
Abstract
Hepatitis C (HCV) infection is common among injecting drug users (IDUs), yet accessing of HCV care, particularly HCV treatment, is suboptimal. There has been little in-depth study of IDUs experiences of what enables or prevents them engaging at every level of HCV care, including testing, follow-up, management and treatment processes. This qualitative study aimed to explore these issues with current and former IDUs in the greater Dublin area, Ireland. From September 2007 to September 2008 in-depth interviews were conducted with 36 service-users across a range of primary and secondary care services, including: two addiction clinics, a general practice, a community drop-in center, two hepatology clinics, and an infectious diseases clinic. Interviews were analyzed using a grounded theory approach. Barriers to HCV care included perceptions of HCV infection as relatively benign, fear of investigations and treatment, and feeling well. Perceptions were shaped by the discourse about HCV and “horror stories” about the liver biopsy and treatment within their peer networks. Difficulties accessing HCV care included limited knowledge of testing sites, not being referred for specialist investigations and ineligibility for treatment. Employment, education, and addiction were priorities that competed with HCV care. Relationships with health care providers influenced engagement with care: Trust in providers, concern for the service-user, and continuity of care fostered engagement. Education on HCV infection, investigations, and treatment altered perceptions. Becoming symptomatic, responsibilities for children, and wanting to move on from drug use motivated HCV treatment. In conclusion, IDUs face multiple barriers to HCV care. A range of facilitators were identified that could inform future interventions.
Introduction
H
HCV infection causes liver inflammation that may damage the liver over time, potentially progressing to cirrhosis and hepatocellular carcinoma. Factors that accelerate this progression include HIV co-infection and heavy alcohol intake, both of which are common among IDUs. 6 Therefore, HCV screening among IDUs is vital, as is monitoring of liver health among those chronically infected, and timely treatment to prevent future complications. The current treatment for HCV is combination therapy with pegylated interferon and ribavirin, which achieves sustained viral clearance in 55–85% of patients, depending on HCV genotype. 7
Accessing of HCV care, particularly HCV treatment, is poor among IDUs. A survey of IDUs recruited from community settings in three U.S. cities found 27.3% had seen a health care provider since receiving a positive HCV diagnosis and just 4.8% had initiated treatment. 8 A survey of IDUs attending primary care and a methadone clinic in Sydney found most were having their HCV monitored—the majority by their local medical officer—but almost one-quarter had unsuccessfully attempted to obtain HCV treatment and one-third had been offered treatment and declined. 9 A similarly poor accessing of care has been reported in Ireland. A cross-sectional study found just 30% of IDUs attending general practice for methadone maintenance had been referred to a hepatology clinic and 3% had initiated HCV treatment. 10 Substantial defection from HCV management pre-treatment at an Irish tertiary care center has also been reported among IDUs. 11
Several barriers to HCV treatment have been reported, including active substance abuse, psychiatric and medical comorbidity, poor adherence with the treatment evaluation process, patient refusal of treatment, and loss of patients to follow-up. 6,12 Additional obstacles amongst those co-infected with HIV and HCV include the need to initiate antiretroviral treatment and advanced HIV disease. 13 These data are based on health providers' reports rather than patients, so do not reveal why patients default from follow-up and refuse treatment.
Qualitative literature on IDUs experience of barriers to and facilitators of HCV care is sparse. Several surveys of IDUs attitudes to HCV treatment reported 53–82% were willing to consider treatment. 8,9,14,15 Willingness was ascertained through responses on a Likert scale to scenarios outlining risks and benefits of treatment, which may not match the meaning and significance of treatment to IDUs, nor reflect actual decision-making in practice. 15 Two surveys investigated IDUs' experiences and motivations to an extent by asking why treatment had not been sought, accepted, or initiated. Motivations for seeking and accepting treatment were not asked. Reasons cited by IDUs in Sydney for being unsuccessful in obtaining treatment included their liver disease was not advanced enough, long waiting lists for treatment, concerns of the medical officer regarding treatment adherence, being a current IDU, and heavy alcohol intake. 9 Reasons for declining treatment offers included concern about treatment side-effects, reluctance to have a liver biopsy, not feeling sick enough, and having other health priorities. 9 Similar reasons were given by IDUs surveyed in Canada for not seeking treatment—additional reasons included lack of information about HCV and treatment, concern about lethargy on treatment, and lack of interest. 14
A more in-depth qualitative study was conducted among IDU women at a detoxification facility in Rhode Island. 16 Barriers and facilitators regarding hepatitis and HIV testing and treatment and hepatitis B vaccination were explored. Prioritization of obtaining drugs, low levels of disease-specific knowledge, stigma associated with injecting, access difficulties, and psychological factors were identified as barriers to care. One facilitator was identified—interest in promoting one's health. There is a dearth of research, however, with IDUs of both genders, in a range of settings and at different stages of HCV care, regarding what enables or prevents them engaging at every level of HCV care, including testing, follow-up, management and treatment. The present study is designed to address this gap in knowledge.
