
Abstract
A randomized, open-label, multicenter study was conducted to evaluate the therapeutic switch to a single-tablet formulation of efavirenz/emtricitabine/tenofovir DF (EFV/FTC/TDF) among virologically suppressed, HIV-1–infected subjects. Eligible subjects on stable antiretroviral therapy (ART) with HIV-1 RNA less than 200 copies per milliliter for 3 months or more were stratified by prior protease inhibitor (PI)- or non-nucleoside reverse transcriptase inhibitor (NNRTI)-based therapy and randomized (2:1) to EFV/FTC/TDF or to stay on their baseline regimen (SBR). Patient-reported measures were quality of life (QOL; SF-36 [version 2]), treatment adherence (visual analogue scale), preference of medication (POM), perceived ease of the regimen for condition (PERC), and a 20-item HIV symptom index. Overall, 203 subjects were randomized to EFV/FTC/TDF and 97 to SBR. Fifty-three percent of subjects had previously received a PI-based regimen; 47% an NNRTI-based therapy. Throughout the study, SF-36 summary scores did not differ significantly from baseline, regardless of previous ART or treatment allocation. Adherence was 96% or more in both groups at baseline and all subsequent study visits. At study conclusion, the EFV/FTC/TDF regimen was considered easier to follow than prior regimens by 97% and 96% of subjects previously receiving PI-based and NNRTI-based therapies, respectively. Overall, 91% of subjects switched to EFV/FTC/TDF indicated a preference over their prior therapy. Switching to EFV/FTC/TDF was associated with transient worsening/emergence of dizziness and sustained improvements in several other HIV-related symptoms. In conclusion, switching virologically suppressed, HIV-1–infected subjects from PI-based or NNRTI-based regimens to EFV/FTC/TDF was associated with maintained QOL and treatment adherence, and improved ease of use and treatment satisfaction.
Introduction
A
Various studies have been performed to evaluate the efficacy and safety of switching to once-daily EFV-based 6,7 or TDF/FTC-based regimens. 8,9 However, to date, this is the only study prospectively designed to examine the switch from a regimen not consisting of EFV, FTC, and TDF, to single-tablet EFV/FTC/TDF. 10 Primary results from this 48-week, open-label, randomized, multicenter study in subjects who were virologically suppressed (HIV-1 less than 200 copies per milliliter) while receiving a variety of protease inhibitor (PI)- or NNRTI-based ART regimens have been previously reported. 10 In brief, subjects who had their treatment simplified to single-tablet EFV/FTC/TDF maintained high rates of virologic suppression that were comparable to those who continued their ART regimen unmodified. Simplification to the EFV/FTC/TDF combination was also well tolerated, with low rates of discontinuation observed in subjects switching to EFV/FTC/TDF, as well as those continuing their original ART. 10 As an extension to the previously reported findings, the current report provides a comprehensive summary of patient-reported outcomes from this trial including quality of life (QOL), treatment adherence, treatment preference and ease of use, and change in common HIV symptoms.
Methods
Study design
This was a 48-week, open-label, randomized, multicenter study conducted in subjects infected with HIV-1 who had achieved virologic suppression on their current ART regimen. A detailed description of the study methods has been previously published. 10 In brief, subjects at 53 sites in the United States and 2 sites in Puerto Rico were randomized (2:1) to either simplify treatment to single-tablet EFV/FTC/TDF or to stay on their baseline antiretroviral regimen (SBR group). The randomized groups were equally stratified according to their existing PI-based (including ritonavir-boosted PI) or NNRTI-based treatment regimen. An Institutional Review Board or ethics committee at each site approved the study protocol and the informed-consent form.
Patients
Enrolled subjects included men or nonpregnant women, who were aged 18 years or older, had documented HIV-1 seropositivity, adequate renal function (defined as creatinine clearance 60 mL/min or greater according to the Cockcroft-Gault formula 11 ) and a life expectancy of 1 year or more. Enrolled subjects had to have a plasma HIV-1 RNA value less than 200 copies per milliliter using the Amplicor HIV-1 Monitor test, version 1.5 (Roche Diagnostic Systems, Inc., Branchburg, NJ) at least 3 months prior to screening and again at screening. For the initial HIV-1 RNA determination, a value less than 200 copies per milliliter measured by branched-chain DNA assay (bDNA; Chiron 3.0®, Chiron Diagnostics, Emeryville, CA) was acceptable for entry; however, all screening measurements were performed using the Amplicor HIV-1 Monitor test, version 1.5. Subjects were not permitted to have an HIV-1 RNA value 200 copies per milliliter or more between the initial and screening measurements.
