
Abstract
Abstract
Over the past decade, there has been a significant increase in preclinical development and clinical use of approved nanomedicines. The nanomedicinal field represents a wide variety of products including early diagnostics such as in vivo imaging, medicinal devices, and innovative therapeutics. Nanomedicines exhibit unique physiochemical properties compared with their nonnanoformulated counterparts; however, clinical reports of moderate-to-severe allergic, anaphylaxis, and hypersensitivity reactions raise major concerns with regard to nanomedicine immunotoxicity. This review summarizes some of the main applications of nanomedicines, safety, and immunotoxicity implications and current testing strategies.
Introduction
Nanotechnology is an increasingly novel area of interest in science and medicine. It is an interdisciplinary field bridging the gap between physical and biomedical sciences, aiming to address unmet needs in medicine. Nanoparticles (NPs) are being applied across various disciplines of medicine due to their design, properties, and application in personalized medicine. 1 They started to emerge on the market over a decade ago and their use has increased exponentially. 2 They are characterized by their advantageously tiny size, with a nanometer being one-millionth of a millimeter and ∼100,000 smaller than the diameter of a human hair. 3
Nanomedicines are generally made of polymeric or inorganic materials with metal and liposomal nanomedicinal products (NMPs) being commonly used in medicine as site-specific drug carriers, for example, in anticancer and cardiovascular drugs.4–7 Several nanodrugs have already entered the market and many more are undergoing clinical trials with multiple indications. 8
NMPs include innovative clinical therapeutics, for example, doxorubicin integrated with polysorbate 80 modifies polybutylcyanoacrylate NP and allows delivery of the drug across the blood–brain barrier. 7 NMPs also include early diagnostics 9 or treatments with high specificity, efficacy, and personalization,10–12 aiding to enhance patient's quality of life.4,7 In therapeutics, active ingredients are often encapsulated by a NP shell, acting as drug delivery vehicles for commonly used conventional nonnanoformulated drugs. Moreover, a possible combination of diagnosis and therapeutics, known as theranostics, within a single nanomedicine formulation is of value for further personalizing therapeutics in individual diseases such as cancer.2,7
Applications of Nanomedicines
NMPs widen the scope of pharmacokinetics for conventional insoluble drugs and overcome barriers such as anatomical, chemical, physiological, and clinical due to their physiochemical properties (Table 1).13,14
Nanoformulations in Medicinal Products
Table showing the type, size, and description of physiochemical properties of the listed nanomedicinal products (modified from Giannakou et al. 14 ).
NP, nanoparticle.
Therapeutic nanomedicines show superiority over standard low-molecular weight drugs because of increased bioavailability, lower accumulation in healthy nontarget tissues, and improved therapeutic index with increased accumulation at target sites improving drug delivery. 2 Such benefits are gained in nano-based cancer therapeutics, an example of this is the Food and Drug Administration (FDA)-approved paclitaxel nanodelivery system. Paclitaxel is one of the most effective chemotherapeutic drugs ever developed, and NP-encapsulated formulas such as Abroxane® have the potential to address the failures of traditional therapeutics. 23
The main areas that nanomedicines are used include cancer, diseases of the central nervous system, cardiovascular disease, and infection control. 24 Nanoformulations present many advantages when compared with conventional medicines, such as improved solubility and pharmacokinetics, reduced toxicity effects, and improved efficacy, alongside better tissue selectivity. 25 Nanomedicines can be developed from different materials, including, proteins, polymers, dendrimers, micelles, liposomes, emulsions, NPs, and nanocapsules. 26
Nanomedicinal approaches have enabled the transformation of “one drug fits all” to the emergence of highly specialized personalized treatment, especially in cancer patients as cancers can differ substantially between individuals. 27 Nanomedicines can be used as a sophisticated drug delivery system as they can be used to target diseased tissue (e.g., cancer) through biomarker recognition as well as the incorporation of pharmacologically active molecules. They involve the use of nanoscale materials, such as nanorobots and biocompatible NPs based on, for example, carbon-derived nanotubes. 28
There are already several drugs that have been FDA approved, these include those used in fungal infections, Abelcet®, metastatic breast cancer, Abraxane®, and acute lymphocytic leukemia, Oncaspar®. See Table 2 for an expanded list of FDA-approved nanomedicines.
