
Abstract
Methicillin-resistant Staphylococcus aureus (MRSA) are challenging pathogenic bacteria that can cause severe infection leading to high mortality rates. We found that both the oxacillin- and cefoxitin-resistant S. aureus strains isolated from clinic showed multidrug-resistant (MDR) characteristics. Through rapid high-throughput screen (HTS) of a compound library, gemcitabine and selen compounds were found to effectively inhibit S. aureus growth. For further improvement, we synthesized selen-containing gemcitabine that demonstrated relatively potent antimicrobial activity against several MDR MRSA in vitro. The HTS assay and gemcitabine selen derivative provided a useful tool to explore an effective molecular target to treat MDR MRSA.
INTRODUCTION
Staphylococcus aureus is a gram-positive opportunistic pathogen most frequently isolated from community- and hospital-acquired infections, and is one of the most significant clinical pathogens, because of its capacity to adapt to diverse environmental conditions. 1 –3 Methicillin-resistant Staphylococcus aureus (MRSA) refer to those S. aureus strains that express the mecA gene or other resistance mechanisms, and have also shown cefoxitin (FOX) or oxacillin (OXA) resistance 4,5 by antibiotic susceptibility testing (AST). Infections caused by MRSA are more difficult to treat than that of methicillin-susceptible S. aureus.
Owing to the abuse of antibiotics, MRSA strains have further developed multidrug resistance (MDR) or extensive drug resistance (XDR). 6 The main mechanisms of drug resistance include β-lactamase production, 7 penicillin-binding protein 2a (PBP2a) encoded by chromosomal gene mecA, 8 and mutations that modified the target sites of antibiotics 9 . Currently, MRSA shows resistance to almost all β-lactam antibiotics being used. In addition, strains of S. aureus are also found resistant to other classes of antibiotics including aminoglycosides, fluoroquinolones, tetracyclines (TETs), macrolides, lincomycin, and others. 10
Vancomycin (VAN) has been employed as the first-line antibiotic for MRSA and most MRSA are sensitive to VAN. 11 However, the burden caused by vancomycin intermediate-resistant S. aureus (VISA) is relatively high, and vancomycin-resistant S. aureus (VRSA) strains are being found more frequently. 12,13 The emergence of resistance to VAN is the most feared circumstance in S. aureus to date. Resistance to the more recently introduced antibiotics, linezolid (LZD) and daptomycin, also has been found in MRSA. 14,15 Given this complex pattern of resistance, which medicines should be prescribed for VISA, VRSA, and even the superbugs resistant to all the antibiotics that may appear in the future? This presents an urgent problem to find effective antimicrobial agents to treat MRSA infection. 16
To discover novel drugs or tool compounds targeting the MDR S. aureus strains, we applied the 2-(3-(2-methoxy-4-nitrophenyl)-2-(4-nitrophenyl)-2H-tetrazol-3-ium-5-yl) benzenesulfonate sodium salt (EZMTT) method to perform a high-throughput screening (HTS) of our own laboratory compound library. 17,18 Furthermore, based on the HTS results, we designed and synthesized a selen-containing gemcitabine (Compound 3 in Fig. 3). Compound 3 showed potent antibacterial effect for both sensitive and MDR S. aureus strains, and more in favor of the resistant strain.
MATERIALS AND METHODS
Reagents, cells, and chemical compounds
Staphylococcus aureus and MRSA strains (MRSA-CYZH, MRSA-XHX, MRSA-ZHF are the ID number of the strain) were obtained from the strain collection from Zhejiang provincial people's hospital; EZMTT was from JNF Bioscience, Inc., (Hangzhou, China). Ciprofloxacin (CIP), FOX, rifampicin, VAN, OXA, levofloxacin (LFX), moxifloxacin (MFX), tetracycline (TET), erythromycin (ERY), and penicillin G (PEN) were purchased from Shanghai Yuanye Biotechnology Co., Ltd; cation-adjusted Mueller–Hinton broth (CAMHB) was purchased from Beijing Solarbio Science & Technology Co., Ltd. Gemcitabine and other chemicals were from Sigma-Aldrich (China). The 500-compound library was our laboratory collections of selen or selenyldiazo compounds 17,18 and some commercial compounds.