Methods
Settings
Current and former IDUs were recruited from settings in the greater Dublin area, Ireland during September 2007 to September 2008. The settings were chosen to reflect the range of settings that IDUs attend for addiction or HCV-related issues, and included: two addiction clinics, a community drop-in center, a general practice, two hepatology clinics, and an infectious diseases clinic (Table 1).
GMS, General Medical Services.
Sample
A maximum variation sampling approach 17 was used to recruit 36 IDUs who varied in their experience of and engagement with HCV care. Recruitment of participants was thus stratified according to the stages of HCV care: from initial screening, to attendance at specialist hospital services for further assessment, to initiating and completing treatment (Fig. 1). Service-users at each setting were eligible to participate if they were over 18 years of age and currently or previously injected drugs. Given the sensitivity of the study topic, those with ongoing psychiatric difficulties known to staff in that setting were not invited to participate.
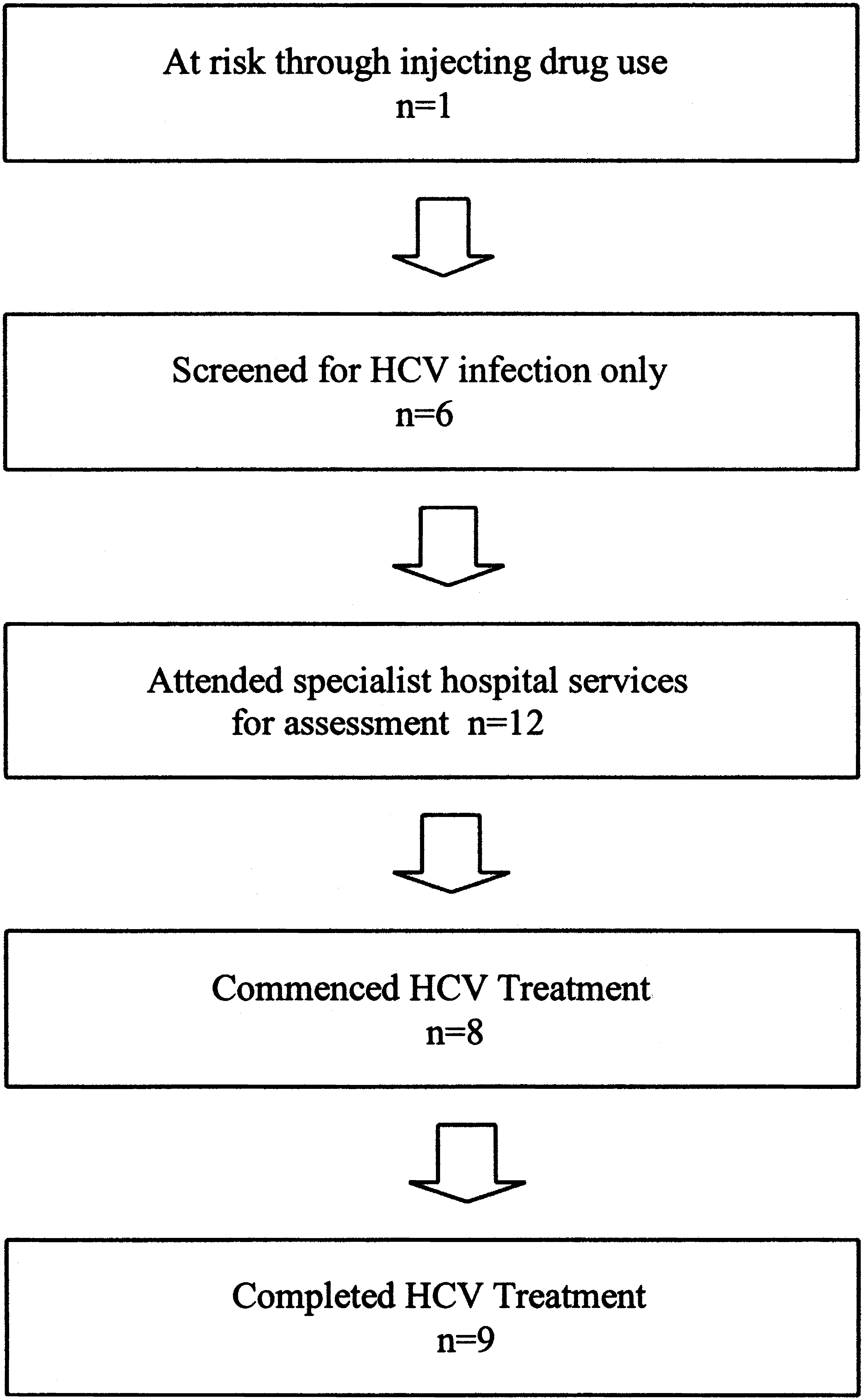
Sampling framework and number of participants (n = 36).