Food and Drug Administration-Approved Nanomedicines
Table showing the name, indication, and year of approval of nanodrugs that have gained FDA approval.
CKD, chronic kidney disease; NSCLC, non-small-cell lung carcinoma.
One of the most recent uses of nanomedicines in 2019 is the use of iodine NPs to increase the efficacy of chemotherapy in intracerebral human glioma. It has been shown in mice that the Doxil® iodine NPs enhanced the effect of radiotherapy compared with Doxil alone by increasing the median life expectancy of the treated mice. This NMP, therefore, shows promise for clinical transition in the future. 29
Other examples of nanomedicine applications are contrast agents for cell imaging, cancer treatments, medical applications, diagnostic devices, drug delivery vehicles, neuroelectronic interfaces, tissue repair, and molecular nanotechnology. Nanomedicines are also important in the implementation of personalized medicine, for example, a drug delivery system can target diseased tissue in patients by recognizing patient-specific biomarkers alongside carrying pharmacologically active molecules to treat the cancer. 1 The use of a drug delivery system can also reduce the amount of the active agent needed, as less of the drug is degraded when traveling to the target organ, resulting in higher bioavailability. Also, nanomedicines can be engineered to be pH sensitive or capable of fusion, this aids the delivery of their contents from the endolysosomal compartment into the cytosol within minutes of internalization. 30 For example, theranostics combines therapy and diagnostics. Advanced theranostic nanomedicines conjucated with a specific target moiety can recognize the target and be internalized through specific receptor-mediated endocytosis. These types of nanomedicines include PEGylated liposomes as nanothernostic liposomes for cancer therapy and diagnosis.31–33
Nanomedicines and Toxicity
Nanotoxicology can be defined as the study of adverse effects of engineered nanomaterials on living organisms and ecosystems and the prevention and amelioration of these effects.34–36
Owing to their properties and their pharmacokinetics, nanomedicines produce different toxicity and adverse events when compared with non-nanoformulated conventional medicines.31,37
The reduced size of the nanomaterials increases cell surface markers and surface area exponentially, leading to complex reactions with bionanointerfaces when exposed to physiological environments. Also, size is a key factor in determining toxicology due to the NPs' ability to translocate across cell barriers or neuronal pathways. Size also determines the mechanism for cell entry as the smallest of nanomaterials can diffuse across cell membranes.31,34
Alongside the advantages of physical chemical drug delivery in NMPs, it is also important to realize the potential issues related to toxicity. This and lack of adequate data regarding their toxicity often challenge the benefits of using nanomedicines. 30 Nanotoxicology research has identified the numerous complex interactions between NMPs and the human organism. 38 In particular, interactions between NMPs and the complex human immune system, with its individual diversity, make preclinical safety assessments of NMPs extremely challenging.1,39
Research shows that nanomedicines can stimulate or/and suppress the immune response, 40 with activation of the immune system being the most frequently observed immune reaction. NMPs have been shown to interact with both the innate and adaptive immune systems.1,41 NMPs interact with the innate immune system through complement activation. Complement-activated pseudoallergic reactions are also a frequent side effect of in vivo intravenous (i.v.) administrated FDA-approved lipid and polymer-based nanomedicines. Since, i.v. administration means immediate interaction with blood, and thus the hosts immune system, there is an increasing risk of immunotoxicity.1,38,42 Antigenicity of NPs causes a cascade of reactions leading to inflammatory processes or adverse drug reactions (ADRs) such as hypersensitivity allergic reactions. ADRs caused by the adaptive immune system through activation of T cells and B cells leading to cascades of cell-mediated and humoral responses have been observed in in vivo mouse models upon administration of inorganic NPs.43–45
Critical factors that contribute to nanotoxicity are size and surface area-to-volume ratios. There is a strong inverse correlation between NP size and toxicity. Toxicity associated with NMPs has hindered their clinical use, due to toxicity issues and the lack of defined safety regulations within the nanomedicine field.39,40,46,47 Advances in nanomedicine have stimulated the development of new assays to evaluate NMP toxicity. One new assay developed by the American Society for Testing Materials (ASTM) evaluates the effects on NMPs on the formation of mouse granulocyte macrophage colonies and is the only standardized method for evaluating immunotoxicity responses by NMPs. 1 Complement activation, secretion of proinflammatory cytokines, lymphocyte activation, and T cell-dependent antibody response are some of the other in vivo and in vitro testing approaches available. 47 However, there are currently no commercially available in vitro assays that test for human-specific NMP effects on the immune system.
