
Abstract
Abstract
Regulatory human health risk assessment of chemicals ideally requires integration of toxicokinetic absorption, distribution, metabolism, and excretion where the respiratory system is a principal exposure route and threshold site for absorption. This study evaluated the permeability capacity of an in vitro human airway epithelium cell model (MucilAir™). Initially, definition of the in vitro method, including development of standard operating procedure confirmation of transferability and assurance of reproducible performance, was established in a preliminary phase involving two independent laboratories using six chemicals (propranolol, atenolol, nicotine, cadmium dichloride, cobalt chloride, and ammonium hexachloroplatinate). A follow-up investigation of method relevance, measuring relative permeability of 30 chemicals, in 1 laboratory is also reported. Absorption through the lung barrier model was determined as apparent permeability coefficient (Papp) following apical and basolateral exposure to nontoxic concentrations. Papp was calculated from chemical concentrations crossing the cell barrier at appropriate time intervals. Comparative permeability of nasal and bronchial epithelium is also reported. Overall, the results demonstrate that MucilAir is an effective barrier model for assessing the permeability of different classes of compounds across the human airway epithelium. Results indicate a generally higher permeability of the airway epithelium for organic compounds compared to inorganic chemicals, with a low-protein-mediated efflux as permeability mechanism. The in vitro test system provides a robust and transferable method for determination of pulmonary absorption, relevant to toxicokinetic modeling and integration into risk assessment of chemicals.
Introduction
C
However, effective prediction of systemic toxicity of chemicals based on in vitro tests is severely limited due to the complexity of physiological reality. Nevertheless, the combination of in vitro methodology and related computer simulation allows improved evaluation of systemic toxicity by integration of relevant factors.4,5 Moreover, toxicokinetics then becomes essential to the development of applicable in vitro alternatives with reliable predictive capacity for human health risk assessment. 7
Absorption is the threshold step of ADME following inhalation, with exposure to the nasal cavity, trachea, and lung tissue (bronchi, bronchioles, and alveoli), including respiratory tract epithelia with characteristic morphology. 8 Nasal absorption may be significant for labile chemicals 9 also correlated to particle size. 10 Consistent with this, the upper airways are generally the absorption sites for microbial infections, and so on.
Available in vitro models for components of the pulmonary system are mainly based on cell lines derived from adenomas, where, although retaining numerous in vivo functions (e.g., beating cilia and mucus secretion), they are not usually cocultured in their natural context, adjacent to smooth muscle cells or immune cells. 11 Also, the potency of cell models to produce certain mucus constituents or surfactant proteins may not be well characterized. 12
Current, in vitro models for lung translocation of chemicals comprise pulmonary epithelial cell lines (e.g., Calu-3 and A549) and primary lung cells, of either human or animal origin (e.g., primary type II pneumocytes). Some coculture systems are available (e.g., with pneumocytes, alveolar macrophages, mast cells, and endothelial cells) for study of lung chemical absorption, 13 but morphology differences such as surface area, cellular variety, and lining composition (e.g., mucus and surfactant) may influence uptake.14,15 Nevertheless, these types of in vitro models have been used to study the translocation of particles 16 and could also be applicable to absorption studies more generally. 17 However, in vitro systems incorporate active metabolizing enzymes causing parallel metabolism. Moreover, culture conditions present an influential factor in absorption assessment. For example, permeability to sodium fluorescein of the bronchial Calu-3 cell line has been found to change when a liquid–liquid system was used to replace an air–liquid culture. The use of cocultures or primary cells, having closer similarity to the native phenotype, would alleviate the limitations of monoculture cell models. 18 For the upper respiratory tracts, in vitro cell culture models of human nasal epithelium based on primary culture technologies have proven relevant for permeability assessment. However, uncertain source availability of reliable human tissues remains a factor-limiting application of the in vitro nasal cell culture model. 9 For integrity evaluation of these types of cell monolayer models, the transepithelial electrical resistance (TEER) can be measured using fluorescein, 14 C-mannitol, and so on.
Another toxicokinetic consideration is bioavailability postinhalation exposure, characterized by chemical release from its matrix with absorption and metabolism of the released fraction before reaching the systemic circulation.19,20 While bioavailability thus depends mainly on the matrix, absorption and metabolism depend more on chemical properties and physiology. 12 Such models, using artificial lung fluid as matrix, are designed to determine pulmonary absorption after inhalation exposure, applicable to nanoparticles, fibers, and various metals. 21
The project described here investigated an in vitro lung barrier system, representative of the nasal human airway epithelium, potentially suitable for absorption studies, aiming to establish threshold values for apparent permeability coefficient (Papp). In this study, a 3D model of fully differentiated human airway epithelium was used (MucilAir™ provided by Epithelix Sàrl, Geneva). 22 MucilAir closely mimics the morphology and function of native human tissue, allowing assessment of upper airway permeability of inhaled compounds. 23 Measurement of Papp for selected chemicals across the MucilAir airway epithelium would be an indicator of uptake by absorption relevant to integration into toxicokinetic modeling.
Materials and Methods
Test system
Primary human cells isolated from the nasal cavity, trachea, and bronchus were received as reconstituted, fully differentiated epithelia in transwells of 6.5 mm of diameter, with a pore size of 0.4 μm (Costar 3470; Corning Incorporated) from Epithelix Sàrl (Geneva, Switzerland). Each epithelium containing about 400,000 cells was cultured at air–liquid interface conditions in a humidified atmosphere in a standard tissue culture incubator (37°C and 5% CO2) according to the provider's protocol. Briefly 700 μL of the basolateral, chemically defined, and serum-free medium (MucilAir serum-free culture medium, provided by Epithelix Sàrl, Geneva, Switzerland) was changed every 2–3 days. With the arrival of the cells, quality checks with each transwell were performed by light microscopy. The epithelia were evaluated on cilia beating, presence of mucus on the cell surface, and their cell morphology. Furthermore, after 7 days in culture, TEER measurements were performed to check the barrier integrity of the epithelia.
