
Abstract
Due to the increasing resistance of various Candida species to azole drugs, particularly fluconazole, it would be of significant importance to look for alternative therapies. The aim of this study was to investigate the antifungal activity of capric acid and its in vitro interactions with nystatin and fluconazole against Candida isolates. A total of 40 Candida isolates (C. albicans, 36; C. kefyr, 2; C. tropicalis, 1; C. glabrata, 1) collected from the oral cavity of neonates with oropharyngeal candidiasis and a reference strain of C. albicans (ATCC 10231) were used in this study. Antifungal activity of capric acid and two comparator antifungal drugs, namely fluconazole and nystatin, was tested according to CLSI M27-A3/M60 method. The in vitro interaction between capric acid with fluconazole and nystatin was determined following a checkerboard method and results were interpreted using fractional inhibitory concentration index. Nystatin had the lowest minimum inhibitory concentrations (range, 0.125–8 μg/mL; geometric mean [GM], 0.6229 μg/mL) followed by fluconazole (range, 0.5–16 μg/mL; GM, 1.9011 μg/mL) and capric acid (range, 128–2,048 μg/mL; GM, 835.9756 μg/mL). When tested in combination, capric acid with fluconazole demonstrated synergistic, indifferent, and antagonistic interactions in 3 (7.317%), 24 (58.536%), and 14 (34.146%) cases, respectively. For combination of capric acid with nystatin, synergistic, indifferent, and antagonistic interactions were observed in 1 (2.439%), 19 (46.341%), and 21 (51.219%) cases, respectively. All cases of synergistic interactions were against resistant or susceptible dose-dependent isolates. Fluconazole, nystatin, and capric acid seem to be more effective when they are used alone compared with their combination. However, their combination might be effective on resistant isolates.
Introduction
Oral candidiasis (oral thrush) is the most common opportunistic fungal infection of the oral cavity that is indiscernible in many cases. Candida spp. are part of the normal flora in the oral cavity of more than half of the world's population. However, they can turn into pathogenic form when any chemical change in the secretory enzymes and growth of beneficial oral bacteria occur. 1 The prevalence of oral candida in infants is 11% to 15% at the respective age. 2 The diagnosis of oral candidiasis is usually based on clinical findings. 3 After Candida albicans, the most common causes of oral candidiasis are Candida tropicalis, Candida glabrata, Candida dubliniensis, and Candida parapsilosis. 4
Treatment of oral thrush includes the control of risk factors and administration of topical or systemic antifungal drugs such as polyenes and azoles. 5 Nystatin is one of the polyene, drugs which binds to the ergosterol in the cytoplasmic membrane of fungi and changes its function. 6 –8 Nystatin has topical effects with low hepatotoxicity and no reported drug interference or adverse effects. 9,10 Fluconazole, a member of the azole group, in another drug of choice for treatment of oral trush. This drug disrupts the synthesis of fungal cytoplasmic membrane by inhibiting the lanosterol 14-α demethylase enzyme. 11,12 However, hepatotoxicity is a common side effect of this drug. 13 Overuse of azole drugs has an important role in the development of fluconazole resistance in Candida species. This resistance has an increasing trend among C. albicans and non-albicans Candida species over recent decades. 14 –16
Saccharomyces boulardii is a nonpathogenic yeast that is used as a fungus with probiotic properties in the prevention or treatment of diseases, such as gastrointestinal infections due to pathogenic bacteria or fungi. 17 –20 Capric acid, a medium-chain 10-carbon fatty acid extracted from S. boulardii, has been reported to demonstrate antifungal activity through inhibition of filamentation against Candida species. Capric acid has higher absorption capacity than long-chain fatty acids, and it has been suggested due to the strong acidic properties of capric acid. 21,22
Despite the promising antifungal activity of capric acid against standard strains of C. albicans (ATCC 28516, ATCC 2091 and ATCC 37037), 21,23,24 there is little information about the effect of this substance on clinical Candida species. Accordingly, we investigated the antifungal activity of capric acid and its in vitro interactions with fluconazole and nystatin on Candida species isolated from neonatal thrush.
Materials and Methods
Ethics Statement
The protocol of this study was in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Iran University of Medical Sciences (IR.IUMS.FMD.REC.1397.338).
Candida Isolate
A total of 41 strains of Candida, including C. albicans (n = 36), C. kefyr (n = 2), C. tropicalis (n = 1), C. glabrata (n = 1), and a reference strain of C. albicans (ATCC 10231) were included in this study. The clinical strains have been isolated from oral lesions of neonates with oropharyngeal candidiasis and have been molecularly characterized in a parallel study (unpublished data).
