
Abstract
The role of psychological factors in predicting HIV sexual transmission risk behavior is increasingly of interest in prevention research. Social anxiety, or anxiety about being evaluated in interpersonal situations, is associated with unprotected insertive anal intercourse among young men who have sex with men (MSM) and with other behavioral risk factors for unprotected intercourse, such as depression, smoking, alcohol use, and drug use. Social anxiety may be especially relevant in understanding HIV risk among HIV-seropositive men, given its stronger association with unprotected insertive than with receptive anal intercourse. In the present study, for which participants were recruited between October 2002 and May 2003, HIV-positive men attending regularly scheduled primary care medical appointments at a community HIV clinic were approached by research personnel and informed about the study topic and procedures. Ninety percent of patients approached agreed to participate, resulting in a sample of 206 patients. The sample was primarily African American, unemployed, of low educational level, and 95% of the sample had an AIDS diagnosis. The present study replicated and extended previous research from community samples by demonstrating an association between social anxiety and unprotected insertive anal intercourse with non-HIV-positive partners in a clinical sample of HIV-positive MSM and men who have sex with women (MSW). This association was maintained controlling for depression, smoking, and club drug use. Social anxiety is a relatively robust risk factor for unprotected insertive anal intercourse among MSM. Future work should examine the mechanisms by which social anxiety is associated with sexual risk among MSM.
Introduction
T
In the only published study to date examining the relationship of social anxiety to unprotected intercourse 10 the investigators looked at two types of social anxiety in a sample of young MSM (ages 16–21) from community settings: social interaction anxiety, or anxiety about interacting with others in dyads or groups, and social performance anxiety, or anxiety about engaging in acts in front of others. Social performance anxiety was associated with unprotected insertive anal intercourse among young MSM, even when accounting for social support and communication about condom use. 10 Neither form of social anxiety was associated with unprotected receptive anal intercourse.
Given the paucity of research in this area and the potential importance of social anxiety as a mental health factor affecting HIV risk behavior, the current study was conducted to replicate and extend previous findings by examining associations between social anxiety and unprotected sexual transmission risk among HIV-seropositive male patients recruited from an HIV clinic. Previous literature has failed to find a consistent association between negative affect (anxiety, depression, and anger) and unprotected intercourse. 14 However, most studies on negative affect and HIV risk have focused on the role of depression and not anxiety. Further, most studies have examined anxiety as a unitary construct 15 –17 despite evidence of several distinct types of anxiety in both clinical and normative populations. 18,19 As such, it has been suggested that future studies provide greater specificity as to which types of anxiety are associated with HIV risk behaviors. 17 In the present study, high social performance anxiety was hypothesized to be associated with unprotected insertive anal intercourse with non-HIV-positive partners among MSM. Given that depression has been found to be associated with unprotected sex among MSM, 20 –22 and is typically correlated with social anxiety, 23,24 the associations between social performance anxiety with unprotected sex were examined controlling for depression. Other risk factors for unprotected sex, such as smoking, 25 alcohol use, 26 –28 and use of club drugs such as ecstasy, ketamine, cocaine, GHB, and crystal methamphetamine, 26,29 –32 were also controlled for in the present study to examine if social performance anxiety would be a robust correlate of unprotected insertive and receptive anal intercourse in multivariate analyses. Given that there is a lack of data on social performance anxiety and unprotected insertive sex among men who have sex with women only (MSW), analyses were also conducted to examine if social performance anxiety is associated with unprotected insertive sex among MSM only, or also among MSW.
Methods
Subjects
Data were collected from 206 HIV-positive men in a large, public HIV clinic in Atlanta, Georgia. Of these, 84 (40.4%) were MSM, 54 (26.0%) were MSW, and 70 (33.7%) reported being abstinent from sex with either a male or female partner in the past 6 months. Fourteen of the MSM had also had sex with women. Participants had a mean age of almost 42 years old, were primarily African American, and unemployed. Almost two thirds completed high school or less. Mean CD4 count was 226.28 (standard deviation [SD] = 211.31; range, 4–1181). Viral loads were detectable in 83.7% of participants (range, 400 to ≥750,000), with 28 (13.3%) showing undetectable viral loads. The sample medical data were representative of the larger clinic population, which specializes in care for patients with advanced HIV disease. For example, the proportion of patients with an AIDS diagnosis in the present sample is 95%, which is similar to the clinic AIDS prevalence of 91%. Demographic and medical characteristics of the study sample are found in Table 1.