Test items
Both inorganic and organic compounds were selected for the permeability tests. Different selection criteria such as the availability of in vivo or in vitro toxicokinetic (absorption via inhalation) data, high solubility in water and saline buffers, and the availability of analytical in-house methods were considered in the choice of suitable compounds. All compounds were obtained from Sigma Aldrich, except oxazepam, which was from Lipomed AG, phenobarbital from Fluka, S-nicotine from Alfa Aesar, and levemedetomidine from TCM (Toronto). For the first experimental phase, three organic compounds (propranolol, atenolol, and nicotine) and three inorganic compounds (cobalt chloride, cadmium chloride, and ammonium hexachloroplatinate) were selected. Stock solutions were prepared by dissolving the compounds in Hank's Balanced Salt Solution (HBSS) at the concentrations of 10 mM of propranolol and nicotine and 0.5 mM of atenolol. All the working solutions were prepared freshly and applied to the in vitro model at a concentration of 100 μM in HBSS. For the second experimental phase, the stock solutions of the compounds were prepared in dimethyl sulfoxide (DMSO) at a concentration of 20 mM and subsequently diluted with HBSS to a final concentration of 100 μM. For the comparative permeability study between nasal and bronchial cultures, stock solutions of salicylic acid were prepared in DMSO at 100 mM and subsequently diluted with HBSS to a final concentration of 1 mM.
Experimental design
The absorption of chemicals through the lung barrier was analyzed after apical or basolateral treatments. To confirm that the passage of the chemicals (absorption) occurs due to passive diffusion and not due to chemical toxicity and secondary barrier damages, a barrier integrity assay has been performed for each tested compound, before being used in the permeability experiments. The barrier integrity was evaluated by measuring the TEER and the permeability for Lucifer yellow (LY; a fluorescent compound) in the presence of tested item. Further on, for the permeability assessment, the compounds were applied at known concentrations and the passage was registered in two directions—apical to basolateral (A-B) and basolateral to apical (B-A)—by measuring the initial and final concentrations in the donor compartment and the intermediate concentrations (at different time intervals) in the acceptor compartment (Fig. 1). A ratio of the Papp coefficient values (asymmetry index) was calculated and the involvement of P-glycoprotein (P-gp)-mediated efflux mechanism was concluded if the B-A/A-B ratio is >1.5.24,25 The in vitro method using airway epithelium MucilAir was first evaluated in one laboratory (EURL ECVAM or European Union Reference Laboratory for Alternatives to Animal Testing) by assessing the permeability for three inorganic compounds (cadmium dichloride, cobalt chloride, and ammonium hexachloroplatinate). After the method was well established, its transferability was evaluated by transferring the test method's standard operating procedures (SOPs) to the second laboratory involved in the project (Pharmacochemistry Department at University of Geneva). Following the transferability step, we were able to evaluate also the interlaboratory reproducibility of the method. For this, three organic compounds were selected (propranolol, atenolol, and nicotine) and the Papp and asymmetry index values obtained in each laboratory were finally compared.
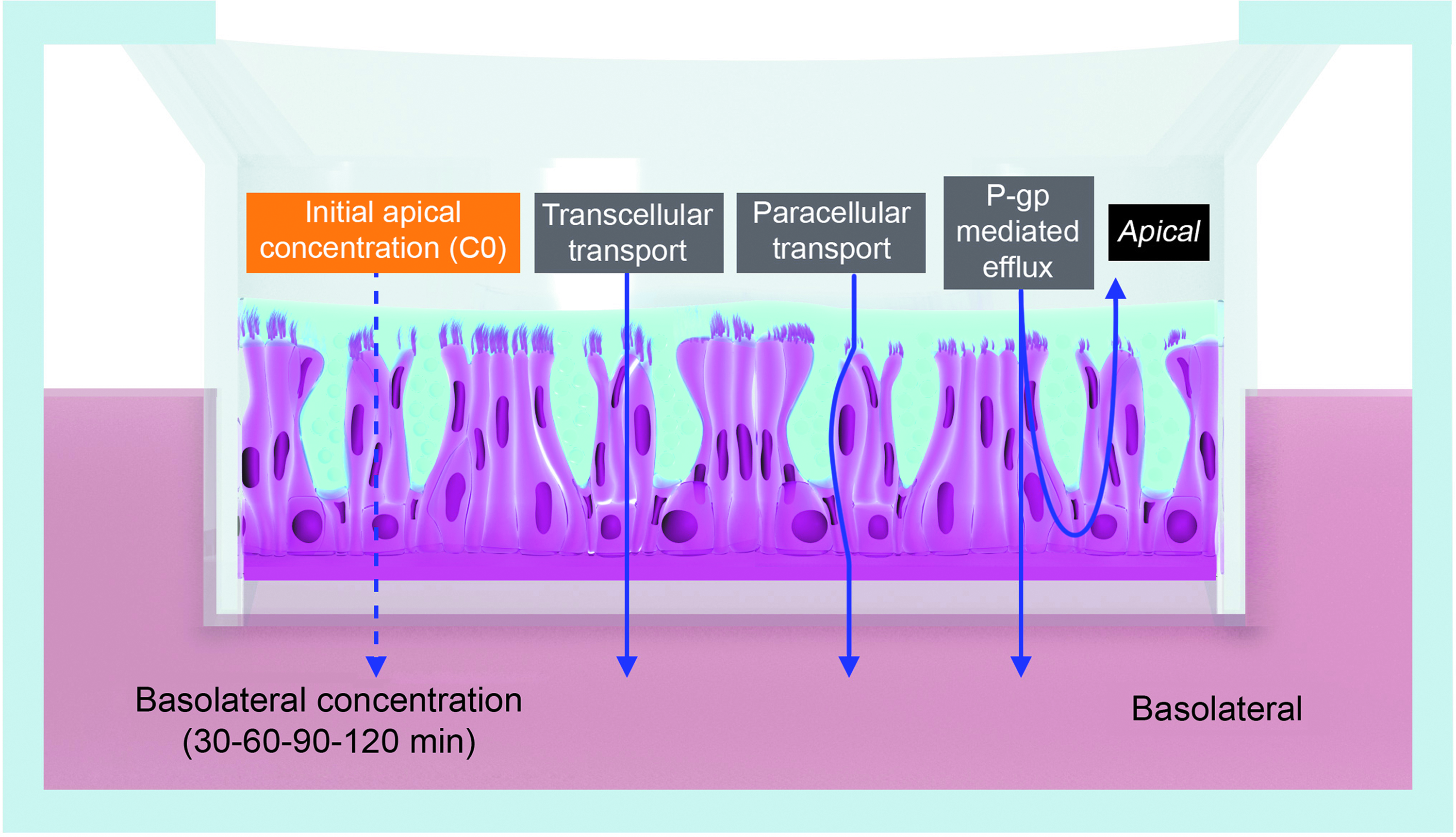
Schematic representation of the A-B permeability procedure using the airway epithelial model. The tested compounds are added in the apical compartment and then the concentrations in the basolateral compartment are measured at different time point intervals up to 2 hours. A-B, apical to basolateral; P-gp, P-glycoprotein.
