
Abstract
AIDS-related mortality has been significantly reduced in areas that systematically adopted highly active antiretroviral therapy (HAART). In Brazil, despite advances in control policy, there is still a lack of evidence about trends in children on causes of death related or not related to HIV/AIDS. We evaluate temporal trends in mortality due to non-HIV–related causes of death in relation to HIV/AIDS-related conditions among children with and without HIV infection. This nationwide study included all deaths in children reported from 1999 to 2007. Mortality odds ratios (MOR) and rates were calculated to assess time trends of death in children with or without HIV/AIDS. These data were analyzed by calendar year, as obtained from official national database. A total of 680,763 deaths occurred in Brazilian children under 13 years of age; of these, 2191 (0.32%) had causes related to HIV/AIDS listed on the death certificate. The mortality rate from HIV/AIDS-related causes in Brazilian children ranged from 0.72 per 100,000 children in 1999 to 0.40 per 100,000 children in 2007, while for selected nonrelated causes the rate of death among HIV-infected children was stable at 0.08 per 100,000 Brazilian children. In children with HIV/AIDS, the MOR of having selected conditions unrelated to HIV/AIDS as a cause of death in 2007 (compared to 1999) was 1.85 (95% confidence interval [CI]=1.11–3.08, p=0.02), but without a significant temporal trend (p=0.413) through the analyzed period. In Brazil, deaths related to HIV/AIDS mortality in children significantly decreased, while the unrelated causes in HIV-infected children maintained a stable trend. These data reinforce the success of national public health policies and the need to offer comprehensive care to children with HIV/AIDS.
Introduction
T
Some studies indicate an increasing frequency of clinical events, and the long-term effects on children are even more striking than in adults, mainly for those infected since the beginning of life via mother-to-child transmission (MTCT). In children an increased occurrence of metabolic disorders, cerebrovascular diseases, mental health disorders, kidney diseases, and bone disorders has been described. 2 –5
The policy of free access to antiretroviral treatment in Brazil has been considered a benchmark for other low- and middle-income countries worldwide. Since 1996, antiretroviral treatment (ART) access is free and universal, both for treatment of HIV infection and for prevention of MTCT. However, complete HIV suppression in those on ART is lower than for comparable U.S. populations. Additionally, high levels of resistant genotypes have been observed in some areas. 6,7
In children, positive impacts have been observed, with falling trends in vertical transmission of HIV, AIDS-related hospital admissions, morbidity and mortality, and increased survival of children with AIDS. 8,9 Two cohort studies on survival of Brazilian children with AIDS have shown a considerable increase in the probability of overall survival after 60 months, from 52.8% to 88.3% 10,11 (1983–1998 versus 1999–2002, respectively).
Despite the clinical and public health relevance, there are no population-based studies in children investigating trends in causes of death from low or middle-income countries after the introduction of HAART, such as Brazil. The present study focuses on mortality among Brazilian children, according to HIV/AIDS infection status, and analyzes the occurrence of nonrelated deaths in relation to HIV/AIDS-related deaths over time.
Methods
We analyzed trends in causes of death reported on death certificates in Brazilian children (younger than 13 years of age) who died between 1999–2007 and who had HIV/AIDS listed anywhere on their death certificates. In this study, this group was defined as “children with HIV/AIDS”; all other children with causes of death not related to HIV/AIDS were defined as “children without HIV/AIDS.”
We used as our data source Brazilian death certificates as standardized by the Mortality Information System (Sistema de Informação de Mortalidade, SIM) of the Ministry of Health, a national electronic database. It is a physician's responsibility to complete the death certificate form. Until 1995, reference codes were based on the International Classification of Diseases (ICD) in its ninth revision, and after 1996 in its tenth revision.
The mortality analysis in this study focuses on multiple causes of death (including both underlying and any other causes), and on the usual approach of underlying causes of death (the disease or condition that led directly to the death). 12 Results are presented separately and compared.
To define the fields with reference to HIV infection or AIDS on death certificates, we used the SIM databases that have no personal identifiers and were obtained from publicly available website. 13 We selected HIV-related deaths for the purpose of this analysis, using the following ICD-10 codes: B20 (HIV disease resulting in infectious and parasitic diseases), B21 (HIV disease resulting in malignant neoplasms), B22 (HIV disease resulting in other specified diseases), B23 (HIV disease resulting in other conditions), B24 (unspecified HIV disease), and Z21 (asymptomatic HIV infection status).