AST of S. aureus by the EZMTT broth microdilution method
Freshly cultured bacteria colonies were selected from Mueller–Hinton agar plates and diluted to 0.5 McFarland concentration with sterilized saline, followed by a 200-fold dilution using CAMHB medium containing 1 × EZMTT reagent (bacteria were diluted 1000-fold in the same way as in the standard microdilution method). Then the bacterial suspensions (100 μL) were added to a 96-well plate containing a series dilution of compounds (or antibiotics), and the cells were cultured at 35°C–37°C.
After 16–24 h, the absorbance at 450 and 600 nm was measured (the antimicrobial susceptibility growth curves of bacteria were measured every hour for 24 h) (Table 1). For comparison, cultures without the compound added or without the bacteria added were carried out as control under the same conditions, and minimum inhibitory concentration (MIC) values were calculated from the data.
HTS Assay Protocol
1. Compounds were stocked in DMSO and diluted with DMSO to 10 mM, 2 mM, and 400 μM. Then 1 μL of each concentration was added to a 96-well plate.
2. One microliter of DMSO was added to a 96-well plate for control.
3. Freshly cultured bacteria colonies were selected from Mueller–Hinton agar plates and diluted to 0.5 McFarland concentration with sterilized saline.
4. EZMTT reagent was diluted 200 × in CAMHB medium.
5. The bacteria cells suspension diluted 200-fold using CAMHB medium containing 1 × EZMTT reagent.
6. Two hundred microliters CAMHB medium was added to a 96-well plate for blank.
7. Plates were lidded and incubated for 24 h at 37°C until read.
8. Inhibition % = (ODcontrol−ODcompound)/(ODcontrol−ODblank) × 100%.
CAMHB, cation-adjusted Mueller–Hinton broth; DMSO, dimethyl sulfoxide; EZMTT, 2-(3-(2-methoxy-4-nitrophenyl)-2-(4-nitrophenyl)-2H-tetrazol-3-ium-5-yl) benzenesulfonate sodium salt; OD, optical density.
Chemical synthesis of selen compounds
Chemical synthesis of Compound 2: Compound 1 (0.52 g, 1.06 mmol) was dissolved in dry tetrahydrofuran (THF) (6 mL) and treated with N, N-diisopropylethylamine (0.41 g, 3.18 mmol). The resulting mixture was added to the selenium chloride compound in dry THF (1.5 mL) in a 50 mL flask in ice bath. After 10 h reaction under the protection of N2 at room temperature, the completion of the reaction was confirmed by high performance liquid chromatography (HPLC). After chromatographic purification, a beige solid product of Compound 2 was obtained (0.4 g, 92% in yield).
Compound 2 (0.3 g, 0.4 mmol) was then dissolved with dry THF (1 mL) in a 50 mL flask and treated with 1 M HCl/ethyl acetate in ice bath and for 6 h at room temperature. The completion of reaction was monitored by TLC. The reaction solution was concentrated and purified by column chromatography (dichloromethane: MeOH = 30:1). After chromatographic purification, a white solid product of Compound 3 (0.2 g, 94% in yield) was obtained.