In the second experimental phase, a panel of 30 organic and three inorganic compounds were used to evaluate the developed SOP and, in particular, its ability to rank relative permeability. A last part of the study was dedicated to shed light on potential differences in permeability due to anatomical origin comparing permeability of salicylic acid on nasal and bronchial reconstituted epithelia.
Barrier integrity
The barrier integrity assay was conducted to establish a nontoxic working concentration for the test solutions, which were used for permeability testing. Therefore, barrier integrity was monitored by measuring the permeability of the highly fluorescent dye LY. LY, which represents a positive control for paracellular transport mechanism, was tested in the presence and absence of test compounds. For the inorganic compounds, barrier integrity testing was conducted in A-B direction. For the organic compounds, the experiments were carried out in A-B as well as in B-A direction. The experiments were performed in six different epithelia and the results were compared with 6 epithelia used as negative controls (LY in absence of test item). For integrity testing, the apical compartment was either filled with 250 μL of HBSS or with LY in HBSS (100 μM) with or without the test item. The basolateral compartment was filled with 500 μL of the LY solution with or without test item or with HBSS. After 30, 60, 90, and 120 minutes of incubation at 37°C in a humidified 5% CO2/95% air atmosphere, 200 μL of the buffer from the basolateral and 100 μL from the apical side were sampled and replaced by the same volume of fresh and prewarmed at 37°C buffer. The LY, which was able to cross the barrier, was quantified by measuring the fluorescence intensity at 428 nm excitation and 540 nm emission using a fluorescence plate reader (TECAN Infinite M200; TECAN Austria GmbH, Grödig, Austria). Moreover, the TEER values of the epithelia before (T0 minutes) and after exposure (T120 minutes) were recorded as described below to check if the test compounds affect the barrier.
TEER measurements
For the TEER measurements, the basolateral and apical compartments of the transwells were filled with 500 μL and 250 μL of prewarmed HBSS (HBSS with sodium bicarbonate, without phenol red) at 37°C. After a 5-minute lasting adaption period of the epithelium to the buffer conditions, the TEER was measured using an EVOM (epithelial tissue volt-ohmmeter) and STX2 electrodes (World Precision Instruments, Sarasota, FL). The TEER was calculated by subtracting the resistance of a cell-free culture insert and the membrane surface according to the following formula:
Permeability assessment
The absorption experiments were performed with 6 MucilAir epithelia per experiment in the A-B and B-A direction. Before the permeability testing, the epithelia were rinsed once with prewarmed HBSS by filling the basolateral compartment with 700 μL of HBSS per well. For the transport studies in (A-B) direction, each of three inserts was filled with 500 μL of warm HBSS (at 37°C) in the basolateral compartment and 250 μL of the prewarmed test compound (100 m μM in HBSS) in the apical compartment. For B-A direction, the apical compartment was filled with 250 μL of HBSS, while the basolateral compartment was containing 500 μL of buffer. The inserts were incubated while shaking the plate at ±70 rpm by plate shaker at 37°C in a humidified 5% CO2/95% air atmosphere. A sample volume of 200 μL was from the acceptor compartment after 30, 60, 90, and 120 minutes and replaced with the same volume of fresh, prewarmed HBSS. At T120 minutes, also 200 μL of the apical solution (donor compartment) was sampled and considered as Tfinal. Aliquots of the initial solutions were analyzed to establish the test item concentration at T0. The samples were stored at room temperature until the end of the experimental time and then analyzed.
Analytical methods
The inorganic compounds were analyzed by a module of HPLC (sampling) and inductively coupled plasma mass spectrometer (ICP/MS/MS) (detection) techniques, through which the HPLC was only used for automated sample injection and not for sample separation. The system composed of HPLC Perkin-Elmer Series 200 equipped with a biocompatible quaternary pump of titanium, needle injector out of titanium/iridium, and a 10 μL sample loop in PEEK, as well as an ICP/MS Perkin-Elmer SCIEX ELAN DRC II and TotalChrom 6.2 software for data processing.
At the EURL ECVAM test facility, the organic compounds were analyzed by a module of HPLC and triple quadrupole mass spectrometer (TQMS) detection techniques. The system composed of HPLC WATERS® Alliance HT 2795 equipped with a 10 μL sample loop, a TQMS Micromass Quattro Ultima, and WATERS MassLynx V.4.1 software for data processing. Two reverse-phase C18 columns (WATERS Symmetry® C18 3.5 μm; WATERS XTerra™ MS C18, 3.5 μm) were used for the analysis of propranolol, atenolol, and nicotine. For propranolol quantification, a mobile phase consisting of 80% acetonitrile, 20% water, 20 mM ammonium acetate, and 0.1% acetic acid at a flow rate of 200 μL/min was used. Water (A) and methanol (B) were mobile phases for atenolol. A linear gradient was set from 50% A to 70% A in 6 minutes and then maintained at 70% for 1 minute. The flow rate was 100 μL/min. A mobile phase consisting of 80% water and 20% acetonitrile was used for the determination of nicotine at a flow rate of 500 μL/min.
