceae strains.
Notably, the antibiotics, trimethoprim and sulfamethoxazole, also interfere with DNA synthesis through modulation of the thymidine salvage pathway. These drugs require special MIC interpretive criteria 18 as they commonly exhibit a phenomenon known as a “trailing endpoint.” Whereas the MIC value is standardly defined as the lowest concentration in a doubling dilution series with no visible microbial growth, the MIC values for trimethoprim and sulfamethoxazole are defined as the lowest concentration with 80% growth inhibition. 18 Therefore, if we apply the same 80% growth threshold for interpretation of the AZT data, the trailing endpoint MIC for the screening strain is 0.53 μg mL−1, nearly eightfold lower than the complete growth inhibition MIC (Fig. 4). Relevance of AZT trailing endpoints to in vivo efficacy will have to be determined through further study.
In vitro resistance to AZT has been reported to arise spontaneously in E. coli, 45 a phenomenon we observed with K. pneumoniae BIDMC12A at a nearly identical frequency (∼10−7, data not shown). Interestingly, this spontaneous mutation rate did not undermine successful AZT monotherapy in high-inoculum, E. coli, systemic calf or mouse pyelonephritis infection models. 48 Additionally, AZT treatment is correlated with a significant reduction in Salmonella relapses among HIV-infected patients, 49 further supporting the hypothesis that development of resistance in vitro does not necessarily preclude AZT efficacy in vivo and the potential for a significant antibacterial effect in humans.
PK parameters previously observed for AZT relative to the MIC values (calculated using complete inhibition rather than trailing endpoint inhibition) determined in our survey of carbapenem-resistant strains (MIC50 = 4) suggest the potential for treatment efficacy. Specifically, in phase I dose escalation trials, intravenous administration of 7.5 mg kg−1 every 4 h was associated with a 4.7 μg mL−1 peak serum concentration. 50 Overall, these observations suggest that AZT may be a therapeutic adjunct for CRE worthy of further experimental investigation. Of note, AZT did not appear to act synergistically with meropenem (FIC >0.5, data not shown).
Spectinomycin and apramycin, aminoglycoside/aminocyclitol antibiotics, were also identified as potent directly acting antimicrobials, with MIC values for the former frequently below cutoffs used to predict susceptibility in human infection (i.e., for N. gonorrhoeae). 12 Both differ structurally from other aminoglycosides (gentamicin, tobramycin, and amikacin). These structural differences presumably account for the absence or reduction in potentially limiting toxicities to hearing and kidney function generally associated with aminoglycosides. Specifically, spectinomycin appears potentially to be neither ototoxic 51 nor nephrotoxic. 52 Similarly, it was previously reported in animal and cochlear explant models that apramycin does not cause ototoxic side effects. 53 Renal toxicity may also be reduced. 53
Therefore, it was of interest to test spectrum of activity performed specifically for spectinomycin because of its availability as a human therapeutic. Spectinomycin proved broadly active against clinical Enterobacteriaceae isolates. More than 59% of carbapenem-susceptible strains and 40% of CRE have an MIC ≤32 μg mL−1, considered susceptible by the CLSI guidelines for N. gonorrhoeae. 12 Importantly, serum levels for spectinomycin reach 200 μg mL−1 after a 4-g dose delivered by intramuscular injection, the typical route of administration for treatment of N. gonorrhoeae. 49 Furthermore, this dosing regimen is not associated with significant side effects. 49 Achievable serum concentrations are well above the MIC50 for our strain collection and presumably at levels favorable to concentration-dependent killing 54 associated with aminoglycoside antibiotics. Therefore, based on in vitro activity and promising side effect profiles, spectinomycin and potentially apramycin as well might provide benefit in treatment of human CRE infection and deserve further investigation.
We point out several potential limitations in our study. Specifically, false negatives may occur in primary screening through degradation of labile compounds during either storage or assay incubation period. We chose to use a 48 rather than a 24-h assay incubation period based on an increased assay specificity (higher Z′) with the former; however, this choice was potentially at the expense of missing hits with labile activity. Of note, BIDMC12A is known to be susceptible to tigecycline based on clinical testing. Nevertheless, tigecycline was not detected as a direct antimicrobial hit in the HTS despite theoretical inclusion in libraries at concentrations above its MIC. Oxidation of tigecycline during long-term storage in screening libraries 12,55 presumably explains its lack of activity, consistent with evidence from a prior HTS effort. 19 It is well known that meropenem is labile, and we paid particular attention to handling of this reagent to ensure consistency of data throughout the HTS, specifically through single use of stock solutions, avoidance of freeze–thaw cycles, and meticulous quality control as described in the “Materials and Methods” section. False negatives may also arise through inclusion of too low a screening concentration, for example, through limitations in dissolving polar compounds in screening libraries. Lastly, the potential for clinical efficacy of known bioactive hits (AZT and spectinomycin) against CRE will need to be explored in PK–PD studies, experiments that we plan to pursue in the future. We note that the MIC90 values for the agents (Tables 3 and 4) likely exceed achievable serum concentrations (i.e., some CRE demonstrate frank resistance). If proven clinically efficacious in follow-up studies, these antimicrobials presumably could not be reliably used for empiric CRE therapy and would require susceptibility testing of clinical isolates to direct appropriate therapeutic use. Nevertheless, with few therapeutic options available for CRE, the potential to treat even a subset of strains may provide substantial clinical benefit.
We believe that the ability to detect direct antimicrobial activity and/or adjunctive activity in the same assay is a particular strength of our approach. Specifically, antimicrobials with the potential to synergize with meropenem, a therapeutically desirable property, might only be picked up as direct antimicrobials in our HTS. However, using our screening strategy, synergy will be uncovered in our more granular secondary assays, as observed for triclosan. Conversely, compounds detected initially as a pure adjunctive may have direct antimicrobial properties uncovered during either synergy or dose–response testing with fresh compound. Therefore, we believe our screening–counterscreening strategy enhances our ability to detect relevant activity against highly drug-resistant CRE.
Taken together, our data provide proof of principle for a screen–counterscreen approach for detecting direct and adjunctive inhibitors of CRE. Intriguingly, data generated with known bioactive libraries highlighted classes of antimicrobials, such as nucleoside analogs and aminoglycosides, that maintain activity despite many potential barriers associated with multidrug resistance. Presumably, their properties and those of small molecules identified in future large-scale screening efforts may be exploited to develop more effective therapeutics against these largely intractable pathogens.
Footnotes
Acknowledgments
This work was supported in part by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under award numbers R21AI119114 and R21AI112694 to J.E.K. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We would like to thank Jennifer Smith, Jennifer Nale, David Wrobel, Stewart Rudnicki, Rachel Warden, and Richard Siu (ICCB-Longwood) for their assistance. We also thank Lucius Chiaraviglio, Yoon-Suk Kang, and Jennifer Tsang for critical reading of the article.
Disclosure Statement
No competing financial interests exist.