Safety, Efficacy, and Immunotoxicity of Nanomedicines
Immunotoxicity is the host's immune response against foreign unfamiliar agents such as viral or bacterial infections.1,38 The human immune system comprises the innate and the adaptive immune responses that include humoral (antibody) or/and cell-mediated (T cell) immune responses. The innate response is an immediate nonspecific immune response against pathogens. The adaptive response is a delayed and highly specific mechanism accountable for allergic and hypersensitivity reactions. 1 Both responses are part of the body's key mechanism of defense against infection. However, the same systems are responsible for immunotoxicity to nanomedicines. Since clinical introduction of NMPs, many adverse immune effects have been reported, including acute immune responses in the form of hypersensitivity, allergy, anaphylaxis, and immunosuppression. 14 Known hypersensitivity reactions are divided into four types (type I, type II, type III, and type IV) (Table 3) based on the underlying mechanism.48,49
Hypersensitivity Reactions Types I–IV a
APC, antigen presenting cell; IgE, Immunoglobulin E; PMN, polymorphonuclear leukocyte.
In particular, Gell and Coombes Type 148–50 hypersensitivity reactions are due to structural similarity of NMPs to antigen epitopes, mimicking re-exposure to the specific allergen.47,49
Immunotoxicity and lack of a routinely used preclinical humanized in vitro test raise serious concerns in present-day safety assessment procedures. As with any medicine, the quality, efficacy, and safety of NMPs needs to be evaluated and approved by regulatory bodies (e.g., the FDA). Currently, there are no regulatory documents dedicated to the evaluation of NMPs and immunotoxicity. Evaluation of nanomedicines is mostly performed using animal models and in vitro tests normally used for conventional non-nanoformulated products. However, as previously outlined, crucial physiochemical, structural, and biological differences between conventional medicines and nanomedicines, as well as interspecies differences of animal models bring into question the validity of applying these tests to NMPs. 14 One solution to this dilemma may be to use human tissue in the development of new in vitro NMP safety tests as demonstrated by current in vitro tests using human skin samples and immune cells for immunotoxicity and sensitivity testing.52,53
The induction of cytotoxicity in cancer cells using nanomaterial-based drug delivery aims to kill cancerous cells and eliminate tumors; however, this can lead to unwanted side effects including toxicity. 54
Some toxicological effects in nanomedicines are dependent on their pharmacokinetics that differ from conventional medicines, the differences in absorption, distribution, metabolism, and excretion (ADME) may result in altered bioavailability at certain sites within the body, thereby resulting in different toxicological responses.1,41
The Human Immune System and Nanomedicines
Activation of the immune system is the most observed immune response in animal models, following the administration of nanomedicines. It is completely independent of the category of the nanomedicines. Moreover, excessive immune stimulation can result in autoimmune disorders and alternatively cause inflammation in tissues, resulting in long-term damage. 1 NPs can not only stimulate but also suppress the immune response 40
NPs can be taken up by immune cells, including monocytes, macrophages, platelets, dendritic cells in the blood stream as well as within tissues such as Kupffer cells of the liver, dendritic cells in the lymph nodes and macrophages, and B cells in the spleen.14,38
NPs interact with protein to form “protein bio-corona” within biological fluids. This interaction can cause activation of the immune response either innate immune response through macrophage phagocytosis and complement activation or adaptive immune response through “danger signals” such as toll-like receptors and activation of the nuclear factor kappa light chain of human activated B cells.1,41,55 The nanomedicinal proteins can, therefore, be seen as foreign by the patient's adaptive immune system and the proteins can be presented to T cells resulting in the cascade of cell-mediated and humoral responses. Depending on the type of protein that is presented, T cells proliferate into T helper 1 cells (Th1), T helper 2 (Th2) cells, or regulatory T lymphocytes (Th17).