At the University of Geneva, the three organic compounds were analyzed by a WATERS Acquity UPLC coupled to a TQMS. The injection was performed with a 5 μL sample loop and data processing by means of the MassLynx V.4.1 software. For the quantification of propranolol and atenolol, a C18 column (Acquity UPLC®BEH 1.7 μM 2.1 × 50 mm) was used. Nicotine was analyzed by both the column mentioned above and an Acquity UPLC®BEH HILIC (1.7 μM 2.1 × 50 mm) column.
Data analysis and statistics
The apparent permeability coefficient (Papp; cm/sec) is an index calculated from the amount of compound transported per time, and the transport surface and is determined according to the following equation:
Where A is surface area of the filter, C0 initial concentration of chemical in the donor fluid, and dQ/dt the amount of compound transported per time.
The asymmetry index (or the efflux ratio) is defined as the quotient of the secretory permeability (B-A) and the absorptive permeability (B-A) and was calculated according to the following equation:
The mass balance (recovery) is defined as the sum of the drug recovered from the acceptor chamber and the drug remaining in the donor chamber at the end of the experiment, divided by the initial donor amount. It is calculated as follows:
Where CD and CR are the concentrations on the donor (D) and receiver (R) sides of the monolayer at the start (0) or end (fin) of the experiment, CS(t) denotes the concentrations of the samples withdrawn at different time points, t, and V is used for each of the respective volumes.
Data are expressed as mean ± standard deviation (SD) of three technical replicates. Statistical analysis was performed using Student's t-test via GraphPad Prism software. A p-value <0.05 was considered to be statistically significant.
Results
Quality control of airway epithelia
A qualitative control (by light microscopy) was performed for each batch of airway epithelia before using the tissues for barrier integrity and permeability experiments. The parameters observed were cilia beating, presence of mucous on the cell surface, cell morphology, and the presence/absence of liquid in the apical compartment. These parameters were used to eventually exclude damaged epithelia and to have a fast evaluation of tissue morphology.
Further on, a quantitative control was performed after 7 days of recovery in culture conditions by measuring the TEER. The average of 22 batches used for the study TEER was 521.17 Ω*cm2 (±66.53). The maximum value was 1046 Ω*cm2 (±175), while the minimum TEER value registered was 239 Ω*cm2 (±62). As the exclusion criterion for TEER was 100 Ω*cm2, all received epithelia were qualified for further use in barrier integrity and permeability experiments.
Barrier integrity assessment
Airway epithelia were exposed in the apical compartment to selected inorganic or organic compounds to evaluate possible barrier damages due to the tested compounds and to select a nontoxic concentration for absorption assessment. Two physiological parameters were registered and compared with the nontreated epithelia (controls). TEER was registered before and 2 hours after exposure and the results did not show any significant change after exposure to selected concentrations. In both experimental conditions (treated and not treated), LY was also added to the tested solution to measure the permeability changes of epithelia over 2 hours of exposure. The LY passage was evaluated by comparing fluorescence intensity in the acceptor chamber and the results showed no changes in permeability (intact barriers), independently of the presence or absence of a tested compound (data not shown). Further on, nontoxic concentrations were used for the absorption assessment experiments. All calculated p-values were >0.05, concluding that there were no significant differences between the parameters obtained on epithelia exposed to tested compounds compared with control.