Compound 3 (selen–gemcitabine) is a white solid (99% purity). 1 H NMR (500 MHz, dimethyl sulfoxide [DMSO]) δ 8.35 (d, J = 7.5 Hz, 1H), 8.06 (d, J = 8.0 Hz, 1H), 7.92 (d, J = 7.8 Hz, 1H), 7.79–7.71 (m, 2H), 7.47 (t, J = 7.5 Hz, 1H), 6.35 (d, J = 6.5 Hz, 1H), 6.20 (t, J = 7.3 Hz, 1H), 5.35 (t, J = 5.4 Hz, 1H), 4.29–4.14 (m, 1H), 3.92 (dt, J = 8.5, 2.8 Hz, 1H), 3.83 (d, J = 9.2 Hz, 2H). MS [M+H]+ m/z: = 446. 13 C NMR (101 MHz, DMSO) δ 166.95, 162.64, 153.99, 145.31, 140.37, 134.64, 129.72, 128.68, 126.92, 126.47, 123.44 (t, J = 257.6 Hz), 96.54, 84.74 (t, J = 30.3 Hz), 81.60, 68.74 (t, J = 22.2 Hz), 59.22. high-resolution mass spectroscope: 446.00613 [M+H]+. Single spot on TLC (CH2Cl2/CH3OH = 10:1; R f = 0.3), and the purity was analyzed by HPLC.
RESULTS
EZMTT method greatly enhanced the sensitivity of the AST assay
The standard microdilution broth method is a commonly used turbidity-based AST method and the bacteria growth is measured using the broth absorbance at the wavelength between 600 and 750 nm. However, the turbidity method is not sensitive enough to detect lower level resistance in bacteria, such as heteroresistance. To enhance the sensitivity of the turbidity method, we developed an EZMTT-based microdilution method; a mixture of the EZMTT reagent and bacteria (instead of bacteria only) was added to a microplate according to the standard microdilution broth method as recommended by Clinical and Laboratory Standards Institute (CLSI). In our previous study, it has demonstrated that the EZMTT reagent can amplify the viability signal of cell growth. 18
The sensitivity of the turbidity and the EZMTT methods was compared by the bacterial growth signal, and the reproducibility was evaluated by the Z factor. As shown in Figure 1, the signal-to-noise ratio of the EZMTT method is approximately five times greater than the turbidity method, and the Z factor of EZMTT method is much better than that of the turbidity method. This indicates that the EZMTT method for S. aureus is extremely sensitive.

The Z factors of the
The results of the EZMTT method are consistent with those of the VITEK method
The MDR S. aureus strains isolated from clinic were initially identified as MRSA (FOX-resistant S. aureus) by VITEK 2 Fox Card, as given in Table 2. Three strains were found to be both OXA and FOX resistant. MDR was defined as acquired nonsusceptibility to at least one agent in three or more antimicrobial categories, XDR was defined as nonsusceptibility to at least one agent in all but two or fewer antimicrobial categories (i.e., bacterial isolates remain susceptible to only one or two categories). 19
Antibiotic Susceptibility Testing Assignment of Clinical Isolated Staphylococcus aureus by the VITEK Card Method and EZMTT Method
Staphylococcus aureus shows cefoxitin (FOX) or oxacillin (OXA) resistance is defined as MRSA. The gray shades in the Table 2 indicate that three clinic isolated Staphylococcus aureus strains are MRSA.
CIP, ciprofloxacin; ERY, erythromycin; FOX, cefoxitin; LFX, levofloxacin; LZD, linezolid; MFX, moxifloxacin; MRSA, methicillin-resistant Staphylococcus aureus; OXA, oxacillin; PEN, penicillin G; TET, tetracycline; VAN, vancomycin.
The AST of these 3 MRSA strains for the 10 antibiotics showed XDR, resistant to 8 antibiotics (FOX, OXA, PEN, CIP, LFX, MFX, TET, and ERY), and sensitivity to only 2 antibiotics (LZD and VAN). However, ATCC25923 was found susceptible to all of these tested antibiotics. The broad range of ineffective antibiotics including penicillin, cephalosporin, fluoroquinolones, TET, and macrolides, indicating that there are fewer options to treat infections caused by these strains. The optimized EZMTT method showed essentially the same AST results as the VITEK Card method, as given in Table 2. This indicates that the EZMTT method for S. aureus is not only sensitive but also reliable.
