
Abstract
Few data exist on the safety of tenofovir (TDF) in HIV-infected patients with preexisting renal dysfunction. We report 12-month changes in renal profiles among 19 such patients (6 patients with history of and 13 patients with current renal disease) in the HIV Outpatient Study (HOPS) who initiated TDF-containing highly active antiretroviral therapy (HAART) during 2001–2005 with TDF dosed mostly at 300 mg once daily. At baseline, the median estimated glomerular filtration rate (GFR) was 49 mL/min/1.73 m2 and the median CD4+ cell count was 322 cells/mm3. Patients had a median 12-month change in estimated creatinine clearance from baseline of −0.3 mL/min (range, −32.2 to +23.6) and the median change in GFR of −0.1 mL/min/1.73 m2 (range, −49.8 to +29.5). We observed confirmed worsening of kidney disease stage in 5 of the 19 patients during follow-up. TDF use can be considered in patients with preexisting or current renal dysfunction who have limited antiretroviral treatment options, require TDF for fully active antiretroviral regimen, and can be closely monitored for incident worsening of renal function.
Introduction
K
Tenofovir disoproxil fumarate (TDF), has been demonstrated to be safe and generally well tolerated for treatment of HIV-1 infection, 5 and has not been associated with substantial renal toxicity in randomized placebo-controlled clinical trials of patients with normal baseline renal function. 6 –10 However, cases of severe renal dysfunction 11 –14 and population-level reductions in creatinine clearance (CrCl) among TDF-treated patients have been reported in observational studies postlicensure. 15 –19 Few analogous data exist for patients with preexisting renal dysfunction who start TDF-containing HAART. In this report, we examined renal profiles among HIV-infected patients with preexisting renal dysfunction who received TDF-containing HAART in the HIV Outpatient Study (HOPS).
Methods
HOPS is a prospective cohort study of HIV-infected patients seen at 10 clinics (public and private) specializing in treatment of HIV disease in seven cities in the United States. HOPS has collected sociodemographic and clinical data abstracted from medical charts on about 8000 patients from 1993 to date.
We analyzed antiretroviral-experienced patients enrolled in the HOPS who received more than 1 month of TDF-containing HAART after November 1, 2001. Observation time began at baseline, defined as the start date of first TDF-containing HAART. Observation was censored at 36 months after baseline, at the time patient discontinued TDF-containing HAART, at death, at loss to follow-up, or on September 30, 2005, whichever occurred first. Subjects were included if they had serum creatinine measured at least once within 6 months prior to starting TDF-containing HAART and at least twice more during follow-up; and if they met criteria for one of the following two subgroups: (1) prior clinical diagnosis of renal insufficiency but baseline creatinine < 1.5 mg/dL and CrCl > 50 mL/min (past renal dysfunction) or (2) baseline creatinine ≥ 1.5 mg/dL and/or CrCl < 50 mL/min, and at least one prior creatinine ≥ 1.5 mg/dL (current renal dysfunction). Subjects were excluded if they had prior or concurrent exposure to adefovir or cidofovir; concurrent pregnancy; or were undergoing renal dialysis.
Creatinine clearance was estimated by the Cockcroft-Gault (CG) equation 20 using age and weight closest in time to the serum creatinine measurement (±3 months); 90% of patients had weight measured within 20 days of serum creatinine. Glomerular filtration rate (GFR) was estimated by the simplified Modification of Diet in Renal Disease (MDRD) equation. 21 Renal disease was staged using the National Kidney Foundation (NKF) classification system by MDRD.
Results
Nineteen patients met inclusion criteria: 79% were male, the median age was 48 years, the median CD4+ cell count was 322 cells/mm3 and the median time since HIV diagnosis was 10.1 years. The characteristics of the subjects are shown in Table 1. Past or current diagnoses included hypertension (9 persons, 48%) and diabetes (2 persons, 11%). Patients' median baseline creatinine was 1.7 mg/dl, median estimated CrCl was 56 mL/min, and median estimated GFR was 49 mL/min/1.73 m2. Six subjects had a prior history of renal dysfunction with normal pretreatment renal parameters; 13 subjects had current renal dysfunction. At baseline, no patient had a NKF GFR stage greater than 3. The median length of follow-up was 13 months (range, 6–35) with a median of 5 creatinine determinations (range, 2–16). Seventeen subjects received TDF dosed at 300 mg once daily; 2 subjects received TDF dosed at 300 mg thrice weekly.
