
Abstract
Following the introduction of highly active antiretroviral therapy, an expanding cohort of adolescents with perinatally acquired HIV (PaHIV) is surviving and emerging from pediatric services with complex transition health care requirements. Transfer from pediatric to adult services has been associated with poorer health outcomes in other chronic diseases. Young people with HIV have the additional burden of stigma, secrecy, and the risk of transmitting HIV to partners and offspring. Maintaining engagement in health care during adolescence is critical. We compare reported satisfaction surveys of health care experiences and preferences of young people with PaHIV attending a U.K. transition outpatient service with young people attending a young persons' diabetes transition service in Australia. All 21 patients in the United Kingdom and 39 young people approached in Australia agreed to participate. The median age for both groups was 19 years, 67% of the PaHIV group were black African and 74% of diabetic group white Australian. Ninety-five percent (18/19) of those with PaHIV and 87% (34/39) with diabetes felt their transition was an easy process. Sixty-eight percent (13/19) of young people with PaHIV and 72% (28/39) of diabetic patients felt moving to their current service had a positive effect on their health. Being treated as an individual, comprehensive management explanations and encouragement to develop independence were cited as “strongly important” by over three quarters of participants with PaHIV. This service evaluation illustrates that careful transition can be a positive event for young people with PaHIV, comparable to that of a well-established diabetes services.
Introduction
A
Transition preferences and experiences of adolescents with a range of chronic diseases have been described. 16 –20 A multicenter U.K. study of over 300 adolescents with juvenile idiopathic arthritis and their parents showed a significant improvement in overall care satisfaction following introduction of a transition program, 17 which included individualized transition plans, a local program coordinator, and age-appropriate transition resources. 21 An Oxford study of 279 young people with diabetes reported significantly higher attendance rates and satisfaction when young people had the opportunity to meet the adult physician prior to transfer. 16 In contrast direct transfer to adult services has been associated with increased morbidity and mortality in some chronic diseases. 22 –24 There is little data reported on patient experiences following the transition care of adolescents with perinatally acquired HIV (PaHIV). 25,26
Following the introduction of highly active antiretroviral therapy (HAART) there has been a significant decrease in HIV associated morbidity and mortality for children with PaHIV. 27,28 Young people with PaHIV are a new and evolving cohort; health care systems require adjusting and developing to meet their specific and complex needs. 29 In comparison to countries (e.g., the United States and Australia) where adolescent care is a recognized specialty, the United Kingdom lags behind in the development of dedicated services for young people living with many chronic medical conditions.
Adolescents living with PaHIV 30 have additional complex medical and psychosocial issues not encountered by other young people with chronic ill health, which require careful consideration to achieve successful transition care. This cohort not only faces the unknown with a lack of data on long-term complications of both HIV infection and the toxicities of HAART but they also have a disease that is potentially transmissible to future sexual partners and their own children. Complex psychosocial obstacles include stigmatization and the challenges of disclosing their HIV status to friends and sexual partners, potentially at coitarche. 2,31 The family impact of PaHIV means some are young caregivers for infected family members 32 while others have lost parents or siblings. 25,31,33,34 Furthermore, the neurocognitive impact of living with HIV throughout childhood is becoming increasingly apparent with poorer school performance, 35,36 particular difficulties in executive functioning, 37 and an increased burden of mental health disorders. 38
Adherence to often complex HAART regimens is necessary in order to maintain virologic suppression, 39 –42 limit the development of viral resistance to therapy 43 and reduce the risk of onward sexual 44,45 and vertical transmission. 46 In order to sustain these goals successful engagement in health care services as well as facilitating young people to take full responsibility for their own health care needs through multidisciplinary support, peer support, and education is critical.
