
Abstract
Sexually transmitted infections (STIs) have been identified as cofactors of HIV transmission. Greater understanding of local STI burdens can assist in the development of more effective STI and HIV prevention strategies. The aim of this study is to determine the prevalence and incidence of STIs among South Indian men and women identified to be at increased risk for HIV infection. Individuals at increased risk for HIV infection were enrolled in a prospective longitudinal study in Chennai, India (n = 480) between August 2002 and December 2003. Participants were enrolled from patients seeking services at an sexually transmitted disease (STD) clinic and a confidential HIV testing and counseling program. The most common prevalent STIs were herpes simplex virus (HSV)-2 (50% of women, 29% of men), syphilis (11% of women, 8% of men), and Trichomonas vaginalis (6% of women). At enrollment, women, participants with no schooling, participants with greater than four sex partners, and single participants were found to be at increased risk for HSV-2 infection (p < 0.05). The two most common incident STIs at 12 months were HSV-2 with 12% of men and 8% of women testing positive and hepatitis B with 2% of men and 5% of women testing hepatitis B surface antigen (HBsAg) positive. In this cohort of South Indian men and women with a high background prevalence of HSV-2, suppressive therapy against herpes replication may have a substantial impact in reducing both HSV-2 transmission and HIV acquisition. With the high incidence of STIs, targeted prevention and clinical management strategies among individuals practicing high risk behaviors may help to slow the continued spread of HIV in India.
Introduction
I
The relative prevalence and risk of developing specific STIs can vary widely across different regional settings. 8,9 It has been suggested that STI treatment interventions can contribute substantially to the prevention of HIV infection in populations with early and concentrated sexually transmitted HIV epidemics. 8,10 In India, the prevalence of HIV remains relatively low at 0.91%. 2 Recent studies conducted in different parts of India have documented high rates of STIs within various groups, such as men who drink alcohol and engage in high-risk behavior, 11 men who have sex with men, 12 female sex workers, 13 and injection drug users 14 as well as individuals attending STI clinics 15,16 ; however, there is a dearth of longitudinal data on the development of STIs. 17
Given the synergistic transmission of STIs and HIV, the present study was undertaken to determine the prevalence and incidence of different STIs and to delineate the risk factors associated with STI transmission among individuals who were identified to be at increased risk for HIV infection in Chennai, India.
Methods
Setting
Y.R. Gaitonade Centre for AIDS Research and Education (YRG CARE) is a large HIV tertiary care community-based center in Chennai, India. 18 Since 1996, it has provided a continuum of care for over 10,000 HIV-infected individuals. Services at YRG CARE include voluntary counseling and testing (VCT), integrated medical services for the treatment of HIV and related illnesses, prevention programs, and nutrition counseling. YRG CARE is also a site for the U.S. National Institutes of Health multisite AIDS Clinical Trials Group (ACTG) and Health Prevention Trials Network (HPTN) clinical trials. This study received ethical approval of the free-standing YRG CARE Institutional Review Board (IRB).
Subjects
Four hundred eighty high-risk HIV-negative individuals who were 18 years or older, residing in or near Chennai, and who were identified to be at increased risk for HIV infection were recruited for this study between August 2002 and December 2003. Individuals were recruited from within patients seeking services at the STD clinic at Stanley Medical College (Chennai) or as part of YRG CARE's confidential HIV testing and counseling program. 19 All participants tested negative for HIV antibodies at enrollment. All participants received treatment free of charge for any STIs diagnosed as part of this study. Participants completed a risk assessment questionnaire at enrollment, and provided blood samples for serologic testing at baseline, at 6 months, and at 12 months. Two hundred seven (43.1%) individuals of the initial cohort provided repeat samples for STI analysis at 12 months. The characteristics of the men and women who presented at follow-up were not significantly different from the individuals at baseline.
Enrollment criteria
Men were enrolled who met at least one of the following self-reported criteria: STI within the past 6 months; sex with a female sex worker at least 5 times in the last 1 year; or vaginal sex with an HIV-infected partner at least once a week over the past 6 months. Women were enrolled who met at least one of the following self-reported criteria: five or more male sex partners in the last year; a current male sex partner who injected drugs in the last year; a new diagnosis of syphilis, Chlamydia trachomatis, Neisseria gonorrhea, first episode of genital herpes, pelvic inflammatory disease (PID) and/or Trichomoniasis in the last year; or exchange of sex for money or drugs in the last year.
