
Abstract
This cross-sectional survey examines the utilization of HIV care and treatment services after HIV diagnosis among women in Vietnam and describes factors that may be associated with failure in seeking services. From May 2007 to November 2007, we conducted structured interviews with 353 HIV-positive women living a Haiphong, a northern province of Vietnam. The women were recruited through a network of people living with HIV/AIDS (HPN+) by means of snowball sampling and through the local, governmental HIV registration system (Provincial AIDS Centre [PAC]). Approximately 26.3% of the study participants had never attended HIV care and treatment services. Failure in seeking the services was associated with not being registered in the PAC (odds ratio [OR]: 3.0; 95% confidence interval [CI]: 1.4–6.4), not having a known HIV-positive family member (OR: 3.2; 95% CI: 1.2–8.3), not having disclosed HIV status (OR: 4.0; 95% CI: 2.0–8.1), and factors associated with the testing situation, whereby women who were tested by chance had a 4.0 times increased OR (95% CI: 1.4–11.7) and women who were tested in relation to antenatal care or delivery had 3.0 times increased OR (95% CI: 1.1–8.5) for failure to seek HIV care compared to women who had been tested because their husbands/partners were sick or had died. We suggest that the posttest counseling and referral system for HIV care and treatment need to be improved. An alternative system for picking up those not wishing to attend the official system might help to approach these needy women.
Introduction
I
In Vietnam, out-of-pocket expenditure for general medical care is a problem; most PLWHA are unable to afford HIV-related medical care and antiretroviral (ARV) drugs. 11,12 However, since 2005, with the influx of funding from international donor agencies and strong commitment by the government on HIV prevention and control program investment and implementation, 13 HIV care and treatment have been freely available in the hardest hit areas, accompanied by intensive information, education and communication on HIV prevention and care. A referral system among HIV testing, care, and treatment services, e.g., between HIV voluntary counseling and testing (VCT) and outpatient clinics for HIV care and treatment, between prevention mother to child transmission (PMTCT) and follow-up HIV care and treatment, has been established to ensure the continuum of HIV care. By the end of 2006, 228 VCT sites had been established and operated at provincial and district levels, and of 506 facilities nationwide providing antenatal care at provincial and district levels, 107 facilities provided the minimum package of PMTCT. 14 The number of people undergoing HIV testing has as a consequence increased. Although men will continue to account for the majority of PLWHA and new HIV infections, the estimated ratio of male to female has gradually decreased, from 3.0 in 2007 to 2.5 in 2012. 15 The husband-to-wife transmission is growing in importance in the country. 16,17
The purpose of this paper is to explore whether HIV-positive women living in a high HIV prevalence area take full advantage of the implemented HIV care and treatment programs and where they do not, to describe the factors that may be associated with the failure of initiating HIV care and treatment.
Materials and Methods
Study setting
Haiphong Province is located in northeastern Vietnam. It comprises 14 districts, has a population of approximately 1.8 million, and is one of the five provinces in Vietnam that is hardest hit by the HIV epidemic. In 2006, the prevalence of HIV infection was 0.5%. 18
At the end of 2005, the Provincial AIDS Centre (PAC) was established to monitor the HIV/AIDS situation in Haiphong in accordance with the decision by the Ministry of Health. Information regarding HIV-positive people who have been tested at clinics and laboratories are reported to PAC. By the end of February 2007, the number of HIV infections reported by PAC was 8142, of which 743 were women. However, this reported number does not cover those who obtain HIV tests at VCT points and wish to keep their status confidential, even when they have to provide personal identity information at outpatient clinics later for HIV treatment, their information is not sent to the PAC.
In the early 2000s, PLWHA groups have been established in Haiphong with support from mass organizations and local authorities to do out-reach activities including approaching people living in their community who are considered at high risk of HIV infection such as injection drug users IDUs and their partners. These PLWHA groups provide information on HIV and support to reach HIV testing services. Since 2004–2005, as the number of PLWHA has been increasing, self-help groups of PLWHA have been established in all districts. While doing outreach activities, they also created relationship with clinics providing HIV care and treatment services to connect PLWHA in their community to the services.
In Haiphong, ARV treatment for adults is freely available at nine outpatient clinics (OPCs) funded by the Global Fund for AIDS, Tuberculosis and Malaria, the President's Emergency Plan for AIDS Relief and the AIDS Health Foundation, United States. The OPCs are operated within state-owned health care facilities according to the guidelines of the Ministry of Health (MOH) and are mostly located in the eight urban districts and towns. The most remote rural district is approximately 40 km from the closet OPCs.