While the Australian Diabetes Transition Support Program (DTSP) has published data describing a significant improvement in diabetic control (HbA1c) and a reduction in diabetes-related ketoacidosis admission rates by one third (p=0.05) 47 following implementation of their transition program, there remain little data on patient experiences of transition models in the United Kingdom for young people with PaHIV. For this reason we chose to compare the health care experiences and preferences of young people with PaHIV attending a new dedicated outpatient U.K. transition service called the 900 Clinic with young people attending a well-established Australian transition service for young adults with diabetes.
Methods
Questionnaire
U.K. Clinic PaHIV
A medical student independent to the service designed and administered a semistructured questionnaire for use in both the United Kingdom and Australia, assessing the transition preferences and care satisfaction of young people attending the services. The questionnaire was piloted by one service user attending the U.K. clinic. The final questionnaire comprised both 7-point Likert scale questions as used by Shaw et al. 48 and open questions prompting free text comments. For each Likert-choice question regarding health care experiences, participants were asked to select “strongly agree,” “agree,” “slighty agree,” “neither agree nor disagree,” “slightly disagree,” “disagree,” or “strongly disagree” for a range of statements. Questions asking about health care preferences required patients to respond to a statement using a similar 7-point Likert scale ranging from “very important” to “not important at all.” Each responder completed their voluntary and anonymous questionnaire in the waiting room and sealed their responses in an envelope. All participants were provided with a letter informing them of the purpose of this service evaluation, how their responses would be stored anonymously, and how such responses would be presented. A verbal explanation was also provided to ensure that all participants were able to give informed consent. All identifiers were removed and responses were stored and analyzed using SPSS (Statistical Package for the Social Sciences) Version 17.0 (SPSS Inc., Chicago, IL). Young people that had transitioned up to 3 years previously were included in the service evaluation. The U.K. service evaluation was approved by the clinical governance department at St. Mary's Hospital, London.
Australian DTSP
A shorter version of the same questionnaire was distributed (following quality assurance project approval by the Westmead Scientific Advisory Committee) at the DTSP at Westmead Hospital, Sydney. This questionnaire only included questions on experiences in their current clinic and of their transition, with the preferences questions omitted. The transition coordinator distributed the questionnaire and the results were analyzed by a medical student independent to the clinic. The transition coordinator was not able to see responses as each responder completed their voluntary and anonymous questionnaire in the waiting room and sealed their responses in an envelope. All participants were provided with a letter informing them of the purpose of this service evaluation, how their responses would be stored anonymously and how such responses would be presented. A verbal explanation was also provided to ensure that all participants were able to give informed consent. The results from this group were stored anonymously and analyzed in the same manner as the 900 Clinic data.
Patient groups and transition services
U.K. Clinic PaHIV
Young people with PaHIV attending a transition service at Imperial College Healthcare NHS trust called the 900 Clinic were invited to participate between July 2008 and February 2009. The clinic team consists of a consultant pediatrician in infectious diseases, an adult senior lecturer in HIV genito-urinary medicine, an adult HIV clinical nurse specialist, and an adult psychologist. The transition process is based upon the sequential model, 4,12,49 where initial preparation occurs at an adolescent-centered pace in the pediatric family clinic and then shared pediatric–adult care occurs within the 900 Clinic itself. The timing of transition to the 900 Clinic was determined not by chronological age but tailored to the individual adolescent. Transition readiness was achieved by demonstrating a basic health care awareness, an awareness of their status, an understanding their disease, and the initial development of their health care management skills. Ongoing transition preparation and assessment was commenced during early adolescence in the family clinic by a multidisciplinary team of pediatricians, psychologists, occupational therapists, physiotherapists, the patient's parents/guardians, and the young person with PaHIV. Self-efficacy, managing their own tablets with parental supervision, and seeing the doctor alone for increasing proportions of consultations are examples of strategies used to encourage independent health care behaviors within the family clinic. The adolescent's perception on their own transition readiness was explored and essential to gauging transitional timing. A multidisciplinary approach is used in the 900 Clinic where adolescents are initially seen by the pediatrician and slowly progress to consultations solely with the adult genito-urinary doctor and nurse specialist, with ongoing psychological involvement if appropriate. Health care management skills and behaviors are focused on throughout ongoing transition within the 900 Clinic. Following an individualized and age-appropriate protocol for transitioning from pediatric to adult-style consultations aims to ensure that young people transition to adult services completely when they have attained appropriate adult health care management skills and behaviors. Young people attend the 900 Clinic for approximately 6 to 8 years before being transferred to an adult outpatient service also based at St. Mary's Hospital.