All enrolled subjects were required to be on an unmodified ART regimen for at least 3 months prior to study baseline; ART was defined as a PI (with or without ritonavir) plus at least two nucleoside reverse transcriptase inhibitors (NRTIs), or an NNRTI plus at least two NRTIs. Subjects were also required to be on their first ART regimen or have documented evidence of viral suppression on a previous PI-based regimen at the time of prior change in therapy. All subjects had to be willing to continue with their current unmodified ART regimen for at least 48 weeks in the event that they were randomized to the SBR group. In addition, screened subjects were required to complete an enrollment survey that evaluated the reason for their willingness to switch to the EFV/FTC/TDF regimen.
Subjects were excluded if they had used any NNRTI-based therapy before their current ART regimen, were currently using an NNRTI-based regimen consisting of EFV plus TDF and FTC, or had used a NRTI-only therapy for more than 7 days prior to their current therapy; subjects in the prior PI-based ART stratum who were receiving TDF and FTC were allowed to participate in the study. Other exclusion criteria included known hypersensitivity or resistance to any of the components of EFV/FTC/TDF, diagnosis of a new AIDS-defining condition (with the exception of CD4 criteria) within 30 days of baseline, history of significant bone or renal disease, history of malignancy with receipt of chemotherapy within 90 days of baseline, and use of nephrotoxic medications or agents known to interact with EFV.
Patient-reported outcome measures
Patient-reported outcomes assessed during the course of the study are summarized in Table 1 and detailed below. Trial participants were required to provide completed assessment forms/questionnaires for all patient-reported outcome measures at baseline and all subsequent visits with the exception of the QOL measure that was only collected at baseline and at weeks 4, 12, 24, and 48. During each visit, forms/questionnaires were reviewed by the study personnel only for the purpose of assuring that all questions were answered.
PERC, perceived ease of the regimen for condition; POM, preference of medication; SF-36, Medical Outcomes Study 36-item Short Form survey; VAS, visual analogue scale.
Quality of Life
Health-related QOL was assessed using the Medical Outcomes Study 36-item Short Form survey (SF-36) questionnaire, version 2. 12 This is a validated, comprehensive, and widely used tool that measures QOL in the general population, as well as in subject groups with diverse chronic diseases. The questionnaire assesses eight health domains, including physical functioning, social functioning, general health, vitality, bodily pain, mental health, role capacity–physical, and role capacity–emotional. A physical component summary score is derived from combined scores for the physical functioning, role capacity–physical, bodily pain, and general health domains; a mental component summary score is derived from combined scores for the social functioning, role capacity–emotional, vitality, and mental health domains. As calculated, the scale scores are standardized to a mean of 50 points and a standard deviation (SD) of 10 points in the U.S. general population.
Treatment Adherence
Patient-reported adherence to treatment was assessed using the visual analogue scale (VAS). 13 For the adherence VAS measure, subjects were instructed to mark a linear scale at a point showing their best estimate of how much of their medication they had taken since their last visit. Previous reports have shown that the VAS minimizes response burden while demonstrating similar validity relative to standard and widely used 3-day self-reports. 13,14 During the study, adherence to treatment within the EFV/FTC/TDF group was also assessed via evaluation of pill counts.
Preference of Medication Survey
Treatment preference was evaluated using the preference of medication (POM) survey, a single-item measure utilized in neuroscience studies, 15,16 which was adapted for use in HIV-infected subjects, but is not validated in this population. For the POM survey, subjects were asked, “How does this current medicine compare to the previous ART medicine(s) your doctor prescribed for your HIV infection?” Response categories were set as (1) much better, I prefer this medication; (2) slightly better; (3) about the same; (4) slightly worse; (5) much worse, I much prefer my previous medication. Because of the stated comparison with the prior regimen, the POM questionnaire was administered only to subjects randomized to the EFV/FTC/TDF group.
Perceived Ease of the Regimen for Condition Questionnaire
Subjects' perception of the ease or difficulty of use of their current HIV medication was assessed using the perceived ease of the regimen for condition (PERC) questionnaire. The PERC questionnaire is not a validated instrument, but was developed specifically for this study. The single statement and related query comprising the questionnaire was as follows: “Medications vary with respect to number of pills, frequency and timing of taking medication, and other instructions. How easy did you find it to follow your current HIV medication regimen?” Possible responses were scored on a four-point, Likert-type scale where 1 = very easy; 2 = somewhat easy; 3 = somewhat difficult; and 4 = very difficult.