MSM, men who had sex with men; MSW, men who had sex with women only. Categories refer to sexual activity in the past 6 months. Percentages may not add up to 100% because of rounding.
Procedures
Participants were recruited for the study between October 2002 and May 2003. HIV-positive men attending regularly scheduled primary care medical appointments at a community HIV clinic were approached by research personnel and informed about the study. Most (90%) agreed to participate. Data were collected via Audio Computer-Assisted Self-Interviews (A-CASI) and a brief clinical interview. Medical information was abstracted from medical records within 1 week of the interview. Participants received a $10 incentive for their participation. All research activities were approved in advance by Institutional Review Boards at Emory University and the Centers for Disease Control and Prevention.
Measures
Demographics questionnaire
Participants completed a demographics questionnaire assessing age, ethnic/racial background, education level, income, and sexual orientation.
Social anxiety
Social anxiety was assessed using the Social Interaction Anxiety Scale and the Social Phobia Scale (SIAS and SPS), 33 which are commonly used companion 20-item measures designed to assess two related but distinct domains of social anxiety: social interaction anxiety (e.g., “I feel I'll say something embarrassing when talking”) and social performance anxiety (e.g., “I feel awkward and tense if I know people are watching me”), respectively. The SIAS and SPS each consist of 20 items and are rated on a 5-point Likert-type scale ranging from 0 = “not at all characteristic of me” to 4 = “extremely characteristic of me.” Total scores for each scale range from 0–80, with higher scores indicating higher social interaction anxiety or higher social performance anxiety, respectively. Both scales were highly internally consistent in adult community and young MSM samples (all α ≥ 0.88) and demonstrated good test-retest reliability and validity. 10,34 Internal consistencies in this sample were α = 0.86 and 0.92, respectively.
The Liebowitz Social Anxiety Scale (LSAS), 35 a clinician-administered psychiatric interview, evaluated anxiety in 11 social interaction (e.g., talking to people in authority) and 13 social performance (e.g., working while being observed) situations using a 4-point Likert-type scale (for anxiety 0 = none, 3 = severe; for avoidance 0 = never; 3 = usually). The social interaction anxiety scale ranges from 0 to 33 and the social performance scale ranges from 0 to 39, with higher scores indicating higher social anxiety. The LSAS social interaction anxiety and social performance anxiety scales demonstrate excellent validity and excellent internal consistency in clinical samples 36 and in the present sample (α = 0.83 and 0.86, respectively).
Depression
Depression was measured using the 21-item, self-report Beck Depression Inventory-II (BDI-II). 37 The BDI-II contains 21 groups of statements about depression. Participants indicate the statement within each group that best describes their symptoms in the past 2 weeks. Scores for each item range from 0 to 3 and total scores range from 0 to 63, with higher scores indicating greater depression. It is highly correlated with the original BDI 38 in both nonclinical and clinical samples (rs = 0.93). 37,39 In the current study, the internal consistency was α = 0.91.
Unprotected sexual behavior
Participants were asked to indicate their frequency of insertive and receptive anal intercourse with men and vaginal intercourse with women, with and without a condom in the previous 6 months with non HIV-positive partners (HIV-negative or unknown serostatus). These variables were not normally distributed and so were dichotomized into 1 = yes and 0 = no engagement in a sexual behavior.