The average distance between women's living place and the OPCs where they were they receive HIV care and treatment services is 12 km. To access ARV, people have to obtain an HIV test and register at a designed OPC for HIV treatment by themselves or they may be referred from VCT, PMTCT and regular clinics. Whenever HIV positive people attend an OPC and wish to register for further HIV care and treatment, they are given an outpatient code. With the code, they can come to the OPCs at anytime for any kind of health problems or have physical and paraclinical examinations including CD4 count every 6 months to see whether there is a need for antiretroviral (ARV) treatment. 19 Patients receive free treatment for opportunistic infection but have to pay for some tests such as CD4 count, liver function analyses, and chest x-rays, these costs may add up $30, depending on available donor-funds. Once PLWHA enter the ARV program, regardless of which OPCs they registered at, they are granted free health care services including ARV drugs at the OPCs monthly, CD4 count every 3 months as well as other tests and treatment if necessary.
Study population
A community-based survey among HIV positive women aged 15–49 was conducted from May to November 2007. A household survey in Haiphong estimated that approximately 0.2% of the female population in the province was HIV positive and 550,000 women aged 15–49 were living in the province (GSO, 2005). Therefore, 1100 women were considered eligible for the study. To make the study as representative as possible, the research team approached participants in all 14 districts of Haiphong through available and possible sources: (1) PLWHA groups that have been established in 13 of 14 districts to form the network of PLWHA (HPN+) and (2) the HIV registration system that is administered by the PAC.
In each district, all HIV-positive female members of the HPN+ network were invited to participate in the study. Then, through the snowball technique, the research team approached other HIV-positive women in the community. When all known eligible women in the district had been approached through HPN+, the research team contacted the PAC workers who worked at the grassroots level to identify women who might not be covered by the HPN+ channel. The PAC workers played a liaison role to invite women to volunteer to participate in the study.
A total of 315 women were identified through the HPN+ network of whom 305 agreed to participate in the study (Fig. 1). The PAC register included information on 743 women; 82 of these women were living outside Haiphong and 378 had provided incomplete or false addresses. Of the 283 eligible women from the PAC register, 9 refused to participate and 226 had already been recruited via the snowball technique. Thus in all 353 HIV-positive women were recruited; 274 women who were registered in the PAC system and 79 who were not.
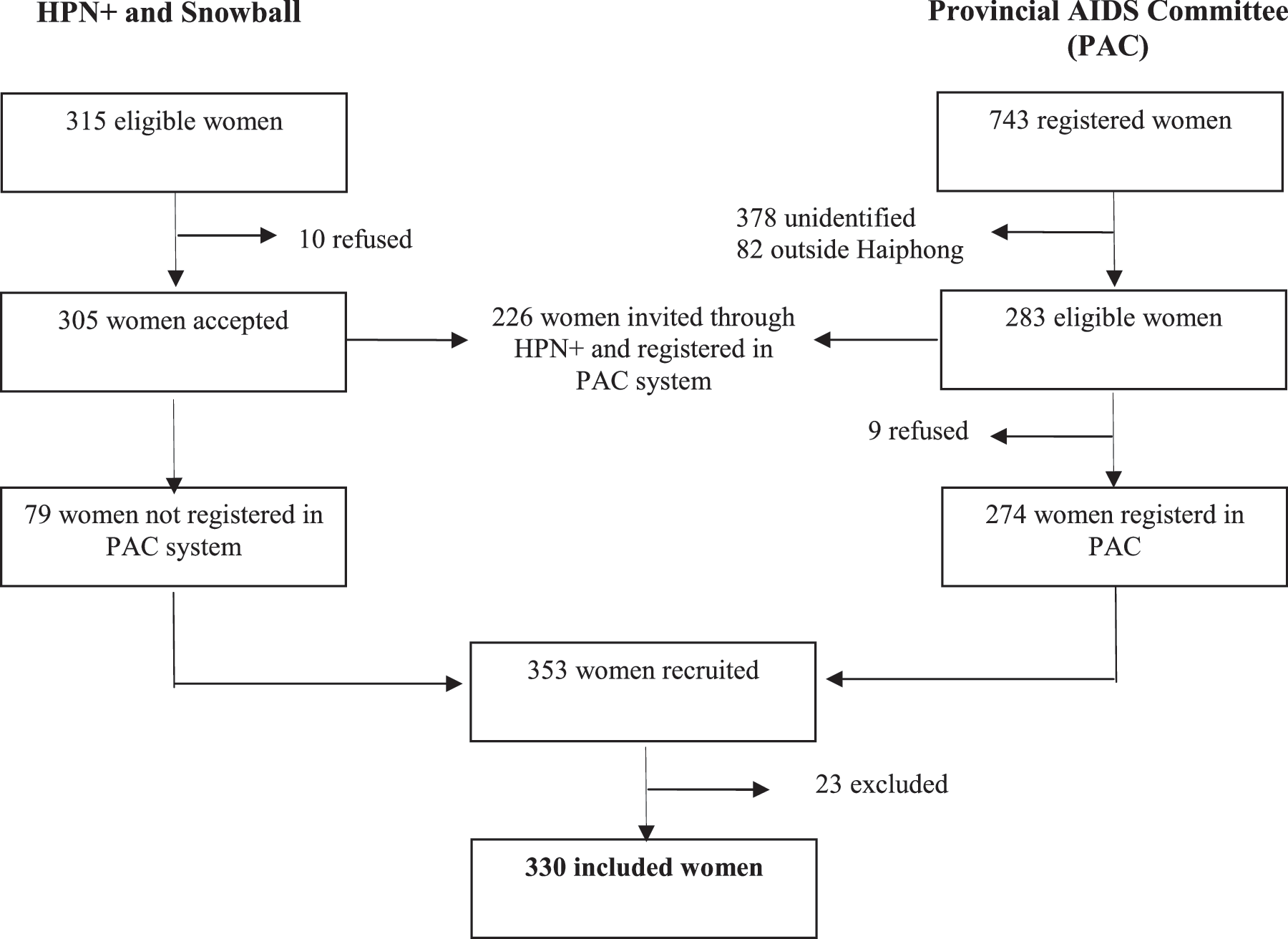
Procedure of recruiting participants in 14 districts of Haphong.
Data collection and analysis