The AST results (S, susceptible; I, intermediate; R, resistance) were determined according to the MIC breakpoints given by the CLSI microdilution method. The breakpoints are listed as follows: OXA (≤2 μg/mL S; ≥4 μg/mL R); CIP (≤1 μg/mL S; 2 μg/mL I; ≥4 μg/mL R); FOX (≤4 μg/mL S; ≥8 μg/mL R); LZD (≤4 μg/mL S; ≥ μg/mL R); ERY (≤0.5 μg/mL S; ≥8 μg/mL R); VAN (≤2 μg/mL S; 4–8 μg/mL I; ≥16 μg/mL R); LFX (≤1 μg/mL S; 2 μg/mL I; ≥4 μg/mL R); MFX (≤0.5 μg/mL S; 1 μg/mL I; ≥2 μg/mL R); TET (≤4 μg/mL S; 8 μg/mL I; ≥16 μg/mL R); and PEN (≤0.12 μg/mL S; ≥0.25 μg/mL R).
Selen derivatives were found to have antimicrobial activity by HTS
Using the optimized EZMTT assay, we screened our compound library using the MRSA-CYZH strain. As shown in Figure 2A of the >500 compounds screened at 50, 10, and 2 μM concentrations, 10 compounds showed good inhibition activity (MIC values ≤2 μM), these compounds are gemcitabine and selen derivatives (in circle in Fig. 2A), such as ebselen, hexylselen, and propylselen (Fig. 2B) and appear to be the top hits.
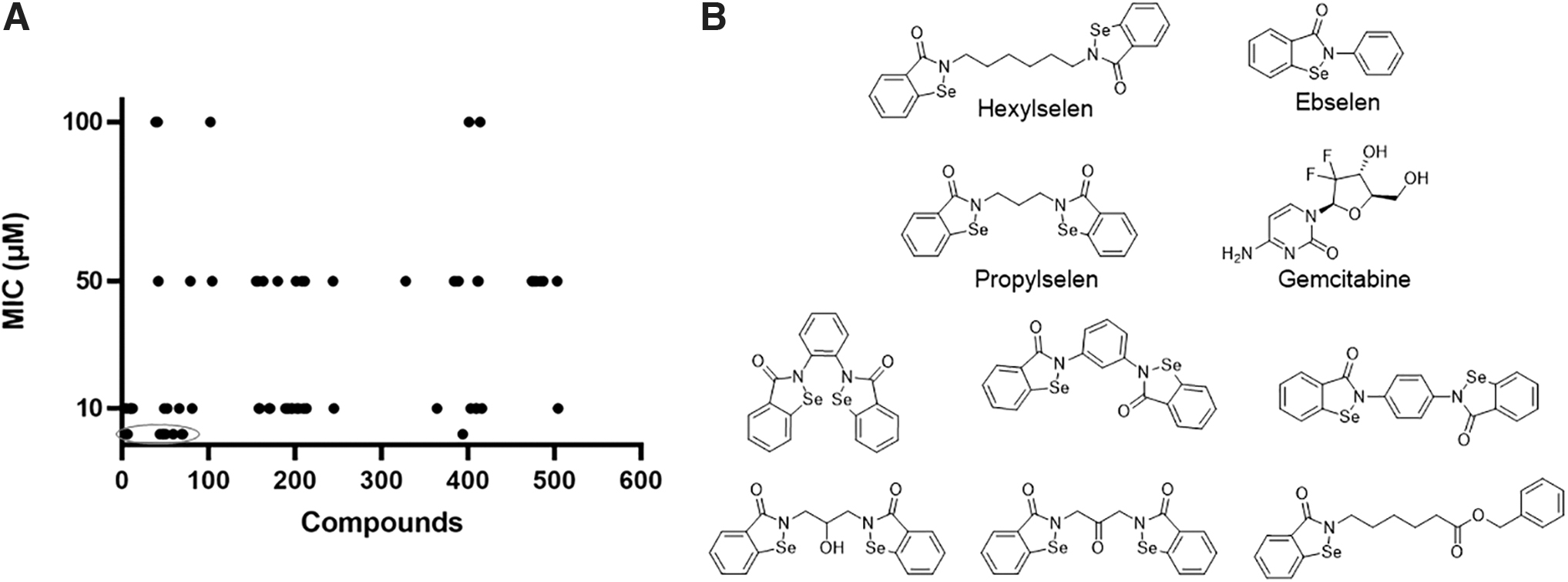
The HTS was performed with EZMTT method using compound library.