Additional measures
Participants indicated if they had been intoxicated when drinking alcohol, used a given drug commonly used by MSM at clubs (methamphetamine, ecstasy, GHB, ketamine, and cocaine), as well as other drugs (other amphetamines, marijuana, heroin, methadone, barbiturates, inhalants, speedball, and hallucinogens) in the previous 6 months. For each alcohol intoxication and use of a drug, participants could indicate they had used a substance 0 times, 1–10 times, 11–20 times, or 30 or more times. Due to non-normal distribution of data for these variables, each variable was recategorized into 0 times or at least once in the previous 6 months. CD4 count and viral load were abstracted from participants' medical records.
Data analysis
An analysis of variance (ANOVA) with Scheffé post hoc tests examined differences in social anxiety among the three groups in the sample (MSM, MSW, and abstinent men). To examine if social anxiety was associated with unprotected insertive sex among MSM only, or among MSW as well, a logistic regression was conducted with unprotected insertive sex (anal intercourse for MSM, and vaginal intercourse for MSW) as the dependent variable, and high versus low social performance anxiety on step 1 and the interaction between social anxiety group and unprotected insertive sex on step 2. Logistic regressions examined associations between men high and low in social anxiety and demographic and medical variables. Finally, multiple logistic regressions were computed with unprotected intercourse with non-HIV partners as the dependent variable. Each variable associated with the dependent variable in univariate analyses at p < 0.10 (depression, club drug use, and tobacco use but not social anxiety) was entered on step 1 and social anxiety on step 2.
Results
Associations of demographic variables with social anxiety and unprotected sex
There were significant differences among MSM, MSW, and abstinent men in LSAS social interaction anxiety scores, F(2, 203) = 4.07, p = 0.02 (3 cases had missing data for abstinent men on this scale). MSW (M = 12.68, SD = 5.90) had higher scores than MSM (M = 9.17, SD = 7.41, p = 0.02) on this scale. For MSM, MSW, and abstinent men, no demographic and medical variables were associated with social anxiety variables except that MSM with high LSAS social interaction anxiety (odds ratio [OR] = 3.23, 95% confidence interval [CI] = 1.29–8.11, p = 0.01), and MSM with high LSAS social performance anxiety (OR = 4.90, 95% CI = 1.90–12.64, p = 0.001), were more likely to have an income less than US $10,000 per year. None of the demographic variables or medical status variables was associated with either unprotected insertive or unprotected receptive anal intercourse among MSM, or unprotected vaginal intercourse among MSW with non-HIV-positive partners.
Predictors of unprotected intercourse with non-HIV-positive partners
Unprotected insertive intercourse among MSM and MSW
Table 2 presents the significant interaction between SPS scores and MSM/MSW status above and beyond main effects of high versus low SPS score and MSW/MSW status. To more fully explore the interaction, the effects of SPS score on unprotected insertive intercourse were examined separately for MSM versus MSW. Among MSM, high SPS score was associated with a greater likelihood of engaging in unprotected insertive intercourse, OR = 15.40, 95% CI = 1.89–125.77, p = 0.01. Among MSW, there was no association between SPS score and unprotected intercourse. The prevalence of unprotected insertive intercourse among MSM versus MSW by SPS score are presented in Figure 1. Per findings of a significant interaction, further results are examined separately for MSM versus MSW.