HIV positive women were invited to participate in a structured questionnaire interview and to have their CD4 count measured. Twenty-three women, who were diagnosed with HIV < 3 months prior to the study, were excluded from the analysis to allow people sufficient time to enter care. 7,20
The dependent outcome—failure in seeking HIV care and treatment—was defined by the women's response of “no” to the question “Have you ever sought HIV treatment after being tested HIV positive?”. Additional information was sought to clarify whether the women were connected to HIV treatment services such as what clinics they came and what tests they received. If the women stated they had never attended HIV care and treatment or if they stated they had attended care outside the notified care and treatment system; either in small clinics without the required license to provide service or by self-treatment at drug stores, they were considered as not having attended HIV care and treatment.
Crude odd ratios (OR) with 95% confidence intervals (CI) were calculated to assess the associations between failure in seeking HIV care and demographic characteristics, interpersonal relations, HIV testing situation and disease situation. Statistically significant variables at p < 0.05 level in the bivariate analyses were included in a multivariate logistic regression model to measure the associations while controlling for potential confounding.
To assess disease situation of women who had not sought HIV care and treatment, 18 self-administered indicators of symptoms proven to be associated with physical and mental health among HIV-positive people regardless of their ARV treatment 21,22 were used. The symptom scale ranges from 1 to 5 where 1 represents absence of symptoms related to HIV and levels 2 to 5 represent increasing severity of the symptoms. The list of symptoms were translated into Vietnamese. The research team consulted a group of 10 HIV-positive women and two physicians who evaluated the contents and wording of the given symptom list. Individual interviews with another twenty women were conducted afterward to pilot the scoring system. Factor analysis was applied to the total sample of 353 women. The symptom of problems with having sex was taken out because most of widowed women who accounted for 30% of total sample stated having no sex in the past 4 weeks. Exploratory factor analysis with principal component extraction method was conducted. Three factors with eigenvalues over 1 emerged. However, only first factor that excluded symptom of fat deposits (eigenvalue = 4.76) had items satisfied the minimum factor loading criteria of 0.6 on one factor and no more than 0.3 on any other factor. Scale reliability analysis using the α with item removed function for all items indicated α = 0.83 for the first factor items and did not suggest any of the items be removed. Thus, 18 symptoms were used for convergence validity. Scores of the 18 symptoms were compared with levels of CD4 count. The result indicated that the total of the symptom scores was significantly higher among women with CD4 counts < 200 copies/mm3 compared to those with CD4 above 200 copies/mm3 (39.9 versus 36.8; p = 0.048).
