
Abstract
Chronic hepatitis C is frequent and aggressive among HIV-positive patients; evaluation for anti-hepatitis C virus (HCV)-specific therapy is mandatory, but it has many limitations, due to efficacy, tolerability but also applicability. The objective of our retrospective analysis was to evaluate the eligibility and feasibility of anti-HCV therapy in HIV/HCV-coinfected patients followed at the II Department of Infectious Diseases, L. Sacco Hospital, Milan, Italy, from 2000 to March 2010. In our database, 545 HIV/HCV-coinfected patients were present, representing 40% of our whole HIV population, and 421 included in the analysis. One hundred twenty-four patients were excluded because of loss to follow-up (81) or deceased (43). Forty-eight patients spontaneously cleared HCV during follow-up (11%). Ninety-nine patients received anti-HCV therapy (26%), while the majority was excluded for several reasons (mainly concomitant diseases and low CD4+ cell count). Globally, we found that in at least one third of untreated patients modifiable barriers to treatment were present. The access to therapy was significantly associated with the absence of history of intravenous drug use (p=0.01), a higher CD4+ cells count at nadir (p=0.01), the presence of more than 6 HAART regimens (p=0.04), higher alanine aminotransferase (ALT) levels (p<0.0001), HCV genotype 2 or 3 (p=0.005). In a multivariate analysis, the same factors remained significantly associated with anti-HCV therapy. In conclusion, the feasibility of anti-HCV therapy in HIV/HCV-coinfected patients, in our highly specialized center, is approximately 26%. Relative contraindications, such as substance abuses, mild and controlled concomitant conditions, and low compliance are common and modifiable in order to reconsider patients as suitable for therapy.
Introduction
C
In this setting, the objective of our study was to evaluate the rate of recruitment and eligibility to anti-HCV therapy in our cohort of HIV/HCV-coinfected patients followed at the II Department of Infectious Diseases, Luigi Sacco University Hospital in Milan, Italy, during the period from 2000 to March 2010. The secondary end point was to verify if there were differences between treated and eligible untreated patients, according to epidemiologic characteristics, HIV infection, and HCV disease, in order to identify potentially modifiable parameters that might be further considered to increase feasibility of combination therapy.
Methods
Study design
We retrospectively evaluated all HIV/HCV-coinfected outpatients followed at the II Department of Infectious Diseases, Luigi Sacco Hospital, Milan, Italy, during the period January 2000 to March 2010, through the analysis of our database. Only HIV/HCV-positive patients with adequate follow-up, defined by the presence of at least one visit during the last year were considered in the analysis.
Patient evaluation
Enrolled patients were routinely tested with enzyme-linked immunosorbent assay (ELISA) for the detection of anti-HCV antibodies.
Anti-HCV–positive patients underwent HCV-RNA testing and HCV-genotype determination. Quantitative HCV-RNA was measured by a branched DNA signal amplification (Quantiplex HCV RNA v2.0; Chiron-Bayer, Emeryville, CA) and qualitative HCV-RNA through polymerase chain reaction assay (Cobas Amplicor HCV Monitor v2.0; Roche Diagnostics, Nutley, NJ).
HCV genotypes were determined by reverse hybridization using the Inno-Lipa HCV (Innogenetics, Ghent, Belgium).
For each patient we considered several parameters derived form the clinical chart: age, gender, HIV epidemiology, length of HIV infection, Centers for Disease Control and Prevention (CDC) stage, median nadir CD4+ cell count, number of HAART regimens, HCV genotype, HCV-RNA level, and alanine aminotransferase (ALT) level. Liver fibrosis was defined by liver biopsy, scored according to METAVIR. Since 2006, when FibroScan® (Echosens, Paris, France) was introduced in our clinic, liver stiffness was used to assess liver fibrosis.