Increase in NKF stage from baseline confirmed by one or more consecutive values.
Additional diagnoses included interstitial nephritis and glomerulonephritis.
RI, renal insufficiency; HTN, hypertension; DM, diabetes; HCV, hepatitis C coinfected; Cr, creatinine; 3TC, lamivudine; ABC, abacavir; APV, amprenavir; ATV, atazanavir, AZT, zidovudine; ddI, didanosine; DLV, delavirdine; EFV, efavirenz; FTC, emtricitabine; LPV, lopinavir; NKF, National Kidney Foundation; NVP, nevirapine; Rtvld, low-dose ritonavir; SQV, saquinavir; T20, enfuvirtide; TDF, tenofovir.
TDF dosing 300 mg daily, unless otherwise specified; 3W = thrice weekly.
During follow-up, a confirmed increase in NKF stage by one or more stage (i.e., worsened renal dysfunction based on 2 consecutive NKF values) was documented in 3 of the 6 patients who had past renal dysfunction and among 2 of the 13 patients with current renal dysfunction, 1 of whom progressed from stage 3 to stage 5 (Table 1). Among 15 subjects with 12 months of follow-up, the mean change in CrCl from baseline was −0.8 mL/min (median, −0.3; range, −32.2 to +23.6) and the mean change in GFR was −1.3 mL/min/1.73 m2 (median, −0.1; range, −49.8 to +29.5). Among the 10 of 13 patients categorized as having current renal dysfunction, the mean 12-month change in CrCl was +2.9 mL/min (median, +4.6; range, −24.0 to +23.7) and the mean change in GFR was +3.7 mL/min/1.73 m2 (median, +7.5; range, −24.3 to +29.5) (signed rank test for changes, p > 0.05 for all; Fig. 1).
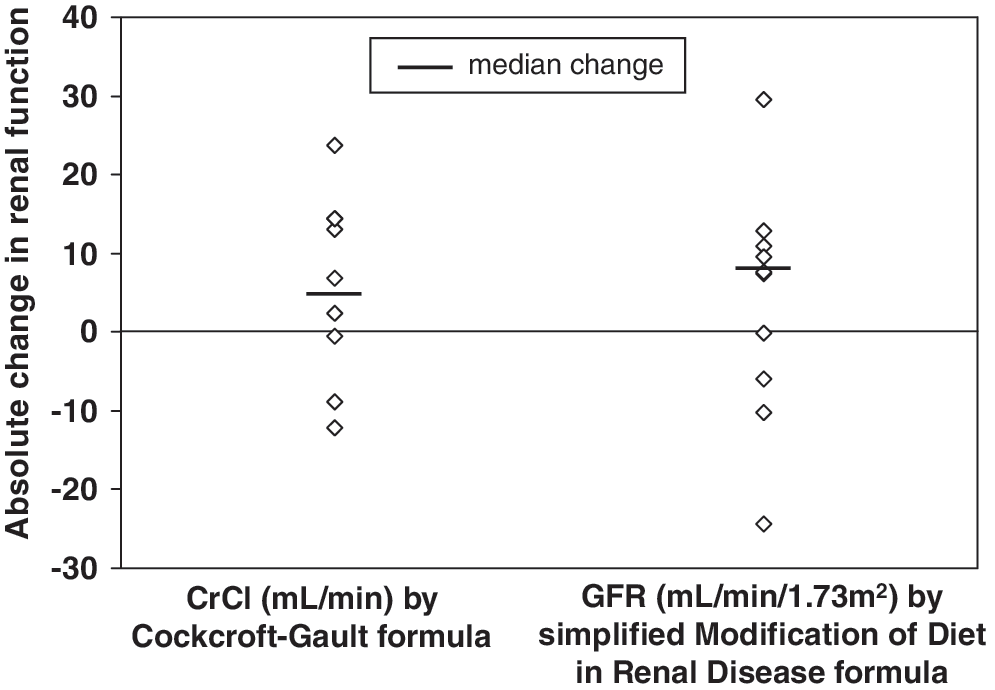
Changes in renal function amount 10 patients categorized as having current renal dysfunction with both baseline and 12-month values, HIV Outpatient Study, November 2001 to September 1005. CrCl, creatinine clearance; GFR, glomerular filtration rate.