HIV Symptom Index
The HIV symptom index is a validated tool used to evaluate the presence and perceived distress linked to symptoms commonly associated with HIV or its treatment. 17 Symptoms assessed in this 20-item, self-reported measure include: fatigue or loss of energy; fevers, chills, or sweats; feeling dizzy or lightheaded; pain, numbness, or tingling in the hands or feet; trouble remembering; nausea or vomiting; diarrhea or loose bowel movements; feeling sad, down, or depressed; feeling nervous or anxious; difficulty falling or staying asleep; skin problems; cough or trouble catching your breath; headache; loss of appetite or a change in the taste of food; bloating, pain, or gas in your stomach; muscle aches or joint pain; problems with having sex; changes in the way your body looks; problems with weight loss or wasting; and hair loss or changes in the way your hair looks. For each symptom, a five-point scale is used to score responses, as follows: (1) no symptom; (2) has symptom, but does not bother; (3) has symptom and bothers a little; (4) has symptom and bothers; (5) has symptom and bothers a lot.
Statistical analysis
The set for analysis included all patients who were randomized into the study and received at least one dose of study medication. Outcome measures were summarized using descriptive statistics. The Wilcoxon signed rank test was used to assess changes from baseline within treatment groups for the SF-36 physical and mental component summary scores and the adherence VAS. Differences between treatment groups in SF-36 scores and on the adherence VAS were assessed using Wilcoxon rank sum test. POM questionnaire and PERC survey results were summarized by number and percentage of subjects for each response category. For the PERC survey analysis, responses were dichotomized to “very easy” (score of 1 point) and “not very easy” (score of 2, 3, or 4 points). HIV symptom index results were summarized for each symptom by number and percentage of subjects providing each response. Responses were dichotomized, for this analysis, to “no symptom” (score of 1 point) and “with symptom” (score of 2, 3, 4, or 5 points). For the PERC survey and HIV symptoms index, the McNemar test was used to assess whether responses at a particular time point were significantly different from responses at baseline; the χ2 test was used to compare responses between treatment groups.
Results
Patient disposition and demographics
In total, 300 subjects received at least one dose of study drug. Of these subjects, 203 were randomized to receive EFV/FTC/TDF and 97 remained on SBR. 10 At baseline, the treatment groups were similar with regard to subject demographics and characteristics (e.g., gender, age, race, ethnic origin, and HIV risk factor), CD4 cell counts (median counts were 517 cells/mm3 and 515 cells/mm3 for the EFV/FTC/TDF and SBR groups, respectively) 10 and scores on patient-reported outcome measures. In both treatment groups, more than 95% of subjects had HIV-1 RNA less than 50 copies per milliliter at baseline. 10 Rates of discontinuation were similar in the treatment groups with 89.2% of subjects in the EFV/FTC/TDF group and 87.6% of subjects in the SBR group completing the 48-week study. The most frequent reasons for discontinuation were adverse events (10 subjects [5%] receiving EFV/FTC/TDF, 1 subject [1%] receiving SBR) and withdrawal of consent (4 subjects [2%] receiving EFV/FTC/TDF, 7 subjects [7%] receiving SBR). 10 Of the 10 patients in the EFV/FTC/TDF group discontinuing because of adverse events, 3 patients experienced moderate (grade 2), and 2 patients experienced moderate to severe (grades 2 and 3), nervous system symptoms and/or psychiatric symptoms. The most frequently reported treatment-related adverse events were diarrhea (8% versus 8%), dizziness (12% versus 2%), headache (5% versus 7%), and depression (8% versus 4%) in the EFV/FTC/TDF versus SBR groups, respectively. 10
At the time of enrollment, 53% of subjects were receiving a PI-based regimen and 47% were receiving an NNRTI-based regimen (Table 2). In general, baseline demographics and disease characteristics were similar within each of the prior ART strata. However, baseline CD4 cell counts were lower in subjects who were receiving a PI-based regimen compared to subjects receiving an NNRTI-based regimen (median counts of 479 cells/mm3 and 550 cells/mm3, respectively). In addition, subjects on PI-based regimens had been diagnosed with HIV infection and were receiving antiretroviral treatment for a shorter period of time than subjects on an NNRTI-based regimen (median of 2 years versus 4 years on treatment, respectively).