Australia clinic
Questionnaires were distributed during October 2008 to February 2009 by the diabetes clinical nurse specialist as the transition coordinator for the service. A dedicated service for 15- to 25-year-olds established in 2001 follows a direct transition model 12,49 with comprehensive multidisciplinary patient handover from the pediatric service in the Westmead Childrens' Hospital to the adult team based at the adjacent but distinctly separate adult Westmead Hospital. No conjoint clinics are conducted at transition. The transition coordinator is responsible for providing adolescents with written and audio-visual information about the adult service, contacting patients by telephone to book their initial appointment, and following up and rebooking missed appointments by telephone, text messaging, and e-mail. 47 Each adolescent is sent a DVD entitled “Moving On” introducing them to the Westmead Transition Service for diabetes, which includes welcoming videos of the staff in the clinic environment.
Results
Demographics
United Kingdom
Twenty-one of the initial 30 young people with PaHIV who had transitioned to the 900 Clinic were approached and all agreed to participate in the service evaluation. Twelve (57%) were female, 67% were black African, and the median age was 19 years (range, 17–21). Not all respondents completed all the questions.
Australia
All 39 young people approached completed the questionnaire; 22 were female, 28 of 38 (74%) were white Australian, and the median age was 19 years (range, 16–22).
Comparison of patient reported satisfaction between the clinic populations
Overall, very high levels of satisfaction were reported by both groups of young people. Figure 1 shows the comparable satisfaction between the DTSP and 900 Clinic. Ninety-five percent (19/20) of young people with PaHIV reported satisfaction with the care they received in U.K. family pediatric clinic and 100% reported being satisfied with the care provided by the 900 transition care clinic. From the Australian cohort 35 (90%) and 36 (92%) of responders were satisfied (“strongly agreed/agreed”) with the care they received at their pediatric clinic and DTSP, respectively. All 900 Clinic responders and 92% (36/39) of DTSP participants felt that they were allowed enough time to discuss their problems. All 900 Clinic responders felt they were treated as an individual and reported feeling comfortable discussing their health and concerns with the 900 team. All young people with PaHIV and 89% (34/38) of DTSP responders reported receiving comprehensive management explanations. Eighty-six percent (18/21) of the PaHIV cohort and 79% (31/39) of DTSP participants “strongly agreed” or “agreed” that they were encouraged to develop more independence and control of their care. Eighty-four percent (16/19) of 900 Clinic and 82% (31/38) of DTSP responders “strongly agreed/agreed” that transferring to their current clinic was explained properly beforehand. Eighty-four percent (16/19) of 900 Clinic and 55% (21/38) DTSP participants “strongly agreed/agreed” they had the choice to move to their current outpatient service when they were ready. Sixty-eight percent (13/19) of 900 Clinic and 72% (28/39) of DTSP responders felt moving from the pediatric to their current service had had a positive effect on their health and well-being. Furthermore, 95% (18/19) of 900 Clinic and 87% (34/39) of DTSP participants felt that their transition had been an easy process.