Permeability (absorption) assessment
In this study, a 3D model of fully differentiated human airway epithelium (MucilAir) was used to assess upper-airway permeability of inorganic and organic compounds.
The permeability of compounds at known concentrations was measured in two directions—A-B and B-A—by analyzing the initial and final concentration in the donor compartment and the intermediate concentrations (at different time point intervals) in the acceptor compartment. The concentrations of the compounds were measured by analytical methods such as ICP/MS and Liquid Chromatography-TQMS. The Papp coefficient was calculated based on the concentrations of compounds that crossed the cell barrier within 2 hours. Finally, a ratio of the coefficient values (asymmetry index) was also calculated.
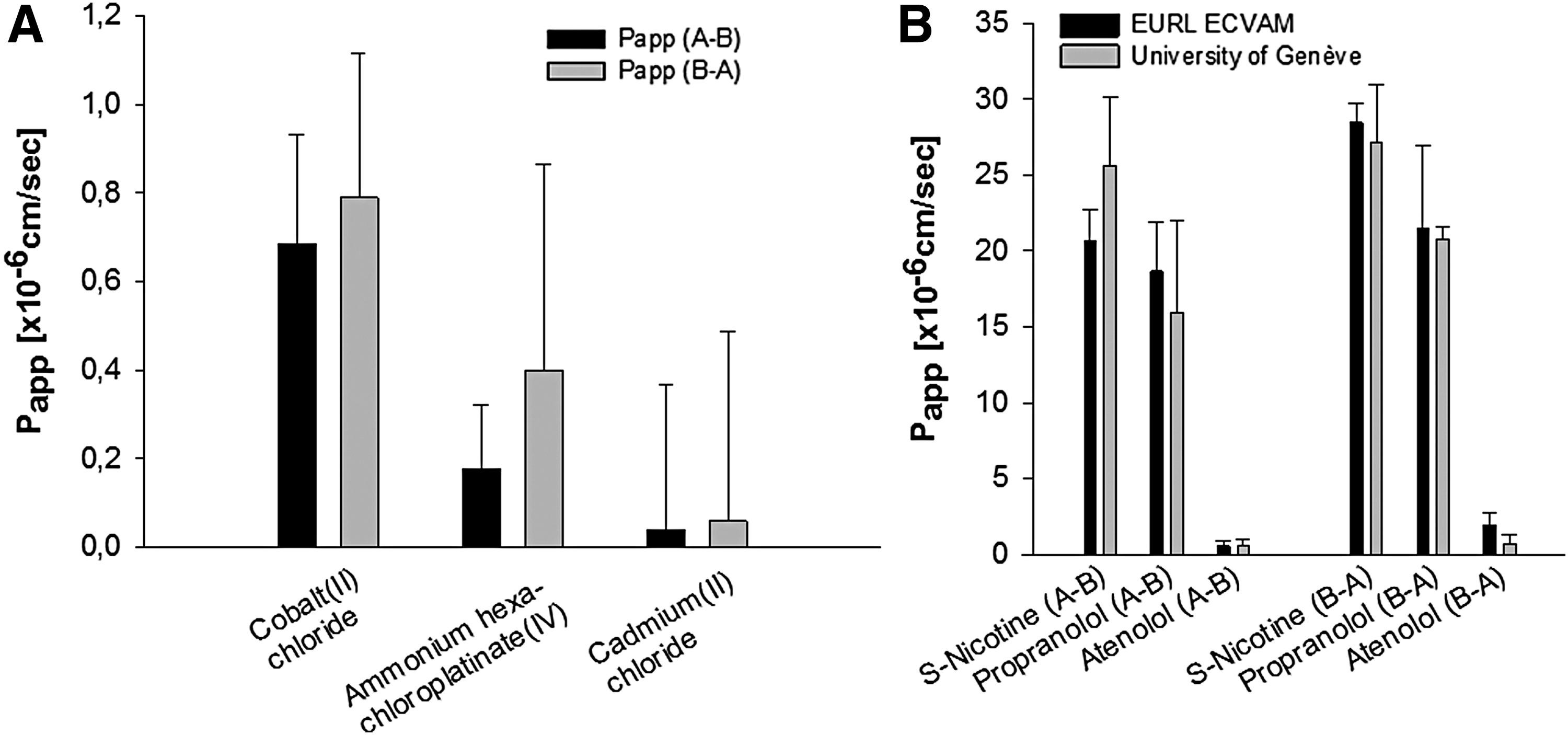
The method was first evaluated at EURL ECVAM by performing a permeability study on three inorganic compounds (cobalt chloride, cadmium chloride, and ammonium hexachloroplatinate) and three organic (propranolol, atenolol, and nicotine) compounds. Permeability testing of organic compounds has been carried out in parallel by EURL ECVAM test facility as well as by the University of Geneva, to evaluate the transferability of the method. Good between-laboratory reproducibility of the results has been observed (Table 1). The obtained results have shown a higher permeability of the airway epithelium for organic compounds comparing with the inorganic test items (Fig. 2). The lowest permeability from A-B compartments was registered for ammonium hexachloroplatinate (1.78 × 10−7 cm/sec), cadmium dichloride (2.72 × 10−7 cm/sec), atenolol (5.98 × 10−7 to 6.49 × 10−7 cm/sec), and cobalt chloride (6.85 × 10−7 cm/sec). The highest permeability measured from the A-B compartments was registered for propranolol (1.60 × 10−5 to 1.87 × 10−5 cm/sec) and nicotine (2.07 × 10−5 to 2.56 × 10−5 cm/sec).
Apparent permeability coefficient (Papp) obtained in the first experimental phase on the inorganic
EURL ECVAM (European Union Reference Laboratory for Alternatives to Animal Testing) results.
University of Geneva results.
Based on our measurements and on calculated apparent permeability coefficients, the following permeability ranking was established: nicotine > propranolol > cobalt chloride > atenolol > cadmium chloride > ammonium hexachloroplatinate.
Generally, the asymmetry index was below or around 1.5 U, which shows low protein-mediated efflux mechanisms involved in the permeability of the tested compounds. Only in one case, of atenolol, an asymmetry index of 3.5 was registered. However, this value was not confirmed by the parallel study.
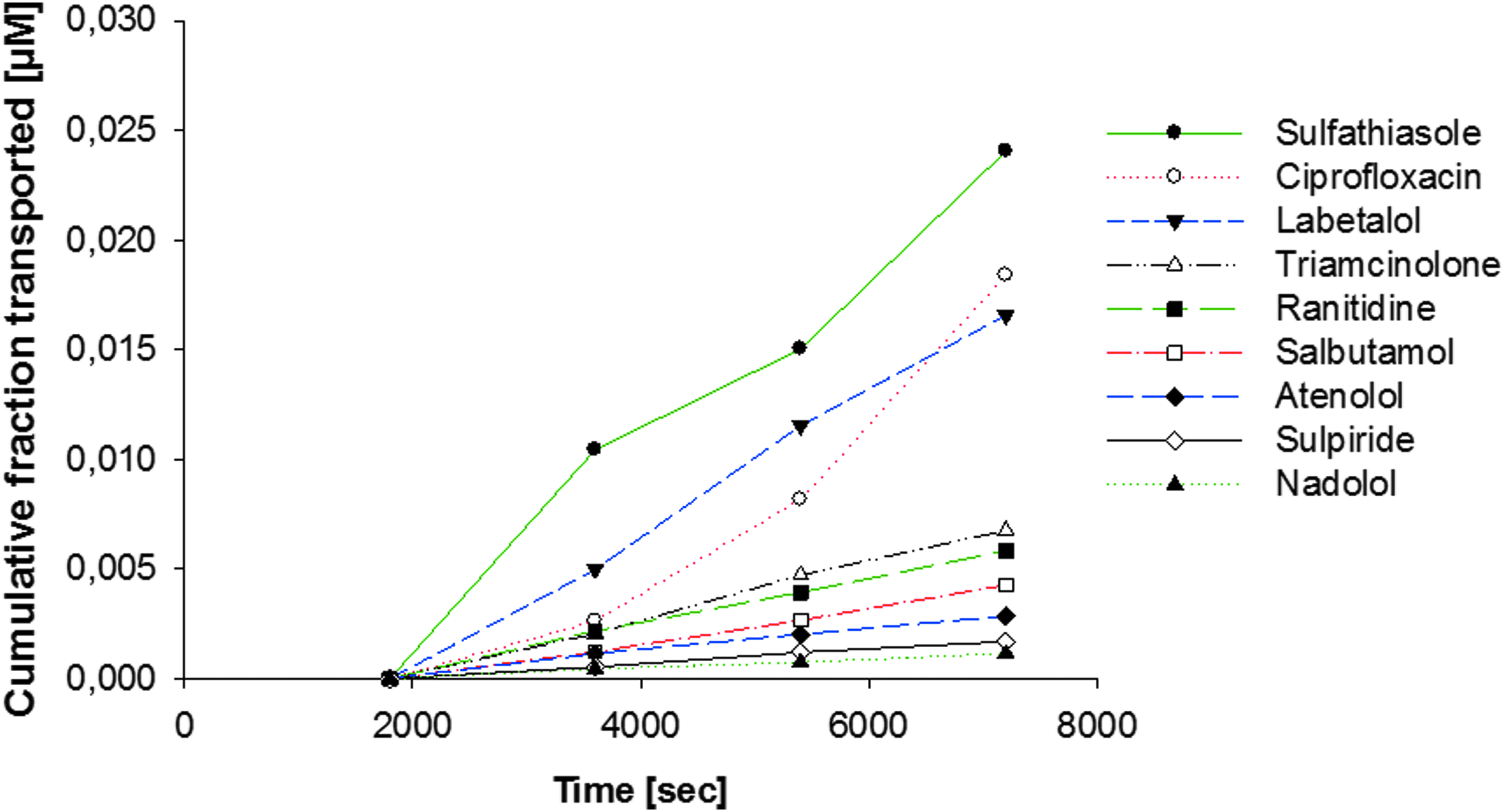
In addition, 30 compounds were tested using the SOP developed in the first experimental phase (Table 2; Figs. 3–5). The lowest permeability from A-B compartments was registered for nadolol (2.06 × 10−7 cm/sec). The highest permeability measured from the A-B compartments was registered for ibuprofen (4.94 × 10−5 cm/sec). Also, the differences in permeability due to anatomical origin were evaluated for salicylic acid on nasal and bronchial reconstituted epithelia (Table 3).