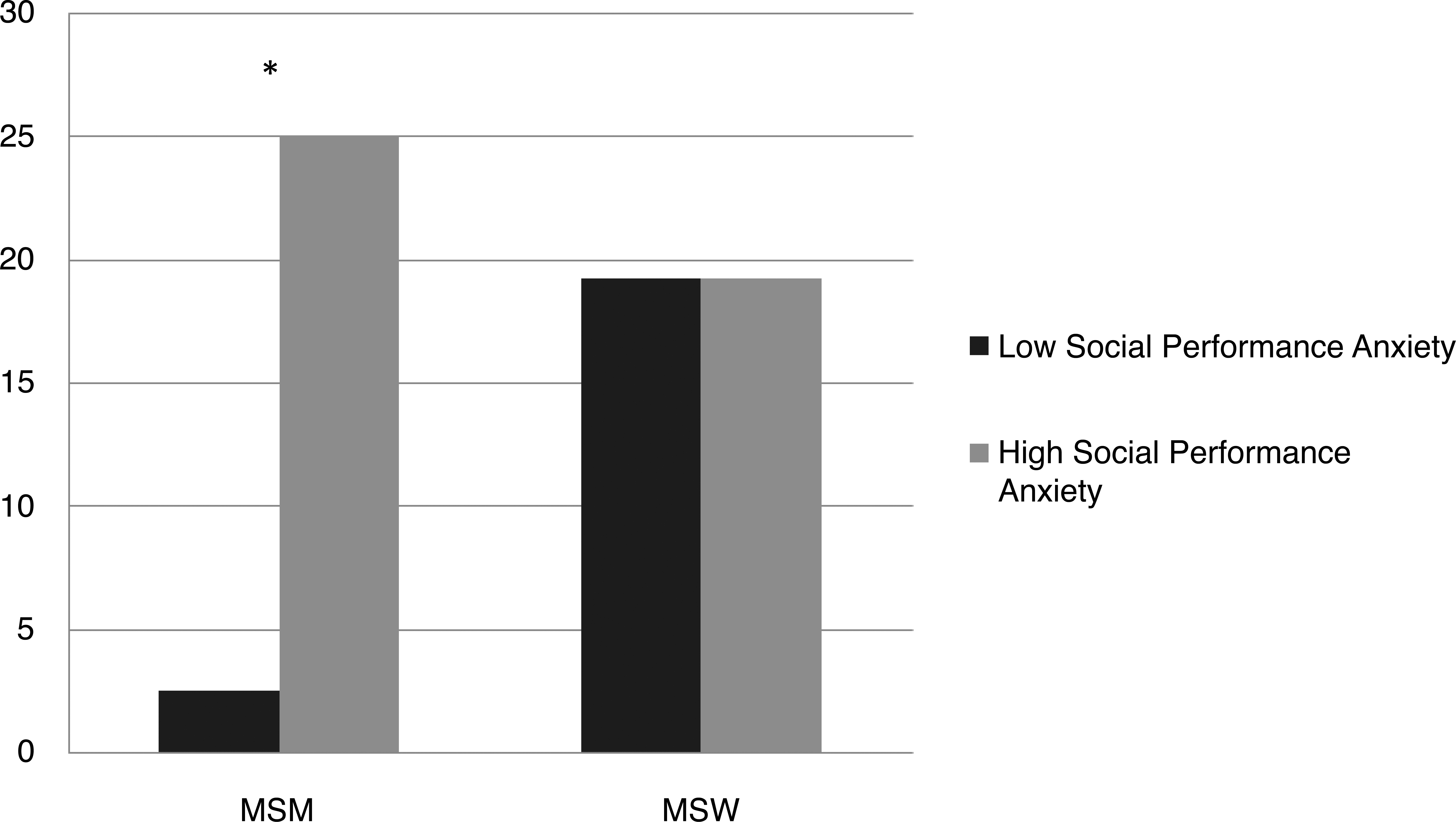
Proportion engaging in unprotected insertive intercourse among men who have sex with men (MSM) and men who have sex with women (MSW) with high versus low social performance anxiety on the Social Phobia Scale (SPS). *p = 0.02 for differences between MSM with high versus low social performance anxiety.
SPS, Social Phobia Scale.