At the end of observation in our analyses, 10 of 19 patients discontinued TDF (including all 5 patients with confirmed increase in NKF stage), except for patient E who continued on TDF-containing regimen (Table 1). Apart from the 2 patients who started on TDF dosed at 300 mg thrice weekly, no other patients had documentation of TDF dose adjustment during follow-up.
Discussion
Previous studies on the safety profile of TDF in HIV-infected persons generally excluded persons with preexisting kidney disease. In this historical case series of HIV-infected patients with past or current renal dysfunction who received TDF-containing HAART (most of whom received higher than currently recommended TDF dosing and had concomitant comorbid risk factors for renal disease), incident worsening of NKF stage was observed, but many patients in this high-risk patient group did not experience a worsening of NKF stage during a median 13 months of follow-up. Of note, a significant number of patients with a past history of renal dysfunction experienced decreases in renal function; one patient (patient G, Table 1) with current renal disease developed reached NKF stage 5 (and discontinued TDF).
This analysis is limited by small sample size. Additionally, in clinical cohorts such as the HOPS, the use of TDF may have been avoided in many patients with baseline renal insufficiency, particularly after rare but severe renal toxicities were first reported, 11,12 introducing the potential for selection bias in our study. Although we analyzed the changes in CrCl and GFR while patients remained on TDF-containing regimen, it must be noted that because some patients discontinued the drug, the magnitude of change in CrCl or GFR we calculated may (unavoidably) underestimate the degree of renal decline that may have been observed had the patients continued on TDF. Because blood specimens were obtained from routinely collected clinical samples, there was no fixed schedule of creatinine measurements and multiple laboratories were used. Diagnoses of incident renal disease were made by the treating physician at each HOPS site according to their clinical training and experience and not by otherwise standardized criteria. Additionally, because of a relative paucity of routine urinalyses, rates of glycosuria or proteinuria are not reported.
This small historical case series of heterogeneous patients reinforces the potential for renal injury in at-risk persons who receive TDF at higher than currently recommended doses. 4 However, the results also suggest that TDF can be considered in patients with past or current renal dysfunction (NKF stage ≤3) who have limited antiretroviral treatment options and in whom the use of TDF is required to construct a fully active regimen. Clinicians should adjust TDF dosing appropriately based on baseline renal function, and monitor renal function at least biannually for incident worsening. 4
Footnotes
Acknowledgments
We thank the thousands of HOPS patients for their ongoing generous participation in the study.
The HOPS study is funded by the Centers for Disease Control and Prevention (contract no. 200-2006-18797).
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
The HOPS Investigators include the following investigators and sites: J.T. Brooks, K. Buchacz, A.C. Moorman, and T. Tong, Division of HIV/AIDS Prevention, CDC, Atlanta, GA; K.C. Wood, R.K. Baker, C. Armon, J.T. Richardson, Cerner Corporation., Vienna, VA; F.J. Palella, J.S. Chmiel, J. Cheley, Feinberg School of Medicine, Northwestern University, Chicago, IL; K.A. Lichtenstein, University of Colorado Health Sciences Center, Denver, CO; K.S. Greenberg, B. Young, B. Widick, C. Stewart, and P. Zellner, Rose Medical Center, Denver, CO; B.G. Yangco, K. Halkias, Infectious Disease Research Institute, Tampa, FL; D.J. Ward and C.A. Owen, Dupont Circle Physicians Group, Washington, DC; J. Fuhrer, L. Ording-Bauer, R. Kelly, and J. Esteves, State University of New York (SUNY), Stony Brook, NY; E.M. Tedaldi, R.A. Christian, Temple University School of Medicine, Philadelphia, PA; R.M. Novak, Jonathan P. Uy, and A. Wendrow, University of Illinois at Chicago, Chicago, IL.
Author Disclosure Statement
B.Y. has received recent research grants from Bristol Myers Squibb, Gilead Sciences, Merck, Roche, and GlaxoSmithKline and/or is a member of advisory boards for Gilead Sciences, GlaxoSmithKline, Merck, Pfizer, Roche and Bristol Myers Squibb. Other authors have no competing financial interests exist.