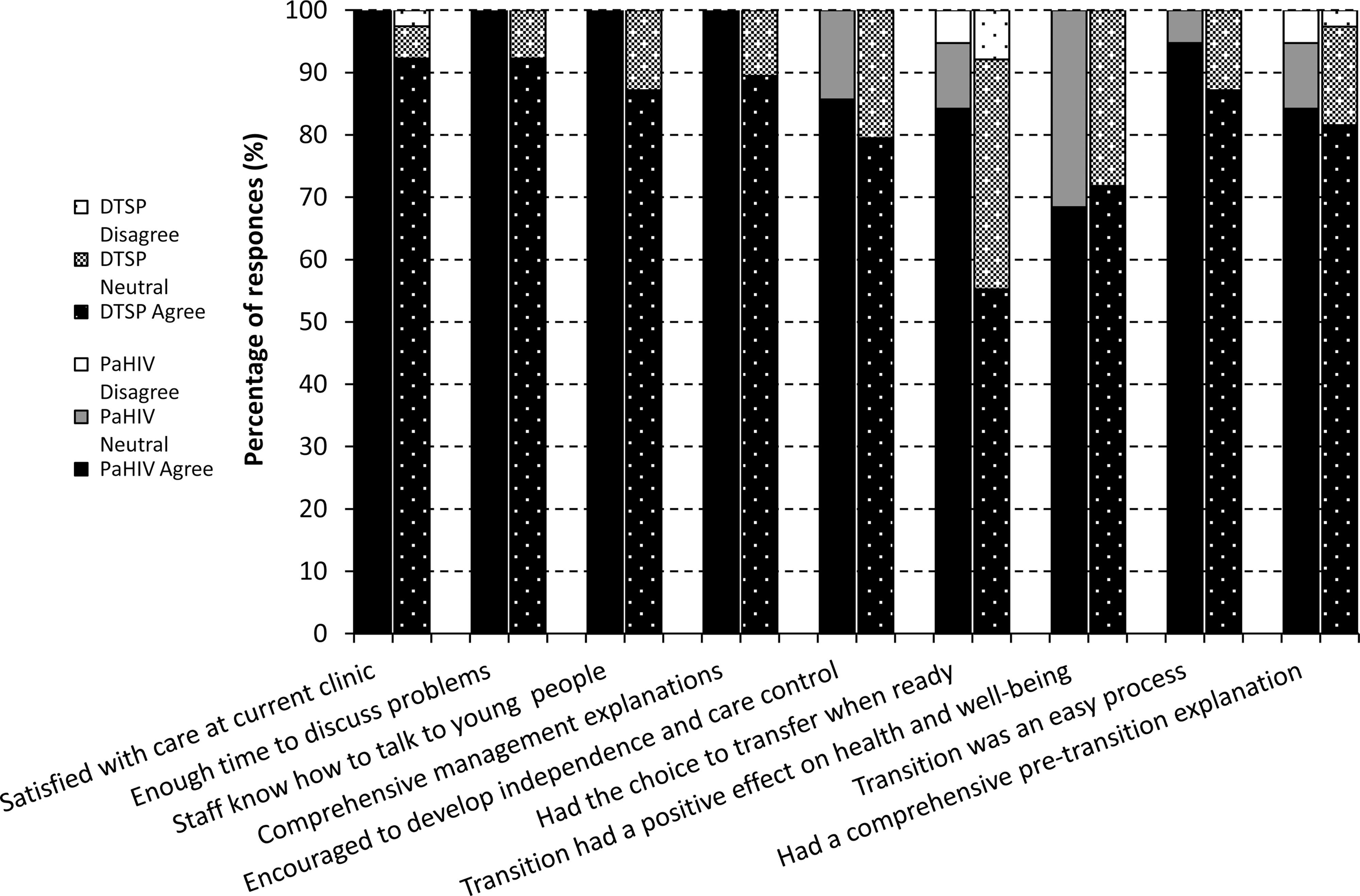
Transition and health care satisfaction of the 900 Clinic for young people with perinatally acquired HIV (PaHIV) and the Australian Diabetes Transition Support Program (DTSP) clinics compared. First bar of each cluster represents the satisfaction of those attending the 900 Clinic service (PaHIV) and the second cluster (dotted) shows the satisfaction of responders in the DTSP clinic. Disagree=“strongly disagree” and “disagree”; Neutral=“slightly disagree,” “neither disagree nor agree,” and “slightly agree.”