MSM: unprotected insertive anal intercourse
High social performance anxiety as assessed by the SPS and by the LSAS, and social interaction anxiety as assessed by the LSAS were all associated with greater likelihood of engaging in unprotected insertive anal intercourse. High depression, use of tobacco, and club drug use were also associated with engaging in unprotected insertive anal intercourse. Simple logistic regressions of variables associated with unprotected insertive anal intercourse with non-HIV-positive partners among MSM are presented in Table 3. In the multiple logistic regression, to avoid multicollinearity among the highly correlated social anxiety predictor variables and to be consistent with previous research, 10 social performance anxiety as assessed by the SPS was entered among the social anxiety variables in the first model. Step 1, including all variables at p < 0.10, was significant, χ2 = 16.69, p = 0.001, Nagelkerke R 2 = 0.33, with only depression emerging as an independent predictor, OR = 6.07, 95% CI = 1.17–31.51, p = 0.03. Step 2, adding social anxiety, was significant, χ2 = 6.22, p = 0.01. Social performance anxiety (SPS) predicted unprotected insertive anal intercourse with non-HIV-positive partners above and beyond the other variables in the model and accounted for an additional 11% of the variance. Only social performance anxiety was a significant independent predictor in the final model, OR = 9.98, 95% CI = 1.11– 89.90, p = 0.04. Multivariate analyses were then repeated with depression, club drug use, and tobacco use entered on Step 1 and social performance anxiety entered on step 2 and unprotected receptive anal intercourse with non-HIV-positive partners as the dependent variables. None of these variables were independently associated with unprotected receptive anal intercourse with non-HIV partners in this second model.
An odds ratio cannot be calculated for tobacco use and unprotected insertive anal intercourse with non-HIV–positive partners, as all people who engaged in this sexual behavior were tobacco users. However, the χ2-statistic is significant.
SPS, Social Phobia Scale; LSAS, Liebowitz Social Anxiety Scale.
To examine whether social performance anxiety was related to engagement in sexual behavior whether or not condoms were used (e.g., having insertive anal intercourse) instead of being specifically associated with unprotected insertive anal intercourse with non-HIV-positive partners, logistic regressions were computed with each social anxiety variable as the independent variable and sexual behavior as the dependent variable. None of the social anxiety variables predicted having engaged in any anal intercourse, any insertive anal intercourse, or any receptive anal intercourse with non-HIV-positive partners.
MSM: unprotected receptive anal intercourse
Only club drug use (OR = 3.08, 95% CI = 1.01–9.36, p = 0.047) was associated with having engaged in unprotected receptive anal intercourse with non-HIV-positive partners.
MSW: Unprotected vaginal intercourse
Social anxiety variables, depression, and substance use variables were not associated with unprotected vaginal intercourse with non-HIV-positive partners among MSW. There was a trend for an association between heroin use and unprotected vaginal intercourse with non-HIV-positive partners, OR = 10.25, 95% CI = 0.83–127.03, p = 0.07.
Possible differences in sexual transmission risk behavior between groups
To examine if differences in the pattern of association between social performance anxiety and unprotected insertive intercourse among MSM versus MSW were due to differences in prevalence of sexual transmission risk behavior between MSM and MSW, a variable was computed indicating the presence of any unprotected sex (vaginal, insertive anal intercourse, and/or receptive anal intercourse) with non-HIV-positive partners in the past six months (Table 1). There were no differences between the two groups in proportion engaging in HIV sexual transmission risk behavior, even controlling for MSM being slightly older than MSW (t[133] = 2.21, p = .03), and more likely to have graduated college (19% versus 2%, χ2 [1, n = 135] = 8.42, p = 0.01).
Discussion
The present study suggests that high social performance anxiety, which has hitherto been unexplored as a risk factor for HIV sexual transmission risk among HIV-positive individuals, is associated in a clinical sample of HIV-positive MSM with a significantly increased odds of engaging in unprotected insertive anal intercourse with non-HIV-positive partners. Specifically, sexual transmission risk appears to be more closely associated with social performance anxiety, or anxiety about being evaluated negatively when performing a behavior, than with anxiety about social interactions. The present study replicates findings among a community-based sample of young MSM that social performance anxiety was associated with unprotected insertive anal intercourse, 10 and extends these findings by demonstrating that social performance anxiety is associated with this high-risk behavior controlling for club drug use, tobacco use, and depression, all of which have been linked to HIV risk behaviors in previous studies. 29,40 Findings also suggest that social performance anxiety may be a specific risk factor for MSM and not all HIV-positive men.