EFV/FTC/TDF indicates subjects randomized to the single-tablet regimen (efavirenz/emtricitabine/tenofovir DF).
SBR indicates subjects randomized to continue their same baseline antiretroviral regimen.
All percentages are given as percent of total N for each column.
3TC, lamivudine; ABC, abacavir; ddl, didanosine; NNRTI, non-nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; ZDV, zidovudine.
Enrollment survey
In response to an enrollment survey conducted at study entry to assess reason(s) for a subject's willingness to switch to the EFV/FTC/TDF regimen (subjects could list more than one reason when responding to the survey), 94% of the overall population cited simplification of their current regimen as a reason; 3% cited intolerability of their current regimen; 18% cited concern about long-term side effects of their current regimen; 5% cited trouble taking current regimen regularly; and 17% cited other reasons, including “curious,” “cost,” “hope to find a cure,” “interested in research,” “lipoatrophy,” “asked by doctor to participate,” and “to help in the understanding of what this could do for others” (Table 3). Responses to the survey were similar regardless of whether the subject was previously taking a PI-based or NNRTI-based regimen.
Subjects could list more than one reason when responding to the survey.
Other reasons included: “curious,” “cost,” “hope to find a cure,” “interested in research,” “lipoatrophy,” “asked by doctor to participate,” and “to help in the understanding of what this could do for others.”
NNRTI, non-nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
Quality of life
At baseline, median scores for the SF-36 physical and mental component summaries were similar between treatment arms and did not vary by prior ART strata (Table 4). Throughout the study, changes from baseline in physical and mental component summary scores were numerically small and were not statistically significant in either arm for the overall study population or in the prior PI-based or NNRTI-based ART strata. Differences between the overall treatment groups for the change from baseline in physical component summary scores were statistically significant at week 48 (mean difference 2.0; p = 0.010, Table 4). At this final time point, changes from baseline in physical component summary scores showed a positive trend (i.e., improved QOL) for the overall EFV/FTC/TDF group, but changes from baseline for the overall SBR group showed a trend in the negative direction (i.e., worsened QOL). Patterns of change in physical component summary scores in the overall groups were primarily reflected in the prior PI-based ART stratum, with differences between the EFV/FTC/TDF and SBR groups reaching statistical significance at week 48 (mean difference 2.4; p = 0.020; Table 4). For the mental component summary, no significant between-group differences were observed.
EFV/FTC/TDF indicates subjects randomized to the single-tablet regimen (efavirenz/emtricitabine/tenofovir DF).
SBR indicates subjects randomized to continue their same baseline antiretroviral regimen.
Comparison with respective SBR group.
NNRTI, non-nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; SF-36, Medical Outcomes Study 36-item Short Form survey.
Treatment adherence
Adherence to treatment, as measured by the VAS, was 96% or more for the EFV/FTC/TDF and SBR groups at baseline and throughout the study. At all postbaseline visits, there were no statistically significant differences between the overall treatment groups in terms of mean adherence or change from baseline in adherence. When the EFV/FTC/TDF and SBR treatment groups were stratified by prior PI-based or NNRTI-based ART regimen, adherence rates remained at or above 96% throughout the study in all subgroups. No statistically significant differences in adherence rates were observed between subjects switched from a previous PI-based regimen to EFV/FTC/TDF and subjects who remained on their original PI-based regimen. Likewise, differences in adherence rates between subjects switched from a previous NNRTI-based regimen to EFV/FTC/TDF and subjects who remained on their original NNRTI-based regimen were small and not statistically significant.
POM survey
The percentage of subjects who preferred the EFV/FTC/TDF regimen to their previous ART (i.e., reported the EFV/FTC/TDF regimen as “much better, I prefer this medication”) increased from 64% at week 4 to 85% at week 48. Overall, 91% of subjects reported that the EFV/FTC/TDF regimen was either “much better” or “slightly better” than their prior regimen at week 48. As shown in Figure 1, preference for the EFV/FTC/TDF regimen was consistent among subjects who had received either prior PI-based or NNRTI-based ART. Over the course of the trial, ten subjects (5%) considered the EFV/FTC/TDF regimen to be much worse than their previous regimen on at least one occasion. Of these 10 subjects, 6 had received prior PI-based regimens and 4 had received prior NNRTI-based regimens (3 subjects had received EFV as part of their prior NNRTI-based regimen). Three of the 10 subjects completed the study, 2 withdrew consent, and 5 discontinued because of adverse events; the adverse events associated with discontinuation of these 5 subjects and considered related to study drug were: dizziness, insomnia, sleep disorder, mood disturbance, mood swings, anorexia, headache, nausea, and personality change. Of the 5 subjects discontinuing because of adverse events, 4 had received a prior PI-based regimen. By week 48, no subjects receiving EFV/FTC/TDF considered this treatment to be worse than their previous regimen (Fig. 1).