Treatment schedule
Patients who underwent anti-HCV therapy were treated with standard IFN with RBV (Copegus®, Roche or Rebetol®, Schering-Plough) during the first months of 2000. Later on, (1) PEG-IFN alpha-2b (1.5 μg/kg per week) was initially administered with RBV at a fixed dose of 800 mg/d, independent of genotype, for those patients who were included in the ICOS study. 7 Subsequently, RBV was prescribed at a weight-based dose of at least 10.6 mg/kg per day. When commercially available, (2) PEG-IFN alpha-2a (180 μg per week) was associated with RBV at a dose of 800 mg/d for genotypes 2–3, 1000 or 1200 mg/d for genotypes 1–4 (for a body weight of less or more than 75 kg, respectively). Treatment duration was usually 48 weeks. According to recent evidence, 27 some patients with genotype 2–3 were treated for 24 weeks in relation to rapid virologic response at 4 weeks.
The positive outcome of anti-HCV therapy was assessed by achievement of SVR, i.e., undetectable qualitative HCV-RNA 6 months after end of treatment.
Statistical Analysis
Patient follow-up began in 2000 and ended in March 2010. Only patients with a visit within the last year were included in the analysis. Patients who underwent anti-HCV–specific therapy were compared to those who were eligible but were not treated. Factors included in the statistical analysis were: age, gender, risk factors for HIV acquisition, duration of HIV infection (more than 10 years), presence of physicians with expertise in hepatology following the patients, nadir CD4+ cells count, CDC stage, number of HAART regimens (more or less than 6), HCV genotype, HCV-RNA level, ALT level, and liver fibrosis. Comparison between groups was performed using Fisher's exact test for categorical variables and t test or Mann-Whitney U test, as appropriate, for continuous variables. Two-sided tests were applied in all comparisons. A p value <0.05 was considered significant. Statistical analysis was performed using Graph-Pad-Instat v3.05 for Windows (GraphPad Software, San Diego, CA). Factors were tested in univariate and multivariate analysis.
Results
A total of 1580 HIV-positive patients were referred to our clinic between January 2000 and March 2010. Screening for HCV and HBV markers was available for 1363 patients: 40% had positive anti-HCV serology. Therefore, 545 HIV/HCV-positive subjects were first considered for inclusion in our database. Four hundred twenty-one patients were included in our final analysis, whereas 124 were excluded (81 lost to follow-up, 43 deceased).
Baseline characteristics of analyzed patients are shown in Table 1. They were mainly men, with a mean age of 47 years. Eighty-three percent were known to be HIV positive for more than 10 years; 96% were on HAART. The majority of patients were CDC stage A (48%, versus 29% stage B and 23% stage C), with a median CD4+ cells count at nadir about 191/mm3. Seventy-eight percent were former injection drug users, while the other 22% acquired the infection sexually.
IDU, injection drug use; HAART, highly active antiretroviral therapy; CDC, Centers for Disease Control and Prevention.
Forty-eight HCV-antibody–positive patients (11%) who did not undergo specific antiviral treatment were HCV-RNA negative, suggesting HCV spontaneous clearance.
Ninety-nine patients (26%) received anti-HCV therapy. Seven patients were treated with standard IFN plus RBV, while most of them received PEG-IFN plus RBV combination. Analyzing the number of treated patients per year, we found a trend toward increasing prescription of anti-HCV therapy in time, from 12% in 2000 to above 20% in 2010 (Fig. 1). Anti-HCV treatment was still ongoing at the time of analysis for 7 patients. Among the 92 subjects who underwent the whole course of therapy and concluded the subsequent 6-month follow-up, SVR rate was 33.6%.
