
Abstract
There is a strong association between domestic violence victimization and HIV infection. This may lead to poor health outcomes including mental health disorders and reduced access to care. A standardized domestic violence screening interview was incorporated into ongoing care in the large and diverse population living with HIV in Southern Alberta, Canada. Results from May through December 2009 are reported, including the prevalence and outcomes of abuse. Thirty-four percent of 853 patients screened reported abuse. Of these, 16% reported abuse in their current relationship, 58% in a previous relationship, and 57% reported a history of childhood abuse. High-risk groups for abuse included females (43%), gay/bisexual males (35%), and Aboriginals (61%). We found an association between a history of domestic violence and delayed access to care (p < 0.05), missed appointments (p < 0.001), and an increased use of clinic resources such as social work (p < 0.0001) and psychiatry (p < 0.001). Mental health conditions prior to HIV diagnosis, including depression (p < 0.0001), suicidal ideation (p < 0.0001), and anxiety disorder (p < 0.0001) were associated with abuse at any time, while a history of adjustment disorder was associated with childhood abuse (p < 0.05). A simple domestic violence screening tool was helpful for identifying patients experiencing abuse in our diverse HIV-infected population. This high prevalence of domestic violence among our HIV patients was associated with poor outcomes and an increased use of medical resources. HIV caregivers should be aware of domestic violence in order to optimize care and refer patients to appropriate support professionals as needed.
Introduction
T
The health consequences of abuse persist well beyond trauma. A World Health Organization (WHO) study concluded that female victims of IPV had poorer self-reported health and were at an increased risk for chronic pain, memory loss, dizziness, and vaginal discharge as well as suicidal thoughts and attempts. 24 Furthermore, IPV is associated with other symptoms such as syncope and seizures, gastrointestinal symptoms, and self-reported cardiac symptoms. 17,18 Childhood abuse has been shown to correlate with a variety of psychiatric disorders. 14,19,25,26
A few studies have examined certain health outcomes associated with abuse within HIV-positive populations. In a study of 50 HIV-positive women currently experiencing IPV, abuse was associated with episodic diseases, chronic pain, and sexually transmitted infections. 27 Abuse may also be associated with a higher mortality rate in HIV patients, 28 although this needs further investigating. A larger study from the United States found that heterosexual HIV-positive victims of violence were more likely to report an outpatient mental health visit in the last 6 months than patients without a history of violence. 29 IPV can prevent access to regular HIV care in numerous ways. 30 Intervening in abusive situations may improve health outcomes and decrease strain on health care resources. Despite a clear association between IPV and HIV, few studies have examined the prevalence and outcomes of abuse within an HIV-positive population.
Several violent domestic events occurring within our patient population prompted us to include an abuse screening interview at the beginning of regular clinic visits as part of routine standardized care at the Southern Alberta HIV Clinic (SAC) in Calgary, Alberta, Canada. In this report, we describe the effectiveness of routine abuse screening in identifying patients for whom abuse counseling may be of benefit. We discuss here the process of incorporating abuse screening into routine clinical practice.
We also examine the self-reported prevalence of childhood abuse and adult IPV within a regional HIV population. Then we assess whether specific clinical factors such as mental illness, suicidal ideation or lifestyle behaviors are associated with a history of abuse. We hypothesize that abuse may significantly impact the health of our patients directly by contributing to poorer health outcomes and indirectly by hindering appropriate care.
Methods
Patient population
The SAC program is an outpatient medical clinic based in Calgary, Canada that provides exclusive multidisciplinary care to all HIV-infected individuals living within Southern Alberta. Demographic and clinical data are collected and updated at each clinic visit. Patients accessing care at SAC sign a voluntary informed consent form allowing administrative data to be used in research projects as approved by the University of Calgary Ethics Committee.
We examined the results of abuse screening for 1053 consecutive regular patient visits between May 27, 2009 and December 27, 2009. All patients at SAC were eligible to be screened and were included in the study population except those with extenuating circumstances, including an inability to isolate the patient (such as those with a family member or in police custody), a significant language barrier, impaired cognitive function, or more urgent medical care issues.
We identified local patients who were both diagnosed and then initiated their HIV care within Southern Alberta allowing us to review from our records any delay in accessing are as well as reported mental health status at the time of HIV diagnosis.