Data collection
An invitation to participate in a research interview about their experience of HCV and barriers to screening and treatment was extended to eligible service-users by staff at each setting. Service-users were provided with an information sheet and a verbal description of the study and those who were interested in participating were invited to meet the researcher (D.S.). At this meeting, the researcher (D.S) again discussed the study along with any residual points requiring clarification and explained how the information would be collected, transcribed, and reported. When satisfied in relation to these issues, potential participants indicated their consent to participate in the study by signing a consent form. No financial incentives were offered for participating. The study was approved by UCD Human Research Ethics Committee and the research ethics committees of the three hospitals involved in the study.
Semi-structured in-depth interviews 18 were conducted with individual participants in a private room at each setting. Interviews lasted approximately 45 min and were audio-taped with participants' permission and field notes taken afterward. The interview topic guide included questions on the participant's history and experience of HCV care, from initial screening through further diagnostic investigations and therapeutic interventions. Using probes and follow-up questions, attention was focused on the factors that the interviewee saw as encouraging or discouraging their accessing of HCV care. Participants were also asked for their suggestions for facilitating access to HCV care in light of the barriers identified. The semi-structured nature of the interviews allowed associated topics to be explored as they emerged. Also, as data collection, transcription, and analysis were proceeding in parallel, emergent issues identified in the analysis were investigated further in subsequent interviews. For example, early interviewees introduced their experience of health care providers and its relation to their accessing HCV care and this was explored further in subsequent interviews.
Data analysis
Interviews were transcribed and analyzed using a grounded theory approach. 19 Initially, transcripts were coded line-by-line using the method of constant comparison. As coding proceeded with detailed memo-taking reflecting on the relationship between codes, coding became more focused and higher order. D.S. coded all of the transcripts, with a selection of transcripts independently coded by W.C. and J.L. Differences in coding were discussed and resolved through revisiting relevant extracts. The developing analysis was discussed at team meetings and codes were revised and renamed appropriately as the analytic process continued. Qualitative software (NVivo 8.0) 20 assisted with the management and coding of interviews.
The developing analysis revealed the factors influencing the uptake of one intervention (e.g., screening) were similar to the factors influencing the uptake of another (e.g., HCV treatment). Thus, the barriers and enablers presented here apply to HCV care in the broader sense. The analysis also revealed that factors operated simultaneously, sometimes in opposite directions of influence, to create at times contradictory and ambivalent experiences. We have tried to portray the nuances of our participants' lived experience. The barriers and facilitators identified are organised under six overarching themes.
Several methods were utilized to enhance the validity of our findings: (1) triangulation of data across multiple settings; (2) an iterative process of data collection and analysis; (3) triangulation of coding across several co-researcher perspectives; and (4) continuation of data collection until no new themes were emerging. 21
Results
Demographics
Of the 36 participants interviewed, 28 were men and 8 were women. They ranged in age from 24 to 54 years, with a median age of 32 years. The median reported age of beginning to inject drugs was 18.5 years (range, 14–29). Of those who reported their main problem drug (n = 28), 79% indicated it was heroin and 21% cocaine. Thirty-three (91%) participants reported testing anti-hepatitis C antibody positive and 4 (11%) participants reported HIV/HCV co-infection.
Perceptions of HCV: Every injector has this invisible infection and its effects are not as serious as those of HIV
Prior to diagnosis and subsequently, participants' perceptions of HCV were shaped by a discourse amongst their peers which minimised and normalised HCV by comparison to HIV. Within this discourse, HIV is presented as a certain death sentence (“Ya have the virus … you're dead man”), while HCV is viewed as non-fatal (“I'm not gonna die of hepatitis C”) and by some, ‘curable.’ HIV is considered rare, while HCV is seen as common (“everybody has it”) and almost commonplace (“it's just like having a tattoo”). This discourse presents HCV infection as relatively benign, undermining perceptions of the seriousness of the infection and any perceived need for medical attention. Benign perceptions of HCV were often referred to in explanations of why further investigations and treatment were not accessed postdiagnosis. The power of this discourse was evident in its residual use even by those who subsequently became more informed and underwent treatment.
Although HCV was minimized and normalized, some participants—particularly women—evidently felt there was a stigma associated with the infection. They worried that consulting the “hepatitis C nurse,” attending the hepatology clinic, and seeking information about HCV in non-private settings risked exposure of their health status. Embarrassment disclosing HCV positivity or admitting risk was a particular concern for women and deterred some from seeking information or testing: I know they'd (health care professionals) … treat ya well and be real nice, but for me anyway, I do be more embarrassed to even say it.