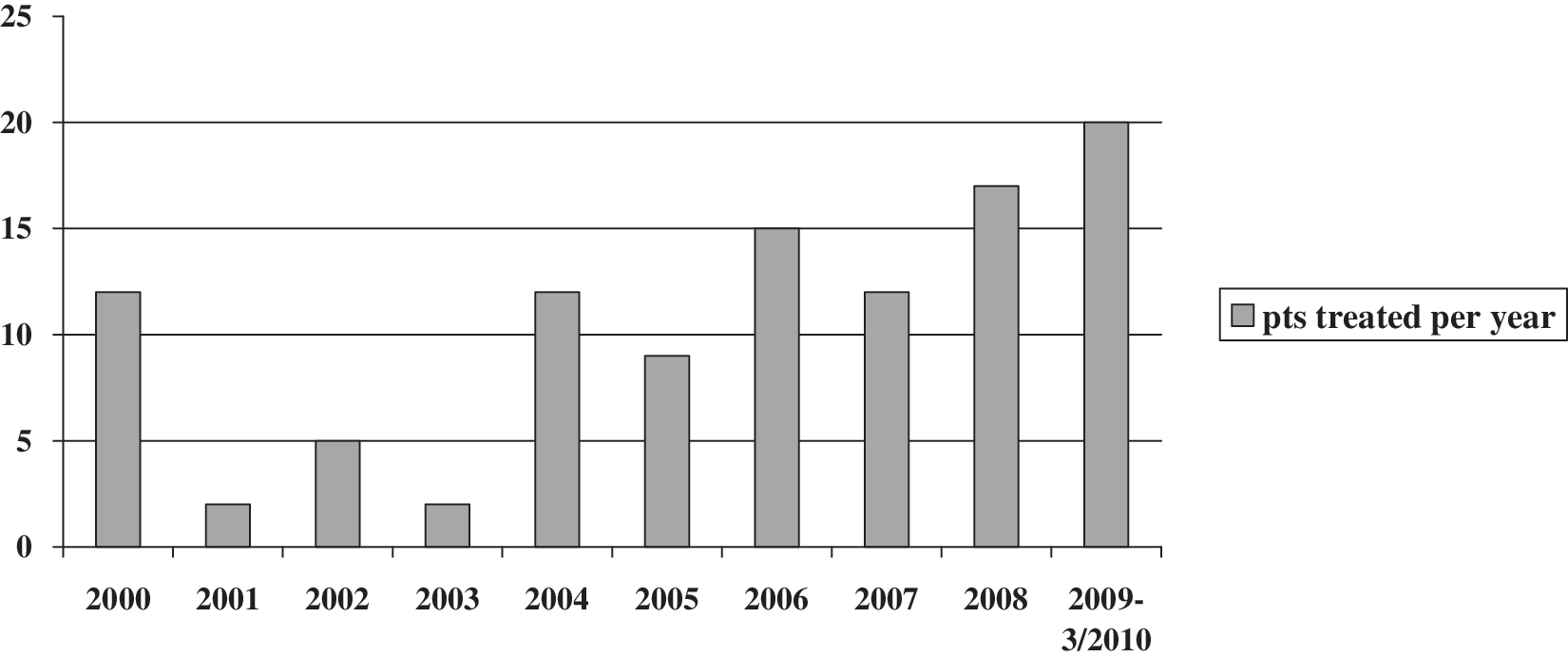
Trend of prescription of anti-hepatitis C virus (HCV) treatment in time, from 2000 to March 2010.
Considering patients excluded from treatment, 87 (31%) had absolute contraindications to anti-HCV therapy, such as serious concomitant illnesses, psychiatric disorders, or thrombocytopenia (less than 50.000/mm3). Twelve patients (4%) had advanced liver cirrhosis (Child-Pugh stage B–C), while for 12 patients (4%) treatment was deemed questionable due to mild liver disease (fibrosis stage F0–1, inflammation grade 1–4, normal ALT) and/or high HCV viral load and genotype 1–4 (Fig. 2).