The abuse screening interview
Either a registered nurse (96%) or a research coordinator (3%) sees each SAC patient as part of their routine physician visits. In addition to routine questions, the interview started with a standardized screening question adapted from the Alberta Health Services guidelines 29 :
Domestic violence and the threat of violence in the home is a problem for many people at SAC and in the community; this can directly affect health. Abuse can be a problem in relationships from all cultures and sexual orientations, and can take many forms: physical, sexual, emotional, isolation, neglect, intimidation, or financial.
We routinely ask all patients about domestic abuse in their lives. This often brings up many strong emotions, including different types of fear and uncertainty, but rest assured that this is a safe place to discuss this issue. Have you or your child(ren) ever experienced domestic abuse in any way?
If the patient disclosed abuse, the interview continued in a semi-structured format; interviewers were asked to identify the type of abuse and when the abuse occurred. Responses were grouped into one of three categories based on when the abuse occurred: (1) as an adult with a current intimate partner, (2) as an adult within a past intimate relationship, or (3) as a child (less than 16 years of age). Based on the conversation, the interviewer categorized the type of abuse into one or more of seven categories based on the guidelines 31 : physical abuse, sexual abuse, emotional abuse, isolation, neglect, intimidation, and financial abuse (Fig. 1).
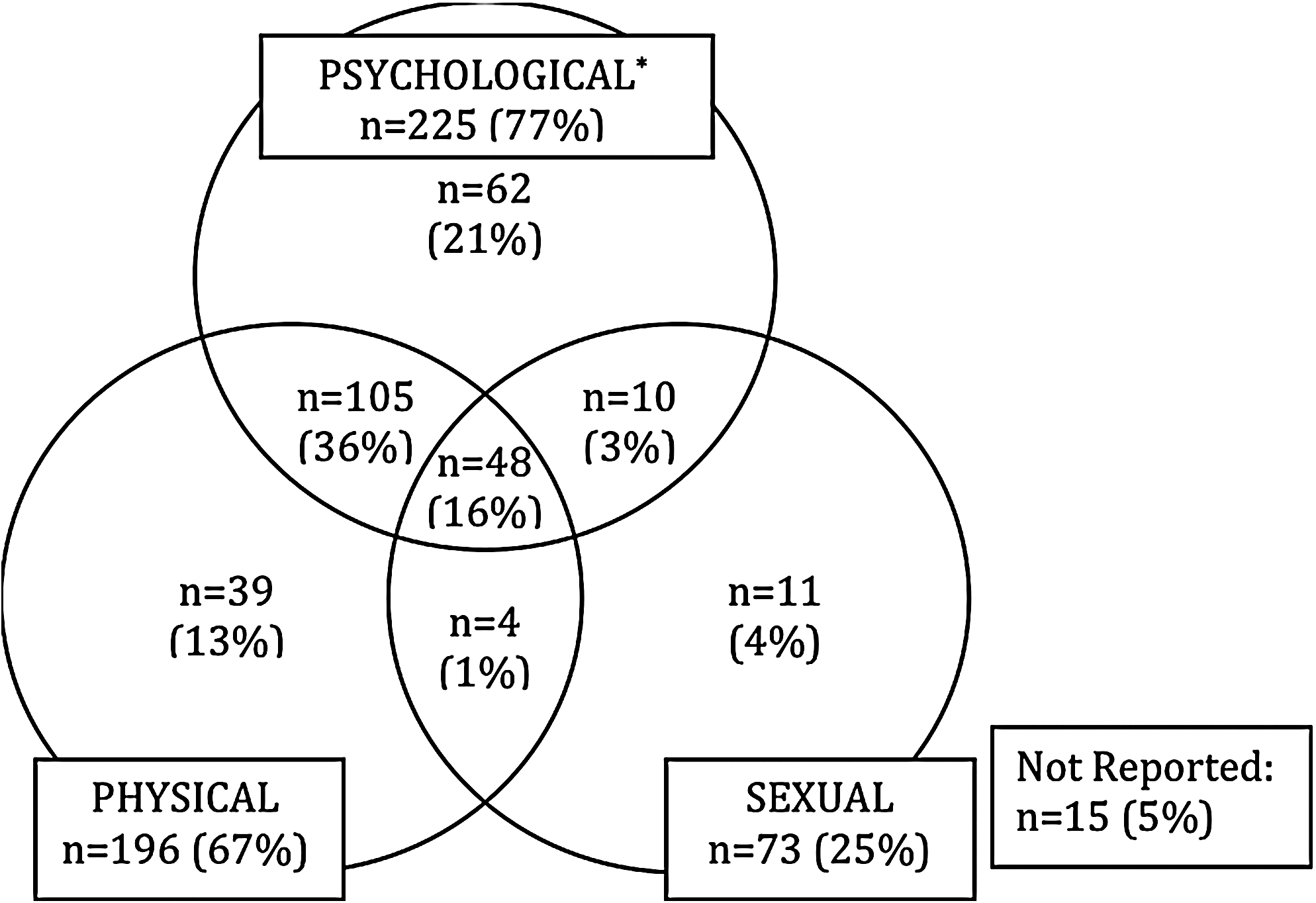
Distribution and proportion of patients experiencing various types of abuse. Abuse is a pattern of controlling behavior (Alberta Health Services Domestic Violence/Abuse Guidelines, 2003). Types of abuse: Physical abuse includes pushing, shoving, biting, hitting, kicking bruising, shaking, restraining, assault with a weapon, burning. Sexual abuse includes any forced sexual activity, sexual harassment, or sexual exploitation. Psychological abuse incorporates the following types of abuse: emotional, neglect, isolation, intimidation, and economic. Emotional abuse includes put-downs, being critical of appearance and/or abilities, excessive jealousy, accusations of infidelity. Neglect includes withholding medication or food, not assisting with matter of hygiene if the abused is a person with a disability. Isolation includes cutting one off from friends and/or family. Intimidation includes threat to kill/hurt friends and/family, violence or threats of violence to pets and/or objects. Economic abuse includes accessing one's funds without permission, controlling how one spends your money, financial dependence.