Some participants felt particularly stigmatized because of the route through which HCV was acquired: [P]eople who got it through blood transfusions, people have sympathy for them but because when you're using drugs it's self-inflicted, people aren't going to have sympathy for ya and they basically don't care.
When few or no symptoms were experienced, participants generally assumed their health was relatively unaffected by the virus: “I'm not sick at the moment. It's not affecting me.” Their perception of good health was reinforced by the absence of overt symptoms and the invisibility of liver damage: “[I]f it doesn't affect ya on the outside … ya think you're invincible to these sorts of things.” When health problems were experienced, some participants were uncertain whether they were due to HCV and pointed to other factors as alternative explanations. The view that HCV infection was not significantly impacting their health was frequently given as a reason why investigations and treatment were not sought or engaged with: I was just thinking like, well I'm grand, I don't feel sick … [S]o why do I need to go (to hepatology clinic)?
Participants' narratives revealed benign perceptions and experiences of HCV could be disrupted through a number of means. Information on the health implications of the infection encouraged participants to have a more serious view of their condition, in turn influencing some to seek or engage with interventions: (GP) explained it to me, “Look, I know you don't feel sick now but.… if you just sit and you just leave it, it can get worse and worse and worse and you could be dead in 20 years.” So I thought then. I said “Yeah, ok, put me down. I'll go and I'll get the treatment done.”
Awareness of the potential consequences of their condition was anxiety-provoking for participants, igniting fears about the future of their health: “[A]m I gonna get sick? Am I gonna die?”
Witnessing others visibly ill or dying from HCV was an “eye-opener” described by several that motivated accessing of care: I seen friends of mine getting sick and turning yellow and I says, I better get treatment.
A few participants reported taking up further investigations and treatment as a consequence of receiving biopsy or blood test results indicating the virus was “active” or causing liver damage. The motivating influence of these clinical markers may be due to refiguring perceptions toward illness rather than health: I got … another test off (GP) … and they said it was active in me. So I just said I'd go (to hepatology clinic).
Participants recommended mainstreaming information about risk factors, health implications, and treatment for HCV infection and education of service-users in addiction clinics in particular. Education was seen as vital to address the minimization of HCV and underlying fears. Some participants noted privacy of care was important to minimize stigma.
Perceptions of HCV care: According to other drug users, the investigations and treatments are more severe than the infection itself
When participants realized HCV infection could have serious health consequences, another set of obstacles deterred them from engaging with care—the circulation among their peers of what participants termed “war stories” or “horror stories” about the liver biopsy and treatment. Stories about the biopsy portrayed a huge needle, a painful procedure, and likely injury or death due to professional error: “[S]he let air or something get in when she was taking the biopsy and the chap ended up in hospital.” Stories about treatment emphasized severe side-effects, such as depression, mood swings, weight loss, hair loss, and experiences akin to heroin withdrawal. Less commonly, treatment stories portrayed it as ineffective, counterproductive or dangerous: “[F]rom what I was hearing on the street, it wasn't really helping and then when treatment was finished, people were feeling a lot worse … and one or two people died.” Many participants reported hearing “horror stories” and the fear aroused created reluctance to engage with hepatology services. One interviewee described hearing “horror stories” in a different context: The structural layout and lack of discretion at a hospital outpatient clinic meant the nurses' “war stories” were overheard by patients: [O]ne of the nurses was telling the other one … that some guy who had been on the hepatitis C treatment … had been told in another hospital that because he was on the interferon-ribavirin treatment, that his cholesterol had gone sky high and he had a heart attack … They were discussing that loudly, so that everyone around could hear … [I]t gripped fear into the people who were going down that road.
Participants' fear of treatment side-effects prevented uptake of investigations and similarly, fear of and resistance to the liver biopsy acted as a barrier to treatment.
Many participants described regaining a fear of needles after giving up injection drug use. Those who underwent HCV treatment reported getting used to self-injecting interferon. However, the liver biopsy, and blood tests particularly, created more difficulty: [E]very week I'm in (hospital outpatient clinic) since last June and I still can't get the knack of giving blood. I'm petrified. I hate it … I'll get a ball of tissue and it'll be shredded to pieces by the time I'm finished.
Participants did not report this kind of anxiety or discomfort when describing their experience of HCV screening, perhaps because most were still injecting drugs when initially tested.
Information on investigations and treatment received from health care professionals, from peers who accessed HCV treatment, and from reading material encouraged interest in and uptake of care. Information from health care professionals altered perceptions of investigations and treatment by letting participants know what to expect, putting risks in perspective and allaying some fears: I ended up going and getting the biopsy because of the (GPs) here telling me about it and that it's not barbaric, the syringes they use these days are a lot smaller. He pinched me arm and says like “That's more than what you'd feel actually when you're getting your biopsy.”