Qualitative experiences
Table 1 summarizes comments made by patients at each of the clinics. Many common themes emerge. Being treated as an adult by staff who listen and respect the views of young people was critical. Both groups commented that they valued the age-appropriate environment of their service. The PaHIV participants expressed satisfaction with a nonstigmatizing environment, which was not raised as an issue by the diabetic patients. Not being ready to mix with adults was more frequently expressed by the 900 clinic attendees than the diabetic service users. All responders from the 900 Clinic agreed that the clinic was more favorable than adult clinics; the reasons given are “because I feel at ease with other young people”; “it feels more individualized+less intimidating”; and “older people are scary.” Seventeen participants “strongly agreed/agreed” that the 900 Clinic was more appropriate for them than the Family Clinic; reasons given for this were “I don't feel like a child”; “I get treated like an adult+my opinions are valued”; and “because I am treated as though I am mature enough to have control of my own health care.” Participants from the DTSP commented that “the staff treat me as an adult, unlike at the children's hospital, where it was intended for children” and “… it is more welcoming and laidback than the children's hospital for this age group.”
All comments are presented here using the words and grammar used by the individual responder.
When asked what was good about their service, participants in both the 900 and DTSP Clinics commented on the openness of staff, willingness to listen and encouragement of young peoples' participation in treatment decisions (Table 1). In addition 900 Clinic participants commented on the importance of inclusivity and lack of stigmatisation. Comments included “The 900 Clinic allows you to feel you're a part of a group of young people all dealing with HIV. I personally feel if I continued in the family clinic or moved to adult care I would feel alienated for many reasons …” and “It doesn't make you feel labelized as having HIV. I feel less daunted about coming to the hospital.” When asked what could be better about their service, many of the comments from both clinics focused on making the clinic available on different days or at locations closer to their home. The few suggestions for improving services for both clinics included further integration of pediatric and adult services and SMS reminders for clinic appointments were suggested by the diabetics but not the PaHIV participants (Table 1).
Transition preferences for the U.K. PaHIV population
To establish the key factors that might improve service provision, the transition preferences of young people attending the U.K. PaHIV service were explored further, summarized in Table 2. Of the 20 patients who had undergone transition, all participants thought that the staff knowing how to communicate with young people and feeling comfortable discussing concerns and health problems with staff were “very important/important.” Nineteen thought having the choice to move when ready was “very important/important” and 16 “strongly agreed/agreed” that they had transitioned when they were ready. Having transition explained prior to transfer, being allowed enough time to discuss problems and knowing the name of the staff in charge of their care was “very important/important” to 95% (20/21) of respondents. Comprehensive management explanations, encouragement to develop independence, and being treated as an individual were rated as “very important” care preferences by 81% (17/21), 76% (16/21), and 81% (17/21) of the young people who responded at the 900 Clinic. Conversely, of the factors that were considered less important, 47% (10/21) thought having the chance to meet other young people with the same condition was “very important/important” and 5 of 21 felt having other young people in the waiting room was “strongly important/important.”
Data are no. (%) of those who responded to each question.
Important=“very important” and “important”.
Neutral=“Slightly important,” “Neither important or unimportant” or “slightly unimportant”.
Unimportant=“Not important” or “Not important at all”.
Inpatient experiences U.K. PaHIV clinic patients
Of the 9 young people who had experienced adult inpatient care, 5 were dissatisfied and four felt the ward staff did not understand their needs, commenting; “they didn't quite understand the needs/my needs as a young person …” and “[I] was put in a large ward in cubicals and felt very exposed.” All stated that they would rather be admitted to a ward designated specifically for young people.