In Vitro Antifungal Activity of Capric Acid
In vitro activity of capric acid, fluconazole, and nystatin against isolates of Candida was determined according to CLSI M27-A3 protocol. 25 For preparation of fluconazole (12,800 μg/mL) and nystatin (6,400 μg/mL) stock solutions, 0.0128 g of fluconazole (Fanavaran Daroui Hackim, Iran) and 0.0064 g of nystatin (Jaber Ebne Hayyan Pharmaceutical Co., Iran) were dissolved in 1 mL sterile distilled water and dimethyl sulfoxide (Merck, Germany), respectively. Capric acid (Merck) was purchased as a liquid and was further diluted using ethanol (Merck) to reach the concentration of 8,192 μg/mL.
The stock solutions were sterilized through a filter (Membrane Solutions, China) with pore size of 0.22 μm. Serial dilution of the stock solution were prepared in RPMI-1640 (R6504; Sigma, Germany), according to the CLSI M27-A3 guidelines to obtain 2 × of the final concentrations ranging from 0.125 to 64 μg/mL for fluconazole, 0.0625 to 32 μg/mL for nystatin, and 8 to 4,096 μg/mL for capric acid. From each concentration of antifungal drugs and capric acid, 100 μL was dispensed into columns 1 to 10 of 96-well microtiter plates. Columns 11 and 12 were assigned as positive (without drug) and negative (without fungal inoculum) controls, respectively.
To prepare fungal inoculum, the isolates were subcultured on Sabouraud dextrose agar (Merck) containing chloramphenicol (50 μg/mL) and incubated at 37°C for 24–48 h. Primary inoculum was prepared in sterile phosphate-buffered saline, the density was adjusted to the recommended concentration by CLSI M27-A3 guidelines 25 and diluted in RPMI-1640. From the final fungal inoculum, 100 μL was added to all wells of 96-well microtiter plates, except for negative control wells. The plates were incubated at 35°C and according to the CLSI M27-A3 guidelines, results were read after 24 h. Minimum inhibitory concentration (MIC) of fluconazole and nystatin were determined as the lowest concentration of drugs that were able to inhibit 50% and 100% of growth, respectively. Results were interpreted according to CLSI M27-A3 and M60 documents. 25,26
Regarding capric acid, the lowest concentration which was able to inhibit 100% of growth was considered as MIC.
In Vitro Interactions Between Capric Acid with Fluconazole and Nystatin
A checkerboard method was used to determine the in vitro interactions between capric acid with fluconazole and nystatin. The same final concentrations of antifungal drugs were used. Regarding capric acid, concentrations ranged from 8 to 4,096 μg/mL. As described previously,
27
50 μL of concentrations of capric acid was added to rows A to G, and 50 μL of concentrations of fluconazole or nystatin were added to columns 1 to 10. Row H and column 11 contained capric acid and antifungal drugs, respectively. Column 12 was used as growth control. Subsequently, 100 μL of fungal inoculum was added to all wells of 96-well microtiter plates. Plates were incubated at 35°C for 24 h and results were read visually. For interpretation of results, fractional inhibitory concentration index (FICI) was calculated when FICI equals to (MIC drug A in combination
Results
When tested alone, nystatin had the lowest MIC values (MIC range, 0.125–8 μg/mL; geometric mean [GM], 0.6229 μg/mL), followed by fluconazole (range, 0.5–16 μg/mL; GM, 1.9011 μg/mL) with MIC modes of 1 and 2 μg/mL, respectively (Fig. 1). All isolates were susceptible to nystatin, except for the C. albicans ATCC 10231, which was susceptible dose dependent. Regarding fluconazole, 31 isolates were susceptible, 6 C. albicans isolates were susceptible dose dependent, and 4 isolates, including C. albicans (n = 3) and C. glabrata (n = 1) were resistant. Compared with antifungal drugs, capric acid demonstrated high MICs (MIC range, 128–2,048 μg/mL; GM, 835.9756 μg/mL) with MIC mode of 2,048 μg/mL. Distribution of Candida isolates based on the MIC values of fluconazole, nystatin, and capric acid are shown in Figure 1.