Every patient disclosing a current abusive situation was asked: “Do you feel safe in your current relationship?” to help identify high-risk situations. 31 Patients indicating safety concerns were promptly referred to a clinic social worker. In addition, social work and/or psychiatric consultation services were made available to any other patients requesting assistance.
Data collection and analysis
Patients were categorized into two groups based on disclosure of abuse as a direct response to the screening question (i.e., a positive screen) compared to patients not reporting abuse (i.e., a negative screen). Patients were further divided into two subgroups: (1) current or past abuse as an adult (adult IPV) and (2) abuse during childhood.
Self-reported sociodemographic characteristics including gender, age at HIV diagnosis, race/ethnicity, sexual orientation, level of education, and HIV-infection risk factor were recorded at the initial clinic visit. In addition, every 3 months patients are asked as part of their regular follow-up at SAC about lifestyle behaviors such as alcohol and tobacco use. Alcohol use is categorized into three categories: heavy (more than 9 drinks per week for females, more than 14 drinks per week for males or a self-reported binge), moderate (less than 9 drinks per week for females and less than 14 drinks per week for males), or none. Cigarette smoking and IDU were reported as either yes or no. Patients known to have ever been incarcerated for more than 60 days were also identified.
For local patients, we evaluated how rapidly newly diagnosed patients accessed HIV care by calculating the number of days between their HIV diagnosis and their initial SAC visit. Because individuals in Southern Alberta cannot obtain HIV care outside of the SAC program, this is a relatively precise measure of any delay in accessing care upon receipt of an HIV-positive diagnosis.
We also calculated the percentage of regularly scheduled clinic visits local patients missed since initiating care at SAC, and assessed whether they accessed other clinic services such as social work and psychiatry. We evaluated how often local patients missed appointments by calculating the percentage of missed regular clinical visits compared to booked clinic visits.
Detailed patient medical history collected during the initial clinic visit included details about previous diagnoses including the mental illnesses: adjustment disorder, anxiety disorder, depression, and suicidal ideation. We included these preexisting psychological factors in our analysis to assess whether there was a relationship between mental health, history of abuse, and the receipt of HIV health care services.
All data were analyzed using p < 0.05 as the level of significance. Univariate binomial comparisons were tested using two-tailed Pearson's χ 2 , while t tests were used for continuous variables.