Discussion
We explored the transition care preferences and experiences of a novel and expanding group of adolescents living with PaHIV. We compared the care satisfaction of this group with those attending an established transition service for young people with diabetes in Australia. This preliminary qualitative service evaluation suggests that transition can be perceived as a positive event by young people living with PaHIV and diabetes, when dedicated transition services are provided. The care satisfaction of those attending the recently established 900 Clinic for young people living with PaHIV was comparable with the satisfaction of those attending the well-established DTSP. Being encouraged to develop adult health management skills, being treated as an individual, and being assessed in an age-appropriate environment are reported as highly important care preferences by young people with PaHIV.
A preliminary U.K. study by Miles et al. 25 in 2004 used semistructured interviews to explore the transition care of 7 young people with HIV aged 16–22 years; 4 were perinatally infected and 3 contracted HIV from blood products. Although this is a very small cohort, participants recommended the development of an age-specific environment, amalgamation of pediatric and adult care, and patient-centered transition timing. 25 Our service evaluation describes how the 900 Clinic offers an integrated pediatric and adult service for young people, which 84% of responders felt they had had the choice to transfer to when ready. Miles and colleagues also reported that gaining independence and control of their care was seen as a benefit, whilst having to develop trust in new doctor–patient relationships was a disadvantage of moving to adult care. 25 In this service evaluation young people attending the 900 Clinic and the DTSP felt encouraged to develop their independence and health care management skills.
Vijayan et al. 26 conducted a U.S. study of 18 young people (aged 12–24) with PaHIV, alongside 15 of their parents and 9 pediatric health care providers. Stigma associated with HIV, fear of ending life-long patient-caregiver partnerships, and adolescents lacking sufficient skills to adapt to adult services were seen as barriers to transition. 26 Comments from our service evaluation such as “it doesn't make you feel labilised as having HIV” and that all 900 Clinic responders felt comfortable discussing worries and health problems with staff are encouraging. Young people when asked to comment on the good aspects of the 900 Clinic wrote: “… but most important TRUST” and “Staff are very caring and good listeners.” It is essential that young people with PaHIV feel they can develop a trusting rapport with their health care providers, given their concern regarding stigmatisation and reluctance to disclose their status to others. 31 Over 90% of 900 Clinic responders felt they comprehended their health and medical needs, felt they understood their medications and reported knowing how to collect them, suggesting that most young people in this service are learning adult health care behaviors.
A Canadian study of 1507 young adults with diabetes revealed significant fewer diabetes-related hospitalizations following transition if the physician remained the same. 23 This patient–doctor relationship is perhaps more important for HIV-infected children because some will lose a family member to the disease and due to the stigma and secrecy around HIV making open discussion extremely difficult for many. 34 Adults living with HIV have recently cited maintaining a single doctor as extremely important to their care 50 with an impact on adherence to HAART. The 900 Clinic pediatric consultant provides continuity between the pediatric and young adult services, which 75% (15/20) of responders felt made them feel more comfortable during transition. Further work exploring clinical outcome of these young people with PaHIV and engagement in service is underway but will provide more clear comparisons between the diabetic and HIV populations.
Young people with PaHIV who fail to access clinical care are a vulnerable group and could risk their health and potential onward HIV transmission to sexual partners and offspring. It has been previously found that regular outpatient attendances in adults with HIV are associated with reduced high-risk sexual behavior 51 and poor attendance has been associated with poorer outcomes. 52 –55 It has also been reported that younger adults with sexually acquired HIV are more prone to poor attendance than older adults. 55 –57 In the pediatric setting community care and social services provide a network of support to help prevent children with HIV being lost to follow-up. Resource limitations in adult social and community services 7,58 can make engaging nonattending young people more difficult. Therefore, provision of specialist outpatient services for young people with HIV are useful for facilitating development of responsible health-related adulthood behavior skills and ensuring dedicated follow-up of adolescents.