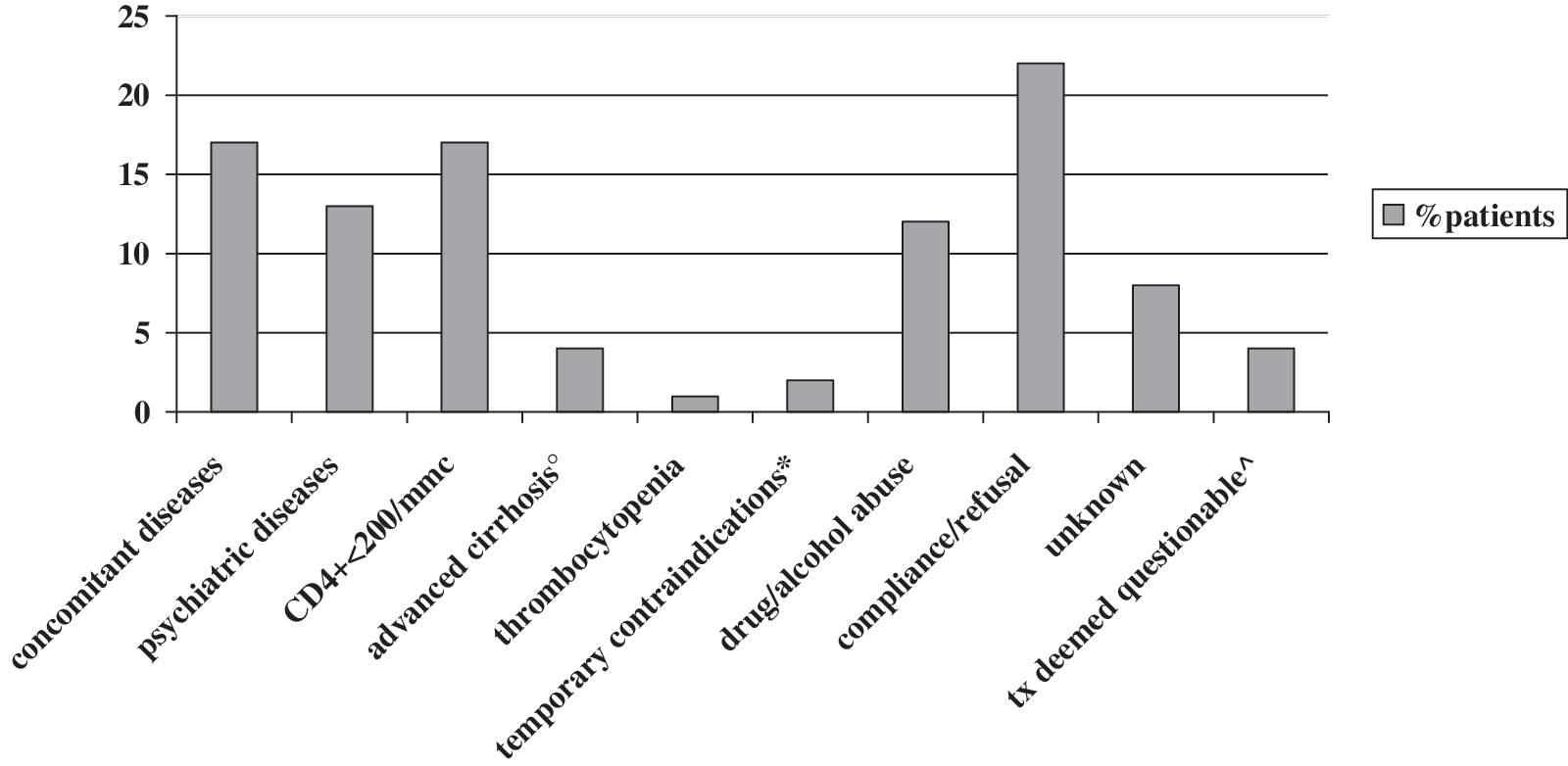
Reasons for treatment exclusion. °Child-Pugh B–C; *pregnancy, family planning; ^mild liver disease (F0-1), genotype 1-4, high HCV-RNA, normal ALT. HCV, hepatitis C virus; ALT, alanine aminotransferase.