Gemcitabine–selen derivative showed antibacterial activity against MDR S. aureus
Ebselen has been reported previously to have antimicrobial activity in MRSA and other strains, 20 –25 as well as having a synergistic antibacterial effect on MDR gram-negative bacterial infections together with Ag ions. 26 The selen derivatives were found as potent mitochondrial glutamate dehydrogenase (GDH) inhibitors in our previous studies. 17 Gemcitabine (2′,2′-difluoro 2′-deoxycytidine), a new cytidine analogue, is a DNA polymerase inhibitor that has become a broad-spectrum antitumor and antiviral drug. 27
Therefore, we were interested whether a combination of selen and gemcitabine, a new type of selen-containing gemcitabine that targets both DNA polymerase and mitochondrial GDH, would be a better inhibitor. We then designed and synthesized a class of new selen compounds by converting the amino group of gemcitabine to a 1,2-benzoisoselenazol-3(2H)-one moiety. 28 The structure of Compound 3 is shown in Figure 3.

The chemical synthesis of selen–gemcitabine (Compound 3). Selenium chloride reacts with Compound 1 in the presence of DIPEA at room temperature to give Compound 2. TBS deprotection of Compound 2 by HCl to give Compound 3 (the selen–gemcitabine). DIPEA, N, N-diisopropylethylamine; TBS, tert-butyl dimethyl.
In vitro antimicrobial activity testing results showed that Compound 3 exhibited stronger antimicrobial activity than Ebselen against MDR MRSA bacteria with MIC values of 0.07–1.0 μM (as given in Table 3). Interestingly, the selen–gemcitabine showed more potent activity than gemcitabine in inhibiting the growth of ATCC25923, MRSA-XHX, and MRSA-ZHF (Fig. 4). However, the activity of selen–gemcitabine to ATCC29213 and MRSA-CYZH is much lower than that of gemcitabine. The enhanced antibacterial activity might be attributed to the inhibition of both targets that ebselen and gemcitabine inhibited in S. aureus, and the mechanism will be investigated in future studies.