Seeing peers and family members complete HCV treatment even through difficult side-effects and having successful outcomes encouraged others. This was identified by several interviewees as having motivated them to seek treatment or accept treatment offers: There was a fella actually in the States that was on the interferon … and it worked for him. And I knew he was very sick and he went through it … [T]hen I met him and he said “It's gone outta me blood, totally gone.” So that's when I said I need to do something about it.
Participants recommended education on investigations and treatment, from the time of testing and diagnosis, to inform service-users what to expect and allay fears. Regarding the liver biopsy, participants advised practice-related strategies to reassure patients, including: informing service-users in advance what to expect of the procedure, providing adequate pain relief during and after, and one interviewee recommended keeping patients in hospital overnight subsequently for observation.
Coping strategies: Blocking awareness, escape, support and positive thinking
Participants used a variety of strategies in coping with HCV infection, investigations, and treatment, including the fears associated with them. Some described actively not thinking about their infection, “pushing it aside,” “try[ing] to forget about it,” which appeared to be a defense against anxiety. Such participants avoided or delayed taking up HCV investigations to protect themselves against “facing up to the truth” or hearing bad news, for example that their liver is badly damaged or they have the genotype least responsive to treatment. In contrast, those who were willing to have the liver biopsy preferred to know the state of their liver. Similarly, those who welcomed the opportunity of screening thought it better to know if they had contracted the infection. Delaying investigations and treatment could generate its own anxiety, as one participant who had HCV for over a decade explained: [I]n the back of me mind all the time I know it's like the clock is ticking … If I don't do something soon … it'll be like too late.
Avoidant forms of coping could be helpful during difficult investigations. Two participants reported using forms of psychological escapism during bloods tests or the liver biopsy to “blank out” fear and pain. As one interviewee eloquently described his biopsy experience: I don't like going in (for a biopsy) … But I'll blank it out as best I can. I've always had from being abused as a kid … this huge ability to escape into like kind of netherworlds somewhere … [S]o I can like sit in a situation that might seem harsh, but like I won't be there … My body might be there but psychologically I'll be astro-flying or something.
Those who sought HCV treatment and accepted treatment offers generally focused on potential benefits such as health improvement or “get[ting] rid of the hep.” Some were hopeful or confident about clearing the virus. Others took the view that “any chance is a chance” and were prepared to give it “one shot.” Such positive thinking helped sustain them through treatment side-effects: I would attribute part of that depression … to the treatment… [T]hen what keeps me going, this is the positive side of it, when it's finished, on a good day I'm gonna feel like really brilliant.
Personal determination assisted a few to persevere through side-effects: I'll give it one chance and I'll do whatever I have to do to give it the one chance … I'll do it to the bitter end, no matter how sore or how painful it is, I'll go ahead with it and just take it as it comes.
The support of partners, family and peers helped participants when treatment was difficult: Having someone to “talk to” and provide encouragement helped in coping with side-effects. Practical support was reported less often but included assistance with childcare and work or study commitments. The education provided prior to and during treatment by health care professionals in hepatology and infectious diseases services, and the attention and concern staff showed throughout treatment, was particularly valued: [E]very time I've come (to hospital outpatient clinic), it's been great. (Nurse) walked through the side-effects, me liver stuff, asked me how everything is. She's been there on the phone. She's called me … That's what the best part of it is. Cos when ya feel like your world's turned upside down and there's someone there that's actually caring about ya, it makes it a lot easier.
A few participants had less educative experiences of treatment: They reported a lack of information and one dropped out of treatment as a consequence. Participants who were struggling with treatment side-effects felt additional support was needed and recommended the development of a peer support structure.
Caring for others was reported by three male participants as ameliorating the impact of treatment side-effects. Two participants who experienced severe side-effects had pet dogs and at times they struggled to maintain their environment. However, the need to feed and exercise their pets improved their own self-care. In the case of one, the emotional bond with his dog was clearly an additional support. [T]hat dog … gets me up early. Keeping him fed keeps me relatively fed, watered, exercised. I've pride in looking after him and having people say “Ah, yeah, he's a lovely coat” or “He's a lovely mannered dog” or “He's very obedient” … So that dog keeps me going.
Another male participant who experienced few side-effects attributed a protective effect to being busy caring for his children. Two female participants had experience of treatment: One had a child but reported struggling to care for him and requiring her parents' help.
Several interviewees recommended counseling to help people come to terms with a HCV positive diagnosis.
Relationships with health care providers: Health care providers' verbal and non-verbal communication influences uptake and attendance at services
Relationships with health care providers, especially trust and confidence in providers, concern for the service-user, and continuity of care, influenced participants' accessing of and engagement with investigations and treatment. Some participants expressed a lack of confidence in health care providers involved in their care or in health care providers in general. Sometimes, they doubted their knowledge and expertise in HCV: “Like AIDS and hepatitis, I don't think doctors know enough about them.” Others' past experiences had created distrust of health care professionals: [A]s far as treatments or anything like that, I wouldn't want treatment … especially off (particular hospital). I mean the trust is just not there anymore.