On the other hand, 57 subjects (22%) were not treated becaue of patient's refusal or low adherence to HAART, 46 (17%) due to low CD4+ cells count (less than 200/mm3). For 8% of patients we were not able to determine from available data any definitive reasons for treatment exclusion.
Globally, approximately one third of patients excluded from anti-HCV therapy had contraindications at least partially modifiable with an adequate medical approach.
We analyzed variables associated with a wider access to anti-HCV treatment, as shown in details in Table 2. In addition, we evaluated the distribution of patients who underwent anti-HCV therapy among six medical clinics in our department: most of the patients who had access to therapy were referred to the medical clinic where an infectious disease physician with expertise in hepatology was present.
Results of univariate and multivariate analysis.
HCV, hepatitis C virus; SD, standard deviation; IDU, injection drug use; CDC, Centers for Disease Control and Prevention; HAART, highly active antivetroviral therapy; RR, relative risk; CI, confidence interval; n.s., not significant.
Liver fibrosis assessment was available in 70% of the patients who underwent anti-HCV therapy and in 43% of eligible patients (p=0.0001): therefore, this parameter influenced significantly treatment decision.
Predictive factors for access to anti-HCV therapy were: no history of past intravenous drug use (p=0.01), a higher CD4+ cells count at nadir (p=0.01), more than 6 HAART regimens (p=0.04), higher ALT levels (p<0.0001), HCV genotype 2 or 3 (p=0.005). Also the presence in the medical clinic of physicians with expertise in hepatology was relevant for the selection of candidates for therapy (p=0.03, relative risk [RR] 2.23; 95% confidence interval [CI] 1.04–4.78). This medical clinic followed mostly those patients who underwent more HAART regimens: only this last variable was then included in multivariate analysis. In multivariate analysis, the same factors remained significantly associated to anti-HCV therapy.
Discussion
In our retrospective analysis we found that feasibility of anti-HCV therapy is 26% in our cohort of HIV/HCV-coinfected patients during the follow-up. This is higher if compared to other previous studies, where it can reach up to 12.5%. 17 –21 The reasons for these differences in results may be due to the fact that studies are not the same in designs (prospective versus retrospective analysis, large cohort studies), different populations considered, period of analysis. Our study is a recent analysis from 2000 through March 2010, which reflects the actual standard approach to the management of HIV/HCV coinfection, following current international guidelines, 27 –29 with a better understanding of how to treat these patients and how to monitor and deal with side effects. In fact, in our analysis we found that the trend of prescription of anti-HCV therapy showed a significant increase especially during recent years (Fig. 1). Similarly, a recent wider prospective study has showed in 2009 a significant reduction of patients excluded from treatment compared to the 2004 and 2006 surveys. 30 In addition, this is a single- center study, performed in a primary department of infectious diseases in northern Italy, which regularly follows approximately 1600 HIV-positive patients. Among them, the prevalence of HCV coinfection is 40%, which is similar to that reported in other studies in the Mediterranean area. 1 Other single-center studies showed even higher rates of prescriptions of anti-HCV therapy. 23,24 In our center, outpatients are followed in six different medical clinics, which have a different range of patients (23–108), who often present different characteristics (concomitant diseases, active drug or alcohol abuses, epidemiologic features). Even if data are not completely comparable, we found differences in the rates of patients' treatment, showing that the higher rates were observed in those medical clinics, where physicians with expertise in liver diseases worked. Another previous study has also showed that among different factors influencing the access to therapy, patients who were followed by a hepatologist more often were those who received more frequently anti-HCV treatment. 25 This emphasizes the fact that the management of HIV/HCV-coinfection should be addressed preferably to experts in this field, especially in those conditions, like in our department, where sufficient resources are available. Globally, 421 HIV/HCV-coinfected patients were included in the analysis. Among those excluded, we found 43 deaths, and in particular 15 (35%) for cirrhosis and its complications; none of these patients previously underwent anti-HCV therapy, suggesting a possible positive effect of IFN plus RBV therapy in slowing liver disease progression. In our study, 48 patients (11%) spontaneously cleared HCV during follow-up, similar to that reported in other series, with a range of 5–10%. 31 –33