Since Th1 cells play a major role in cellular immunity and release of Th1 type cytokines, for example, interferon gamma, tumor necrosis factor alpha, and macrophage polarization to the inflammatory phenotype MI, while Th2 cells promote humoral immunity, insight into the Th1/Th2 balance after nanomedicine exposure can aid in assessing the subsequent immune pathway.44,56
Since the introduction of nanomedicines to the clinic, there have been several cases of acute immune responses to the NMP product in the form of hypersensitivity reactions, this is often due to the structural similarity of NM to viral antigens, which can trigger nonspecific humoral immunity and cause the complement system to produce an immediate eliminatory response. An overview of the complement pathways is shown in Figure 1. In particular, when nanomedicines are administered i.v., they interact immediately with the blood and the immune system. 1 Furthermore, acute allergic reactions that are in line with the symptoms of Gell and Coombes Type 1 classification, not initiated by pre-existing antibodies, can occur after administration of nanomedicines available in the clinic. 54
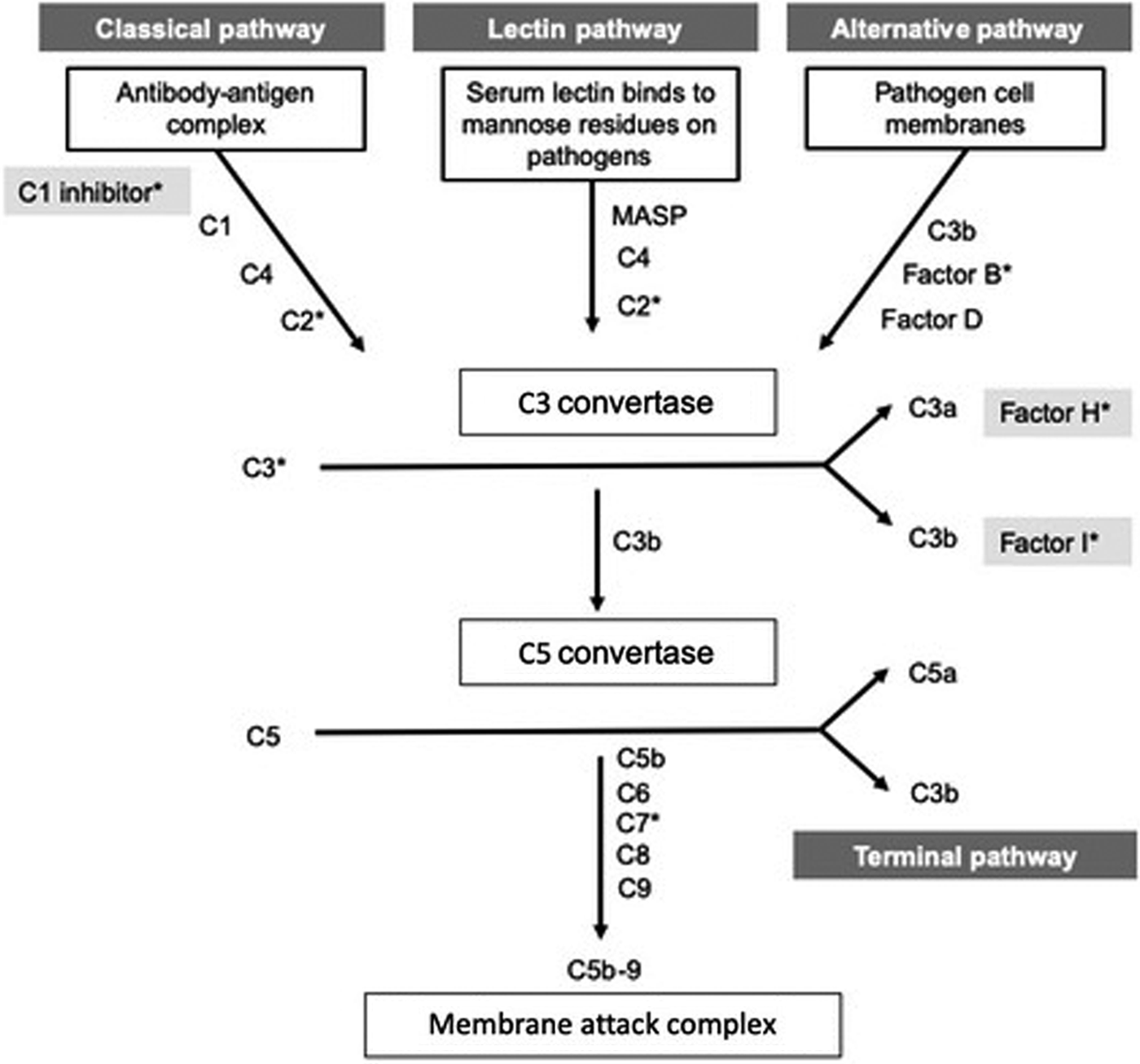
Flow chart showing the three pathways in complement activation, including the classical, lectin, and alternative pathway, the complement provides the frontline of the immune defense as has the capability to eradicate all types of microbes (modified from Warwick et al. 59 ).
Alternatively, pseudoallergic reactions show a strong correlation with complement activation, which can result in the release of anaphylatoxins C3a, C5a, and the subsequent release of thromboxane A2, alongside other anaphylatoxin mediators. Liposomes have shown to activate the antibody and nonantibody-derived mechanisms of the immune system (through the classical or alternative pathway). This is referred to as complement activation-related pseudo allergy. 57
Hypersensitivity to Liposomes
Doxil, a liposomal medicine, which has been approved for the treatment of HIV-related Kaposi's sarcoma, has shown to cause cardiopulmonary distress in a substantial percentage of human subjects upon infusion. 58 A recent study reported acute allergic responses in 13 out of 29 cancer patients administered with Doxil.
Another study showed that 3%–45% of patients administered with liposomes developed an acute allergic reaction; with some patients showing symptoms similar to that of an Immunoglobulin E-mediated Type 1 allergy. Symptoms included cardiopulmonary distress such as dyspnea, tachypnea, hypertension/hypotension, and chest and back pain. However, this reaction differed from Type 1 allergy as no previous sensitization (as seen with NPs) is required and the severity of symptoms seems to decrease with later treatments. This has been reported to occur after the administration of several commercially available nanomedicines (liposomes, micelles, and polymeric nanospheres). The understanding of the causative factors in producing this reaction could result in better design and nanoengineering strategies to prevent hypersensitivity in future nanomedicines. 59