We evaluated the presence of selected non-HIV/AIDS–associated causes, as defined previously by Pacheco et al. 14 : non-HIV–related neoplasms (C00-C80, except C46–Kaposi's sarcoma), diabetes mellitus (DM; E10-E14), cardiovascular diseases (CVD; I00-I99, except I46-cardiac arrest), digestive diseases (K00-K93), genital–urinary diseases (N00-N99), and external causes (S00-Y98). To analyze the consistency of our data, they were compared with official national data, based on underlying cause of death.
In a first step, HIV/AIDS-related and nonrelated mortality rates for multiple causes of death from 1999 to 2007 were calculated. These mortality rates were calculated by dividing the number of deaths in each calendar year by the population of children, and presented per 100,000 children. Child population estimates were obtained from the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística, IBGE) based on a national population census in 2000 and yearly official estimates (1999, 2001–2007). 15
Second, the analysis was based on a methodology used in a previous study that evaluated temporal changes of causes of death among HIV/AIDS patients of all ages combined at the population level. 14 We estimated mortality odds ratios (MOR) as described in that study, which focus on relative trends rather than the absolute chance of death from these causes.
Statistical analysis was done with STATA 11.0 software package (Stata Corporation, College Station, TX).
Results
From 1999 to 2007, there were 8,903,551 reported deaths in Brazil. Of these, 102,797 (1.15%) had a record of causes related to HIV/AIDS listed on the death certificates. In children, a total of 680,763 (7.65%) deaths were recorded, with 2191 (0.32%) children who died of HIV-related causes as multiple causes of death. During the study period, the specific mean mortality rate for these causes was 0.54 per 100,000 children with a declining trend from 0.72 per 100,000 children in 1999 to 0.40 per 100,000 children in 2007 (p<0.001; Fig. 1). Based only on underlying causes of death, a total of 2006 (0.29%) deaths related to HIV/AIDS were reported from 1999–2007. This corresponds to an HIV/AIDS-specific mean mortality rate of 0.50 per 100,000 children. There were an additional 185 (2191 versus 2006) deaths related to HIV/AIDS when multiple causes of death were included, as compared to the underlying cause.
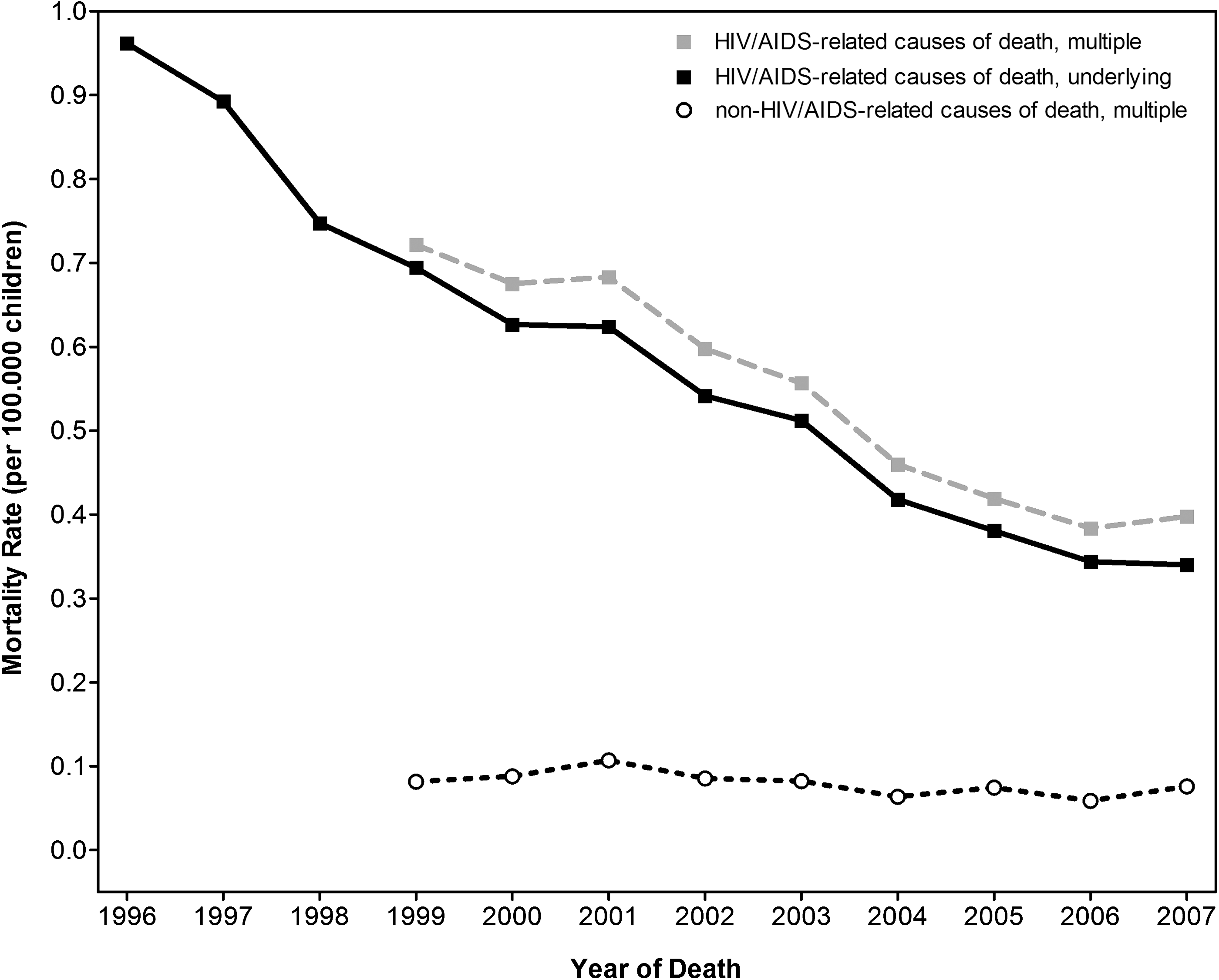
Mortality rates for HIV/AIDS-related and HIV/AIDS-nonrelated causes of death in children with HIV/AIDS, Brazil, 1996-2007. Full data for nonrelated causes of death are only available since 1999.
For the selected non-HIV–related causes of death, the mortality rate was stable in the 1999–2007 period at approximately 0.08 per 100,000 children in the Brazilian population (Fig. 1).
In HIV/AIDS-infected children, multiple causes of death unrelated to HIV/AIDS were recorded in 321 children, 11.3% of cases in 1999, as compared to 19.1% in 2007 (Table 1).
MOR, mortality odds ratio; CI, confidence interval.