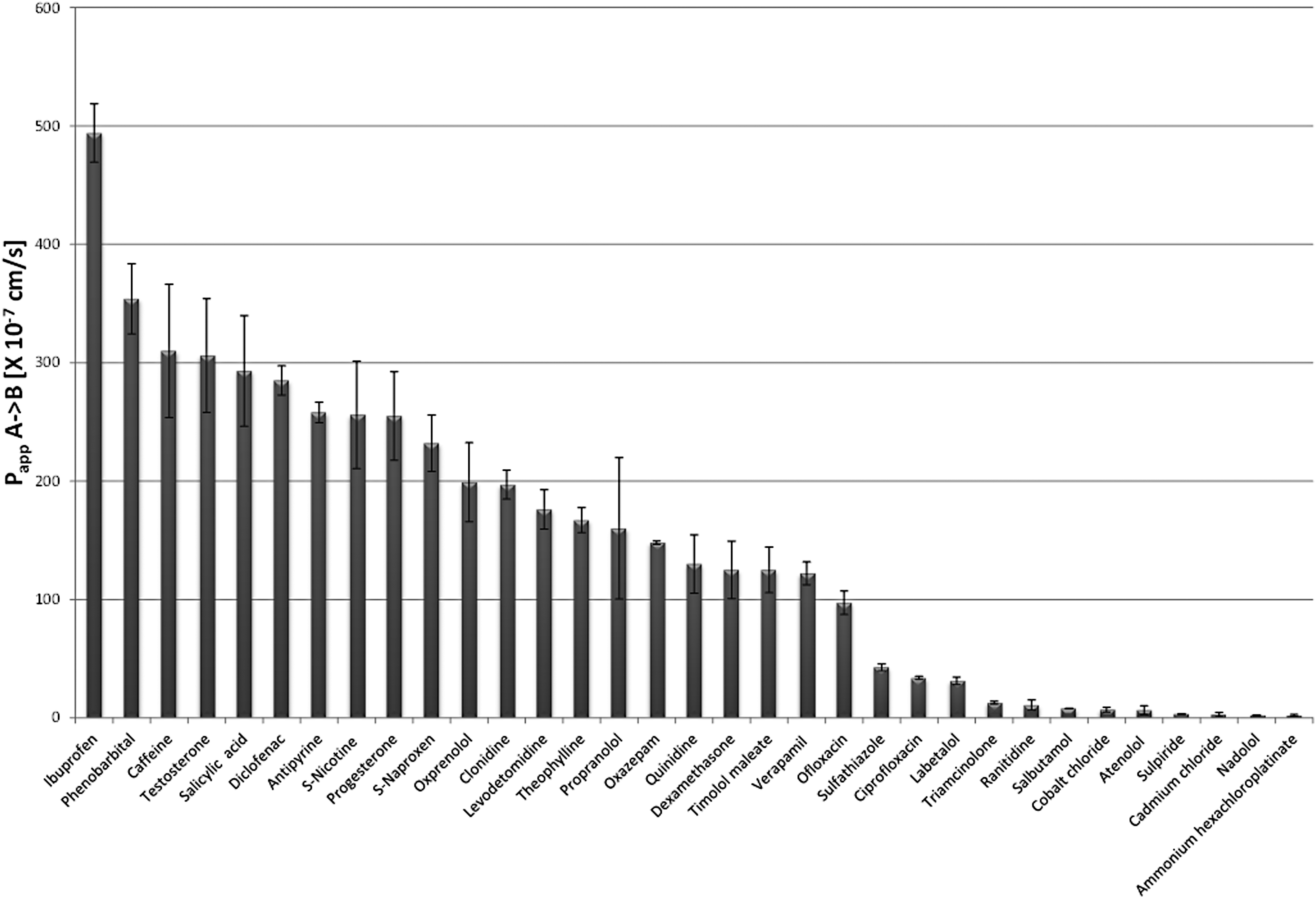
Apparent permeability coefficient (Papp) from A-B obtained from 33 reference compounds (n = 3). Data are expressed as mean ± SD. SD, standard deviation.