Toxicity with the Anticancer Drug Paclitaxel
Paclitaxel is one of the most effective chemotherapeutic drugs and has been reported in the literature to have a range of toxicological effects. Paclitaxel (Taxol) can be bound to albumin as a delivery vehicle (known as nab-paclitaxel or Abraxane). The bound and unbound forms can show adverse effects in patients. Both drugs show similar frequencies of adverse effects such as neutropenia, gastrointestinal disorders, nerve damage, arthralgia, and myalgia. Other adverse effects showed a different frequency in occurrence when patients were administered paclitaxel and nab-paclitaxel, with 55 adverse effects for conventional paclitaxel and 165 adverse effects for nab-paclitaxel. Adverse effects that were specific to nab-paclitaxel were nervous system disorders, eye disorders, respiratory, thoracic, and mediastinal disorders among others. Overall, there are more adverse effects shown in response to nab-paclitaxel, but this could be due to their use in different indications, such as their use in the treatment of different cancers. 37 There have been strategies developed to reduce adverse and toxic effects in nanomedicines; the use of materials that are biocompatible and biodegradable and the incorporation of surface coatings reduce the accumulation of NPs in the liver and spleen and reduce toxicity. 26
Testing the Safety of Nanomedicines
The emergence of nanomedicines has raised questions regarding current safety assessment procedures and whether they provide an accurate evaluation of the quality, safety, and efficacy of NMPs when applied to nano-specific aspects. 37 The safety evaluation for nanomedicines may require a different approach from conventional drugs due to their difference in size as they may respond in different ways due to their unique properties. Owing to inadequate availability of data on the toxicity responses of nanomedicines, there is a great encouragement for multidisciplinary studies to understand nanomedicine toxicity and develop adequate testing procedures. 60
Toxicity testing of nanomaterials can be carried out using in vivo and in vitro assays to identify potential hazards by establishing a dose–response relationship to enable the characterization of the hazard. The genuine accepted approach is to assemble a risk assessment paradigm, consisting of hazard identification, hazard characterization, exposure assessment, and risk characterization. 61
Challenges in the Safety Assessment of Nanomedicines