Figure 2 shows the trend of the MORs observed in HIV/AIDS and non-HIV/AIDS groups, in children by year of death, with 1999 as the reference. The MOR of having a selected condition unrelated to HIV/AIDS as a cause on the death certificate (2007 versus 1999) was 1.43 (95% confidence interval [CI]=1.39 to 1.47, p<0.001) in children in non-HIV/AIDS group, and 1.85 (95% CI=1.11 to 3.08, p=0.02) in the HIV/AIDS group (Table 1). Despite the increase of non-HIV/AIDS causes in children with HIV/AIDS over this time, the MOR temporal trend test was not statistically significant (p=0.413; Table 1).
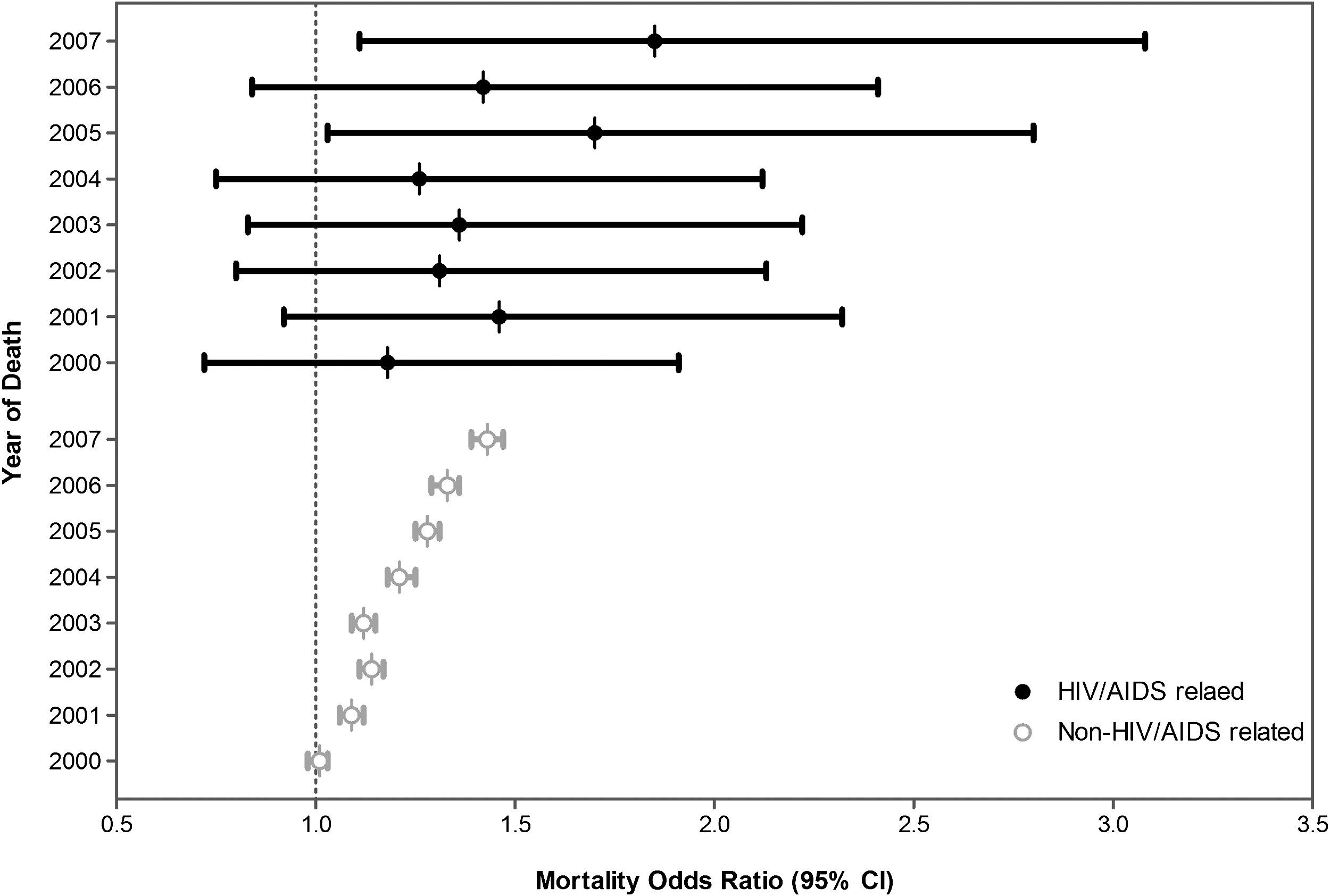
Mortality odds ratios and 95% confidence intervals (horizontal bars) of non-HIV/AIDS–related causes of death (as multiple causes) in children who had and who did not have HIV reported on the death certificate, by year of death (as compared to 1999). CI, confidence interval.
During the period of 1999–2007, in the group of children with HIV/AIDS, 321 (14.7%) deaths (multiple causes) in children were from CVD, in comparison to 123,086 (18.1%) deaths in children without HIV/AIDS. In relation to deaths from cancer: 15 (0.68%) and 9923 (1.46%) deaths were observed, and deaths from diabetes accounted for 3 (0.14%), and 1446 (0.21%), respectively.
Discussion
This study presents the first population-based evidence from an emerging country on temporal trends in causes of death in children with HIV/AIDS after HAART implementation. Our data show a stable trend in selected causes of death not related to HIV/AIDS in these children, in contrast to observations made in developed countries. 2,16 –19 The results also add further evidence to Brazilian studies indicating a reduction of specific mortality related to HIV/AIDS causes of death.