Participants appreciated when providers showed concern for their welfare. Some felt providers involved in their care were unconcerned about them. Others felt stigmatised by providers on account of their drug use and reported inequitable treatment: “[Y]a can't get past the triage nurse.” Experiences and expectations of stigmatisation discouraged a few from accessing hepatology services.
Continuity of care, where the relationship was positive, allowed familiarity to develop and participants felt comfortable seeking information and receiving care from that provider: (Nurse) was always here (hospital outpatient clinic) any time I'd come up. She was the one gave me bloods. She gives me the needles (interferon injections) in me belly … I think it's a connection. Like I'd sooner quicker (Nurse) stick the needle into me than me partner and I'm with him 14 years.
Participants described a variety of relationships with health care providers, particularly with doctors prescribing methadone: Some reported frictional, distant or impersonal relationships: “Me doctor (GP) knows nothing about me. Me doctor knows me name, that's it.” Others described good rapport and supportive and encouraging relations: “Even though I have slips … I can talk to me doctor (GP) about it.” Participants had mixed experiences of HCV management. Some described GPs who were informative and encouraged further investigations and treatment. Others received little information. When information was imparted, medical jargon could be a barrier to understanding: “The doctor, he just said … “hepatitis C and blah blah blah.” I didn't understand what that meant.” Many felt they knew little about HCV and had significant gaps in their knowledge even years after diagnosis, including misconceptions about routes of transmission, such as believing HCV could be contracted through shared toilet facilities, “dirt” or “dust,” reusing one's own needle, and according to one participant, the “continuous puncturing of your veins.” Some voiced uncertainty about the risk of developing HCV-related complications and how lifestyle factors could impact their condition. Most of those who felt well-informed reported learning what they know quite late in the health care process, from health care professionals at specialist hospital services prior to and during treatment.
Participants recommended greater communication between health care providers and service-users, including explaining the purpose and results of investigations.
Pressures toward and facilitators of HCV care: Contact with services, encouraging professionals, family ties, recovery from addiction, and convenience facilitated uptake of care
Contact with health care or prison services was the main facilitator of HCV screening. Most participants were initially screened when they entered a drug treatment program or prison; some were tested when they were hospitalized. Female participants' contact with services varied slightly from males. At least one female participant was tested when she went for a smear test; another was tested when pregnant. While prison facilitated screening, it was a barrier to HCV treatment for two participants. In the case of one, treatment was not initiated as his sentence was shorter than the duration of treatment; in the case of the second, his hospital appointments were not facilitated by the prison and although given a due date to start treatment, this was never followed up.
Reasons participants gave for having HCV testing included perceiving screening as a routine or standard part of the program or institution. Most did not mind having testing or appreciated the opportunity. One interviewee felt refusing was not a viable option, however: [T]here was a lot of things going on, people getting thrown off their (drug treatment) courses … I don't know if they would've done that if I'd said no. They probably wouldn't have but … why rock the boat?
Other reasons for having testing included concerns about possible HIV infection, perceived risk behaviors such as sharing injecting equipment in prison or with someone they considered likely to have an infection, or because someone they had shared with had tested positive for a blood-borne virus. Although participants cited these additional motivations, the fact that most did not get tested until coming into contact with services suggests convenience is the most important facilitator. Convenience impacted attendance at specialist hospital services and uptake of treatment. Distance from the hospital discouraged attendance. A couple of participants who received HCV treatment at their addiction clinic found this more convenient.
Two participants were screened for HCV infection decades after their drug use, upon becoming symptomatic. Both were approximately 10 years older than the other participants and had given up drug use almost 30 years previously. One had been unaware that he was at risk of HCV infection. He had given up his drug use without any form of treatment. The other had attended a rehabilitation center.
Health problems motivated a few participants to access HCV care post-diagnosis: These participants experienced a deterioration in health or the appearance of disturbing symptoms which they attributed to HCV: “I woke up … and the bottom part of my legs had swollen. Like they were bigger than my head … So … I tried to link back in (with hepatology clinic).” Many of those who were not engaging with investigations and treatment reported they would consider doing so if they became ill.
Those who had HCV treatment or were interested to have it were frequently motivated by emotional ties with partners and children and concern about the impact of a shortened lifespan or poor health upon their family. Some reported that when they met their partner and/or had children that they began to consider addressing their HCV: [S]ee, I hadn't any kids (at diagnosis) … It was only in later years, now that when I have children an' all, ya tend to look at it, ya know, look after yourself, if anything happens me there's nothing to look after them.
Emotional bonds and family responsibilities were usually one of a number of factors influencing treatment.