Diagnostic tests
Blood samples were collected from consenting participants at each study visit. Urine was collected from consenting men, and from women if they refused endocervical swab collection. Laboratory tests of urine or vaginal secretions included Multiplex PCR for Chlamydia trachomatis and Neisseria gonorrheae (Roche Diagnostics, Basel, Switzerland). Enzyme-linked immunosorbent assay (ELISA) were run on plasma samples for hepatitis B surface antigen (HBsAg; Hepanostika HBsAg Uni-Form II, Biomerieux, The Netherlands), and for herpes simplex (HSV)-2 antibodies (Focus Diagnostics, Cypress, CA). A 1.1 cutoff was used to determine HSV-2 seropositivity. Rapid plasma reagin (RPR) (Span Diagnostics, Surat, India) was performed for Treponema pallidum. The range of RPR titers was 1:1–1:128; RPR repeat titers were not performed. Particle agglutination (TPPA; Serodia, Japan) was done to confirm diagnoses. For female participants, Trichomonas vaginalis In-Pouch culture was performed on vaginal secretions (BioMed Diagnostics, White City, OR).
Statistical analysis
Prevalence of STIs was calculated at baseline, and incidence of STIs was calculated at 12 months based on participants who had both baseline and 12-month samples available. Relative risks were then calculated both at baseline and 12 months to assess the specific demographic risks associated with prevalent and incident STIs. Statistical analyses were performed with SPSS software (version 13.0; SPSS, Chicago, IL). A p value less than 0.05 was considered statistically significant.
Results
At the time of enrollment, of the 480 high-risk HIV-uninfected individuals; 49% were male, with a mean age of 31 years; 88% identified Tamil as their mother language. Twenty-three percent were single, 54% married, 18% living with a partner, and 5% widowed or divorced. Close to a fifth (18%) reported no formal education and 21% were unemployed (Table 1).
Over two fifths of men (42.6%) had nonprimary female sexual partners, 12.7% of men had a primary female sexual partner, 3.2% of men had ever had males as their sexual partners, 8.6% of men had both female and male sexual partners, and 9.8% of men disclosed no current sexual partner. Over two-fifths of women (46.2%) had a primary male sexual partner, 52.5% of women had non-primary male sexual partners, and 1.3% disclosed no current sexual partner.