Results
Prevalence
A total of 853 of 1053 (81%) of consecutive patients attending a regular clinic visit between May 27 and December 27, 2009 were screened. Patients who were not screened (n = 243) did not differ significantly by gender, age, race/ethnicity, sexual orientation, or HIV risk factor. Patients were not screened for a variety of reasons, usually due to extenuating patient circumstances, however some patients declined screening and others were missed because of staff time constraints. Two hundred eighty patients disclosed abuse in response to the initial screening question and an additional 14 patients reported abuse on further discussion with the interviewer for a total of 294 (35%) patients reporting a history of abuse. Overall, 14% of the study population only reported IPV as an adult, 9.5% only in childhood, and 9.6% stated they had experienced abuse both as an adult and as a child. 14 (4%) reported earlier abuse but did not specify precisely when the abuse occurred. Twenty-three percent of patients reporting adult IPV stated that it had occurred within their current relationship whereas 85% stated that it had occurred in a past relationship; abuse occurred in both current and past adult relationships for 9% of the respondents.
Nine (19.6%) of the 46 patients reporting abuse in their current relationship did not feel safe in their present situation and were referred to a clinic social worker. In more than 25 other cases, a referral was made to social work, psychiatry, or further counseling elsewhere.
Types of abuse (Fig. 1)
Of those abused, 172 (58%) reported more than one type. Psychological abuse, encompassing emotional (77%), neglect (7%), isolation (12%), intimidation (13%), and economic abuse (12%), was the more prevalent form of violence followed by physical (67%) and sexual (25%) abuse. Fifteen patients did not specify the type of violence they experienced.
Demographic characteristics
Females were more likely to have been abused compared to males (p < 0.01) with 43% reporting some form of abuse. There was no association between abuse and age at HIV diagnosis (Table 1).
Bisexual includes 52 males and 5 females.
Self-reported at initial visit.
Includes First Nations, Inuit, and Métis.
Includes 162 patients native to sub-Saharan Africa, 1 born in the United States, and 4 born in Latin/South American.
OR, odds ratio; CI, confidence interval; IDU, injection drug use; MSM, men who have sex with men; MSW, men who have sex with women.
Aboriginal Canadians (i.e., First Nations, Métis, and Inuit) had the highest prevalence of reported abuse (61%), while those self-identifying as black had the lowest (20%); significance was maintained for both childhood and adult abuse.
A significant difference in reported abuse was found between groups based on gender and self-identified sexual orientation (p < 0.01). Heterosexual females (41%) were more likely to report abuse than heterosexual males (26%); 34% of gay males and 44% of bisexual patients (both males and females) had experienced abuse. A strong correlation exists between being abused as a child and being victimized as an adult (odds ratio [OR] = 9.0, 95% confidence interval [CI] = 4.92–16.46).
When considering HIV risk factors, patients with IDU are more likely to report current or past abuse (49%) than men having sex with men (MSM; 34%) or men having sex with women (MSW; 31%; p < 0.001). IDU had a higher risk of child abuse and trended higher for adult abuse as well. Of note, MSM were more likely to be abused as children than MSW.
Additionally, specific lifestyle factors that correlate with abuse include smoking (p < 0.001), less than high school education versus some university or college education (p < 0.0001), a known history of incarceration (p < 0.05), and IVDU (p < 0.05; data not shown). There was no significance found for alcohol abuse.
Preexisting psychological factors
Overall, 25% of 604 ‘local’ patients reported a history of clinical depression, 15% anxiety, 11% suicidal tendencies, and 4% adjustment disorders at the time of HIV diagnosis (Table 2). Patients reporting any of these conditions at the initial visit were more likely to have reported abuse (p < 0.0001), except adjustment disorder which approached significance (p = 0.08). Of patients reporting abuse, 36% had a history of clinical depression prior to their HIV diagnosis, 23% had episodes of anxiety, 17% thoughts of suicide, and 6% had a previous professional diagnosis of an adjustment disorder. A history of childhood abuse was significant in all of these conditions (p < 0.0001, p < 0.0001, p < 0.0001, and p < 0.05, respectively).
IPV, intimate partner violence; OR, odds ratio; CI, confidence interval.
Accessing care
The median CD4+ lymphocyte count at time of first evaluation for patients reporting abuse was higher 348/mm3 (interquartile range 150–575) than for those who did not report abuse (263/mm3, 94–490). Twenty-eight percent of abused patients classified as late presenters (i.e., <200/mm3) compared to 40% of patients who did not report abuse (p < 0.05). Patients with a history of abuse were also more likely to have delayed accessing care at SAC (Table 3). The time from diagnosis to initial visit was more than 90 days for 27% (57/208) of abuse patients compared to 19% (76/389) of nonabused patients (p < 0.05).