For some, HCV treatment was part of moving on from drug addiction: HCV infection was viewed as “the last straw” hanging over them from their drug use and addressing their health situation part of their overall life improvement. [T]here's no point in getting off drugs and getting a job if you're gonna have this horrible disease hanging over your head… So I chose to do the interferon and … hope I was cured.
Participants also noted that giving up drugs created a stable space within which they could take care of their health and have time to attend hospital appointments.
A number of participants reported “need[ing] a push” or a “kick up the backside” if they were to have investigations and treatment. The push which they needed usually consisted of encouragement and advice, often from a service-provider: “The doctor sitting there … telling ya “Look, you've hepatitis C. You need to go do something about this.”
Obstacles to and pressures against HCV care: Continued substance use, employment, contraindications, lack of reminders and lack of opportunity reduced uptake and attendance at services
Uncontrolled drug addiction was the main barrier to HCV screening prior to contact with services that participants identified and a barrier to further HCV investigations and treatment. Participants described uncontrolled drug addiction as having their life consumed by drugs: “it's just a constant 24-hour thing,” “it just consumes every part of you.” Days are filled finding money to feed one's habit while the need for drugs crowds out other concerns. Participants emphasized that this diminished life space left little concern for one's health or time to attend appointments.
Employment also made making and keeping appointments difficult, an obstacle that was obviated in specialist hospital services by nurses' flexibility. The potential impact of HCV treatment side-effects upon job performance and ability to make ends meet was a significant concern for those considering treatment. One participant delayed treatment until he had secured job tenure while another had to give up work because of treatment side-effects. Current educational commitments posed a competing priority to investigations and treatment in the case of two participants.
Participants described lengthy waiting times during hospital outpatient visits, which a few noted was difficult for those addicted to drugs. Forgetting dates led service-users to miss hospital appointments, a difficulty which some attributed to the length of time prior to appointments and one interviewee attributed to the tendency of drug users to “live in the here and now.” One interviewee reported recently receiving reminders from the hospital in the form of texts to his mobile phone that helped.
Lack of opportunity to access investigations and treatment was described. A few participants noted difficulty for those not on methadone maintenance programs to access HCV screening or to know where to go for testing. Others reported not being referred to specialist hospital services for further HCV investigations and treatment or being referred after a considerable number of years: It was the first doctor (GP) that told me I had hepatitis. He was the one that had me on the methadone but he never referred me to doctors or never told me that you have to go here about your hepatitis … [I]t was just left.
Several reported their doctor had not discussed treatment availability. Others had not been offered treatment subsequent to referral. A few reported having to “chase” treatment more or less successfully themselves: I … actually chased my doctor (GP) … I'd ring him “Any news, any news?” He said “No news.” So I rang … (hospital) here and I said like “What's the situation like? I put in for this, now I need it. What's happening?” So I got more motivated because me son and me wife but I had to chase it.
Participants perceived the requirement of 6 months abstinence from alcohol and illicit drug use in order to obtain HCV treatment as a barrier for many. Several, however, reported giving up drug or alcohol use in order to obtain treatment: (Hepatologist) said he'd help me with the interferon but I had to stop drinking. So I just stopped drinking.
Two participants had health conditions that contraindicated HCV treatment.
Interviewees recommended making HCV care easier to access. Some suggested a “one-stop shop” approach where all HCV investigations and treatment could be accessed in the one location.
Discussion
Our findings suggest many factors influence access to HCV care by IDUs and rarely is just one factor in isolation an issue. Primary obstacles to care were perceptions of HCV as relatively benign, feeling well and fear of investigations and treatment. This is consistent with previous surveys of IDUs exploring treatment barriers. 9,14 Participants' perceptions were influenced by the discourse about HCV and “war stories” about the liver biopsy and treatment within their peer networks, and compounded by an uncertain knowledge. The study by Lally et al. 16 of IDU women similarly found a low-level of knowledge about HCV was a major barrier to care. Knowledge uncertainty and the discursive production amongst IDUs of HCV as relatively benign have been reported as barriers to HCV prevention. 22
Learning HCV infection can cause serious, life-threatening liver disease, becoming symptomatic or receiving test results showing the impact of the virus encouraged uptake of care, which is consistent with survey findings that physical health problems and being told by a health provider that HCV can cause liver damage and liver cancer are associated with greater treatment willingness. 8,14
Experiences of the infection and perceptions of its management and treatment were not straightforward, however. Some participants expressed uncertainty regarding whether their health problems were due to HCV and attributed them to other factors—highlighting the importance of subjective feelings and judgements as well as clinical markers in perceptions of health and illness. 23 Despite the discourse that “everybody has hep,” some participants—particularly women—felt stigmatized because of the infection and feared exposure of their health status, which impacted negatively on help-seeking. These concerns have also been reported by women who acquired HCV infection iatrogenically, highlighting the need for privacy of care and strategies to minimise stigma. 24 Fear of test results and of pain during investigations are also not unique to the substance abusing population, and are reported obstacles to cancer screening. 25
Difficulties accessing HCV care were reported, including limited knowledge of testing locations, not being referred for treatment, ineligibility for treatment because of drug or alcohol abuse, and the inconvenience of travelling. Participants' accounts of some health providers not referring them for specialist investigations and treatment are consistent with previous findings on HCV management in general practice. 10,26 Participants' accounts of some providers not discussing or offering treatment are also consistent with other studies of IDUs. 8,9,14 Limited knowledge of testing sites and the inconvenience of travelling were obstacles reported by Lally et al. 16 's IDU women also. Whereas Lally and colleagues' 16 participants, however, reported health providers were not as likely to offer hepatitis testing as HIV testing, this was not an obstacle described by our participants.