At the time of enrollment into the study, 50% of women and 29% of men tested positive for HSV-2, 11% of women and 8% of men for syphilis, 6% of women for Trichomonas vaginalis, 5% of women and 0.65% of men for Chlamydia trachomatis, 2% of women for Neisseria gonorrheae, and 5% of women and 5% of men for HBsAg (Fig. 1).
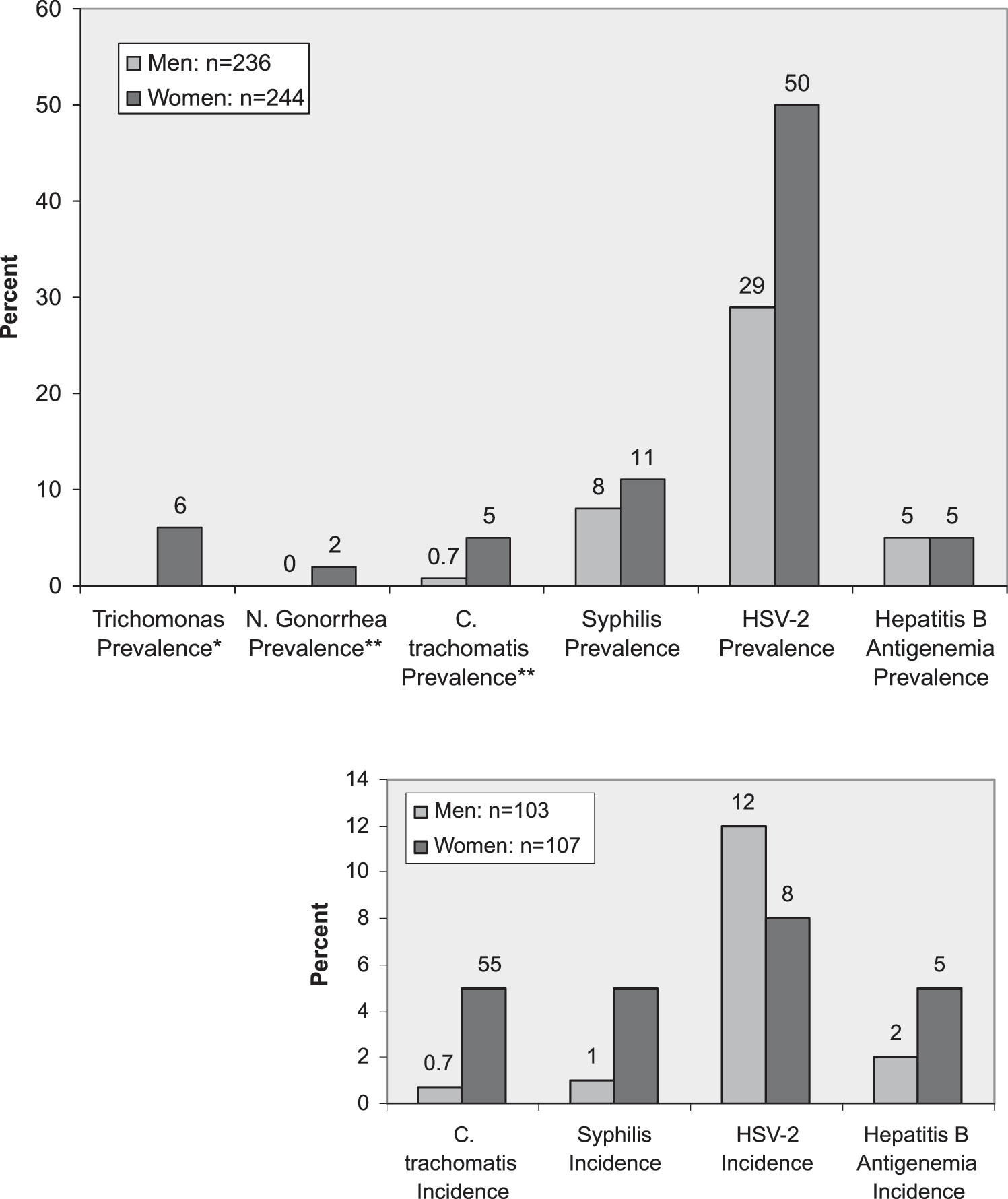
Prevalence at enrollment (n = 480) and incidence after 12 months (n = 207) of sexually transmitted infections (STIs) and Hepatitis B among study patients. *NA, not applicable for male participants; **126 participants (81 men and 45 women) refused to provide urine or vaginal secretions for testing at enrollment
At the time of enrollment, women were 8 times more likely to test positive for chlamydia (relative risk [RR]: 7.8, 95% confidence interval [CI]: 1.01–60.0, p = 0.01) and were 1.7 times more likely to test positive for HSV-2 (RR: 1.7, 95% CI: 1.35–2.17, p = 0.0001) than men. Participants who never went to school were 9 times more likely to test HbsAg positive (RR: 8.95, 95% CI: 1.80 – 44.5, p = 0.005), twice as likely to test positive for syphilis (RR: 1.9, 95% CI: 1.08-3.61, p = 0.03), 1.7 times more likely to test positive for chlamydia (RR: 1.7,95% CI: 1.3–2.1, p = 0.001), and 1.6 times more likely to test positive for HSV-2 (RR: 1.6, 95% CI: 1.3–2.1, p = 0.0001) than those participants who had undergone some formal education. Unemployed participants were 1.6 times at risk to test positive for syphilis (RR: 1.6, 95% CI: 1.3–2.03, p = 0.001) than employed participants. Married participants were less likely to be infected with HSV-2 (RR: 0.7, 95% CI: 0.61–0.95, p = 0.01) than single participants. Participants who had greater than four sexual partners in the past 6 months were more likely to be infected with syphilis (RR: 2.74, 95% CI: 1.43–5.28, p = 0.01) and HSV-2 (RR: 1.32, 95% CI: 1.02–1.70, p = 0.04) than those participants who had less than four partners in the past 6 months.
At the end of the 12-month follow-up period, HSV-2 was the most common incident STI with 8% of women and 12% of men testing positive (Fig. 1). One percent of men and 5% of women tested positive for syphilis, 1% of men and 3% of women for Chlamydia trachomatis, and 2% of men and 5% of women for HBsAg. Participants who had undergone no formal education were four times more likely to develop a new syphilis infection (RR: 4.00, 95% CI: 1.26–12.68, p = 0.03) than those participants with some formal education. There was no association between number of current sexual partners, gender, employment, or marriage status with the risk of developing any of the other STIs accessed in this study.