Once in care, local patients with a history of abuse missed more scheduled regular clinic visits and saw clinic social workers and psychiatrists at a higher frequency than local patients with no history of abuse. Patients disclosing abuse missed on average of 20.7% of scheduled medical appointments compared to 15.2% for non abused patients (p < 0.001). Patients with a history of abuse were also more likely to previously have attended one or more appointments with a clinic social worker (82% versus 65%, p < 0.0001) and a clinic psychiatrist (35% versus 21%, p < 0.001) than those with no history of abuse.
Discussion
The implementation of the abuse screening survey within a clinical setting was well received by both patients and staff. The initial screening question elicited responses in over 96% of patients presented with the survey; however, some patients only admitted abuse with further discussion. This underscores the importance of open dialogue between the interviewer and patient. There may be some fear associated with disclosing abuse to a health care worker; however, HIV-care sites may be the ideal place for abuse screening because engagement with the same caregivers repeatedly for an extended time helps foster trusting relationships, which may increase willingness to disclose. The screening question alone captured most of those disclosing abuse.
The availability of in-house social workers provided access to immediate and extensive counseling. Other patients were referred to psychiatrists, professional abuse counselors, or health care professionals outside of SAC, as required. Although there is limited evidence of effective interventions, 32 nine patients required immediate intervention in their current situation. For safety purposes, all receive regular follow-up on their situation. In some cases, we facilitated the transition to a safe housing shelter, removing the patient from immediate risk of harm.
Subsequent clinic visits may give patients previously not disclosing abuse a safe venue to discuss abuse at their discretion. The relationships established within HIV-care may be the only opportunity a patient has to discuss these issues in a safe environment.
The prevalence of self-reported abuse among our population was 35%; 67% of those patients were abused as adults, and 53% as children. These findings are consistent with previous studies identifying a high prevalence of violence victimization among HIV-infected persons. 2 –6,10,33 In the United States and Canada, the prevalence of physical assault among ever-partnered women was estimated at 22% and 29%, respectfully, 34,35 while the prevalence of domestic abuse of all types (i.e., physical, sexual, emotional, isolation, neglect, intimidation, and economic) among women in our study was 43%. The high prevalence of abuse within the HIV-infected community highlights the need for domestic violence intervention and awareness programs targeted specifically at those living with HIV.
In our study, women were 1.6 times more likely than men and over twice as likely as heterosexual men to have experienced IPV, which is consistent with other research. 10,36,37 Violence against women is gaining international attention as a global problem with significant health consequences. Given that women comprise over half of HIV infections worldwide, 38 violence against women is an important part in the fight against HIV. Violence against women intersects with the HIV pandemic through multiple pathways such as direct transmission through forced intercourse, increased sexual risk-taking behaviors, abuse after disclosure of HIV status. 9,10
We found a high rate of abuse among gay and bisexual males in our population; these groups are often overlooked. 36,37,39,40 HIV disease continues to disproportionately affect MSM 38 ; it is therefore important to recognize the high rate of abuse within this population. Although there is sparse evidence addressing same-sex intimate partner violence (SSIPV) and HIV, one study found a positive correlation between psychological abuse and physical abuse among HIV-infected MSM in urban areas of the United States. 41 In our study, gay and bisexual men were almost twice as likely as heterosexual men to have a history of IPV, which suggests abuse may be an underlying factor contributing to the HIV epidemic within this group. Public health policy addressing the high prevalence of SSIPV among HIV-infected men may help reduce HIV incidence.
The global burden of childhood abuse has not been consistently measured; however, one study suggests that the childhood abuse rate is less than 10% for males and between 10% and 20% for females. 37 A higher prevalence of child abuse among gay men has been shown previously, 28 which was not seen in our analysis; however, MSM were more likely to have experienced child abuse than MSW and bisexuals had higher rates than both gay and heterosexual men. In our study, 19% of males experienced child abuse. It is difficult to know whether our HIV-infected population has a higher risk of previous childhood abuse.