While the barriers and facilitators identified within this study are broadly consistent with those identified by Lally et al., 16 our participants described a more extensive range of influences on HCV care, particularly facilitators. Additional barriers identified within our study included feeling well, stigma associated with HCV, fear of liver biopsy, forgetting appointments, and demands of work and study. Additional facilitators included becoming symptomatic, the influence of trusted health professionals, a desire to rid oneself of a virus associated with drug use, and the influence of peers who completed treatment. The broader range of influences identified in our study may be due to our more heterogenous sample.
Limitations
A relatively small number of women were interviewed, although this is reflective of the lower number of women in drug treatment. 27 Service-users with ongoing psychiatric difficulties were excluded from the study. This likely limited the potential exploration of mental health problems as a contributing barrier to HCV investigations and treatment.
Only one person who had never been screened for HCV was interviewed. This may indicate successful implementation of protocols around screening. However, most participants were on a methadone treatment program and those who were not on methadone had given up their drug use a number of years ago. Thus, the experiences of current IDUs with little contact with services may be under-represented here.
Implications for clinical practice and future research
Our findings support the mainstreaming of HCV education to target people before they begin injecting drugs and to reach those whose drug use was many years ago and who may be unaware they are infected. Health promotion strategies aimed at IDUs in particular should address perceptions of HCV as relatively benign and views that feeling well mean the virus is having a low impact. Attention should be focused on ensuring IDUs understand the potential health implications of HCV infection, without compounding their fear and reducing possibility of engagement in long-term follow-up. Availability of treatment should be emphasized and lifestyle measures explained (including engagement with follow-up) that may improve their outcomes. Sustained education among IDUs on HCV investigations and treatment should be a priority, so service-users know what to expect and have realistic perceptions of risks and potential side-effects. Involving peers—particularly those who completed HCV treatment—in health promotion efforts may be beneficial.
Increasing accessibility of HCV investigations and treatment should also be a priority. Discussing treatment with IDUs and referring them for specialist investigations emerged as obvious ways of improving access based on the accounts of our participants. Consideration should also be given to providing HCV treatment at locations where IDUs receive their methadone treatment, disseminating information on sites which offer HCV testing, and providing testing at needle exchanges.
Health providers need to be aware that IDUs perceptions of the infection and its care may be conflicted and ambivalent, and there are many and opposing influences on uptake of care which may change over time. Maintaining an open and ongoing dialogue with IDUs, based on trust and concern, may assist their decision-making.
Effective communication regarding the purpose of tests and meaning of results is important for the supportive function it serves and the influence it has on interest in treatment. Preparation for liver biopsy is important—particularly, highlighting the advantage of being better informed about the current health of one's liver and discussing patients' concerns and anxieties. Additional supports while on HCV treatment and peer support should be explored. The intensive education, support and encouragement provided by specialist nurses greatly assisted participants through HCV treatment. We suggest consideration be given to this intervention being provided more widely, especially as part of addiction and hepatology care.
We recommend the perspectives of IDUs who are currently injecting drugs and in little contact with services be explored in future research, as this group likely face challenges different from IDUs on methadone. A fuller picture of barriers to care would be provided by an investigation of the experiences and perspectives of service-providers who deliver HCV care to IDUs and we are currently investigating the obstacles and facilitators encountered by providers. We recommend the strategies suggested above for improving care form the basis of a “complex intervention” and this be evaluated.
Footnotes
Acknowledgments
This study was funded by a Health Research Board grant RP2006/165. Many thanks to the service-users who shared their experiences with us and the health/social care professionals at each site whose assistance made the study possible. We also thank our colleagues Anne MacFarlane (Department of General Practice, NUI Galway), Paul Sullivan (Department of Humanities and Social Sciences, University of Bradford), Jan Klimas, and Catherine Anne Field (School of Medicine, UCD) for their helpful comments and feedback on earlier drafts.
Author Disclosure Statement
No competing financial interests exist.