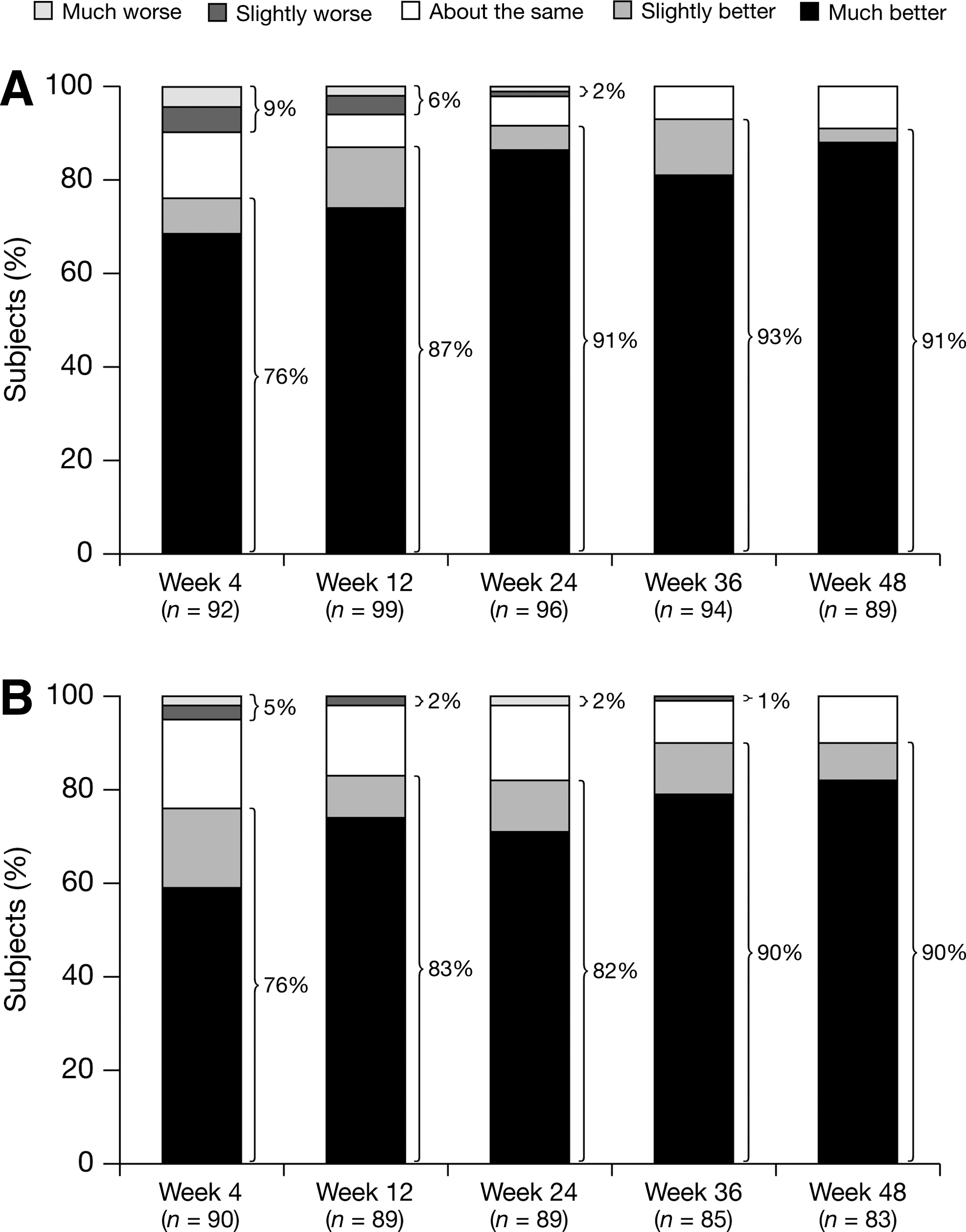
Categorical summary of preference of medication (POM) survey scores through 48 weeks of efavirenz/emtricitabine/tenofovir DF (EFV/FTC/TDF) treatment in subjects switched from prior protease-inhibitor–based (
PERC questionnaire
At the baseline visit, the percentage of subjects who reported that it was “very easy” to follow their current HIV medication regimen was lower in the EFV/FTC/TDF group (68%) than the SBR group (75%), though this difference was not statistically significant. From week 4 onward, the percentage of subjects who considered their regimen “very easy” to follow was significantly higher among those who were switched to EFV/FTC/TDF than those continuing on SBR (Fig. 2). By week 48, 97% of subjects in the EFV/FTC/TDF group reported that their current regimen was “very easy” to follow, compared with 81% of subjects in the SBR group (p < 0.0001). For all postbaseline visits, the percentage of subjects in the EFV/FTC/TDF group who considered their regimen “very easy” to follow was significantly higher than at baseline (p < 0.0001); the percentage of subjects in the SBR group who considered their regimen as “very easy” to follow did not change significantly from baseline. At all postbaseline visits, a significantly higher percentage of subjects who switched to EFV/FTC/TDF than subjects continuing on SBR reported that the regimen was “very easy” to follow, regardless of whether they had received prior PI-based or NNRTI-based ART (p ≤ 0.05). By week 48, 97% and 96% of subjects switched to EFV/FTC/TDF from prior PI-based and NNRTI-based regimens, respectively, considered that their current regimen was “very easy” to follow; these percentages were significantly higher than recorded for subjects continuing PI-based or NNRTI-based ART (83% and 79%, respectively; p ≤ 0.01).

Percentage of subjects rating their current regimen as “very easy” to follow in response to the perceived ease of the regimen for condition (PERC) questionnaire. a p < 0.001; b p < 0.0001 versus the stay on their baseline regimen (SBR) group.
HIV symptom index
Examination of results from the HIV symptom index revealed two main categories for significant changes from baseline among subjects switched to EFV/FTC/TDF: (1) transient worsening/emergence of certain symptoms and (2) sustained improvements in specific symptoms. The percentage of subjects in the overall EFV/FTC/TDF group who reported symptoms of dizziness or lightheadedness was significantly higher at week 4 compared to baseline (p = 0.0014; Fig. 3). This change from baseline