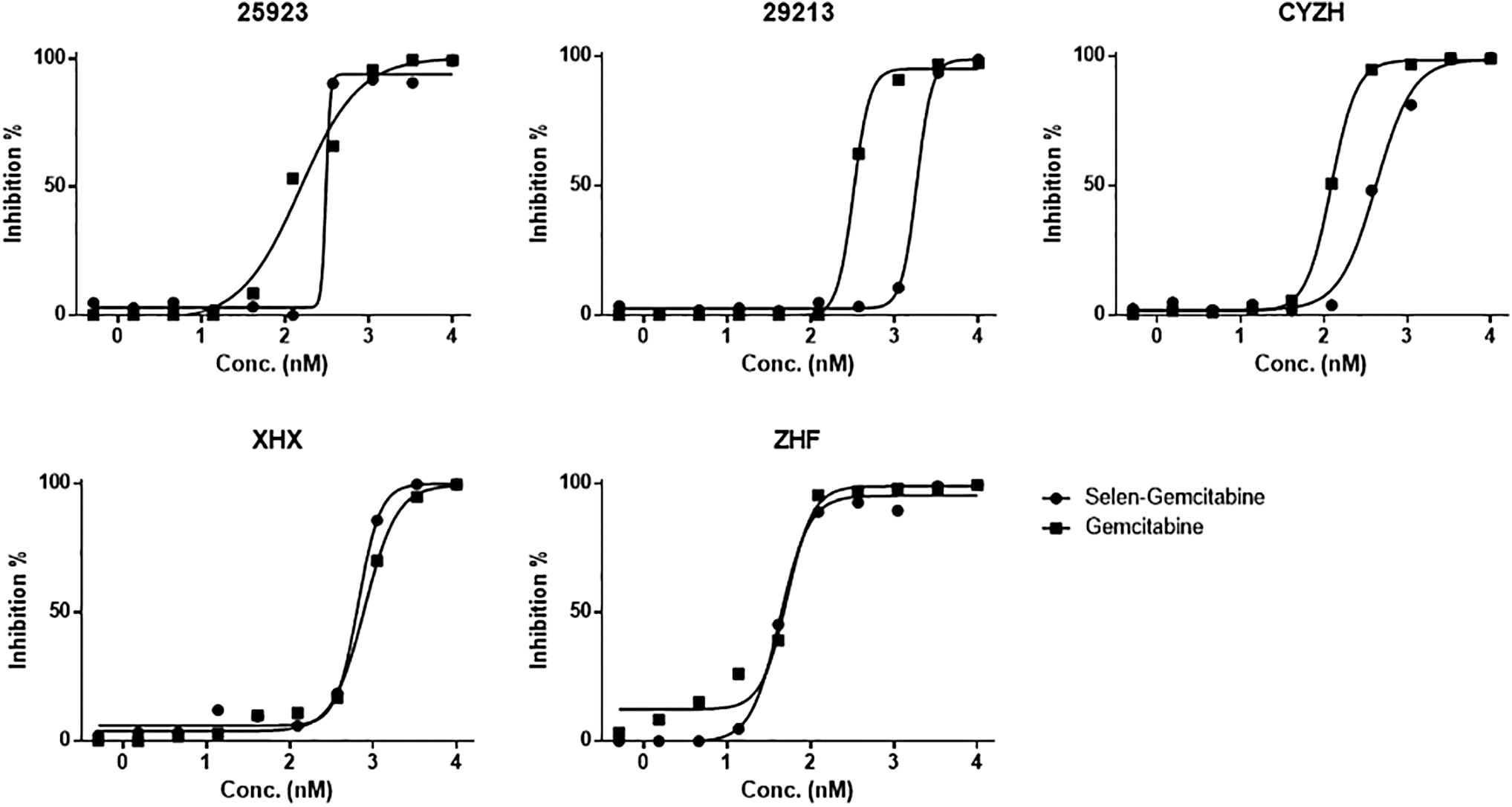
Comparison of IC50 curves between gemcitabine and selen–gemcitabine.
The Minimum Inhibitory Concentration (μM) of Gemcitabine and Its Derivatives Against Staphylococcus aureus
DISCUSSION
MRSA is one of the common pathogenic bacteria in clinic, and can cause a series of different degrees of infection, and even life threatening. 5,6,10,11 There are all kinds of antibiotics for treatment of MRSA including penicillin, cephalosporins, macrolides, aminoglycosides, TET, glycopeptides, and so on, and VAN has been employed as the first-line antibiotic for MRSA. 16 However, due to the abuse of antibiotics, MRSA strains have further developed MDR or XDR, and VRSA strains are being found more frequently. 12,13 Finding effective antimicrobial agents to treat MRSA infection has become an urgent need in clinic. More sensitive detection of resistance and the development of new antibiotics are ways to overcome this problem.
The standard microdilution broth method is a commonly used turbidity-based AST method and is more convenient and cheaper than the VITEK card method. However, the sensitivity of the turbidity method is unsatisfactory for the detection of lower level resistance in bacteria, especially for the heteroresistance that may further transition to completely resistant. 29 So the precise and sensitive AST for the rapid screening effective agent is crucial. To enhance the sensitivity of the turbidity method, we optimized an EZMTT-based microdilution method that mixed the EZMTT reagent and bacteria into a microplate.