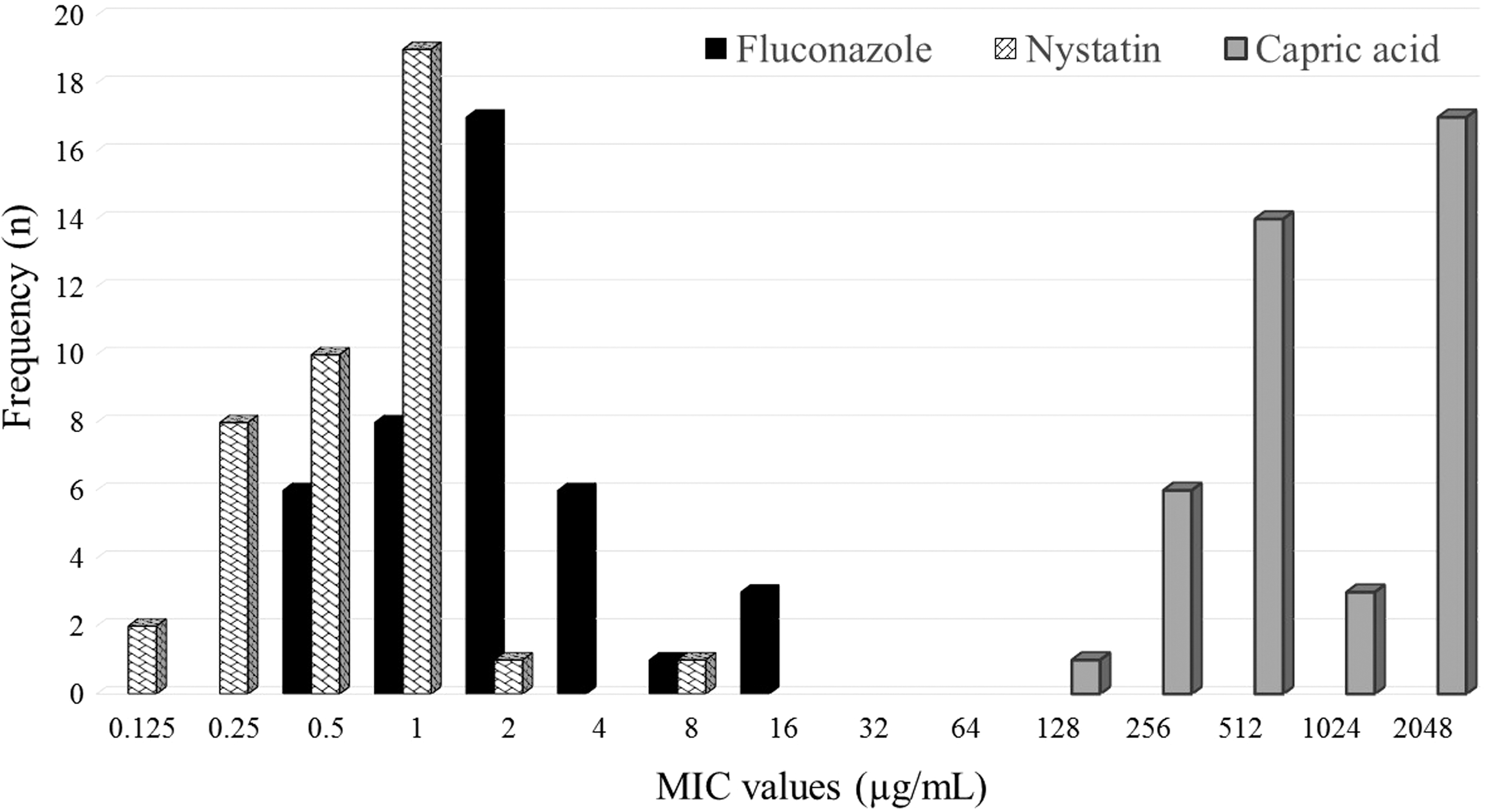
Distribution of 41 Candida isolates based on the MIC values of fluconazole, nystatin, and capric acid. MIC, minimum inhibitory concentration.
Table 1 shows the MICs of capric acid, fluconazole, and nystatin when tested alone and in combination, and the results of in vitro interactions. In the checkerboard assay, the interactions between capric acid with fluconazole were synergistic against 3 (7.317%) isolates (1 resistant C. albicans ATCC 10231, 2 susceptible dose dependent C. albicans isolates); FICI range (0.1875–0.375), indifferent against 24 (58.536%) isolates (FICI range, 0.75–4), and antagonistic against 14 (34.146%) isolates (FICI >4).
Minimum Inhibitory Concentrations of Capric Acid, Fluconazole, and Nystatin and Their In Vitro Interactions Against Candida Isolates from Oral Thrush
ANG, antagonism; CPA, capric acid; FICI, fractional inhibitory concentration index; FLZ, fluconazole; IND, indifference; INT, interpretation; MIC, minimum inhibitory concentration; NYS, nystatin; SYN, synergism.