Discussion
This study demonstrates the high prevalence of untreated STIs, including syphilis, HSV-2, and hepatitis B, with high rates of incident sercoversion of Hepatitis B and HSV-2 after 1-year of follow-up in a population of South Indians at increased risk of HIV infection. Recent studies have documented varying rates of STIs among South Asian cohorts. In a cohort of slum dwellers in Bangladesh, a high rate (>5%) of syphilis was documented. 20 A study conducted among high-risk women in Western India found similar rates of trichomoniasis and chlamydia as this study, but much higher rates of N. gonorrhea. 13 Recent studies conducted in western and southern India have identified a high prevalence of HSV-2 14 , 15 However, an earlier multination study among antenatal clinic patients found relatively lower rates of HSV-2 among Indians with Indian women having lower rates of HSV-2 than their male counterparts. 9
In addition to unprotected sexual intercourse, STIs have been shown to be independent facilitators of HIV transmission and acquisition. 3 In this study, having more than four sexual partners in the past 6 months was significantly associated with HSV-2 and syphilis infection at enrollment. Although four times as many women had a primary sexual partner compared to men, women had equal or higher prevalence of all STIs accessed. Women were significantly more likely to test positive for HSV-2 and syphilis than men. This suggests that many of the high-risk Indian women in this study may have been infected by their male partners. The epidemiology of HSV-2 has been shown to differ between men and women with a greater probability of transmission from male-to-female than female-to-male. 6,21 Men with genital HSV-2 have been shown to have more recurrences than women, which may explain the higher rates of male-to-female transmission, 22 but a substantial number of HSV-2 transmissions may occur from asymptomatic partners as well. The findings of the current study suggest that HIV and STD prevention programs should promote women-controlled safer sex measures. Studies conducted in other Asian settings have similarly noted the need for gender-specific STI interventions in light of gender-related differences in HIV-related perceptions and sexual behaviors. 23,24
Through laboratory testing the current study likely provided diagnosis to many asymptomatic individuals who did not know their infectious status. Current Indian treatment guidelines recommend VDRL and HIV testing of patients engaging in high-risk activities as part of routine STI care to be delivered through general health services. 25 Prior studies from India have shown that a large number of individuals with STIs may be harboring asymptomatic STIs, 13,26 which could contribute to the silent transmission to the community. Another study from western India found that reported symptoms had little correlation with the presence of actual infection. 27 In this scenario, STI screening programs that target symptomatic individuals may not be adequate without laboratory-based testing.
The current study documented a high incidence of HBsAg positivity among study participants. A prior study in this part of India documented a similar level HBsAg community seroprevalence (5.7%). 28 Although the vaccine is available upon request in India, there is currently no routine hepatitis B vaccination program in place. Since sexual activity is the most commonly reported risk factor among persons with acute hepatitis B, STI clinics can serve as a particularly effective venue for delivering Hepatitis B vaccinations. 29,30 The findings of the present study support the need for a more proactive approach to vaccinate uninfected adults at risk for hepatitis B.
Greater findings of STI prevalence and incidence in diverse regional settings may help in the design of more effective HIV prevention strategies. A recent meta-analysis suggested that in areas of high HSV-2 prevalence, a high proportion of HIV in the general population is attributable to HSV-2. 6 In areas such as India with a high prevalence of HSV-2, as documented in this study, suppressive antiviral therapy solely against HSV-2 may have an impact on HIV transmission and acquisition. 31,32 Over the past decade, there has been substantial evidence to demonstrate that certain STIs enhance the transmission of HIV, although not all STI interventions may reduce HIV transmission. 10 Various models have suggested that STI treatment may have the greatest impact on HIV transmission rate early in a regional HIV epidemic. 10 In India where the national prevalence of HIV infection remains below 1%, programs should be developed that aggressively treat STIs in individuals at high-risk for HIV infection.
Due to the documented synergy between HIV and STIs, it has been suggested that the rapid diagnosis and treatment of STIs could serve as a cost-effective HIV prevention strategy. 4 In this study population, with the high incidence of syphilis and prevalence of other treatable STIs, targeted bacterial STI management strategies may help to slow the continued spread of HIV in India. However given the high rates of HSV-2 in this study population, for which there is no cure, this approach may require modification. Additionally, sexual histories and partner management should be a standard component of clinical care at STI clinics and centers providing voluntary counseling and testing (VCT) services for HIV. The prevalence rates of certain STIs, such as HSV-2 and syphilis in this study, may be high enough to warrant universal screening.
Footnotes
Acknowledgments
We are grateful to the clinical and laboratory staff of the YR Gaitonde Centre for Research and Education (YRG CARE), Chennai, India, for their generous facilitation of the study. We would like to thank the AIDS International Research and Training Program of the Fogarty International Center of the National Institutes of Health (NIH) (Grant No. D43TW00237), the Lifespan/Tufts/Brown Center for AIDS Research (CFAR) (Grant No. P30 AI42853), and the HIV Prevention Trial Network 052 (HPTN) of the NIH (Grant No. 5U01 A148040-02), for financially supporting this study.