Previous studies mostly from high-income countries have shown that HAART reduced AIDS-related deaths in children. 17 –22 This reduction varied between 67% and 99%, but comparison is limited as different study designs were applied. In our study, the analysis based on multiple causes of death from 1999 to 2007 shows a continuing reduction of 45.8% (0.72 versus 0.39 per 100,000 children) in HIV/AIDS deaths. Additionally, of the total of 2191 deaths in children with HIV/AIDS analyzed, 92% had HIV/AIDS as an underlying cause of death, with a strong decreasing trend in the mortality rate. Our results confirm previous data from the Ministry of Health on reduced mortality rates in children with HIV/AIDS (based on the underlying causes). 23 Brazilian children represented from 1984 to 2008 3.4% of total AIDS cases and 2.3% of reported deaths. There was a significant reduction by 50% in the incidence rate of AIDS in children younger than 5 years of age, from 5.9 in 1998 to 3.0 per 100,000 children in 2008. 23,24
In addition, reduced reduction of MTCT of HIV was observed. 25,26 The MTCT rate was initially estimated at 16% from 1988 to 1993. 27 A subsequent national study including almost 3000 children showed a rate of 7.1% in 2001. 25 Since 1999, over 90% of AIDS cases in children in Brazil had MTCT as the mode of HIV transmission. 23,24
Additionally, other national studies confirm the sustained increase in survival to 60 months after AIDS diagnosis in children. 10,11,28 In the second national cohort study 94.8% of children had received ART, and the survival probability at 60 months after AIDS diagnosis in children with use of HAART was significantly higher as compared to those without. 10
Brazil's national policy of HIV/AIDS control, especially the provision of universal and free access to HAART since 1996 can be seen as a milestone in this context. 28,29 In 2008, the estimated number of Brazilian children under 15 receiving antiretroviral therapy was 8000, with HAART coverage ranging from 65% to more than 95%. 29 The increasing access to HAART impacts on natural history of HIV infection in children. 2,16,30 –32
Striking reductions in mortality from opportunistic infections have been observed mainly in developed countries. 17,18,33 The current challenges seen in high-income countries are also observed in some areas in Brazil, such as the occurrence of long-term complications associated with HAART and HIV infection. 9,34 However, in addition to the significant reduction of HIV/AIDS-related causes of death in children with HIV/AIDS, we observed a stable sustained trend from 1999 to 2007 in HIV/AIDS-nonrelated causes of death in this group of children.
This situation indicates a possible future trend of epidemiologic transition where the causes of death nonrelated to HIV/AIDS have greater relative importance, and will present a potentially higher absolute frequency.
The MOR associated to mortality rates is only a measure to analyze trends and not to compare risks between groups. The MOR estimates the relative risk by comparison with a group in which all causes of death combined are assumed to be constant over time. Pacheco et al. 14 suggested the use of MOR because in Brazil there are no systematic and official sources to estimate the prevalence of HIV infection in each age group. In this study, the denominator for the MOR is not constant: AIDS-related deaths have gone down dramatically.
We identified that these estimates show an increased trend but without statistical significance. The non-HIV/AIDS–related conditions are making up a higher proportion of deaths among children with HIV/AIDS by the MOR analysis because deaths from HIV/AIDS-related causes are going down while the non-HIV/AIDS–related causes maintain a stable trend. The association of MOR and mortality rates in the analysis reinforces the trends of HIV/AIDS-nonrelated causes of death in relation of HIV/AIDS related causes in children with HIV/AIDS.
In contrast to another population-wide study, 14 it was not possible in our study to verify the temporal trends for specific causes: only 321 children had non-HIV–related causes documented. In the other study, with the increase of life expectancy and the importance of chronic disease-related deaths, a large number of diagnoses are reported in the death certificates. 14 These trends were not verified in our study. This may be explained by the lower magnitude of the AIDS epidemic on children in Brazil, due to the significant reduction of MTCT of HIV and the enhanced survival. Otherwise, if MTCT is lower, then the denominator of children with HIV and those more likely to contribute to the numerator with deaths from opportunistic infections at early ages will be smaller. Those who are aging with HIV and more likely to have serious non-AIDS–related end points or death from chronic disease are then the larger portion of the denominator. The cohort most affected by the pediatric epidemic in Brazil might simply not yet be old enough to observe the types of end points seen in the U.S. epidemic.
This study is highly representative, as it included all death certificates during a period of 9 years in a country of continental dimensions, major social and economic inequalities, and an established public policy of coping with AIDS. The use of multiple causes of death related to HIV/AIDS avoided losing information among conditions not classified as the underlying cause of death, providing a more accurate support for planning and evaluating health programs. 35
Our study is also subject to limitations, mainly related to the use of a secondary database that may have variations in sensitivity/specificity in terms of analysis of causes of death. 14 Completion rates of death certificates in children are not known, and it is possible that regional differences of the quality of SIM may have affected the results. Additionally, there is no way to control in this population-based study for confounders. Considering the national policy, most children who progressed to death had a higher probability to access HAART as compared to children who died before 1999. However, we recognize that in some areas in Brazil, children are still diagnosed at a late stage, sometimes even at the moment of death. In addition, completion rates of the death certificate forms for children in Brazil may vary by regions.
In conclusion, HAART use in children is associated with a significant reduction in HIV/AIDS specific mortality in Brazil, reinforcing the importance of the policy of universal access to HAART. The relative stabilization in non-HIV/AIDS–related conditions as causes of death in HIV-infected Brazilian children stresses the need to integrate HIV/AIDS programs with other national health programs such as long-term nontransmissible disease management.
Footnotes
Author Disclosure Statement
No competing financial interests exist.