Capric acid in combination with nystatin resulted in synergistic interaction only in 1 (2.439%) C. albicans ATCC 10231 strain (FICI = 0.375), indifferent interaction in 19 (46.341%) cases (FICI range, 1.0625–3) and antagonistic interaction in 21 (51.219%) cases (FICI >4).
Discussion
One of the facets of people's health assessment is attention to their oral cavity. Candidiasis is one of the most common and widespread human fungal diseases, which has increased strikingly in recent years. 29 Overall, all of the drugs tested in the present study have a documented clinical effect on Candida infections. Nystatin and fluconazole are effective drugs for the treatment of oral thrush but drug resistance in various Candida species due to overuse of these drugs has become a medical problem. 10,11,30
Combination therapy is a promising method to increase the effectiveness of antimicrobial therapy for infections that are nonresponsive to routine therapies. The combination of two or more antifungal drugs or nonantifungal drugs has been appraised toward overcoming therapeutic failures. 31,32 The main advantages of antimicrobial combination therapy include obtaining synergistic antifungal effect by lower concentrations of drugs in comparison to their use individually.
Decreased dosages of antifungal drugs result in decreased toxic side effects, reducing the chance of secondary antifungal resistance and possibly shortening the treatment period. 33 Accordingly, in the present study, the effect of capric acid in combination with nystatin or fluconazole was investigated. Results indicated that capric acid alone, had a stronger effect against oral Candida isolates than its combination with common antifungal drugs. Meanwhile, it should be highlighted that combination of capric acid with fluconazole and nystatin is efficacious against some resistant and susceptible dose-dependent isolates. These findings partly approbate with the reports of a number of studies, which also find the same result with our results. Some in vitro studies have demonstrated the effectiveness of fluconazole and nystatin used alone or applied in combination with capric acid.
Jadhav et al. in a gene expression study investigated the effect of capric acid and caprylic acid on the virulence of a standard strain of C. albicans (ATCC 90028). Results of this study showed that these acids are able to inhibit the yeast-to-hypha transition and stop the normal cell cycle. 34 Scheibler et al. combined chlorhexidine with nystatin to investigate their effect on the biofilm of C. albicans. Based on their results, the effect of drugs alone on biofilm was better and more effective than the combination. 5 Ninomiya et al. combined terpinene-4-ol and capric acid and examined its effect on C. albicans filamentous growth in mice with oral candidiasis. They observed that the interaction between these two compounds was synergistic and inhibited the filamentation of C. albicans, although, could be an appropriate candidate for oral thrush therapy.
Bergsson et al. investigated the susceptibility of three strains of C. albicans to a number of fatty acids and monoglycerides and concluded that capric acid had the most fungicidal effect on all these strains. 23 Fan et al. studied the effects of nystatin and fluconazole in patients with recurrent vulvovaginal candidiasis and concluded that both drugs were effective during the first course of treatment. Nonetheless, after persistence in the course of the drug for 6 months, they found that the improvement in the nystatin group was much better than the fluconazole group. Since some Candida species were resistant to fluconazole, nystatin could be effective in the treatment of a number of fluconazole-resistant Candida species. 35
Hsieh et al. appraised the effect of the combination of antimicrobial photodynamic therapy (aPDT) with fluconazole in the inactivation of planktonic cells and biofilm of C. albicans. The authors observed that the application of fluconazole for 48 h, followed by aPDT diminish the biofilm metabolism from 100% to 5%. 36 Barkvoll et al. showed that the MIC values of chlorhexidine digluconate and nystatin in combination were significantly higher than the values for each of the drugs alone. The results revealed that the combination of the drugs is not effective in vitro against C. albicans. This finding implies that nystatin and chlorhexidine digluconate may be antagonistic inhibitors of the growth of C. albicans. 37
Conclusion
According to our results, capric acid alone, had a stronger effect against oral Candida isolates than its combination with common antifungal drugs, and its combination effect with fluconazole and nystatin was shown to be effective on resistant species in a number of cases. So, it can be concluded that although capric acid does not seem to be helpful in combination with fluconazole or nystatin against susceptible isolates, the combined therapy might be a promising choice for oral candidiasis induced by C. albicans resistant to nystatin and fluconazole. However, this finding needs future studies to be further clarified.
Footnotes
Acknowledgments
The authors are grateful to Jaber Ebne Hayyan Pharmaceutical Company for their valuable help and also, the Research Vice President of the Iran University of Medical Sciences.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported financially by the Iran University of Medical Sciences (grant no. 98-1-4-13970).