It demonstrated that the EZMTT reagent can amplify the viability signal of bacteria, 30 and the EZMTT method can detect as low as a single S. aureus cell after 24 h incubation, and the reproducibility of the method is much higher than the traditional turbidity method with Z factor being 0.95 versus 0.53. The AST result is consistent with that of the microdilution broth method as defined by CLSI and the VITEK method. So the EZMTT method can be used for antimicrobial HTS of antibiotics or chemotherapy agents.
The three MRSA strains isolated from clinic patients showed MDR or XDR, and resistant to almost all commonly used antibiotics. The novel mechanisms of action of antibiotics may overcome its resistance. By HTS of our laboratory's compound library with the EZMTT method, it was found that Ebselen and its derivatives, as well as gemcitabine, have good antibacterial activity against these MDR or XDR MRSA strains. Ebselen, a selen compound, has been reported previously to have antimicrobial activity in MRSA and other strains, 20 –26 as well as for the MDR bacterial infections.
In our previous studies, Ebselen and its derivatives were found as potent mitochondrial GDH inhibitors. 17 GDH plays an important role in maintaining energy metabolism and homeostasis in mammalian cells and also have a role in drug resistance in bacteria. 31 –33 As a cytidine analogue by inhibiting DNA polymerase, gemcitabine was reported to have a broad-spectrum antitumor and antiviral activity. 27 Therefore, we designed and synthesized a selen-containing gemcitabine to investigate if the compound could target both DNA polymerase and mitochondrial GDH to show improved antibacterial activity, especially for these MDR and XDR MRSA.
By converting the amino group of gemcitabine to a 1,2-benzoisoselenazol-3(2H)-one moiety, we obtained a selen-containing gemcitabine Compound 3. As we expected, Compound 3 showed potent antibacterial activity against the clinical S. aureus strains, especially for the XDR MRSA in vitro. Among the three compounds tested (Table 3), Compound 3 showed the best activity against ATCC25923, MRSA-ZHF, and MRSA-XHX. However, Compound 3 did not show improved activity against ATCC29213 and MRSA-CYZH.
Gemcitabine undergoes a series metabolism in cells and thus provided a broad-spectrum antitumor and antiviral activity. 27 When the amine group of gemcitabine was derivatized with selen (Compound 3), it might block a gemcitabine metabolite formation that is important to inhibit a certain target of S. aureus. However, further investigation is required to understand the mechanism of action of Compound 3.
CONCLUSIONS
In summary, we applied both the EZMTT and VITEK methods to perform the AST of several clinically isolated S. aureus strains, and interestingly, the OXA- and FOX-resistant MRSA strains showed MDR and XDR. A brief HTS screening in our laboratory's compound library showed that hexylselen, ebselen, propylselen, and gemcitabine are good inhibitors of clinical MRSA strains. In addition, we designed and synthesized a novel selen-containing gemcitabine by converting the amino group of gemcitabine to a 1,2-benzoisoselenazol-3(2H)-one moiety in three steps with 86.5% overall yield.
Gemcitabine and its selen derivative showed potent antibacterial activity against the clinical S. aureus strains, especially for the XDR MRSA. Therefore, Compound 3 provides a new group of chemicals that can be used as a lead compound for future discovery of new antibiotics or tool compounds to treat or investigate the mechanism of MDR in S. aureus strains.
Footnotes
AUTHORS' CONTRIBUTIONS
B.H.R. and Z.C. designed the study; Z.C., J.L., Y.W., R.B., W.W., X.G., D.L., Y.L., carried out experiments about EZMTT; and Q.H. provided the clinical strains and VITEK card results.
DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
We acknowledge the financial support from Fuyang government innovation grant (H1160200772).