In addition, the main reasons for not seeking HIV care and treatment were also descriptively presented by frequency tabulation. All statistical analyses were conducted using R 2.8.1 (R Foundation, GNU Project).
Ethical consideration
The study was cleared by National Committee for Population, Family and Children of Vietnam and The Danish National Committee on Biomedical Research Ethics. Informed written consent was obtained. Information on HIV care and treatment in Haiphong was provided to participants after questionnaire interview.
Results
Failure in seeking HIV care and treatment among HIV-positive women
Eighty-seven of the 330 eligible women (26.3%) had not sought HIV care and treatment. The median of the interval between the HIV test and the study inclusion among these 87 women was 113 weeks (Shapiro test W = 0.83, p < 0.001). The percentage of women not seeking care from 2005 and onwards when ARVs had, in fact, been freely available was 32.7% (73/243), while the figure prior to 2005 was 16.1% (14/87) (χ2 test, p = 0.007). Women who were tested for HIV after 2005 were significantly less likely to disclose their HIV status to family members and were less likely have a known HIV-positive member in their families compared to women who had HIV test prior to 2005.
Among the 87 women who had not sought HIV care and treatment, 58 (66.7%) consented to having their CD4 count measured. Of these 58 women, 17 (29%) had CD4 < 200/mm3 and were therefore, according to the national guidelines, in need of ARV treatment, 19 whereas the remaining 41 (71%) had CD4 counts above 200/mm3 and therefore not in need of ARV.
Factors associated with failure in seeking HIV care and treatment
The women's awareness of HIV when tested was significantly associated with failure in seeking care and treatment (Table 1). Hence, women tested for HIV by chance, including those having regular medical check-ups at their workplace and/or for job applications, had a 4.0 times increased OR (95% CI: 1.4–11.7) for failure compared to the group of women who were tested for HIV because they themselves were sick or their husbands/partners were sick or had died. A similar association was found among women who were tested in relation to antenatal care or delivery; they had an increased OR of 3.0 (95% CI: 1.1–8.5) for failure in seeking HIV care and treatment. In addition, women who did not have a known HIV-positive family member had a 3.2 times increased OR (95% CI: 1.2–8.3) for failure in seeking HIV care and treatment. Likewise, the OR for failure was 4.0 times (95% CI: 2.0–8.1) higher among women who had not disclosed their HIV status to family members compared to those who had. The multivariate analysis also indicates that not being registered in the provincial management/monitoring system (PAC) increased the odds (OR 3.0; 95% CI: 1.4–6.4) of not having accessed HIV care and treatment.
Four women who refused to answer the question on drug use were excluded from the analysis.
OR, odds ratio; CI, confidence interval; PLWHA, people living with HIV/AIDS; PAC, provincial AIDS Centre.
Reasons for not seeking HIV care and treatment are presented in Fig. 2. The majority of the women (61%) considered that they were in good health and therefore felt no need for HIV care and treatment. The mean of the 18 symptom scores was 1.9, meaning symptoms occurred but did not bother the women. Of the 18 symptoms, the three symptoms that mostly bothered the women were fatigue (81.4%, mean score: 2.5), headache (76.7%, mean score: 2.7), and feeling dizzy (76.7%, mean score: 2.6; Table 2).