In 2006, the Nanotechnology Task Force was initiated to address the safe and sustainable development of nanotechnologies.62,63 This would involve developing instruments to monitor nanomaterial exposure in air and water; the development of models for predicting the impact of nanomaterials on environmental and human health; finding and developing methods to evaluate toxicity that have been validated; and developing systems for evaluating health and environmental impact of nanomaterials over their entire life cycle. An article by Nyström and Fadeel 64 suggested that the following challenges would need to be addressed in the next 5–10 years. These include to develop validated in vitro assays with a set of reference materials, establish ex vivo models to assess routes of administration, develop in silico methods to determine biological and toxicological effects, develop the understating of ADME in vivo, establish a relevant paradigm to understand factors involved in nanomaterial interactions within living systems, and provide research teams who are involved in the development of assays with interdisciplinary training (clinical, biological, engineering, and toxicology). 64
In Vitro Testing of Nanomedicines
There are several toxicities that can be tested for using in vitro methods. These include carcinogenicity, immunotoxicity, proinflammatory responses, genotoxicity, and cytotoxicity (necrosis and apoptosis, cell proliferation, membrane integrity and metabolism, and cell morphology alterations).
Carcinogenicity
The in vitro test for carcinogenicity is the cell transformation assay, this is a relatively new approach that measures the potential cell transformation (one step in the cancer process), this assay can detect both genotoxic and nongenotoxic carcinogens. In 2015, the European Union Reference Laboratory for alternatives to animal testing issued a document proposing to use of the “In vitro Syrian hamster embryo (SHE) cell transformation assay” in part of a weight of evidence approach to test substances for carcinogenic potential. 65
Immunotoxicity
There are very limited in vitro tests for immunotoxicity as adverse effects are not always readily detected in conventional immunotoxicity methods. 65 However, more recently human-based skin explant assays have been shown to be novel additional tools for the assessment of immunotoxicity, including adverse immune reactions to both chemicals and small molecule drugs and can be adapted for testing nanomaterials and nanomedicines.52,53
Proinflammatory response
An in vitro test to test for a proinflammatory response is reverse transcription polymerase chain reaction that detects gene expression of proinflammatory genes in reporter cell lines and can be used without or in parallel with enzyme-linked immunosorbent assay. 65
Genotoxicity
An in vitro test for genotoxicity is the AMES assay, but it can be ineffective. Alternatively, the mammalian cell gene mutation assay or adaptation of the mammalian cell micronucleus assay that detects chromosome breakage leading to an additional nucleus (micronucleus) during cell division can be used.38,65
Cytotoxicity
Cytotoxicity is cell damage that can be caused by a range of intracellular changes, such as apoptosis and necrosis (programmed cell death vs. accidental cell death), cell proliferation, alterations in cell metabolism and membrane integrity, and changes in cell morphology.