was primarily driven by a significant worsening/emergence of these symptoms among subjects switched from a prior PI-based regimen. As a result, the percentage of subjects in the overall EFV/FTC/TDF group experiencing symptoms of dizziness or lightheadedness was significantly higher than in the overall SBR group at week 4 (p = 0.018). Significant differences from baseline in the percentage of subjects experiencing dizziness or lightheadedness symptoms were observed at week 4 only and were not observed during the remainder of the trial (Fig. 3). Overall, three subjects discontinued treatment during the study due to dizziness or lightheadedness symptoms, all of whom had switched from a prior PI-based regimen to EFV/FTC/TDF. All three subjects discontinued within the first 4 weeks of the study.

Proportion of subjects reporting dizziness or lightheadedness on the HIV symptom index. a p < 0.002; b p < 0.0014 for within treatment group comparison of postbaseline to baseline.
In the overall EFV/FTC/TDF group, a significantly lower percentage of subjects reported symptoms of diarrhea or loose bowel movements; bloating, pain, or gas in the stomach; changes in the way their body looked; and problems having sex, at week 48 versus baseline; changes from baseline in the percentage of subjects reporting these symptoms in the overall SBR group were not statistically significant at Week 48 (Table 5).
EFV/FTC/TDF indicates subjects randomized to the single-tablet regimen (efavirenz/emtricitabine/tenofovir DF).
SBR indicates subjects randomized to continue their same baseline antiretroviral regimen.
Within-group comparison of percentage at Week 48 with percentage at baseline using McNemar test.
NNRTI, non nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
Among subjects who had received a prior PI-based ART regimen and who were switched to EFV/FTC/TDF, significant improvements between baseline and week 48 were seen for two symptoms: diarrhea or loose bowel movements, and changes in the way their body looked. Subjects who had received a prior PI-based regimen and remained on that regimen (SBR group) showed a statistically significant improvement in bloating, pain, or gas in the stomach at week 48 (38% with symptom at baseline versus 23% with symptom at week 48; p = 0.032); although some improvement from baseline in this symptom was also reported by subjects switched from a PI-based regimen to EFV/FTC/TDF, the change at week 48 showed only a trend toward statistical significance (37% with symptom at baseline versus 25% with symptom at week 48; p = 0.059; Table 5).