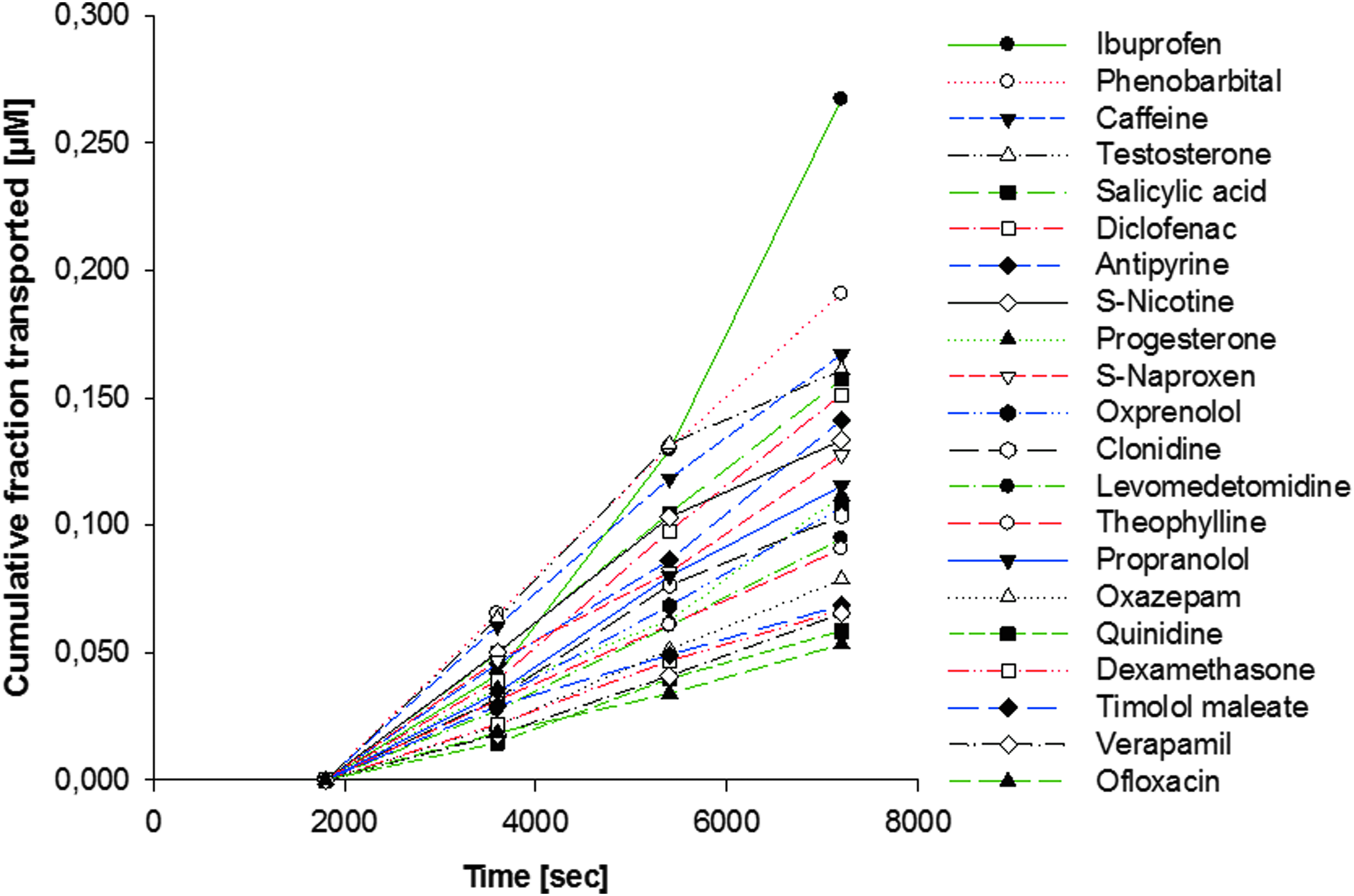
Cumulative fraction (μM) of organic compounds (n = 3) of higher and middle permeable organic compounds across airway epithelium in A-B direction. A-B, apical to basolateral.
Cumulative fraction (μM) of organic compounds (n = 3) of low permeable organic compounds across the airway epithelium in A-B direction. A-B, apical to basolateral.
SD, standard deviation.
Discussion
One of the biggest limitations of the in vitro test systems is the lack of systemic and kinetic features that are an integral part of the animal test systems. To predict the toxicity of a chemical on human heath, we need to define the possible exposure scenario and select the most relevant in vitro models, adapting an integrated test strategy as envisioned by 21th century toxicology movement.4–6 Since the respiratory system is one of the main entries of the toxic substances into the human body, it is imperative to know how the chemicals interact with and across this biobarrier. Up to now, respiratory permeation studies have been performed on cell lines such as Calu 3 or A549.26,27 However, even though useful, cell lines have lost most of the in vivo phenotypes, A549 does not even form tight junctions, a crucial feature of biobarriers. 27 The in vitro human airway epithelial model used here, MucilAir, made of primary epithelial cells and cultured at the air–liquid interface, replicates closely the morphology and function of native human tissues. Therefore, the in vitro system is much more relevant in predicting human response. As far as we know, this study is the very first attempt to assess the permeability of different chemical compounds through an in vitro human airway epithelium (MucilAir), in two independent research groups. Adopting the modular approach used for validation of alternative methods, 28 this study tried to include test definition, within-laboratory reproducibility, transferability, aspects of between-laboratory reproducibility, aspects of predictive capacity, and applicability domain. Accordingly, we have developed SOPs that were initially evaluated during a first set of studies on three organic and three inorganic compounds (propranolol, atenolol, nicotine, cobalt chloride, cadmium dichloride, and ammonium hexachloroplatinate), in two independent laboratories. In the second phase, a panel of 30 compounds were tested in one laboratory to evaluate experimental procedures and in particular the ability to rank relative permeability.