Apoptosis and necrosis can be detected through Annexin-V that can be used to test for the loss of membrane asymmetry (apoptosis) and can be coupled with propidium iodide to detect necrotic cells. Apoptotic/necrotic cell proportion can also be determined by flow cytometry. Cell proliferation can be determined through the colony forming efficiency assay. Compromised membrane integrity can be determined using neutral red uptake that results in the acquirement of a blue color in dead cells and no color in live cells. To monitor cell metabolism, tetrazolium salts can be used for evaluation of mitochondrial activity as mitochondrial dehydrogenase enzymes cleave the tetrazolium ring; these enzymes are only functional in active mitochondria, and lastly, cell morphology can be monitored using phase contrast microscopy to visualize morphological alterations. 65
Hemocompatibility assays
There is a range of hemocompatibility assays that can be carried out on blood samples. The main hemoincompatibility problems that can occur in response to nanomedicines are thrombosis, coagulation, platelet activation, blood cell changes, and complement activation. The more associated adverse effect of nanomedicines is the complement activation, assays can be carried out to detect the presence of C3a, C5a, Bb, iC3b, C3 convertase, and C5 convertase among other complement components. 66
In Vivo Testing of Nanomedicines
In vivo, the most sensitive and relevant animal model for human hypersensitivity reactions is the porcine model, i.v.-injected nanomaterials show a cardiopulmonary response in a porcine model. Pigs are particularly sensitive to intrapulmonary injection of nanomaterials (particularly liposomes), they have been shown to develop major hemodynamic changes in response to very small amounts of injected nanomaterials. Certain liposomes result in the rise and fall of systemic arterial pressure, a rise in pulmonary arterial pressure (PAP) changes in heart rate, cardiac output, and electrocardiogram (ECG) readings (detection of arrhythmias and cardiac arrest). Monitoring of in vivo models was carried out by analyzing blood samples, ECG monitoring, and the utilization of an ADinstruments Powerlab monitor connected to a converter box (monitors PAP, ambulatory blood pressure, central venous pressure, and sulfur levels). 67
Preclinical Hazard Evaluation Strategy
The hazard evaluation strategy (HES) is a three-tiered concept that covers physiochemical characterization, NP interactions, and hazard assessment, this is adaptable to different exposures and applications. This was designed by Siegrist et al., 68 to test the suitability of injectable engineered NPs (ENPs). Nanomedicines can be very diverse in relation to many factors such as chemical identity, size, geometry, surface modifications, and intended clinical uses. These formulations often share some properties (spherical, aspect ratio, diameter <1 μm, and stable dispersions). As these, however, do not provide much information once the nanomedicine is injected, ENP interaction needs to be assessed. The two main factors that can determine preliminary information on biological reactions are cellular uptake and intracellular persistence as low intracellular persistence and low cellular uptake can result in limited biological interactions; these factors also help categorize nanomedicines into hazard groups. The HES is shown in Figure 2 as modified from Ref. 68

The hazard evaluation strategy for nanomedicines. This is based on a three-tier approach combining physiochemical characterization, nanoparticle interaction, and hazard assessment. This testing strategy can identify potential safety risks of nanomedicines and can provide the basis for subsequent in vivo studies (modified from Siegrist et al. 68 ).
Conclusion
In conclusion, nanomedicines show great potential in a range of disciplines such as cancer treatments, diagnostic tools, and drug delivery vehicles; however, due to their small size, they react differently when compared with conventional drugs due to their different pharmacokinetics, However, there is a need to develop improved and validated in vitro strategies to detect nanotoxicity especially, immunotoxicity as available assays do not always readily detect adverse immune effects. The development of multidisciplinary tests would provide a more cost-effective way of testing nanomedicines for nanotoxicity. Moreover, the development of human in vitro tests would overcome the issues of extrapolating data from animals to humans, currently none of these tests is commercially available.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.