We found observable differences of those indicating abuse in the black and Aboriginal populations. Black patients were primarily immigrants native to sub-Saharan Africa (97%) and reported significantly lower abuse rates than the Caucasian population. Our findings contradict abuse estimates from studies conducted in Sub-Saharan Africa, which show rates of IPV against ever-partnered women higher than 40%. 24 Our findings mirror those of the 2003 Canadian Women's Health Surveillance Report which found that women born outside of Canada report lower rates of all types of violence compared to Canadian-born women. 42,43
Canadian Aboriginal peoples have a high prevalence rate of HIV infection 44 and violence against women. 36,42 In our study, Aboriginal peoples had the highest prevalence of abuse at 61%. A greater focus on abuse prevention and intervention within this population may help reduce the burden of violence among Aboriginal communities and improve HIV-related outcomes.
Of the seven types of abuse examined, emotional abuse, physical abuse and sexual abuse were the most common. To our knowledge, there is no previous research examining the prevalence of various forms of abuse among an HIV population. Evidence suggests that psychological abuse may predict of poor health outcomes as strongly as physical or sexual violence. 16 –20,45 Most patients reporting abuse experienced multiple types, which have been shown to have an additive effect influencing health outcomes, 16,19 although further research is necessary in this area.
Our finding that abuse victimization is related to less education is supported by other findings, 6,8,23,41 as is smoking, 46 and IDU. 2,10,17 One study suggested a bidirectional causal relationship between drug abuse and IPV. 47
Our study builds on previous knowledge linking poor mental health with both childhood abuse and adult IPV, 24,48,49 and extends it to an HIV-infected population. We suggest there is a link between abuse at any time and a clinical history of depression, anxiety and suicidal ideation prior to and after an HIV diagnosis. Psychiatric disorders, especially depression, have been shown to predict poor HIV outcomes 50 and may complicate care. 51 Notably, our study found that a history of adjustment disorder at the initial clinic visit was associated with a history of child abuse but was not significant for domestic violence victimization as an adult; childhood abuse may lead to maladaptive coping mechanisms. Clinicians must take abuse into account when managing psychiatric disorders within HIV patients because of the higher risk of abuse victimization as well as its associations with health.
In our population, patients with a history of abuse generally were diagnosed earlier in their disease (based on higher CD4+ lymphocyte counts), which may be a result of more frequent usage of medical resources. 52 They were, however, more likely to delay initiating HIV treatment, and miss more appointments than nonabused patients. Patients who attend appointments less regularly have been shown to have lower CD4+ cell increases and attain undetectable viral loads less often than patients with better attendance. 53,54 Patients with a history of abuse were more likely to previously have been referred to a social worker and a psychiatrist. Patients with a history of abuse may require additional support and utilize more health care resources.
Although our study underlined the impact of domestic violence within an HIV-infected population, there were some limitations. The intent of the abuse screening process was primarily clinical and therefore conducted using semistructured interviews, which may have led to interviewer biases. There may also have been a selection bias within the screening process; for example, patients who were too sick to be screened may be more likely to have been abused. However, this was most likely minimal as 81% of patients were screened for abuse and the patients who were not screened were demographically similar to those screened.
Using a simple abuse screening tool, we found a high prevalence of abuse among our HIV-positive population and identified groups with an increased risk: women, gay/bisexual men, and Aboriginals. HIV-care sites may be the ideal location for abuse screening because continuous follow-up fosters trusting relationships that may enable successful interventions. Domestic violence screening is an important first step in identifying individuals who may be suffering from abuse and its consequences. Further research is needed to identify optimal interventions; however, facilitating safer living situations for some patients may justify screening in itself. HIV caregivers need to be aware of the high rate of abuse among their patients and encourage screening given the high impact of domestic abuse on health outcomes such as consistent access to HIV care, mental health, and physical health.
Footnotes
Acknowledgments
The authors would like to thank Christina Carrillo, Darcia Latimer, Sherry Hurtubise, Nel Burroughs, Janet Furseth, Patricia Miller, Natalie Marshall, Kevin Dong, and the staff at the Southern Alberta Clinic for their hard work embracing and administering the screening survey. Ms. Carrillo and Miller were instrumental in the development of the screening program. We also would like to thank Linda McCracken for lending her expertise to the development of the screening question and staff training.
Author Disclosure Statement
No competing financial interests exist.