As quality control of the epithelia, in addition to qualitative control such as morphology of epithelia, cilia beating, or the presence of mucous, an important, quantitative measurement is TEER: it should be above 100 Ω*cm2, which is the case in this study. For permeability studies, various chemicals with known transport mechanisms can be used as positive control for biological barrier permeability, such as LY or 14 C-mannitol for paracellular transport, propranolol or warfarin for transcellular transport, rhodamine 123 or amprenavir for P-gp-mediated efflux. 24
As for permeation of tested compounds, Papp values range between two orders of magnitude: 4.94 × 10−5 (ibuprofen) to 2.06 × 10−7 cm/sec (nadolol) with a 240-fold difference between the higher and lower permeant. The moderately and highly lipophilic compounds such as propranolol, as well as dexamethasone, diclofenac, ibuprofen, naproxen, progesterone, quinidine, testosterone, and verapamil, are transported more rapidly than hydrophilic ones. The data obtained for hydrophilic β-adrenergic compounds (atenolol and nadolol) and anticholinergic amino-salt (glycopyrronium), as well as the antipsychotic—sulpiride or antibiotic—ciprofloxacin, suggest a contribution of paracellular way or other pore pathway for transport (Fig. 3).
Interestingly, the Papp values for salbutamol obtained in this study are quite similar to that reported by Mamlouk et al. 29 based on Calu-3 cells (7.91 × 10−7 vs. 1.83 × 10−6, about twofold difference). However, there are almost two magnitudes of difference of the Papp values for ibuprofen between these two studies (4.94 × 10−5 vs. 3.01 × 10−7). These differences highlight the need to use in vitro models that closely replicate in vivo morphology and physiology.
Now the questions are as follows: (1) Is the MucilAir model relevant? (2) Are the results reliable?
The in vitro upper airway epithelial models are often considered as less important and relevant than alveolar ones, because the surface area of the upper airways is much smaller than alveolar space. The relevance and importance of a model should not be judged by surface area or number of cells, because using the same arguments, it is possible to demonstrate the contrary. Citing Paracelsus, “All things are poisons, for there is nothing without poisonous qualities. It is only the dose which makes a thing poison.” A type I pneumocyte has an average diameter of 100 μm, 30 covering a surface area about 7850 μm2. The alveolar space is estimated to be 75 m2. Therefore, when a given amount of toxicant reaches the alveolar space, if it is evenly distributed and spread, each type I pneumocyte will be exposed only to 1/10,000 of the original dose inhaled from the nose or mouth. In other words, the cells exposed to highest concentration of toxicant and therefore at higher risk are located at the upper airway, not in the alveolar space. Consistent with this analysis, viral and bacterial infections in human beings start mostly from the upper respiratory tract, the nose, trachea, and bronchi. Since the toxicant is obliged to pass through the upper airways before getting into alveolar regions, one could argue that it would be enough to assess its toxicity on upper airway epithelial cells, which is not true.
It should also be kept in mind that most deadly and dreadful cancers are often, if not always, originated from a single mutated cell, 31 which may be induced by environmental toxicants. Squamous lung cancer represents at least 30% of all lung cancers. 32
Even for drug delivery, the upper airway epithelial models are also highly relevant! Indeed, much efforts have been made to deliver the drugs through nasal route, which offers a number of distinctive advantages for systemic delivery such as rapid attainment of therapeutic drug levels in the blood and bypassing of hepatic first-pass metabolism. 33
Are the data reliable and predictable for human in vivo situation? For the following reasons, we think they are. In addition to the intrinsic morphologic and functional criteria previously mentioned, the studies on toxicity testing of drugs as well as respiratory viral infections provided strong evidence for in vitro and in vivo correlations in each corresponding subject. By testing a set of compounds with (n = 8) or without (n = 7) respiratory toxicity following inhalation in vivo, Balogh Sivars et al. 34 demonstrated that the results of toxicity test on MucilAir system are highly correlated with the data obtained in vivo, with 88% sensitivity and 100% specificity. Tapparel et al. 35 showed that MucilAir can efficiently support the infection and growth of rhinovirus type C, which could only grow in human beings.
Caco-2 is a cell line widely used for assessing permeation of compounds. 36 For certain compounds, for example, ibuprofen, the Papp values obtained on MucilAir are comparable to that from Caco-2 system, with a magnitude of 10−5, 37 which is highly permeable. Good correlation has been found for drug absorption in human jejunum and Caco-2 cells, especially for passively absorbed drugs.38,39 This is quite surprising because the Caco-2 system not only lacks the architecture and organization of human jejunum but also lost some (genetic and phenotypic) features of the human enterocytes. On the contrary, the good in vitro and in vivo correlation of Caco-2 system reinforces our conviction that the permeation data obtained from MucilAir should also be correlated to and predictive for in vivo situations, based on the fact that MucilAir replicates both the morphology and function of human airway epithelium, and the airway epithelium is relatively simple and homogeneous. However, it is not within the scope of this article to establish an in vitro and in vivo correlation model for human lung permeation. Nevertheless, efforts have been made in this direction: there is evidence suggesting that the permeability characteristics of Calu-3 cells correlated to the rate of drug absorption from the rat lung in vivo (R 2 = 0.94). The absorption predicted from the regression equation correlated well with observed values. 40 To establish a predictive kinetic model for the entire human lung based on in vitro cell models, the permeability characteristics of small airway epithelium and alveolar epithelium should also be evaluated in the future, 41 to be integrated into a single predictive model.
Influence of the anatomical region and age of cultures
Nasal and bronchial transport of salicylic acid (1 mM; pH 7) has been studied in several batches of MucilAir with ages of cultures ranging from 1 to 13 months (Table 3). Mean permeability values of 2.45 × 10−5 are obtained for the nasal version and 1.43 × 10−5 for the bronchial versions. Only minor differences are observed, suggesting that nasal version might be a good surrogate to the bronchial epithelium for permeability studies.
Overall, the results demonstrate that MucilAir is an effective barrier model for assessing the permeability of different classes of compounds across the human airway epithelium. Not only is it a more reliable representation of the native phenotype but also robust and easy to use. The methods are transferable, and the results obtained are highly reproducible.
In conclusion, this study indicates that the 3D human airway epithelium (MucilAir) is a relevant and reliable tool for evaluating pulmonary permeation/absorption of chemicals in human lungs.
Footnotes
Acknowledgments
The study was funded by CTI/KTI.
Author Disclosure Statement
The authors state no conflict of interest.