Among subjects who had received a prior NNRTI-based regimen and who were switched to EFV/FTC/TDF, significant improvements between baseline and Week 48 were seen for bloating, pain, or gas in the stomach (p = 0.007; Table 5); no statistically significant changes between baseline and week 48, were reported for any symptoms among subjects who had received a prior NNRTI-based regimen and remained on that regimen (SBR group).
Discussion
This was the first trial to prospectively evaluate a switch to the fixed-dose, single-tablet regimen of EFV/FTC/TDF in HIV-1–infected subjects who were virologically suppressed on their previous PI-based or NNRTI-based regimens. Patient-reported outcomes indicated that, following the switch to EFV/FTC/TDF, QOL and treatment adherence, which were high at baseline, were well maintained, and treatment ease of use and patient satisfaction improved. As previously reported, subjects switched to EFV/FTC/TDF also maintained high rates of virologic suppression that were comparable with rates among subjects who continued their unmodified baseline antiretroviral regimen. 10
When assessing the patient-reported outcomes from this trial, it is important to consider that the trial enrolled subjects who were both stable and virologically suppressed on their baseline ART regimen and thereby implicitly excluded subjects with poor adherence or treatment-limiting adverse reactions. This inherent selection bias for a stable, suppressed population may have restricted the ability to observe significant improvements following the switch to a new regimen. Indeed, the inclusion criteria could have naturally led to the selection of patients with good baseline QOL and a high level of treatment adherence, which may explain the lack of improvement in these measures observed during the course of this 48-week study.
As antiretroviral options have increased and HIV-infected patients effectively treated with ART are living longer, the improvement or maintenance of health-related QOL has become an increasingly important goal of treatment for HIV medications. 1 In the current study, baseline QOL scores were similar to general population norms, likely reflecting the beneficial impact on QOL of the subjects' existing PI-based or NNRTI-based regimens. Throughout the 48-week study, changes in SF-36 physical and mental health summary scores were numerically small and scores observed at end of study were not significantly different from baseline, regardless of whether the subject was switched to EFV/FTC/TDF or continued their existing therapy. Overall, the outcomes suggested that simplification of an existing PI-based or NNRTI-based regimen to EFV/FTC/TDF was associated with maintained QOL. Significant between-group differences were observed in the change in physical component summary scores in favor of EFV/FTC/TDF for both the overall population and the prior PI-based ART stratum at week 48; however, at present, the clinical relevance of these numerically small changes in QOL summary scores is unclear.
Rates of treatment adherence measured throughout the trial using the VAS method were very high (≥96%), both among subjects who switched to EFV/FTC/TDF and those remaining on their existing ART regimen. These high rates of self-reported treatment adherence were consistent with adherence rates reported for the EFV/FTC/TDF group using the standard pill count method (adherence rate of ≥95% for 89% of subjects). 10 Evidence from the non-HIV literature suggests an inverse relationship between treatment adherence and frequency of dosing. 18 In addition, a number of studies conducted in HIV-infected subjects who were either treatment naive or stable on ART, have demonstrated an association between a reduction in dosing frequency and/or pill burden and improved adherence. 7,19 –21 Though improvement in adherence may have been anticipated in the current study, high adherence rates at baseline (≥96%) may have limited the ability to demonstrate an improvement in this parameter. A lack of significant improvement in adherence among stable, suppressed subjects who switch regimens has also been noted in a recent meta-analysis, which assessed the impact of once-daily regimens on treatment adherence. 22
Results from this trial indicated that switching to EFV/FTC/TDF was associated with improved ease of use and enhanced patient satisfaction. From the Week 4 visit onward, more than 90% of switched subjects who responded to the PERC questionnaire indicated that the single tablet regimen was easier to follow than their previous regimen. By week 48, 97% of subjects on prior PI-based regimens and 96% of subjects on prior NNRTI-based regimens considered the EFV/FTC/TDF regimen easier to follow than their prior therapy. Likewise, with the exception of five subjects who had difficulty tolerating EFV/FTC/TDF and discontinued due to adverse events, outcomes from the POM survey indicated that the majority of subjects switched to EFV/FTC/TDF preferred this regimen over their prior therapy. Indeed, by the end of the study, 91% of all subjects stated that EFV/FTC/TDF was “much better” or “slightly better” than their previous ART, with 85% indicating that they much preferred the simplified regimen. Notably, this preference for EFV/FTC/TDF was apparent, regardless of whether the subject had received a prior PI-based or NNRTI-based regimen.