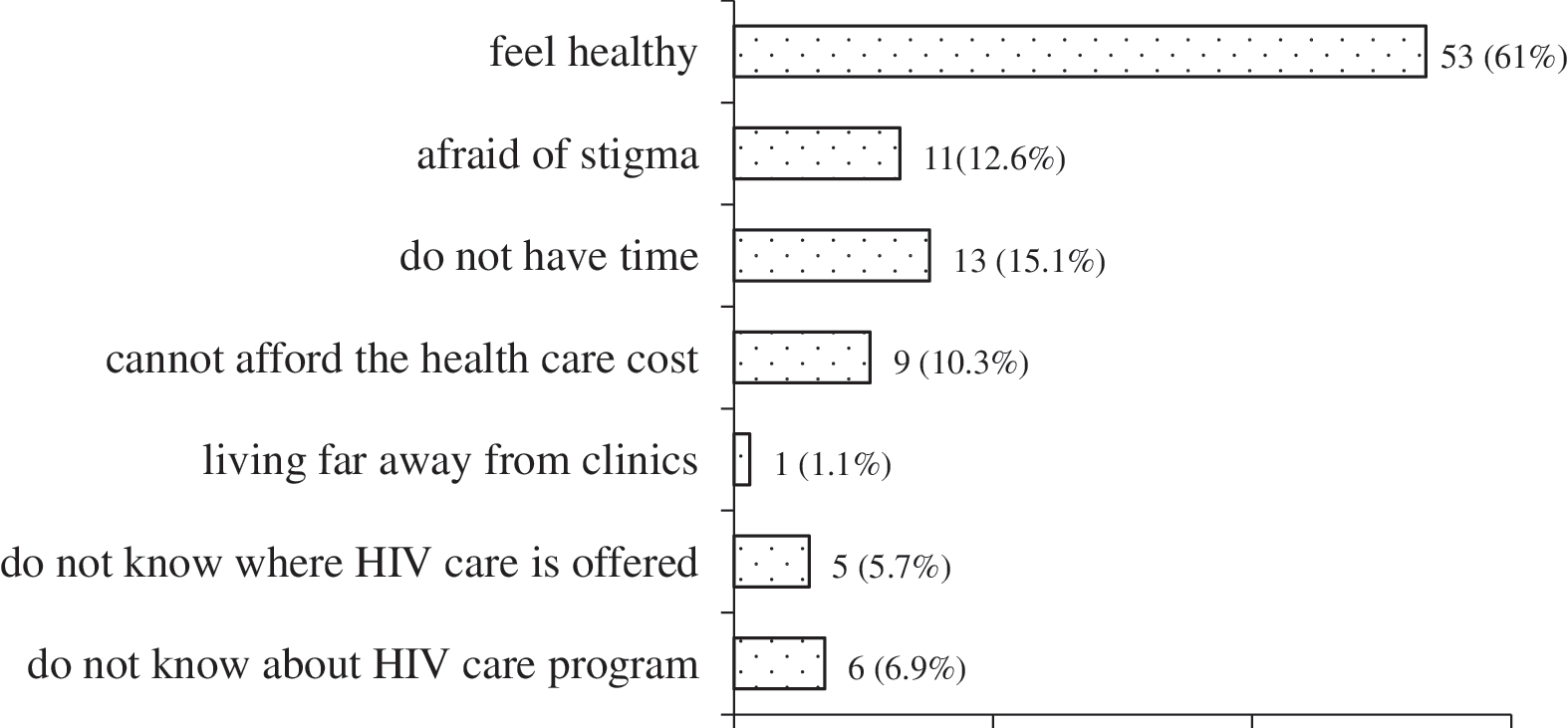
Reasons for not attending HIV care and treatment.
One woman could not complete this enquiry.
Among 87 women who failed to seek HIV care and treatment, 68% were unable to name the place where they would find HIV care and treatment services, and 7% did not know about the service availability.
Discussion
More than one fourth of HIV-positive women self-reported having never attended HIV care and treatment. Lack of registration, lack of disclosure, and lack of awareness were associated with failure in seeking HIV care and treatment.
Failure in seeking care and treatment was prevalent, a finding that should be seen within the context of the Vietnamese HIV testing guidelines where the importance of posttest counseling and reattendance for ongoing care is strongly emphasized. The fact that many women never sought HIV care suggests that the posttest counseling offered is not optimal. Meanwhile researchers have shown that posttest counseling and the interaction between health care providers and women is considered one of the driving forces behind uptake of HIV care and treatment among PLWHA. 1,23 Interventions aiming at improving the quality of posttest counseling should be considered. Additionally, the availability of ARVs may have influenced the women's uptake HIV care and treatment. In Haiphong, ARV is mainly available through the public health system. Women might fear being stigmatized, if attending public health care, because they are afraid that their HIV status may be disclosed by the health staff. 24 Similarly, in Thailand PLWHA tend to bypass local public health centers to avoid disclosure of their HIV status. 25 The problem of poor attendance may be addressed by a more diverse HIV/AIDS care and treatment system, where various stakeholders and organizations are involved and where the service is attuned to the priorities and concerns of PLWHA.