To date, consideration of social anxiety as an HIV sexual transmission risk factor has been limited in comparison to such factors as depression and recreational drug use. Given that unprotective insertive anal intercourse is one of the behaviors most likely to transmit HIV to others, 41 these findings suggest that social anxiety in HIV-positive MSM, particularly performance anxiety, is an important psychological factor to address in the development and implementation of HIV risk reduction interventions. If socially anxious MSM are at increased risk of having unprotected anal intercourse, then HIV prevention interventions incorporating social anxiety-related concerns may not only reduce social fear and related psychological impairment (see Rodebaugh et al. 42 for a review of social anxiety treatments), but may also decrease the threat of transmitting HIV among MSM. Further work examining the mechanisms by which social anxiety may potentially lead to risky sex would be useful when designing these interventions.
The present study is limited by its small sample size, which may have limited statistical power for social interaction anxiety as assessed by the SIAS and other non-social anxiety measures. The sample size also limited ability to assess individual club drugs increasingly associated with sexual risk among HIV-positive MSM such as crystal methamphetamine. 32 Clinical interviews were used along with self-report measures only for social anxiety, with self-report measures only for depression, smoking, and substance use. Future research should therefore examine if findings would be maintained using multiple assessments for non-social anxiety measures. The sample was also recruited from a clinic primarily serving patients diagnosed with AIDS, with the vast majority of patients sampled having a detectable viral load and low CD4 counts. Future studies may wish to examine whether social anxiety may predict risky sexual behavior among patients with less advanced HIV disease.
Several possible directions for future research in this area are suggested by the finding of the current study. For instance, it would be useful to further elucidate the mechanisms by which social performance anxiety might influence patterns of unprotected insertive intercourse among MSM. Given that motivations to reduce anxiety in social situations has also been associated with engaging in sexual intercourse under the influence of crystal methamphetamine among MSM, 31,43 some MSM may use be using drugs to cope with anxiety when interacting or performing sexual acts with potential or actual partners. The role of social anxiety in crystal methamphetamine use is especially useful to examine given that crystal methamphetamine use is associated with unprotected anal intercourse among MSM and STI infection. 44 –46 Further, given the consistency in findings that social performance anxiety is a predictor of insertive anal intercourse, it is quite possible that sexual performance anxiety and specifically fear of erectile difficulties 47 may mediate the relationship between social performance anxiety and lack of condom use as the insertive partner. It is also possible that a third variable may moderate the association between social performance anxiety and unprotected anal intercourse, such as perceived support from friends for engaging in condom use or attitudes toward barebacking versus condom use. 48,49 Lastly, future studies may wish to examine how social anxiety influences transmission risk behavior across different types of sexual relationships, such as with primary partners versus casual partners. These research questions can be assessed using structural equation modeling or other methods that are useful for testing theories of how social anxiety may be related to sexual risk behaviors among MSM with multiple measures examined in a single analysis.
It may also be useful to examine other ways in which social anxiety affects the lives of HIV-positive MSM. A substantial proportion of HIV-positive individuals report experiencing HIV/AIDS stigma by noticing that others avoid being near them or exclude them from social events because of their HIV status. 50 Among HIV-positive MSM, internalized stigma is associated with higher anxiety, 51 which could be in part due to social anxiety about being judged negatively for being HIV positive, but this association needs to be examined in future research. The higher social interaction anxiety among MSW than among MSM may be due to the higher internalized stigma among heterosexual than among non-heterosexual HIV-positive populations. 51 HIV/AIDS stigma may be associated with greater social anxiety among HIV-positive populations in general, thereby potentially increasing risky sexual behavior.
Finally, future research in this area might focus on the effects of social anxiety on other forms of psychosocial impairment found among HIV-positive individuals, such as psychiatric comorbidity, homelessness, and low quality of life. 52 As a psychiatric diagnosis of social anxiety disorder 18 is associated with even higher social anxiety than was found in the present study of nonpsychiatric patients, an examination of the effects of social anxiety disorder on sexual risk behavior among HIV-positive persons is also warranted.
Footnotes
Acknowledgments
This research was supported in part by a micro grant award from the Developmental Core of the Emory Center for AIDS Research (Grant number P30 AI050409). Portions of this paper were presented at the 2004 International AIDS Conference.
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.