Two hundred seventy-four patients (74%) did not undergo anti-HCV therapy for several reasons. Considering the reasons for patient's exclusion to therapy, we found that the great proportion of patients (31%) were not treated because of the presence of absolute contraindications, especially concomitant diseases (cardiovascular diseases, severe psychiatric disorders). Twelve percent of our patients were excluded because of active alcohol or drug abuse, which is lower than that reported in other studies, 34,35 but these data may be confounded by the fact that it is a retrospective analysis. Low adherence or patient refusal was the cause of exclusion in 22% of the patients, which is relevant if we considered that it should be modifiable with specific interventions. The perception of HCV infection as relatively benign may be one of the reasons of barrier to therapy in these patients, as also pointed out in a recent study in drug users. 36
Finally, in our study, in 20 patients (8%) no definitive reason for exclusion was found based on the patient's clinical chart, emphasizing the fact that adequate screening and monitoring of liver disease is still lacking in few patients, even currently in a primary health care clinic.
In all, 117 patients (31%) presented no actual or temporary contraindications to anti-HCV therapy, showing that these patients might be appropriately referred for therapy with specific approaches, as confirmed by another study. 21 This underlines the need to make big efforts by physicians to consider each HIV/HCV-coinfected patient potentially suitable to therapy and to apply specific interventions to cross over modifiable barriers.
Considering the characteristics of eligible but not treated patients, compared to those who underwent anti-HCV therapy, we found that they were more frequently IDU, suggesting that these patients may be considered unsuitable for therapy because of the risk of lower adherence to therapy. However, several previous reports showed that those patients should be referred for therapy with specific interventions, showing to be as compliant if adequately followed. 37 Considering HIV infection, we were more confident in treating patients who had higher mean nadir CD4+ cell counts (239 versus 191, p=0.01). In addition, in treated patients we found a significant higher numbers of patients who underwent a higher number of HAART regimens modifications (≥6) compared to eligible patients (p=0.04; RR=1.36; 95% CI 1.03–1.80). This may reflect the higher risk of occurrence of liver enzyme elevation, which has negative impact on HAART tolerability and may be one of the reasons to refer for anti-HCV therapy in order to improve HAART tolerability itself. In fact, previous studies have demonstrated that treatment of chronic active hepatitis C reduced the risk of occurrence of hepatotoxicity associated to antiretroviral therapy. 38,39 Considering HCV infection, it is not surprising that most of the excluded patients were genotype 1–4 compared to treated patients (p=0.005; RR=1.52; 95% CI 1.14–2.0), in relation to the lower response rate to anti-HCV therapy. In addition, we found that ALT levels was significantly higher in treated patients if compared to eligible patients (132 versus 73, p<0.0001), underlining that the presence of liver enzyme elevation is important to address patients to antiviral therapy and it may represent a good reason either for physicians or for patients.
In conclusion, our results show that feasibility of chronic hepatitis C therapy in HIV-positive coinfected patients, in a highly specialized center, is 26%. However, in several cases, relative contraindications are present and should be adequately modified through specific interventions by means of multidisciplinary approaches (especially in case of substance abuse or mild psychiatric disorders), in order to reconsider patients as suitable for therapy. In the absence of absolute contraindications, big efforts should be made by physicians to offer an adequate counseling for anti-HCV therapy in all coinfected patients.
Footnotes
Acknowledgments
We are indebted to Davide Minisci for valuable help in data collection.
Partially presented at the 6th International Workshop on HIV & Hepatitis Coinfection, May 31 to June 2, 2010, Tel Aviv, Israel.
Author Disclosure Statement
No competing financial interests exist.