At week 4 of the study, the HIV symptom index results indicated a significant worsening of symptoms of dizziness or lightheadedness among subjects switched to EFV/FTC/TDF, primarily among those switched from a prior PI-based regimen. Three subjects receiving EFV/FTC/TDF discontinued treatment due to symptoms of dizziness within the first 4 weeks of the trial, all of whom were switched from a PI-based regimen. Importantly, the worsening of dizziness or lightheadedness was transient and no dizziness-related discontinuations or significant differences in the percentage of subjects experiencing these symptoms were noted beyond week 4. This outcome was perhaps predictable considering that (1) current guidelines state that short-term central nervous system effects, including dizziness, may be seen in patients following initial administration of EFV, 1 (2) dizziness is a noted common side effect in the EFV product insert, 23 and that (3) similar transient central nervous system effects have been reported in prior studies assessing the switch from PI-based to EFV-based regimens. 6
In the present study, switch from a PI-based or NNRTI-based ART regimen to EFV/FTC/TDF was associated with sustained improvements from baseline in several symptoms commonly related to HIV infection or HIV medications. Gastrointestinal-related symptoms, including diarrhea or loose bowel movements and bloating, pain, or gas in the stomach were reported in a significantly lower percentage of subjects switched to EFV/FTC/TDF at week 48, compared to baseline. No significant changes from baseline in these symptoms were reported at week 48 among subjects in the overall SBR group. However, it is noteworthy that a significantly lower percentage of subjects continuing their prior PI-based regimen reported bloating, pain, or gas in the stomach at week 48, compared to baseline.
Since this was an open-label study, there may be a potential bias, for some measures, in relation to expectations for the new regimen to provide benefits over the previous medication(s). Moreover, the impact of this potential bias may be particularly apparent on subjective measures that are reliant upon patient judgments, including the patient-reported measures adopted in the current trial. In addition, switch studies have a tendency to appeal to subjects who are inspired to switch their existing therapy or components of that therapy, and consequently, randomization to the SBR group may have also biased responses against the existing therapy for certain patient-reported outcomes. Thus, the findings of the current study must be interpreted with respect to these, and other potential limitations. In addition, given the primary aim of assessing the safety and effectiveness of simplifying therapy to a single-tablet regimen of EFV/FTC/TDF from a wide array of antiretroviral regimens, a double-blinded design was not considered feasible.
In conclusion, switching virologically suppressed HIV-1–infected subjects from their existing PI-based or NNRTI-based regimen to EFV/FTC/TDF was associated with maintained QOL and treatment adherence, improved ease of use and treatment satisfaction, and sustained improvements in several commonly encountered HIV-related symptoms. Most importantly, as has been previously reported, these patient-reported benefits were observed in association with maintained virologic suppression. 10
Footnotes
Acknowledgments
This study was funded by Bristol-Myers Squibb and Gilead Sciences. Editorial support was provided by Jean Turner and Richard Daniel, of PAREXEL, and was funded by Bristol-Myers Squibb.
ClinicalTrials.gov Identifier: NCT00365612
Author Disclosure Statement
S. Hodder has received consultant fees from Bristol-Myers Squibb, Gilead, and Tibotec. She has also received research support from Bristol-Myers Squibb, Gilead, Pfizer, and Tibotec.
K. Mounzer has received speaker and consultant fees from Bristol-Myers Squibb and Gilead.
E. DeJesus has received consultant fees and lecture fees from Bristol-Myers Squibb, Gilead, GlaxoSmithKline, Merck, Tibotec, and Vertex. He has also received research support from Abbott, Achillion, Avexa, Boehringer-Ingelheim, Bristol-Myers Squibb, Gilead, GlaxoSmithKline, Merck, Pfizer, Roche, Schering Plough, Taimed, Tobira, Tibotec, Vertex, and Virco.
A. Farajallah and K. Grimm are employees of and stockholders of Bristol-Myers Squibb. S. Esker is an employee of Bristol-Myers Squibb.
J. Flaherty, R. Ebrahimi, and J. Ecker are employees of and stockholders of Gilead Sciences.