Having the chance to meet others with PaHIV was not a priority for many of the responders from the 900 Clinic. Miles et al. 25 reported that some adolescents with HIV expressed fears regarding potentially predominately gay male health care environments. The free comment sections of this service evaluation revealed that many responders felt more comfortable at the 900 Clinic because of its age-appropriate environment, away from “scary” adults and “little kids.” This was not articulated by the diabetic service users.
It is disappointing that 5 of the 9 young people in this service evaluation who had had an adult inpatient experience had negative experiences regarding their care. Lack of appreciation of the needs of individual young people and insufficient age-appropriate facilities were among the adult ward deficiencies commented on. With an overwhelming majority of patients expressing wishes for a young persons' inpatient facility, it may be necessary to consider inpatient services of this kind to cater for young people suffering with chronic disease. Such findings warrant further research.
The findings described by this questionnaire-based service evaluation are qualitative in nature with small subject numbers, though representing over two thirds of those attending the 900 Clinic at the time of the study. The 900 and DTSP Clinics' 100% response rate is encouraging. As patients were only approached in the outpatient service waiting room, young people who found the 900 and DTSP Clinics difficult to attend due to intercurrent illness, commitments, or personal problems would be less likely to be included. The omission of responses from individual young people not engaging in services represents inherent bias of any clinical service evaluation. Extension of this work to those young people failing to engage or attend transition services would be an important follow-up study for both populations. Although, as the data collection period spanned over 8 months for the 900 Clinic, it is expected that even individuals that attended the service less regularly would be included. One hundred percent of adolescents transferring out of the pediatric Family Clinic have been successfully engaged in the 900 Clinic, leaving not a single young person lost to follow-up. The shorter data collection period of 5 months for the diabetic patients attending the DTSP was less ideal. The patients were recruited by a medical student independent to the 900 Clinic, which may have encouraged participation and eased potential concerns regarding negative responses being seen by clinic staff.
It is encouraging that reported satisfaction of those attending this new service for young people living with PaHIV was as positive as that of responders attending a well-established and evaluated outpatient service for young adults with diabetes in Australia. Sixty-eight percent of responders reported that transition to the 900 Clinic had had a positive effect on their health and well-being in comparison to 72% of those responding at the DTSP. While the mean ages and gender demographics of the two cohorts were similar, diverse cultural and ethical differences exist between the two cohorts and it is difficult to speculate on the impact on the responder's perceptions and satisfaction. Although the two groups were transitioned using different models it is thought that both transition programs adopted the age-appropriate approach, and were flexibly paced to the individual needs of the adolescent. 5 There is no superior transition model 4,5,12 and both transitional services in this service evaluation adopted the key principles previously described as key to successful transition; adolescents in both cohorts were encouraged to develop autonomy and self-management skills 13 and were catered for by a multidisciplinary team responsible for transition with clear transition policies. 5,14,15 Health care resources available to adolescents with PaHIV transitioning in hospitals without funding for a dedicated transition clinic may be limited, however, the fundamental principles of transition, including following an age-appropriate transition protocol can be realistically achieved in these settings. It is possible that the transition coordinator distributing the questionnaire in the DTSP could have some influence on responses, however, all participants were informed that responses would be analysed by a medical student independent to the clinic and that the transition coordinator would not be able to see their completed questionnaire. It would be useful to further study these two groups assessing biological markers of disease activity and progression pre- and post-transition.
This preliminary qualitative service evaluation suggests that young people with perinatally infected HIV feel similarly to those with diabetes, that a dedicated transition service tailored to their requirements can have a positive influence on their health care and personal development. How sustainable this patient-centered approach proves to be in the face of increasing patient numbers and financial constraints requires regular evaluation. Further research on the impact of planned transition care on engagement, attendance and health care outcomes including prevention of onward transmission of HIV and the cost-benefit of such specialist services is required for this challenging and expanding population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.