At the grassroots level, PAC staff are in charge of verifying personal information of HIV-positive cases reported and registered to PAC system. Once the HIV-positive persons are identified, PAC staff approach and provide them with information and counseling on HIV. The present study showed that lack of registration was associated with an increased ORs for not seeking HIV care and treatment. Another study shows women fear stigmatization if their status is known to PAC staff who are also health care providers in their living areas. 26 Hence, to reach HIV-positive women with HIV care and treatment, it is essential that confidentiality is strictly adhered to.
Disclosure of HIV infection and having an HIV positive family member were linked with an inclination to seek HIV care and treatment. This result suggests that in a northern Vietnamese context, HIV-positive women are less likely to be at severe risk of being stigmatized and abandoned by their family because they often have been infected by their spouse, who has been an injecting drug user. 27,28 Other studies have similarly documented that disclosure of HIV status may enhance access to care and social support. 29,30 Although the women in our study perhaps were not at high risk of being stigmatized by their families, the potential negative consequences of disclosure should be considered when advocating for disclosure. Because despite the family provides an essential source of financial support to HIV positive members and protects them from outside stigma and discrimination, the family's members at the same time expose their HIV positive members to these attitude and behavior. 31 In many settings, particularly women are considered at risk for abandonment and discrimination if they disclose being HIV positive. 23,32
Awareness of AIDS risk had an impact on the women's treatment seeking behavior. Hence, women who were tested by chance or during pregnancy or delivery were less likely to seek HIV care than those who were tested when they themselves were sick or their husband/partner were sick or had died of AIDS. The finding most likely reflects that women who had an AIDS affected partner were aware of their own AIDS risk and the availability of the HIV care and treatment program and acted accordingly, whereas women who were tested by chance or during pregnancy did not have the same awareness and were therefore less likely to attend care. Similarly, in the United State it has been found that the PLWHA's lack of awareness of their AIDS risk at the testing time is associated with an 18-month delay in seeking health care. 20 The finding implies more attention to the relation of seeking HIV care and treatment after the test and the testing programs. A study in six provinces of Vietnam in 2006 indicated that the current PMTCT was heavily child focused. 33 Therefore, posttest counseling, especially for women attending antenatal care, and child delivery services needs to include health care for the mothers. In addition, the referral system between PMTCT and follow-up HIV care and treatment also needs to be interconnected.
Feeling healthy was stated to be the main reason for not seeking HIV care and treatment. The result is in accordance with the CD4 count measurement, where 71% of the women, who had not attended care, had a CD4 count above 200/mm3 and therefore not in need of ARV. Apparently symptom is very important to HIV positive women's decision on seeking care and treatment. However, that 7% of women did not know the HIV treatment program availability and 68% were unable to name the places if they need the treatment indicated that they might be at risk of late HIV treatment, especially who lack family support due to their HIV status closure. This suggests that information on existing HIV care and treatment programs should be delivered in posttest counseling and diversified to reach PLWHA. In addition, symptom index needs to be further validated in Vietnam and it would be applied for clinical management on PLWHA's illness course.
The issue of selection bias has to be considered in the present study. First, HIV-positive women comprise an underground and hard-to-reach group of women, therefore, it is difficult to guarantee the representation of the study population. The research team therefore had to link up with available sources such as the PAC channels and the HPN+ channel and apply the snowball technique to approach the study population. However, the PAC register does not include the total population of HIV-positive women.
Furthermore, among the women listed in the PAC, more than half could not be reached because they were living in another places or correct contact information was missing. It has been documented elsewhere that young women are possibly underrepresented in our study population (unpublished data) because young women under 25 years old accounted for 20% of the study population whereas the same applied for 33% of the PAC-registered women. Therefore, the age factor might be underestimated. In addition, the study sample accounted for approximately one third of the target population, yet most participants were connected to either PAC or PLWHA group. We were unable to approach women who had tested for HIV from VCT service and wanted to keep their status confidential. However, one of this study's strengths is that it relied on a community-based approached and recruited women from different channels to attain as representative a study population as possible. Second, seeking HIV care and treatment in the private sector is not reflected in the present study. Currently there are no private clinics licensed to provide HIV treatment service. However, HIV-positive women who had no connection to either PAC or PLWHA groups and were unable to be approached by the research team might access HIV treatment at private clinics to keep their information completely confidential.
In conclusion, more than one fourth of HIV- positive women are not accessing the established health system for HIV care and treatment. Posttest counseling and referral for HIV care and treatment need to be improved. In addition, an alternative system for picking up those not wishing to attend the official system might help to approach these needy women.
Footnotes
Author Disclosure Statement
No competing financial interests exist.